
Rehabilitation for Children while Playing with a Robotic Assistant in a
Serious Game
L.V. Calderita
1
, P. Bustos
1
, C. Su
´
arez Mej
´
ıas
2
, B. Ferrer Gonz
´
alez
2
and A. Bandera
3
1
RoboLab, University of Extremadura, C
´
aceres, Spain
2
GIT, UCAi, Hospital Universitario Virgen del Roc
´
ıo, Sevilla, Spain
3
Grupo ISIS, University of M
´
alaga, M
´
alaga, Spain
Keywords:
Neuro-rehabilitation Therapies, Socially Assistant Robotics, Augmented Reality, Serious Games, Paediatric
Patients.
Abstract:
Traditional neuro-rehabilitation therapies are usually repetitive and lengthy, reducing motivation and adher-
ence to the treatment and thus limiting the benefits for the patients. Moreover, exercises are usually not
customizable for the patients, further increasing their disengagement with the treatment. The outcome is then
a boring session day after day. This is more pronounced when the patient is a child. However, the execution of
these repetitive movements is really needed, as it alters the properties of our neurons, including their pattern
of connectivity. Correctly driven, this process finally allows to improve the neural functionality. The question
is then: how can we improve the motivation and immersion of the patients into the therapy? We could try to
convert the boring therapy into a funny one. This will help to the patients, but also to the practitioner. For
this end, computer-assisted technologies have been extensively employed in the last years. Within this re-
search field, this paper proposes to engage the child to the therapy by immersing her into an augmented reality
scenario, where it will play several serious games. The adherence to the session will be further increased by
incorporating a social robot as a playmate. This robot will be a personal trainer, that will perform the session
in the real world with the patient. Additionally, the robot will be able to record the data for each session. This
data could be subsequently used by the rehabilitation specialists for monitoring and/or adapting the therapy to
the patient’s needs.
1 INTRODUCTION
Exploiting the use-dependent plasticity of our neu-
romuscular system, neuro-rehabilitation therapies are
devised to help patients with some motor impairment.
These therapies take advantage of the fact that the
motor activity alters the properties of our neurons,
including the pattern of their connectivity, and thus
their functionality (Leocani and Comi, 2006). Hence,
a sensor-motor treatment where the patient makes cer-
tain movements, will help him to (re)learn how to
move the affected body parts. Because lack of arm-
movement control directly affects activities of daily
living and independence (Whitall et al., 2000), this
improving of the upper-limb motor function is of
great importance.
The basis of the rehabilitation process is the repe-
tition of certain movements, being the recovery corre-
lated with the frequency and intensity of these move-
ments. On the contrary, passive movements -postures-
are insufficient to alter motor recovery. Hence, the fo-
cus of the rehabilitation should be on movement co-
ordination (active) rather than muscle strengthening
(passive) (Hermano and Hogan, 2009). This tradi-
tional rehabilitation process comes at a cost: therapies
are usually repetitive and lengthy, reducing motiva-
tion and adherence to the treatment and thus limiting
the benefits for the patients (Steultjens et al., 2003).
Clinical experiments demonstrate that motivation
is an important factor for successfully addressing a
lengthy neuro-rehabilitation therapy and it is usu-
ally employed as a determinant of rehabilitation out-
come (Colombo et al., 2007). Hence, active engage-
ment towards a therapy is typically equated with mo-
tivation. Technology-assisted training can provide
engaging and task-oriented training using patient-
tailored feedback to support the (re)learning of motor
skills (Timmermans et al., 2009). From pioneering
systems such as the Lokomat from Hocoma (Jezernik
et al., 2003), the application of computer-assisted
89
V. Calderita L., Bustos P., Suárez Mejías C., Ferrer González B. and Bandera A..
Rehabilitation for Children while Playing with a Robotic Assistant in a Serious Game.
DOI: 10.5220/0004646700890096
In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics (VirtRehab-2013), pages 89-96
ISBN: 978-989-8565-80-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

technologies to rehabilitation has generated a pos-
itive feedback from therapists. For instance, the
ArmeoSpring, a more recent proposal from Hocoma,
is a robotic tool to improve therapy by facilitating in-
tensive and functional movement exercises. As it is
proposed by Colombo et al, this tool supports the ther-
apy by motivating, game-like tasks (Colombo et al.,
2007). Video games have long been known to be en-
gaging to play. Thus, if rehabilitation games with
a similar degree of engagement are created, it will
be possible to improve the therapeutic results. For
this end, gaming consoles that combine entertainment
and exercise such as the Nintendo Wii or the Sony
Eyetoy can be employed. On the contrary, commer-
cial games could not be useful for people with mo-
tor function problems. They are often too fast and
frequently provide negative feedback when they are
lost (Burke et al., 2010). The design of rehabilita-
tion games requires the a priori definition of the spe-
cific profile of the patient and the rehabilitation ob-
jectives. Some of these rehabilitation games employ
virtual (augmented) reality technology to immerse the
patient in a virtual scenario. For motor function reha-
bilitation, it is also common to incorporate technology
to track the movements of the patient. This tracked
data can be then used to drive a graphical represen-
tation of the patient (or a part of her) in the virtual
world. The advantages of this scenario are twofolds:
it enables the patient to achieve a high degree of con-
trol onto her activity on the game; and it improves
the degree of engagement of the game. Both issues
improve the rehabilitation therapy, increasing the pa-
tient’s control of her movements (there is a goal like
in functional-based therapies) or her motivation.
This paper proposes to combine the engagement
capabilities shown by rehabilitation games with hand-
off assistive robotics. Given the inherent people ten-
dency to engage with life-like social behaviour, the
use of the robot for augmenting or maintaining the
patient’s motivation provides an important advantage
over game-based approaches (Fasola and Mataric,
2011). Thus, socially assistive robots emerge as a
new field of robotics whose aim is to develop systems
that assist patients through social rather than phys-
ical interaction (Tapus et al., 2007). They provide
therapy oversight, coaching and motivation using the
robot’s abilities to interact and maintain the interest
of patients. These robots are described as an intersec-
tion of assistive robotics (those that provide assistance
to a person) and socially interactive robotics (those
that communicate with people through social, non-
physical interaction) (Feil-seifer and Matari
´
c, 2011).
We have developed a system that uses low-cost gam-
ing and robotics technologies for the rehabilitation of
paediatric patients with upper-limb motor deficit due
to cerebral palsy or brachial plexus palsy (obstetric),
but without significant cognitive or communicative
deficits.
1.1 Motivation
Cerebral palsy is a neurological chronic impairment
usually caused by a prenatal brain defect or by brain
injury during birth, that has a specific influence in
certain motor areas. It can appear in the first gesta-
tion day or within the first three or five years, mani-
festing with several symptoms including muscle tone,
posture and movement disorders. In addition, cogni-
tive impairments, communicative disorders, and con-
vulsive seizures (epilepsy) may be present. The inci-
dence of cerebral palsy is about 2 per 1000 live-births
in developed countries and slightly greater, about 2.5
per 1000, in developing countries. Longer prevalence
has been detected due to the increase in survival rate
in children born with low weight or other risk fac-
tors such as premature, maternal-child malnutrition
and having a pregnancy with low control. This large
incidence has an important impact on the clinical re-
sources. For instance, in 2010, 1.135 new patients
asked for a first session on paediatric rehabilitation
due to this pathology, and a total of 2.957 patients
where attended at the Hospital Universitario Virgen
del Roc
´
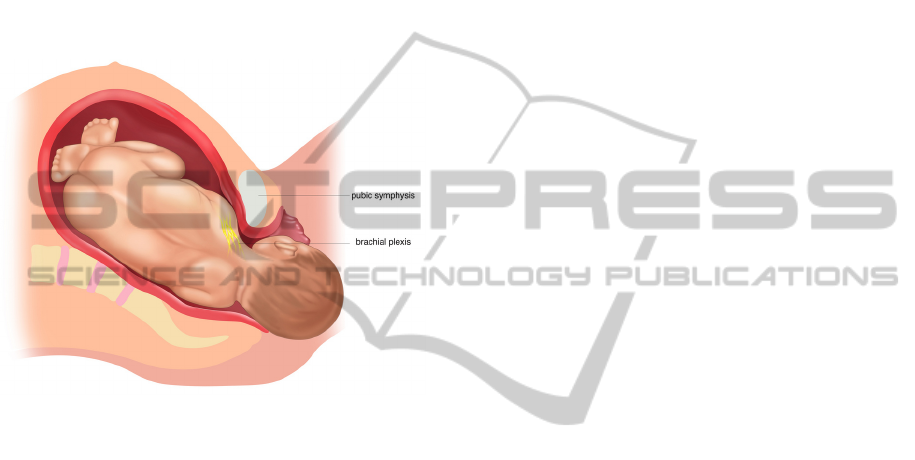
ıo (HUVR) in Seville. On the other hand, ob-
stetrical brachial paralysis is defined as a flaccid pare-
sis of an upper extremity due to traumatic stretching
of the brachial plexus received at birth, with the pas-
sive range of motion greater than the active range mo-
tion (see Fig. 1)
1
. Brachial palsy is a paralysis in-
volving the muscles of the upper extremity that fol-
lows mechanical trauma to the spinal roots of C5 to
T1 during birth. Injuries are transient, with full re-
turn of function occuring in 70-92 % of cases (Mich-
elow et al., 1994). In Spain, we find about 160-230
new cases of this pathology per year, which will be
associated to other visceral, vascular or cranial in-
juries. There is certain stability in the incidence of
this pathology in recent years, but this ranges from
0.5 to 1.9 per 1000 live-births.
In order to ensure that children suffering from
these two pathologies achieve the highest level of re-
covery possible, it is essential that they start sched-
uled physical therapy sessions as soon as possible.
These sessions should also be regularly conducted (in
an ideal case, it would be desirable that each patient
will be treated every day). However, both issues are
not always possible due to the lack of therapists. In
fact, at HUVR, these patients are usually treated one
1
http://catthsu.com/medlegal.html
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
90
time per week. Also, it must be noted that the degree
of affectation of each patient is very different accord-
ing to both the seriousness of the disease and the bod-
ily functions affected, so it is essential that rehabilita-
tion sessions will be personalised. However, the con-
ventional rehabilitation treatment for these patholo-
gies is usually based on the repetition of a set of te-
dious exercises. This is a problem for paediatric pa-
tients due to their young age, as they would prefer do-
ing fun exercises instead of repeating the same move-
ments for twenty minutes. The resulting loss of moti-
vation can be a serious obstacle for the therapy.
Figure 1: Shoulder dystocia.
The described scenario is then suitable for the ap-
plication of new therapies based on a socially assis-
tive robot, being the use case where our robot will un-
fold its abilities. Thus, the robot acts as a coacher in
the session, explaining the exercises to the child (’we
will now play to’) and providing positive messages
through verbal and non-verbal channels. Games will
be based on an augmented reality framework, where
the entire body of the child will be projected inside a
virtual world. Within this world, the child could wear
a superhero themed uniform and will be encouraged
to perform specific exercises. In the pilot study pre-
sented in this paper, we investigated the effects of this
system on motor recovery but also on acceptance and
satisfaction grade from the patients and medical staff.
1.2 Organization of the Paper
The rest of the paper is organized as follows: Sec-
tion 2 describes the involved technologies and the pro-
posed therapy. Experimental results are presented at
Section 3. Finally, Section 4 draws the main conclu-
sions and briefly introduce future work.
2 METHODOLOGY
2.1 Involved Technologies
Traditional rehabilitation therapies may be tedious.
The problem is even worse when the patient is a child.
The medical staff in this project has reported us its ex-
perience with children and adults. An immediate ob-
servation is that the effort of the practitioner to main-
tain the attention and motivation must be greater when
the patients are children. Thus, if the therapist works
with paediatric patients, she will usually need to use
little games or toys to keep their adherence to the
treatment. Within this framework, we have provided
the physiotherapists with a new tool: Ursus. Ursus
is a robot designed to conduct rehabilitation exercises
with children, developed by the RoboLab Group with
the collaboration of the Hospital Universitario Virgen
del Roc
´
ıo (Seville). It is a low-cost design in which a
static torso holds two robotic arms with five degrees
of freedom (DoF) each, a three DoF neck and an ar-
ticulated mouth. The head is capable of generating
simple emotions. The full platform is composed of 14
DoF and is 140 cm tall. After several revisions, it cur-
rently looks just like a big teddy bear (see Fig. 2). The
final goal for Ursus is to make the patient move the af-
fected upper limb in each therapeutic session accord-
ing to a predefined plan. These movements should
be as correct as possible and repeated with a proper
cadence.
In order to achieve this goal, Ursus will try to en-
gage the child in the game. These therapeutic games
are more than just entertainment, being their main
purpose that the patient performs specific movements
for rehabilitation (Rego et al., 2010). As described
in Section 1, games can try to improve the immer-
sion of the player into the action by using virtual or
augmented reality. To help and encourage the child
to play the game, we propose to incorporate to this
scenario a robotic playmate. Ursus will explain to
the child how to play using synthetic speech and will
project on a screen an Augmented Reality (AR) game.
In this game the child is the main actor and is encour-
aged to perform specific tasks such as grabbing some
fruits from a tree or throwing them to a basket. A
snapshot of the real scenario is illustrated in Fig. 3.
Ursus is equipped with a Red-Green-Blue and Depth
(RGBD) sensor, such as a Kinect from Microsoft or a
Xtion from Asus (Khoshelham and Elberink, 2012)
and with speakers. All software and hardware com-
ponents are running on-board within a conventional
laptop powered by the RoboComp robotics frame-
work (Manso et al., 2010) (see (Mej
´
ıas et al., 2013)
for further details about Ursus).
RehabilitationforChildrenwhilePlayingwithaRoboticAssistantinaSeriousGame
91

Figure 2: Ursus: a robotic platform for neuro-rehabilitation
therapies.
Although we could use the capacity of the OpenNI
library for tracking human bodies, we have integrated
this ability within a model-based approach for human
motion capture. We provide some results on Section
3 (see (Calderita et al., 2013) for further details). The
aim is to employ the chest or the torso of the child
like a visual landmark of augmented reality. Then, we
build a virtual scenario around the child for each re-
habilitation session (see Section 2.2 for further details
about the games). As we a priori knows the profile of
the patient, each game can be easily customizable.
2.2 The proposed Therapy
As Figure 3 shows, when the exercise begins there is
one child in front of Ursus. The child motion is cap-
tured using the depth channel of the RGBD sensor
and the previously commented approach. This hu-
man motion capture algorithm is based on the OpenNI
library and provides the position and angles of the
joints of the person under analysis. This informa-
tion is further filtered using a kinematic model of the
child (Calderita et al., 2011; Calderita et al., 2013) to
avoid unreal poses and changing bone lengths. The
accuracy of the system is enough to deal with the task
since the medical staff does not evaluate more than
ten degrees of freedom.
Currently, our serious games are very simple and
they only try to encourage the correct performing of
certain movements. Nevertheless, the simplicity of
these games proved to be valid for the patients in our
experimental evaluations (children whose age ranges
from 3 to 7 years old). In these games, Ursus controls
the device that projects the real image of the child in-
side of a virtual scenario. This image is also taken
from the RGBD sensor but now using the color chan-
nels (Khoshelham and Elberink, 2012). In real time,
Ursus merges both sources of information to create
on the screen a, so called, augmented scenario. It is
over this video sequence where the virtual world is
projected. The game virtually dresses the child with
a red-and-blue themed uniform, much in the spirit of
Superman or Spiderman suits. This uniform partially
covers the limbs and torso of the child. On the floor,
close to the child, there is a big tree with apples next
to a basket. Up in the air, an enormous apple is in-
flated and deflated, seeking to capture the attention of
the patient. It should be noted that the location of all
objects inside the virtual scenario is relative to the po-
sition of the patient, as she is the reference landmark.
The child is verbally encouraged by Ursus to take
the apple and put it into the basket. To this end, Ursus
uses a probabilistic grammar to generate the adequate
sentences in real-time. This algorithm takes into con-
sideration the time from the beginning of the session,
the number of repetitive movements performed and
the current state of the interactive game. The aim is
to encourage and help the child to pass the current
level of the game. We consider that the child’s moti-
vation will be greater if she thinks that Ursus is a real
playmate. And this feeling is enforced by ’humaniz-
ing’ the human-robot interaction process. Thus, Ur-
sus synchronizes the speech generation with current
movements of its lips (Cid et al., 2011) and also with
correct non-verbal gestures (e.g. when it says ’yes’
or ’no’, it simultaneously enforces the sentence with
a current motion of its head).
The game suggests repetitive exercises to the child
and Ursus encourages her to do these movements
through verbal and non-verbal (it also performs the
movements) cues. It is a real playmate. Taken into
account the patient’s profile and how she is respond-
ing to the current session, the difficulty of the game
can be adapted by the practitioner through a simple
control panel. This panel also allows the practitioner
to change the boundary of the game, to select other
games or to show to the patient previously recorded
videos with the exercises to perform. Finally, this
control panel also allows to visualize the patient from
the RGB camera that is mounted on Ursus. Further-
more, all data is recorded by Ursus, allowing to the
medical professionals the off-line visualization of the
session. This off-line monitoring (see Fig. 4) of the
patient’s movements is displayed using a graphic in-
terface (GUI) that not only provides the video se-
quence, but also numeric information about the am-
plitude (in milimeters) of the movements.
2
2
see a more extended example of the GUI at https://
www.youtube.com/watch?v=3NsYDbwsBYs
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
92

Figure 3: Ursus, patient and AR-based serious game in action. The picture was taken at the Hospital Virgen del Roc
´
ıo (Seville,
Spain) and provides a good snapshot of the sessions with reals patients.
3 EXPERIMENTAL EVALUATION
3.1 Participants
This work focuses on the rehabilitation of paediatric
patients with upper-limb motor deficit due to cerebral
palsy or brachial plexus palsy (obstetric), but with-
out significant cognitive or communicative deficits.
In order to evaluate the proposed therapy, an exper-
imental group of six paediatric patients was chosen
by the medical staff of the Department of Rehabili-
tation of the Hospital Universitario Virgen del Roc
´
ıo
at Seville (Spain). As aforementioned, the age of the
children ranges from three to seven years old. They
present upper-limb motor deficit due to cerebral palsy
or brachial plexus palsy.
3.2 Rehabilitation Objectives and
Preliminary Results
Ursus performed several rehabilitation sessions with
this group of patients. The session was presented to
the child more like a game with a robotic friend than
a repetition of exercises. In any case, the mandatory
movements demanded by the games include shoulder
flexion and abduction, elbow flexion and extension,
wrist flexion and extension, and forearm pronation
and supination. There was always a therapist super-
vising the session. In an on-line fashion, she was able
to perceive how the patient made the movements us-
ing the information provided by Ursus. This monitor-
ing allowed the therapist to personalise the treatment
and determine the evolution of the recovery. Showing
calmly the correct movements with his arms, talking
about interesting matters for the child, playing mu-
sic and projecting pictures, videos and augmented re-
ality (AR) games on an external screen, were some
of the resources that Ursus pull out to capture the
child’s attention and interest. It is important to note
that the main difficulty here was to detect the atten-
tional state of the patient when using each resource,
in order to correctly decide what to do next. Games
based on augmented reality technologies were a nat-
ural extension for Ursus, which was always tracking
the patient’s silhouette.
The clinical variables that were used for evalu-
ating the clinical evolution of the patient were pas-
sive and active articular balance of the shoulder, el-
bow and hand; degree of concordance (i.e. precision
of the movements performed by the child with re-
spect to theoretical values); motor function of upper-
limbs (’Nine Hole Peg Test’) and patients’ satisfac-
tion (’Goal Attainment Scale’). However, the val-
idation methodology of the therapy must also con-
sider, in our case, metrics related to human-robot in-
teraction. These metrics should quantify the level of
attention and engagement between robot and child.
In this work, qualitative results were obtained from
several polls of all the participants in the experiment
(paediatric patients, parents and technical and medi-
cal staff). These polls were conducted before and af-
ter the sessions and the answers were classified de-
RehabilitationforChildrenwhilePlayingwithaRoboticAssistantinaSeriousGame
93

Figure 4: The visualization of the session in the off-line mode.
pending on the satisfaction level of the experience.
From them, it can be concluded that the physical ap-
pearance of Ursus was quite satisfactory and that pa-
tients enjoyed the rehabilitation session and they con-
sidered it more fun and motivating than only using
the conventional treatment. Moreover, the medical
staff also considered the rehabilitation session posi-
tive for the children rehabilitation process, and the re-
sults recorded by the robot very useful for analysing
the evolution of the patients and planning personal-
ized future rehabilitation sessions. Briefly, it can be
concluded that Ursus was able to achieve a high level
of engagement by the patient, maintaining the levels
of motivation and adherence to the treatment.
On the other hand, one of the main contributions
of this work is the capability of the robot Ursus to
measure and record the whole therapeutic session. As
aforementioned, we employ the method recently pro-
posed by the authors in (Calderita et al., 2013) to
capture the patient motion. Basically, we propose to
use a human model to constraint the body motion to
reachable and valid positions. It filters the deviations
of the 3D position of several relevant body parts as
model limb lengths converge toward stable values in
the learning phase (Calderita et al., 2013). Thus, even
although the OpenNI tracker provides 3D centroids
for all body parts in all processed frames, these val-
ues are modified as the model adopts, for every rele-
vant body part, the 3D position that is closest to the
centroid provided by OpenNI, but constrained by the
human model kinematics. Using this approach, the
angular positions of the patient’s limbs are recorded
in real-time with a precision of a few degrees. As Ta-
ble 1 shows for the right elbow, the joints positions are
also recorded with a precision of only few centime-
ters. Results depicted in Table 1 show that the pro-
Table 1: Mean errors and standard deviations of the right
elbow, in centimetres (Calderita et al., 2013).
Mean err Std dev
OpenNI centroids 6.7 cm 2.7 cm
Fixed limb lengths 7.2 cm 2.3 cm
Adaptive limb lengths 4.9 cm 1.7 cm
posed method improves the accuracy of the OpenNI
tracker, decreasing both elbow mean error and stan-
dard deviation.
4 CONCLUSIONS AND FUTURE
WORK
In this paper, we describe our short-time experiences
on the rehabilitation of paediatric patients with upper-
limb motor deficit due to cerebral palsy or brachial
plexus palsy (obstetric). The idea of using a social
robot as a playmate increased the motivation and in-
terest of the children in the rehabilitation sessions,
showing us that the acceptance of Ursus was not a
problem in this scenario. It was very nice to see how
one of the children, after conducting the session, ap-
proached to Ursus to give it a hug. On the other
hand, the acquisition of data information about the
session was conducted on real-time, in a very pre-
cise way (see (Calderita et al., 2013) for further de-
tails about our approach for human motion capture).
Furthermore, this data can be replayed and analysed
at any time by the specialists, allowing them to com-
pare the evolution of the patient, in each session, in a
new quantitative way. We expect to improve with this
methodology and techniques the current procedures
based on standard tests.
Future work focuses on extending these experi-
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
94

Figure 5: Ursus interacting with a child.
ences, designing new interactive AR games specif-
ically aimed at generating therapeutic movements
while providing a stimulating and joyful experience.
Finally, during the sessions, the robot will register all
movements made by the child and will compare these
movements with the normalized patterns defined by
the physicians. The computed difference should be
used to generate on-line reinforcement verbally syn-
thesized discourses and expressions. It is important
to consider that, despite we have presented a rather
simple scenario, the complexity of keeping the child’s
attention during twenty minutes each session and dur-
ing tens of sessions, is daunting. Only a well designed
robot with a suitable cognitive architecture and the
knowledge of trained clinicians provides the neces-
sary material to pursue this kind of research.
ACKNOWLEDGEMENTS
This work has been partially granted by the
Spanish Ministerio de Econom
´
ıa y Competitividad
(MINECO) and FEDER funds under coordinated
project no. TIN2012-38079.
REFERENCES
Burke, J., McNeill, M., Charles, D., Morrow, P., Crosbie,
J., and McDonough, S. (2010). Designing engag-
ing, playable games for rehabilitation. In Proc. 8th
Intl Conf. on Disability, Virtual Reality and Assoc.
Technologies, Vi
˜
na del Mar/Valpara
´
ıso, Chile, August,
pages 195–201.
Calderita, L., Bachiller, P., Bandera, J., and Bustos, P.
(2011). Mimic: A human motion imitation component
for robocomp. In Proceedings of the 1st Workshop on
Recognition and Action for Scene Understanding (RE-
ACTS 2011), M
´
alaga, Spain.
Calderita, L. V., Bandera, J. P., Bustos, P., and Skiadopou-
los, A. (2013). Model-based reinforcement of kinect
depth data for human motion capture applications.
Sensors, 13(7):8835–8855.
Cid, F., Cintas, R., Manso, L., Calderita, L., S
´
anchez, A.,
and N
´
u
˜
nez, P. (2011). A real-time synchronization al-
gorithm between text-to-speech (tts) system and robot
mouth for social robotic applications. In Proceedings,
Workshop en Agentes F
´
ısicos (WAF 2011), Albacete,
Spain, pages 81–86.
Colombo, R., Pisano, F., Mazzone, A., Delconte, C.,
Micera, S., Carrozza, M., Dario, P., and Minuco, G.
(2007). Design strategies to improve patient motiva-
tion during robot-aided rehabilitation. Journal of Neu-
roEngineering and Rehabilitation, 4(1):1–12.
Fasola, J. and Mataric, M. (2011). Comparing physical and
virtual embodiment in a socially assistive robot exer-
cise coach for the elderly. Technical report, Technical
Report CRES-11-003, Center Robotics and Embed-
ded Systems, University of Southern California.
Feil-seifer, D. and Matari
´
c, M. J. (2011). Ethical principles
for socially assistive robotics.
Hermano and Hogan, N. (2009). A working model of
stroke recovery from rehabilitation robotics practi-
tioners. Journal of NeuroEngineering and Rehabili-
tation.
Jezernik, S., Colombo, G., Keller, T., Frueh, H., and Morari,
RehabilitationforChildrenwhilePlayingwithaRoboticAssistantinaSeriousGame
95

M. (2003). Robotic orthosis lokomat: A rehabilitation
and research tool. Neuromodulation: Technology at
the Neural Interface, 6(2):108–115.
Khoshelham, K. and Elberink, S. O. (2012). Accuracy and
resolution of kinect depth data for indoor mapping ap-
plications. Sensors, 12(2):1437–1454.
Leocani, L. and Comi, G. (2006). Electrophysiological
studies of brain plasticity of the motor system. Neuro-
logical Sciences, (1).
Manso, L., Bachiller, P., Bustos, P., N
´
u
˜
nez, P., Cintas, R.,
and Calderita, L. (2010). Robocomp: a tool-based
robotics framework. In Simulation, Modeling, and
Programming for Autonomous Robots, pages 251–
262. Springer.
Mej
´
ıas, C. S., Echevarr
´
ıa, C., Nu
˜
nez, P., Manso, L., Bus-
tos, P., Leal, S., and Parra, C. (2013). Ursus: A
robotic assistant for training of children with motor
impairments. In Converging Clinical and Engineer-
ing Research on Neurorehabilitation, pages 249–253.
Springer.
Michelow, B., Clarke, H., Curtis, C., Zuker, R., Seifu, Y.,
and Andrews, D. (1994). The natural history of ob-
stetrical brachial plexus palsy. Plast. Reconstr. Surg.,
93(4):675–680.
Rego, P., Moreira, P. M., and Reis, L. P. (2010). Seri-
ous games for rehabilitation: A survey and a classi-
fication towards a taxonomy. In Information Systems
and Technologies (CISTI), 2010 5th Iberian Confer-
ence on, pages 1–6. IEEE.
Steultjens, E. M., Dekker, J., Bouter, L. M., van de Nes,
J. C., Cup, E. H., and van den Ende, C. H. (2003).
Occupational therapy for stroke patients a systematic
review. Stroke, 34(3):676–687.
Tapus, A., Mataric, M. J., and Scassellati, B. (2007). So-
cially assistive robotics. IEEE Robotics and Automa-
tion Magazine, 14(1):35.
Timmermans, A. A., Seelen, H. A., Willmann, R. D., and
Kingma, H. (2009). Technology-assisted training of
arm-hand skills in stroke: concepts on reacquisition
of motor control and therapist guidelines for rehabil-
itation technology design. Journal of neuroengineer-
ing and rehabilitation, 6:1.
Whitall, J., Waller, S. M., Silver, K. H. C., and Macko,
R. F. (2000). Repetitive Bilateral Arm Training With
Rhythmic Auditory Cueing Improves Motor Function
in Chronic Hemiparetic Stroke. Stroke, (10).
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
96
