
Forceplates Data Reliability Tested on Children with Neuromuscular
Disabilities
Sarah Rosen
1,2
, Carole A. Tucker
3
and Rahamim Seliktar
1
1
School of Biomedical Engineering, Science and Health Systems, Drexel University,
3141 Chestnut Street, Philadelphia, PA, U.S.A.
2
Shriners Hospitals for Children, 3551 North Broad Street, Philadelphia, PA, U.S.A.
3
Department of Physical Therapy, Temple University, 3307 North Broad Street, Philadelphia, PA, U.S.A.
Keywords: Gait Forces, Gait Cycle, Gait Impulse, Gait Consistency, Pediatric Gait.
Abstract: The “gait cycle” is considered the fundamental repetitive element of locomotion and is often used in
comparative analyses between pathological and normal gait. One device that is used to measure ground
reaction forces in the gait laboratory is a six degrees of freedom force transducer (“Force Plate”). Gait labs
use two or more force plates to measure forces during one or two complete strides. Often, the walker “aims”
to step sequentially on the force plates. This aiming may cause significant distortion of the person’s gait
pattern. To validate the measured result as representative of the individual’s gait, a “Gait Consistency Test”
was developed by Seliktar et.al with a group of adult individuals. The present study employed the
consistency test to the ground reaction force records of two groups of children; typically developing
children and children with cerebral palsy. The children’s gait consistency study yielded even better results
than the adult study; the results showed that the consistency test is useful for screening children’s gait data
and should be used to ensure higher fidelity of the measured data. The test applied equally to normally
developing children and to children with gait pathologies.
1 INTRODUCTION
The hypothesis that is being tested in this work is: Is
it legitimate to assume that human being ambulate
by performing repetitive patterns (rhythm) of
movement, often referred to as “Gait Cycles?” These
cycles, if exist, should apply equally to normal gait
as well as pathological gait. If such rhythm does not
exist, then the term “Gait Cycle” is invalidated and
would not be appropriate to be used in comparative
gait analysis.
3D human motion analysis relies on the use of
dynamic data acquired with the aid of motion
tracking and ground reaction forces measurement
instruments. The usefulness of the raw data
characteristics themselves is often apparent in
detection of gait abnormalities. The processing of
the force and motion data to yield joint forces,
moments and power during gait, further enhances its
utility (Gage 2004). The relative simplicity of the
ground reaction forces (GRF) characteristics makes
them attractive as a clinical assessment tool, as
opposed to the abundance of the kinematic data.
Moreover, the joint moment information derived
directly from these forces, further enhance the utility
of these data in understanding the “human gait
engine.”
Considering the importance of the ground
reactions as the main driving force of the overall
human mechanism little has been done to address
the validity and consistency of the measured GRF
data during gait. The awareness of the shortcomings
of the force plates as the primary available
instrument, has led people to develop devices for
continuous measurements of the ground forces.
Nevertheless, all the new developments were
restricted to measurement of the vertical component
only. Seliktar et al. (Seliktar, Yekutiel, Bar 1979)
developed a “Gait Consistency Test” to determine if
due to the person’s aiming towards the force plates
or due to any other environmental distractions, the
steady state nature (rhythm) of the measured gait is
distorted. The test was designed to ensure that the
velocity of the body center of mass is “the same”
(within certain variation limits) at any two
equivalent points of (at least) two consecutive
303
Rosen S., A. Tucker C. and Seliktar R..
Forceplates Data Reliability Tested on Children with Neuromuscular Disabilities.
DOI: 10.5220/0004934303030306
In Proceedings of the International Conference on Biomedical Electronics and Devices (TPDULL-2014), pages 303-306
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
cycles. The premise of the test was that the
velocities of the CM is governed by the ground
forces and hence the force-time integral (Impulse)
equals the difference in Momenta ∆ (the
Impulse-momentum theorem):
(1)
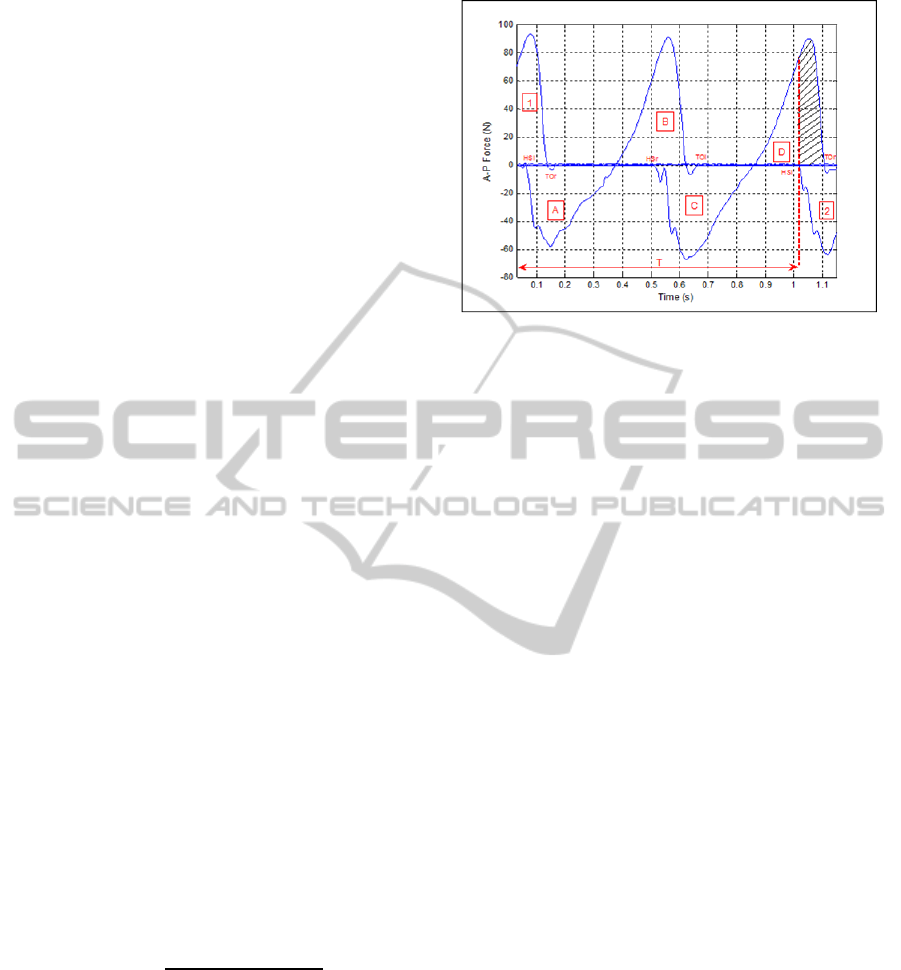
over a full cycle, should be zero, as illustrated in
Figure 1. Since the GRFs are vectors, the antero-
posterior (A-P) force component was selected as the
most adequate to be used for such validation of the
results.
According to Newton’s 2
nd
Law, for a system,
the ground reaction forces and the gravitational force
are driving the center of mass of the body;
∑
G
(2)
Since the impulse of the driving forces equals the
difference in mass times velocity, the force-time
integral between those two points, in rhythmic gait,
must be zero. Nevertheless, small variations between
cycles are expected and therefore absolute zero is
not a feasible expectation.
The decision to use the A-P component for
validation of the consistency is due to the authors’
observation that human gait is less cyclical in the
medio-lateral (M-L) and the measured vertical force
is inconvenient to use, because of the body weight
superposition. Moreover, because the A-P force is
responsible for the forward progression of the body
it is more likely to reflect deviations from rhythmic
steady state gait due to environmental biases.
Previously reported results of the study were
obtained from 28 adults with normal and
pathological gait. Consistency was defined as the
sum of the A-P impulse over one full gait cycle
divided by the absolute values of impulse for both
the braking and propulsion forces, Figure 1 and
Equation (2) describe the calculation:
%
|
|
|
|
|
|
|
|
(3)
When looking at Figure 1 and Equation (3) it is clear
that the contribution of impulse 1; the impulse of the
right foot from the time of the left foot heel strike to
when the right foot toes off, is not accounted for in
the calculation.
This is because only 2 force plates were available
and the assumption made was that the areas denoted
as 1 and the dashed part of area D are almost
equivalent. The consistency threshold value was
determined to be 7.3% meaning that values greater
than 7.3% for the gait cycle would be considered
Figure 1: The GRFs in the A-P direction during two force
plate strikes of an able bodied individual. HS stands for
heel strike and TO for toe off. ‘l’ and ‘r’ stand for the left
and right sides. T represents the time of duration of the
gait cycle.As depicted in the illustration of figure (1),
consistency was calculated over two force plate strikes, for
both legs, left and right.
inconsistent and should be removed from further
analyses. Clinical gait analysis is commonly
performed in children with cerebral palsy (CP), and
even though the GRF data is typically relatively
underutilized in comparison to kinematic data it can
provide a useful tool for ensuring the data used is
representative. Currently the method used for
ensuring representability is by averaging a number,
usually three, trials of gait analysis. In the current
study, the above approach was applied to three
groups of children: typically developed children
(TD), children with diplegic CP (DCP) and children
with hemiplegic CP (HCP) to determine the utility
of the gait consistency test.
2 METHODS
Subjects: Retrospective data from a sample of 53
ambulatory children who underwent gait analysis
testing at Shriners Hospital for Children (SHC) –
Philadelphia, Motion Analysis Laboratory from
2001-2006 was used in this analysis. The first group,
TD, consisted of 8 males and 8 females, 7-17 years
of age (Mean=11.2, SD= ±2.1). The second group,
DCP), consisted of 8 males and 8 females, 9-17
years of age (Mean=12.5, SD= ±2.0). The third
group, HCP, with left (n=8) or right (n=13) sides
affected, consisted of 10 males and 11 females, 10-
17 years of age (Mean=12.9, SD= ±2.3). The
analysis included 2 walking trials for each subject
and an average of 2 gait cycles per trial.
Data Collection: Data were obtained from
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
304
motion analysis database and report reviews. Data
were only included for children with CP who did not
use assistive devices during ambulation, and
completed two trials during which consecutive gait
cycles for each of the four force plates was
available.Only trials during which only a single foot
landed on each of the force plates was deemed
acceptable (e.g. trials during which 2 feet or more
landed on a single force plate were discarded). This
retrospective data used in this study was collected
during gait analysis utilizing motion capture and
force plate data collection during level ground
ambulation. The Motion Analysis Laboratory at
SHC–Philadelphia is equipped with an 8-camera
MX-Vicon motion capture system (Vicon Motion
systems, Lake Forest, CA) and 4 AMTI force plates
(Advanced Mechanical Technology Inc.,
Watertown, MA). Analog force plate data were
synchronized and collected through the Vicon
system software. Each subject wore shorts and a T-
shirt throughout the evaluation and gait analysis was
performed with the subject walking barefooted and
walking at his/her freely chosen walking speed along
an 8.4-meter level walkway. Force data were
collected when the subject traversed the middle 5
meters.
Data Analysis: Force plate data in the A-P
direction that had been collected at 1200Hz
sampling rate, was extracted from the Vicon’s c3d
files and imported into Matlab 7.1 (The Mathworks
Inc. Natick MA) for further analysis. A custom-
written Matlab program was used to calculate gait
consistency, as defined in Equation (2). A one-way
ANOVA test was used to determine significant
differences in the consistency values between the
three populations (Portney & Watkins 2009).
3 RESULTS
Data extraction resulted in a total of 2 trials for each
of the 53 subjects. The ANOVA test revealed the
values for the three populations were not
significantly different (F=1.18, p=0.31). An average
consistency value was calculated for the three
populations separately, and for the entire population
as a whole. Results for the pediatric population
demonstrate that children can consistently ambulate
within a motion analysis laboratory setting. The
consistency test values can be found in Table 1 and
Figure 2. These results were extremely close to the
findings of Seliktar et al. (Seliktar, Yekutiel, Bar
1979) and show consistency is achieved with a ratio
below 6.33%.
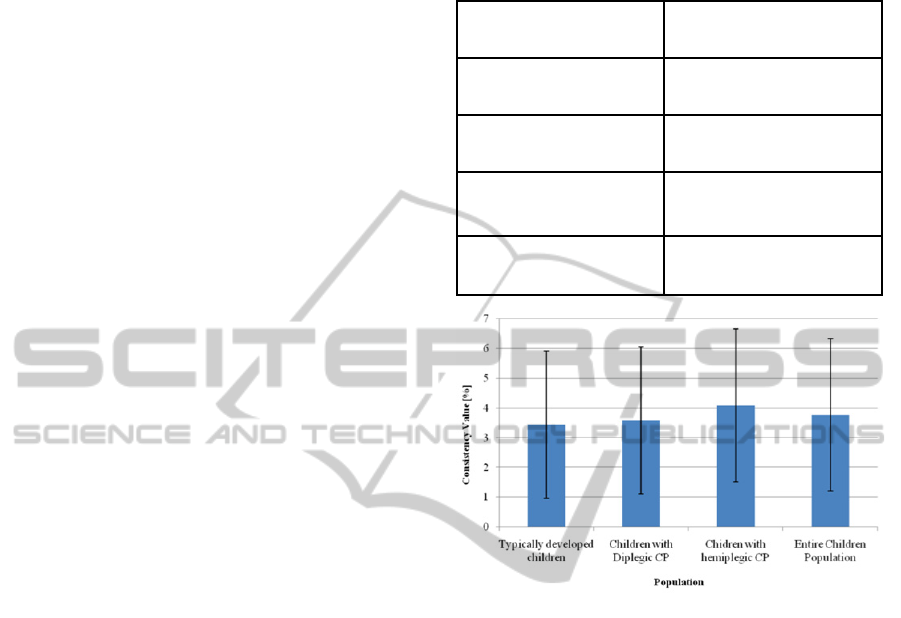
Table 1: Results of the consistency test for typically
developed children, children with diplegic CP and children
with hemiparetic CP.
Population
Average Consistency
value [%]
Children with Typical
Development
3.44 ± 2.48
Children with Diplegic
CP
3.59 ± 2.47
Children with
Hemiparetic CP
4.09 ± 2.58
Entire population with
no regards to condition
3.77 ± 2.56
Figure 2: Results of the consistency test for typically
developed children and children with diplegic and
hemiplegic CP. Results are presented as the mean with the
standard deviation.
4 CONCLUSIONS
The results of the study support the application of a
gait consistency test to children with typical
development and with CP. Our findings are
consistent with those found by Seliktar (Seliktar,
Yekutiel, Bar 1979) supports the definition of an
inconsistent gait in children to be one in which the
consistency value is above 6.33%. Given no
significant differences in the consistency values for
each of the three populations, it appears gait
consistency is not dependent on the presence, or
absence, of pathological conditions. The consistency
test reflects ambulation at a constant speed of
progression (velocity averaged per cycle), and many
gait parameters are affected by gait velocity – or
relative changes in gait velocity over consecutive
cycles (e.g. speeding up or slowing down during gait
analysis trials). The application of such a
ForceplatesDataReliabilityTestedonChildrenwithNeuromuscularDisabilities
305

consistency test to ensure gait trials are compared
across steady state trials, this measure provides a
simple means to assess whether a specific gait cycle,
chosen for analysis is in fact a representative gait of
the child.
ACKNOWLEDGEMENTS
The authors would like to thank the staff at Shriners
Hospitals for Children - Philadelphia Motion
Analysis Laboratory for its assistance in this study
and the support obtained from the Calhoun
Fellowship Fund of the School of Biomedical
Engineering Science and Health Systems at Drexel
University.
REFERENCES
Gage, James R. The Treatment of Gait Problems in
Cerebral Palsy. London: Mac Keith, 2004. Print.
Portney, Leslie Gross., and Mary P. Watkins. Foundations
of Clinical Research: Applications to Practice. Upper
Saddle River, NJ: Pearson/Prentice Hall, 2009. Print.
Seliktar, R., Yekutiel, M., Bar A. (1979). Gait Consistency
Test Based on the Impulse-Momentum Theorem.
Prosthet Orthot Int. 3 (2), 91-98.
Winter, David A. Biomechanics and Motor Control of
Human Movement. Hoboken, NJ: Wiley, 2009. Print.
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
306
