
Technology in Physical Therapy
Wireless Sensors and the Sensorimotor Training
A. Thiers
1
, A. l’Orteye
2
, K. Orlowski
1
and T. Schrader
1
1
Brandenburg University of Applied Sciences, Department of Informatics and Media, Brandenburg an der Havel, Germany
2
St
¨
adtisches Klinikum Brandenburg GmbH Akademisches Lehrkrankenhaus der Charit
´
e,
Abteilung Medizinische Schule, Brandenburg, Germany
Keywords:
Wireless Sensors, Sensorimotor Training, Proprioception, EMG Data, Motion Data.
Abstract:
The usage of evidence based decision making is supported along the different professions in the health care
system. State of the art in the physiotherapy, especially in the sensorimotor training is that the therapy planning
mainly based on the experiences of the physiotherapist as well as by the information given by the manufacturer
and the literature. The aim of this study is to show, that the wireless sensor s are a benefit in planning as well
as during the execution of the therapy. Therefore different assumptions were verified. Additionally, a survey
about the acceptance and the benefit of the sensors was made. Ten test persons performed a laterality test
and the sensorimotor training on three different exercisers. During the whole training the muscle activity as
well as the motion data was document by the usage of wireless sensors. Immediately after the training, all
test persons fulfilled the survey. The study revealed that is important to investigate the training in more detail.
Nevertheless, most assumptions are seen as basic principles, they could not be verified. The evaluation of the
surveys figured out, that the usage of wireless sensors can be seen as an advantage, but the application has to
be optimized.
1 INTRODUCTION
Use of evidence based decision making is promoted
across the different professions along the health care
system. Based on multiple issues, the use of evidence
has become extensively attractive. One of these issues
is the documentation of the great diversity of treat-
ment methods in the management of a variety of dif-
ferent conditions. Additionally, the handling of medi-
cal errors as well as the identification of trends in tech-
nology assessment (Jewell, 2010).
The current status of the therapy planning mainly
rests upon theoretical knowledge, observations just
like “trial and error”. The establishment of a special
therapy was supported by the development and dis-
semination by a respected authority (Mangold, 2012).
One treatment, which is established in the preven-
tion, the therapy, the rehabilitation as well as in the
improvement of the athletic performance is the senso-
rimotor training (H
¨
afelinger and Schuba, 2010). In-
duced by the variety of application fields the training
itself is going to become more and more attractive.
Consequently, the availability of, particularly, special-
ized equipment is steadily increasing. In contrast, the
impact of the training on the body is not yet fully in-
vestigated (R
¨
uhl and Laubach, 2012).
The positive benefit of the training depends on the
correct application of the equipment. Due to the dif-
ferent materials, functions and characteristics of the
exercisers the correct usage might be challenging. In
particular, the therapy planning is still quite incom-
pletely investigated. Hence, the training is based
on the experiences of the individual physiotherapist
and additionally by the given background informa-
tion of the literature as well on the manufacturer’s
data regarding the exercisers characteristics (R
¨
uhl and
Laubach, 2012).
The myofascial chains is one method of treatment
which is often mentioned in the literature. Kabat has
developed a method to integrate weakened muscles
in a special muscle chain to optimize their behav-
ior during the execution of certain motion patterns.
However, this chains cause the activation of the pro-
prioceptive capabilities of the musculoskeletal system
and leads to the strengthening of the weakened mus-
cles. Several different methods derive from the my-
ofascial chains from Kabat. For instance the holistic
model of all muscles chains by Struyff-Denys. The
500
Thiers A., l’Orteye A., Orlowski K. and Schrader T..
Technology in Physical Therapy - Wireless Sensors and the Sensorimotor Training.
DOI: 10.5220/0004913405000505
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 500-505
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
aim of the application of the principle of the myofas-
cial/ muscles chains is to adopt the behavior of mo-
tion from everyday life as well as from sports into the
therapy process. Consequently, up to date the princi-
ple of the myofascial/ muscle chains is still integrated
in the physiotherapists working process (Richter and
Hebgen, 2007; Tittel, 2012).
Next to the literature of basic principles of the
therapy, a highly important role in the planning of
the treatment is played by the manufacturer’s in-
formation about the exercisers. One popular exer-
ciser is the “Balance Board”. It’s responsibilities in-
clude the strengthen of the musculature of the but-
tocks, the legs, the back and the abdomen (Sport-
Thieme, 2012). Consequently, the following effects
were attributed to the training on the Balance Board.
Firstly, the improvement of the inter- and intramuscu-
lar coordination of the muscles of the feet, the legs,
the lumbar spine, the thoracic spine and the cervical
spine. Secondly, staying with both feed on the Bal-
ance Board, should cause the enhancement of the sta-
bilization in the region of the lumbar spine, the pelvis
and the hip (Bertram and Laube, 2008).
The aim of the current study was to show that there
is a positive benefit when wireless sensors were used
in the sensorimotor training. The usage will lead to
an evidence based therapy planing. Furthermore, the
effects of the training on the body were investigated
in more detail. The research documented the training
of ten subjects of three different exercisers. Addition-
ally, test regarding the laterality were made was well
as inquiries concerning the acceptance of the mea-
surements.
2 MATERIAL & METHODS
2.1 Measurements
The Shimmer
TM
measurements are small and wire-
less sensors. The usage of the Bluetooth technology
allows for online data streaming in real-time (Shim-
mer Research, 2011).
The EMG (Electromyography) daughterboard
provides pre-amplification of the EMG-Signal. The
non-invasive method represents the whole activity of
a muscle using either two or three channel data acqui-
sition (Shimmer Research Support, 2012).
The gyroscope module records the angular veloc-
ity of three axis. It consists of a single as well as of a
dual axis angular rate gyroscope (Kuris, 2010).
2.2 Exercisers
For the evaluation of the sensorimotor training the be-
havior of the subjects were documented on three dif-
ferent exercisers.
2.2.1 Balance Board
The Balance Board is an exerciser with a multidimen-
sional instability, figure 1. Its top is made of stable
and reinforced plastic with a diameter of 40 cm. The
height of the board is 9 cm. The aim of the train-
ing on the Balance Board is in general to strengthen
the musculature of buttocks, legs, back and abdomen
(Sport-Thieme, 2012).
Figure 1: Balance Board.
2.2.2 Rocker Board
One characteristic of the Rocker Board is its one-
dimensional instability, figure 2. Again, there is a di-
ameter of 40 cm, but in this case a height of 7.5 cm.
The aim of the Rocker Board is to train the coordi-
nation, the stamina, the strength as well as the mo-
tor skills. The Board is either used with a forward-
backward or a left-right deflection (Bad-Company,
2013).
Figure 2: Rocker Board.
2.3 Experimental Setup
Supporting the objectives to develop a useroriented
experimental setup and to generate a test procedure,
which can also be executed in patients therapy, the
design of the study was made in cooperation with ex-
perienced physiotherapists of a medical school.
The aim of the study is on the one hand to inves-
tigate the sensorimotor training and on the other hand
to show the benefit of the usage of wireless sensors
in the physiotherapy, especially in the sensorimotor
training. To have a more detailed look at the sensori-
motor training different questions were analyzed:
TechnologyinPhysicalTherapy-WirelessSensorsandtheSensorimotorTraining
501

• Verification of the principle of the myofascial/
muscle chains
• Verification of the manufacturer’s data
• Verification of the the given information by
the literature, for example exercisers with one-
dimensional instability are easier to handle
than exercisers with multidimensional instability
(Grifka and Dullien, 2008)
• Verification of the correlation of laterality and be-
havior on the exercisers
• Acceptance of the measurement units
The study involved ten young and healthy subjects
(seven male and three female). They gave their writ-
ten consent to participate after being informed about
the test procedure. They perform a special test proce-
dure on each of the three exercisers. Furthermore, a
test for the laterality of the hands as well as of the feet
were made. Additionally, a questionnaire about the
acceptance of the wireless sensors had to be fulfilled
by the subjects.
2.3.1 Exerciser-tests
The development of the tests sequences on the ex-
erciser derived from a previous study (Thiers et al.,
2013b; Thiers et al., 2013a).
The measurements on the exercisers requires the
use of two different types of Shimmer
TM
sensors.
The two gyroscope sensors were places centrally on
each exerciser. To verify the different assumption of
the manufacturers and the literature the EMG sen-
sors were placed down the legs. In detail: M. bi-
ceps femoris, M. vastus lateralis, M. tibialis anterior
and M. soleus. Both, the skin preparation as well as
the placement of the Ag/AgCl electrodes follows the
recommendations of the SENIAM Project (SENIAM
project, 2012).
One test sequence comprised of a reference mea-
surement in front of the equipment and the record-
ing on the exerciser. The test sequence had to be per-
formed for each of the three exercisers and the order
of the training equipment was randomized for each
test person. The measurement on the exerciser was
divided into four consecutive phases of changing dif-
ficulty and duration, table 1. Another characteristic of
the test procedure was the symmetrical requirement
to both body sides. All recordings have been done
without shoes and were supervised by an experienced
physiotherapist.
2.3.2 Laterality-test
The outcome of previous studies had shown that there
is a dominance body side (Thiers et al., 2013b; Thiers
Table 1: Test procedure.
Phase Task Duration
1 Eyes open 30 s
2 Eyes closed 30 s
3 Throwing a medicine ball 60 s
4 Eyes open 30 s
et al., 2013a). Next to the handedness the phenom-
ena of the laterality is also relevant for other paired
parts of the body (Weineck, 2004). To establish a link
between the laterality and the measured values differ-
ent test were made. On the one hand the handedness
was tested. Additionally, the laterality of the feet was
checked, too.
On the whole, six tests for the handedness and ten
test for the laterality of the feet were made. For a gen-
eral overview a balance test was made, too. Therefore
the subject had to stand on two scales, with each foot
on one scale.
2.3.3 Surveys
To determine the acceptance of the measurement units
a questionnaire was developed. Concerning the con-
tents of restrictions during the execution of the trials
when wearing the sensors, the benefit of the sensors
as well as the transferability of the technology into
physiotherapists everyday life.
The surveys were fulfilled by prospective physio-
therapists and students of medical informatics.
2.4 Data Analyzes
The data analyzes process started with the application
of a notch filter. Additionally, a band-pass filter was
used (Merletti and Parker, 2004). Afterwards, the nor-
malization of the EMG data took place. Therefore,
the average muscular activity, when staying in front
of the exerciser, was calculated and used as normal-
ization value. Hence, the absolute values were trans-
formed into relative values by using the data of the
reference measurement and were presented percent-
age values of the stance.
Next to the normalization a full-wave rectifica-
tion of the EMG data was made (Merletti and Parker,
2004). To evaluate the recordings in the time domain,
different statistical values were computed as interim
results. Both, the mean as well as the maximum val-
ues were computed over a time window of 512 ms
for the whole signal (Gu et al., 2010). Subsequently,
the course of the maximum values over time was cal-
culated. Furthermore, the mean value of the max-
imum voltage values for each phase as well as for
the complete procedure were computed. In addition
HEALTHINF2014-InternationalConferenceonHealthInformatics
502
to the previous parameters the accumulated EMG ac-
tivity (iEMG) was evaluated, too. Firstly, the EMG
was integrated over time. The next step comprised of
the calculation of the area under the EMG for a cho-
sen time period, also known as iEMG (Robertson and
Caldwell, 2004; Medved, 2000). This procedure was
performed on the one hand for each phase and on the
other hand for the complete test procedure. Further-
more, the course of the iEMG was documented for
the whole over time by the summation of the iEMG
during the execution of the exercises.
As a complementary evaluation to the physiologi-
cal data, the motion data was also analyzed. The gy-
roscope data was low-pass filtered and then the direc-
tion of motion as well as the current deflection was
computed.
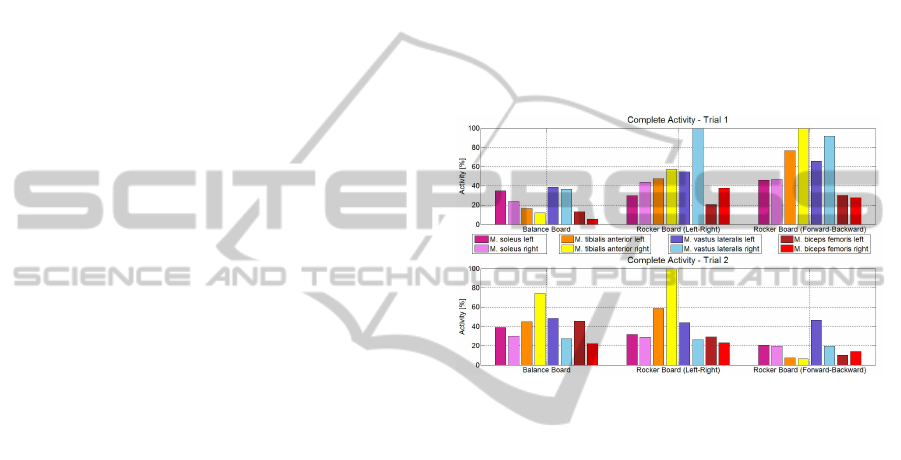
3 RESULTS
The illustration 3 provides a brief overview of the
complete muscular activity of each muscle on each
exerciser for one test person, a left-hander, during two
different trials. After the first execution a short feed-
back was given to the test persons. A few weeks later
the test persons have repeated the whole experimental
trial.
The muscle with the highest strain during each
trial represents the 100 %. The values of the remain-
ing muscles were presented in relation to the 100 %.
The subject achieved the highest values during
trial one with the right M. vastus lateralis as well as
with the right M. tibialis anterior. The highest over-
all strain is documented for the forward-backward
Rocker Board. In contrast, the training on the Balance
Board seems to be the lowest challenge for the sub-
ject. Except the Balance Board, the right body side
is always providing the highest EMG values. Trial
one figures out the following points: the training on
the exercisers with the one-dimensional instability re-
quired higher EMG activity than the training on the
exerciser with the multidimensional instability. Al-
though, the subject is a left-hander and the laterality
test of the feet shows that in eight out of ten tests the
preferred leg is the left one, mainly the right body side
was dominant. The M. biceps femoris achieved com-
paratively low EMG activity, this reflects a contrast
to the assumption of the myofascial/ muscles chains.
In detail, the expected muscle behavior following the
theory of the chains of the supporting and the free leg
was not documented (Tittel, 2012).
After the execution of the first trial the test persons
received a feedback to there individual performance
on the exercisers. With a delay of a few weeks the
experimental setup was repeated. The documented
values were illustrated in the lower part of figure 3.
The major outcome is the new sorting of the EMG ac-
tivity values of the single muscles, which also leads
to different levels of difficulty of the exercisers in
comparison to the first trail. In this case, the highest
muscle strain is achieved by the right M. tibialis ante-
rior on the left-right Rocker Board. Furthermore, the
EMG values document, that the forward-backward
Rocker Board represents the smallest challenge. An-
other change is shown in the dominance of the right
body side. The second trial documents an increased
occurrence of higher voltage values of the left body
side.
Figure 3: Comparison of two trials of one subject.
The current figure 4 visualizes the average maximum
voltage values for each muscle when the subject used
the Balance Board.
One finding of the figure is, that for all muscles the
lowest values were achieved during the initial phase.
Consequently, this indicates that a slow relaxation
took place because the first and final phase require an
identical task.
A second finding is that the highest values were al-
ways achieved by the M. tibialis anterior. Partially the
remaining muscles only had produced voltage values,
which are similar to that during the reference mea-
surement in front of the Balance Board. This obser-
vation speaks against the principle of the myofascial/
muscle chains, again. Additionally, the documented
values do not support the manufacturers information.
The main part for the maintenance of the equilibrium
on the Balance Board is done by the M. tibialis an-
terior. Already the musculature of the thigh is only
slightly involved.
Another outcome of figure 4 is that in most cases
the higher voltage values were achieved by the mus-
culature of the right body side. Both, the test of the
laterality of the handy as well as the test of the feet re-
sult in the dominance of the right side (hand-six out of
six right dominance, feet- eight out of ten right dom-
TechnologyinPhysicalTherapy-WirelessSensorsandtheSensorimotorTraining
503

inance). Whereas the balance test on the scales docu-
mented a state of equilibrium (29 kg - 30 kg).
Figure 4: Average maximum values: Balance Board.
Figure 5 documents the results of a set of ques-
tions from the survey. Immediately after the execu-
tion of the experimental setup the questionnaires were
fulfilled.
The first question was about the restrictions during
the training when wearing the sensors. No one of the
ten test persons had documented to feel any restric-
tion. Next to the small form factor of the sensors the
material for the fixation of the measurements is very
important for freedom of movement.
The next question addressed the problem of the
personal feeling when wearing the sensors. The sub-
jects had to decide whether they feel unpleasant or
not. Only one person had reported to feel uncomfort-
able. This was justified in the temporarily strong fix-
ation of the sensors, which was afterwards optimized.
The third question handled the benefit of the sen-
sors. All test persons have reported to see a benefit of
the usage of the sensors. On the one hand the subjects
documented that one benefit is to see the muscular
activity and to get a feedback. On the other hand the
subjects see the opportunity to get objective results
about the current state of the therapy.
The last discussion point was the transferability
of the sensors into the physiotherapists everyday life.
Nine out of ten test persons thought, that it is possible
to use the wireless sensors in the practice. Neverthe-
less, often one point of criticism was mentioned. The
application of the electrodes had needed a high de-
mand on time. For an effective usage this application
has to be optimized.
4 DISCUSSION
The main finding in this experimental study is that
wireless sensors can support the sensorimotor train-
ing. On of the most common principles among phys-
iotherapists experts is the method of the myofascial/
Figure 5: Acceptance and benefit of wireless sensors.
muscles chains. Often the therapy planing is based
on this knowledge. However, the EMG patterns of
the two subjects have shown that against the expecta-
tions, already the ischiocrural musculature only has
a limited participation in the sensorimotor training.
This observation was confirmed by the EMG values
of the remaining test persons, too.
Additionally, the statements of the manufacturer‘s
about their products were validated. Again, this as-
sumption could not be verified. For the character-
ization of an exerciser more detailed information is
needed, for example about its consistency as well as
of its inertia.
One assumption about the therapy planning is, that
the training on an exerciser like the Rocker Board,
which has a one-dimensional instability is easier than
on an exerciser with a multidimensional instability.
The principle behind: the higher the instability the
more the musculature has to stabilize (Grifka and
Dullien, 2008). The comparison of the needed EMG
activity on the individual exercisers has shown, that
the Rocker Board is always requiring the higher par-
ticipation of the muscles. This observation was made
for all of the ten test persons.
Previous studies (Thiers et al., 2013b; Thiers et al.,
2013a) have shown, that there is frequently a domi-
nance of one body side regarding the produced volt-
age values. The analyzes of the motion data has
shown, that there is no correlation to the duration
of the deflection to one side. Mostly the deflection
values have shown that there is a uniform distribu-
tion regarding the duration of the individual direc-
tions. Hence, there is the assumption, that there is
a correlation to the laterality of the subject. Often
after the laterality-test there was the recognition that
no clear assumption concerning the dominance of the
legs could be taken. Nevertheless, the test persons
mostly have shown a preferred side. This was also
reflected by the EMG values. The ambiguity could
maybe caused by the specialization of the test persons
HEALTHINF2014-InternationalConferenceonHealthInformatics
504

in different sports.
The survey figured out, that the subjects have seen
a benefit in the usage of wireless sensors in the sen-
sorimotor training. Although, they have critical look
at the transferability into everyday life. Therefore, it
is needed to perform different improvements to opti-
mize the time exposure.
5 CONCLUSIONS
The investigation of the sensorimotor training reveals
that a more detailed look at the therapy planning is
needed. In the current study each test person has
shown different EMG patterns. Consequently, it is
not possible to make general assumptions about the
effects of the exercisers. For an effective usage of the
equipment a personal analyze of the behavior of the
muscles is needed. Therefore the usage of wireless
sensors is a benefit.
Furthermore, the correct application of the equip-
ment would be supported, if the manufactures pub-
lish more information about their exercisers. Data like
the diameter or the height of an exerciser are too gen-
eral to draw reliable conclusions about the effects the
equipment would cause in the training.
All test persons have shown a dominance of one
body side. This observation was invisible to the naked
eye. Using EMG sensors enables physiotherapist to
an objective assessment of the muscle behavior and
to adapt the training to the individual performance of
the patient.
The great diversity of the voltage values of the
muscles of one test person within two trials makes
clear that the behavior of the subject is mainly based
on its individual form of the day. To handle this chal-
lenge the usage of wireless sensor as a real time feed-
back would be possible.
The variety of different EMG patterns of the in-
dividual subjects as well as the differences in the be-
havior of one test person within two trials shows the
necessity of an evidence based treatment in the ther-
apy. This evidence based approach could be realized
by the usage of wireless sensors.
REFERENCES
Bad-Company (2013). Deluxe balance board set 45cm aus
holz in studio-qualit
¨
at. Website. Available online
at http://www.webcitation.org/6Fg4kjCXJ; visited on
April 6th 2013.
Bertram, A. M. and Laube, W. (2008). Sensomotorische Ko-
ordination: Gleichgewichtstraining auf dem Kreisel.
Thieme.
Grifka, J. and Dullien, S. (2008). Knie und Sport:
Empfehlungen von Sportarten aus orthop
¨
adischer
und sportwissenschaftlicher Sicht. Deutscher Arzte-
Verlag.
Gu, Y., Li, J., Ruan, G., Wang, Y., Lake, M., and Ren,
X. (2010). Lower limb muscles semg activity dur-
ing high-heeled latin dancing. In Lim, C. and Goh, J.,
editors, IFMBE Proceedings. Springer.
H
¨
afelinger, U. and Schuba, V. (2010). Koordinationsthera-
pie: Propriozeptives Training. Meyer & Meyer Ver-
lag.
Jewell, D. V. (2010). Guide To Evidence-Based Physical
Therapist Practice. Jones & Bartlett Learning.
Kuris, B. (2010). Kinematics Guide Revision 1e. Shimmer
Research.
Mangold, S. (2012). Evidenzbasiertes Arbeiten in der
Physio- und Ergotherapie: Reflektiert - Systematisch
- Wissenschaftlich fundiert. Springer.
Medved, V. (2000). Measurement of Human Locomotion.
CRC Press.
Merletti, R. and Parker, P. A. (2004). Electromyography.
John Wiley & Sons.
Richter, P. and Hebgen, E. (2007). Triggerpunkte
und Muskelfunktionsketten in der Osteopathie und
manuellen Therapie. Hippokrates.
Robertson, D. G. E. R. and Caldwell, G. (2004). Research
Methods in Biomechanics. Human Kinetics.
R
¨
uhl, J. and Laubach, V. (2012). Funktionelles Zirkel-
training: Das moderne Sensomotoriktraining f
¨
ur alle.
Meyer & Meyer Verlag.
SENIAM project (2012). Sensor placement. Website.
Available online at http://www.seniam.org; visited on
October 25th 2012.
Shimmer Research (2011). Shimmer-brochure-pack. Tech-
nical report.
Shimmer Research Support (2012). EMG User Guide Rev
1.2. Shimmer Research.
Sport-Thieme (2012). Sport-thieme
R
sport- und ther-
apiekreisel. Website. Available online at
http://www.webcitation.org/6BgicOk7Y; visited on
October 25th 2012.
Thiers, A., l’Orteye, A., Orlowski, K., and Schrader,
T. (2013a). Analyse der muskul
¨
aren stabilisation
w
¨
ahrend des sensomotorischen trainings bei verwen-
dung von ger
¨
aten mit ein- und mehrdimensionaler in-
stabilit
¨
at mit hilfe von drahtlosen sensoren. GMDS
2013 58. Jahrestagung der Deutschen Gesellschaft f
¨
ur
Medizinische Informatik, Biometrie und Epidemiolo-
gie (GMDS) e.V.
Thiers, A., l’Orteye, A., Orlowski, K., and Schrader, T.
(2013b). Investigation of the sensorimotor training
analyzing exercisers with one-dimensional and mul-
tidimensional instability. icSports 2013.
Tittel, K. (2012). Beschreibende und funktionelle Anatomie.
Kiener.
Weineck, J. (2004). Optimales Training. Spitta Verlag
GmbH & Co.
TechnologyinPhysicalTherapy-WirelessSensorsandtheSensorimotorTraining
505
