
Knowledge Management Concepts and Processes in Healthcare
Research Plan for Doctoral Thesis
Helvi Nyerwanire
1
, Erja Mustonen-Ollila
1
, Antti Valpas
2
and Jukka Heikkonen
3
1
Department of Software Engineering and Information Management, Lappeenranta University of Technology,
Lappeenranta, Finland
2
Department of Obstetrics and Gynaecology, South Karelia Social and Health Care District, South Karelia, Finland
3
European Commission Joint Research Centre, Unit JRC.G1 Scientific Support to Financial Analysis, Ispra, Italy
1 STAGE OF THE RESEARCH
This study presents a research plan for a doctoral
thesis about Knowledge Management in Healthcare.
It outlines objectives, research problems, state of the
art, methodology and expected outcome. The study
introduces current knowledge management concepts,
the research questions, and a conceptual framework
of knowledge management processes. It also
outlines data collection methods and data analyzing
methods. In this study both qualitative analyzing
methods with the grounded theory approach and
quantitative data analysis with novel intelligent
computing and analyzing methods are applied.
This doctoral study is planned to take a total of
five (5) years (January 2012- January 2017) in
which the output will be five (5) conference articles,
and one journal article. Furthermore, a relevant
introductory section of the thesis will be written in
this period. One conference article has been
accepted in 2012, another conference article was
submitted for reviewing purpose in 2014, and one
journal article is in preparation.
2 OUTLINE OF OBJECTIVES
It has been claimed that knowledge is
conceptualized from different disciplines
(Hernández and Noruzi, 2010). For instance
accountants measure it on the balance sheet;
information technologists want to codify it on
systems; sociologists want to balance power with it;
psychologists want to develop minds because of it;
human resource managers calculate a return of
investment on it; and training and development
officers want to make sure that they can build it. An
individual can decide on where and when to apply
knowledge in order to get the best results
(Hernández and Noruzi, 2010). Among health care
practitioners, knowledge is captured in social
interaction, e.g. when physicians and nurses meet
patients. Physicians transfer their knowledge and
expertise in meetings and consultations sessions, and
they can express and interpret diagnosis reports,
create new expert knowledge by reading, by learning
in traineeship, and having discussions (Nonaka,
1994; Alavi and Leidner, 2001). Collective
knowledge exists in networks in organizations, and
knowledge is internally ingrained in people (Alavi
and Leidner, 2001), and people learn in the practice
community through participation with each other,
e.g. cardiologists can belong to a community of
practice transferring and receiving knowledge on
best practices (Grover and Davenport, 2001).
In this study, the primary objectives and goals
are to discover and conceptualize knowledge
management concepts and processes in healthcare,
specifically in a hospital environment, by combining
information systems science, knowledge
management science, medical science, nursing
science, sociology of knowledge, management
science, and computational intelligence (Polanyi,
1966; Nonaka, 1994; Nonaka and Takeuchi, 1995;
Nonaka and Konno, 1998; Alavi and Leidner, 2001;
Dalkir, 2005; Mustonen-Ollila, 2005; Raitoharju et
al., 2007; Oinas-Kukkonen et al., 2008; Mustonen-
Ollila and Heikkonen, 2008a, 2008b, 2009; Oinas-
Kukkonen et al., 2009; Lahtiranta, 2009; Koskinen,
2010; Greig et al., 2012).
3 RESEARCH PROBLEM
The research problems, research question (RQ) and
related studies and theories of knowledge
management processes are shown in Table 1 below.
Thus, the research questions (RQ) to be
answered are as follows. RQ1) How do nurses and
physicians acquire for new knowledge at the
3
Nyerwanire H., Mustonen-Ollila E., Valpas A. and Heikkonen J..
Knowledge Management Concepts and Processes in Healthcare - Research Plan for Doctoral Thesis.
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
Table 1: Knowledge management processes, research problems, research question (RQ) and related studies and related
theories.
Knowledge
management
processes
Research
problems
Research question (RQ) and related studies Related theories
Knowledge
acquisition (1)
Acquisition
mechanisms
RQ1) How do nurses and physicians acquire
for new knowledge at the research site?
(Huber, 1991; Mustonen-Ollila and
Heikkonen, 2003; Dalkir, 2005; Mustonen-
Ollila, 2005; Whelan et al., 2009)
Organizational learning (Dalkir, 2005;
Huber, 1991; Morr and Subercaze, 2010)
Knowledge
creation and
construction (2)
Social
construction
of
knowledge
RQ2a) How do nurses and physicians create
and construct knowledge at the research
site? (Huber, 1991; Nonaka, 1994; Alavi
and Leidner, 2001)
RQ2b) What impact has organizational
learning, unlearning and internal learning on
knowledge creation and construction at the
research site? (Hsiao and Chang, 2011)
Latour, 1991
Organizational learning (Huber, 1991; Morr
and Subercaze, 2010). Learning in
organizations (Ferriani et al., 2005; Morr
and Subercaze, 2010). Organizational
unlearning (Venable et al., 2010)
Knowledge
transfer (3)
Knowledge
transfer,
transfer
problems
RQ3a) How do nurses and physicians
transfer knowledge at the research site?
(Wang and Lu, 2010; Lauder et al., 1999;
Dalkir, 2005)
RQ3b) What are the knowledge transfer
problems at the research site? (Mustonen-
Ollila and Heikkonen, 2003; Morr and
Subercaze, 2010; Ferlie et al., 2012)
Knowledge sharing and communities of
practice (Dalkir, 2005; Eppler, 2007).
Learning and knowledge transfer (Lauder et
al., 1999; Wang and Lu, 2010; Morr and
Subercaze, 2010; Ferlie et al., 2012)
Knowledge
storage (4)
Knowledge
management
systems,
information,
data
RQ4) How do nurses and physicians store
knowledge at the research site? (Hanvanich
et al., 2006).
Organizational memory (Paoli and Prencipe,
2003).
Knowledge management processes and
management systems (Alavi and Leidner,
2001; Gold, 2001; Nonaka and Konno,
1998; Nonaka and Takeuchi, 1995)
Knowledge
application (5)
Application
mechanisms
RQ5) How do nurses and physicians apply
knowledge at the research site? (Huber,
1991; Dalkir, 2005; Morr and Subercaze,
2010)
Knowledge application (Huber, 1991;
Dalkir, 2005; Morr and Subercaze, 2010)
Organizational
learning,
unlearning and
internal
learning (6)
Learning
and
unlearning
mechanisms
RQ6) How do nurses and physicians learn
from existing knowledge and new
knowledge at the research site? (Hsiao and
Chang, 2011)
Organizational learning (Huber, 1991; Morr
and Subercaze, 2010). Learning in
organizations (Ferriani et al., 2005; Morr
and Subercaze, 2010). Organizational
unlearning (Venable et al., 2010)
research site? RQ2a) How do nurses and physicians
create and construct knowledge at the research site?
RQ2b) What impact has organizational learning,
unlearning and internal learning on knowledge
creation and construction at the research site? RQ3a)
How do nurses and physicians transfer knowledge at
the research site? RQ3b) What are the knowledge
transfer problems at the research site? RQ4) How do
nurses and physicians store knowledge at the
research site? RQ5) How do nurses and physicians
apply knowledge at the research site? RQ6) How do
nurses and physicians learn from existing knowledge
and new knowledge at the research site?
4 STATE OF THE ART
Different types of knowledge have been identified
and integrated into existing and emerging healthcare
information management practices (Alavi and
Leidner, 2001; Lahtiranta, 2009; Gold et al., 2001;
Nonaka and Konno, 1998). We have expanded Alavi
and Leidner’s study (2001) to cover new theoretical
knowledge concepts found in earlier research
(Nyerwanire and Mustonen-Ollila, 2012) (See Table
2).
First, clinical medical expert knowledge is
IC3K2014-DoctoralConsortium
4

bounded to physicians' medical knowledge and
expertise both in practice and theory (Iwai and
Ishino, 2009; Hill, 2010; Morr, 2010). Second,
collective knowledge means that organizations learn
from internal and external sources of organizations
and sub-networks (Morr, 2010). Finally, knowledge
is embedded in the members, tools, and tasks of the
organization (McGrath and Argote, 2000; Wegner,
1986) and the knowledge of these three sub-
networks and their combinations is important to find
out what kind of knowledge the organization, and in
our case especially the healthcare environment needs
to be able to accomplish their work properly.
Healthcare practitioners use their experience by
applying it in medical practice. Evidence-based
medicine is a form of organizational learning in the
knowledge management context (Morr and
Subercaze, 2010).
4.1 Conceptual Framework of
Knowledge Management Processes
Knowledge management processes are
conceptualized in Figure 1.
In Figure 1, the research context is the Central
Hospital of South Karelia Social and Healthcare
District, and the unit of analysis is a department or
several departments at the hospital. The processes in
Figure 1 are shown as ellipses with a number
ranging from 1 to 5 (knowledge acquisition,
knowledge creation and construction, knowledge
transfer, knowledge storage, and knowledge
application) or with dashed arrows (internal
learning, organizational learning, and organizational
unlearning).
Knowledge acquisition involves searching for
valuable knowledge, and external knowledge may be
acquired by importing knowledge components
directly or by depending on intermediaries (Huber,
1991; Mustonen-Ollila and Heikkonen, 2003;
Mustonen-Ollila, 2005). Whelan et al. (2009) argue
that an organizational gatekeeper is the key
individual who connects the organizational members
to the external sources of information, and the
organizational members are kept up-to-date with the
outside information by communicating with the
gatekeepers.
Learning influences knowledge creation, and
according to Oinas-Kukkonen et al. (2009),
knowledge provided by evidence-based medical
guidelines and drug information databases help
physicians to learn new things. Raitoharju et al.
(2007) state that an electronic patient record enables
creation of organizational knowledge, and it is a
useful tool to survive in everyday work in primary
care. According to Dalkir (2005), in decision-
making and clinical practice knowledge is
transferrable through individual learning for
example by observation (Hall and Walton, 2004). It
is also possible that knowledge transfer can occur
without the individual being aware of it happening
(Dalkir, 2005). Learning in groups occurs through
discussions, meetings and lecture sessions in which
people share their experiences (Dalkir, 2005).
Table 2: Knowledge concepts, definitions, examples, and past research.
Knowledge concepts Definitions Examples Past research
Clinical medical expert
knowledge
Knowledge dwells on the
healthcare practitioners’ medical
degree, skills and experience
Expertise on diagnosis of patient
needs
Iwai and Ishino, 2009;
Hill, 2010; Morr, 2010
Collective knowledge Knowledge exists in organizations
and their sub-networks
Organizational learning Morr, 2010
Member-member
network knowledge
Knowledge is embedded in
network members
Members are the human
components of the organization
McGrath and Argote,
2000
Task-task-network
knowledge
Knowledge is embedded in tasks Reflects the organization’s goals,
intentions and purposes
McGrath and Argote,
2000
Tool-tool network
knowledge
Knowledge is embedded in tools,
such as information systems
Tools are the technological
components (hardware, software,
and systems)
McGrath and Argote,
2000
Member-task network
knowledge
Knowledge about who knows
certain tasks
Members are allocated to certain
tasks
McGrath and Argote,
2000; Wegner, 1986
Member-tool network
knowledge
Knowledge about who knows
certain tools
Members are allocated to certain
tools
McGrath and Argote,
2000; Wegner, 1986
Member-task-tool
network knowledge
Knowledge about who knows
certain tasks with certain tools
Members are allocated to certain
tasks with certain tools
McGrath and Argote,
2000; Wegner, 1986
Task-tool network
knowledge
Knowledge about what tasks are
performed with what tools
Tasks are performed with certain
tools
Wegner, 1986
KnowledgeManagementConceptsandProcessesinHealthcare-ResearchPlanforDoctoralThesis
5
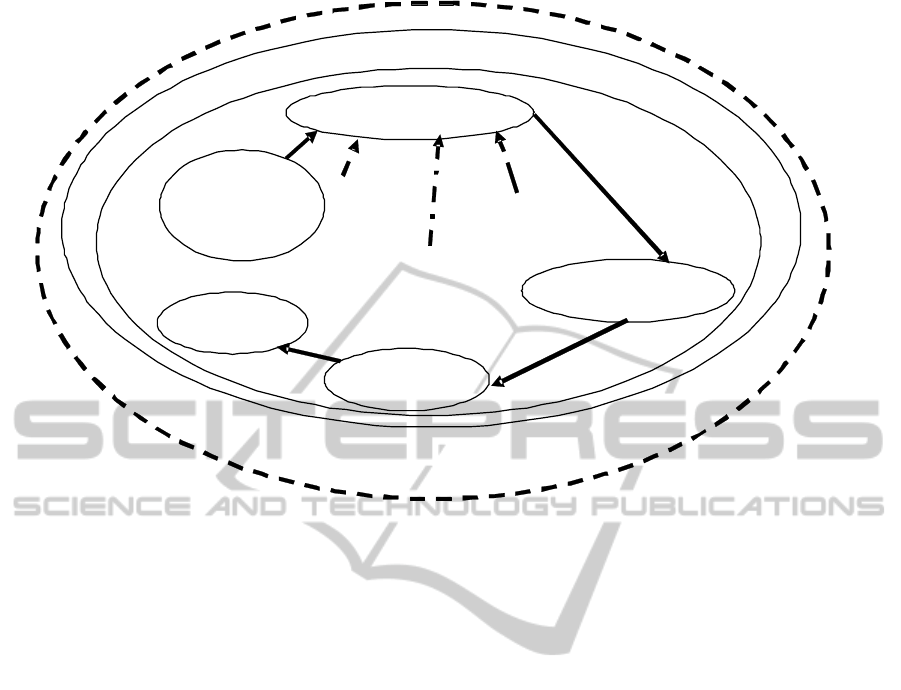
Figure 1: The conceptual framework of the study.
Lauder at al. (1999) state that knowledge transfer is
the ability to apply knowledge gained in one
situation in another similar situation, or to use
metacognitive strategies to act in a novel situation.
New knowledge is generated by the influx of
information into an individual’s mind, combined
with the existing knowledge of this individual, and
then communicated further and made explicit
(Blumenberg et al., 2009). After knowledge
creation, it needs to be transferred throughout the
healthcare organization. The knowledge that is
relevant and right to be transferred needs to be
determined as well (Dalkir, 2005). The formal
communities of practice include meetings, and the
informal communities of practice will include
discussion groups, study groups and online
communities (Wang and Lu, 2010). The more
knowledge is shared between individuals, the more
opportunities there are for knowledge creation
(Dalkir, 2005). Due to the reason that communities
are formed with different ways of working and
adoption of different vocabularies, they may not
understand each other (Dalkir, 2005). For example
human actors in IT and the business domain often
speak different technical and procedural languages
(Blumenberg et al., 2009). For instance one domain
can articulate requirements, goals and constraints
that another domain can think of as being
unreasonable and uncooperative (Blumenberg et al.,
2009).
Knowledge storage can be defined as the
organization’s memory which comprises the
knowledge and information that the people working
in the organization possess through their skills and
experiences. The collective memory of the
organization is the organizational culture expressed
through the routines and attitudes inhabiting in
groups and networks (Paoli and Prencipe, 2003).
Organizational memory can be mental abilities and
issues inside the organizational members, but also
the information possible to retrieve, such as copies
of memos, letters, spreadsheets, and data stored in
computers constitute organizational memory (Paoli
and Prencipe, 2003). Alavi and Leidner (2001) claim
that knowledge management systems are a
supporting class of systems to the organizational
processes of knowledge management and knowledge
storage. The organization’s computer-based
communication and information system applications
contain databases, repositories, directories, and
networks.
Knowledge application is the ability to use the
learned material in new and concrete situations by
applying rules, methods, concepts, principles, laws,
and theories (Dalkir, 2005), and knowledge is shared
from different sources. The use of external
knowledge will create new knowledge (Huber,
1991).
Internal learning has two modes of knowledge:
tacit and explicit knowledge. Tacit knowledge is
Knowledge creation&
constructio
n
(2)
Central Hospital
Knowledge transfer (3)
Organizational
unlearning
Internal
learning
Knowledge
acquisition (1)
Knowledge
application (5)
Organizational learning
Knowledge
storage (4)
Department
IC3K2014-DoctoralConsortium
6

gained through clinical and practical experience
(Dalkir, 2005). Räisänen et al. (2010) argue that the
use of healthcare information systems has enhanced
individual learning and group learning, and the
physicians can achieve and create new knowledge
by using information systems. A physician will
require also other knowledge than medical and
clinical knowledge, such as technical skills,
academic knowledge, a hospital’s and healthcare
organization’s cultural knowledge, management
know-how, and administrative skills The knowledge
of healthcare organizations can be transferred to an
individual, a group or a system (Willams and Baláž,
2008). According to Oinas-Kukkonen et al. (2008), a
patient relationship management system is affected
by the impact of the knowledge work performed by
the physicians in a hospital, and the use of the case
system seems to enhance knowledge creation. The
knowledge transfer barriers are lowered between the
physicians and the patients by enhancing
communication through a follow-up system (Oinas-
Kukkonen et al., 2008).
In organizational learning, knowledge is stored
in databases in documents, and the learning entities
are both the individual and organization (Mustonen-
Ollila and Heikkonen, 2003; Morr and Subercaze,
2010). This kind of organizational learning is ‘old
organizational learning’. On the other hand, new
organizational learning means discovering new
theories, practices and innovation and then
distributing or transferring that new knowledge to
the organization (Mustonen-Ollila, 2005; Morr and
Subercaze, 2010).
Organizational unlearning means that old
organizational knowledge is disregarded. The
knowledge considered for elimination is the same
knowledge that led the organization to its previous
success (Turc and Baurnard, 2007), and there is a
need to remove or reject previously used practice
from the organization (Mustonen-Ollila, 2005).
Therefore, change and learning theories are relevant
and should be included in a framework in order to
draw a comprehensive image of processes at work in
the changing organizations (Turc and Baurnard,
2007; Venable et al., 2010).
5 METHODOLOGY
5.1 Data Collection
The case study approach (Yin, 2003) has been
chosen for this study. The primary data sources are
both open-end and structured interviews conducted
at South Karelia Social and Health Care District’s
Central Hospital. Furthermore, archival records are
used as secondary data sources. The interviews are
transcribed and sent to the interviewees to be
checked and corrected. The open-end interviews
create the possibility for individuals or groups to
express themselves freely questionnaires.
First, a pilot study was carried out in the
Obstetrics and Gynecology department of South
Karelia Social and Health Care District’s Central
Hospital in January - March 2013. After the pilot
study, four other departments were included in the
research, and new interview rounds have been and
will carried out in the following order: in January -
April 2014, a second round of interviews was carried
out in the Obstetrics and Genecology department.; in
March - May 2014 the first interview round was
carried out in the Paediatric department.; in March -
June 2014 the first interview round is carried out in
the Paediatric Neurology department.; in May - June
2014 the first interview round will be carried out in
the Surgical department.; and finally in May 2014
the first interview round will be carried out in the
Anaesthesia and Surgery department.
The interview questions have been improved
after each interview round to match the healthcare
organization's knowledge management base better.
The interviews have been and will be tape-recorded
and transcribed. Before the interview, permission is
asked from the interviewee to use the tape recorder.
In the interviews, a predesigned interview protocol
is used, called structured interview, and the
interview questions are sent to the interviewees in
advance (Creswell, 2007).
According to Creswell (2007), the individuals
considered for the interviews need to have
participated in the process or action, and they must
be given the time and place to be interviewed. Our
study is in line with this, because the hospital
arranges the place and time for the interviews, and
the Chief physician of the Obstetrics and
Gynecology department of the Central Hospital acts
as the research site coordinator. Creswell (ibid.) also
highlights the importance of type of sampling and
the number of interviews needed. In any needed
legal permission or arrangements inside the hospital,
the research coordinator is essential, because in the
hospitals and healthcare organizations in Finland the
national laws and regulations are very strict, and also
the interviews need a specific time table, because
they must not affect the patient care work.
KnowledgeManagementConceptsandProcessesinHealthcare-ResearchPlanforDoctoralThesis
7

5.2 Data Analysis
5.2.1 Qualitative Data Analysis with the
Grounded Theory Approach
This study is a qualitative inquiry based on the case
study approach (Yin, 2003; Creswell, 2007). This
method is best suited for social sciences, as it allows
the researcher to interact with the society through
interviews and observations for the purpose of
acquiring the desired data. The researcher will be
able to combine various data sources such as
archival records, interviews, observations, audio
recording, and even quantitative data for the analysis
without restricting the data formats (Joan and Pastor,
2007). The Grounded Theory (GT) approaches of
Glaser and Strauss (1967), Pawluch and Neiterman
(2010) and Corbin and Strauss (1990) are used in the
data collection and analysis. According to Corbin
and Strauss (1990), there are three levels of coding
in the Grounded Theory: open, axial and selective
coding. Open coding reveals similarities and
differences in the data so as to unveil the concepts,
classes and relationships between the concepts in the
data. Similar concepts will be put into the taxonomy
of categories. There is a need to set the dependencies
and relationships between concepts and classes thus
in axial coding categories are analyzed. Through this
the development of the relationships between
concepts will reveal new concepts and relationships.
Selective coding integrates and refines the fully
developed categories into theories. The main theme
of the research emerges from the data during this
phase, but after the main theory is established, the
researcher still refines the categories by trimming off
unwanted ones and filling in those still poorly
developed. In our study, a department in a central
hospital is the unit of analysis. The sample has not
been limited to a certain number of departments,
because the goal of the study is to achieve deep
understanding of the selected case departments and
to identify their knowledge management concepts,
relationships and processes.
Finally, when a research is a collective case
study by nature, it aims at creating a new theory.
The multiple case study approach is applied when
aiming at developing a new theory, and this study
will also utilize a new methodological approach
where both qualitative and quantitative research
approaches are applied. As the quantitative research
approach we use novel intelligent computing and
analyzing methods, which are described in the next
section. The theory creation should thus combine
both multiple data collection methods. The
triangulation will make it possible for the multiple
data collection techniques to provide stronger
substantiation of concepts. Collecting different types
of data by different methods from different sources
produces a wider scope of coverage and may result
in a fuller picture of the phenomena under study.
Especially Eisenhardt (1989) suggests that both
quantitative and qualitative data should be used in
any study. The flexibility given by GT makes it
possible for the respondents to express their views
and opinions easily and freely.
5.2.2 Quantitative Data Analysis with Novel
Intelligent Computing and Analyzing
Methods
As this is study also quantitative, a large sample of
data will be collected in order to carry out the
needed statistical analyses (Kohonen, 1989). The
exploratory data analysis approach is needed for
generating hypothesis due to weaker assumptions
and prior knowledge about the data. Classified
hypothesis testing is applied to reject or accept
hypotheses whenever available. Data mining
techniques are tools for exploratory data analysis.
These include clustering, regression, classification
and association analysis techniques. The goal of data
mining is to find unsuspected relationships and to
summarize the data in novel ways that are both
understandable and useful for the goals of the
project. Especially data visualization methods, such
as the Self-Organizing Maps (Kohonen, 1989,
1995), Bayesian networks (Heckerman, 1996),
multidimensional scaling and hierarchical clustering,
are needed for the understanding of deeper domain
and variable dependencies. For data regression,
linear and non-linear methodologies of classification
and association analysis, combined with variable
selection and uncertainty analysis are applied. As the
general framework, the Cross Industry Standard
Process for Data Mining (CRISP-DM) approach has
been selected. The modeling part includes the
methods mentioned above.
6 EXPECTED OUTCOME
The scientific contribution of the project will be to
create a new theory called knowledge management
life cycle in healthcare, based on the discovered
empirical findings. The practical and managerial
contribution will be helping physicians and nurses to
understand their own valuable knowledge capital
and practice, getting familiar with knowledge
IC3K2014-DoctoralConsortium
8

management practices in the hospital, and helping to
build up better healthcare information systems. The
methodological contribution will be using diverse
qualitative research methods such as the Grounded
Theory and novel intelligent computing methods
together.
REFERENCES
Alavi, M. and Leidner, D.E. (2001) ‘Review: Knowledge
Management and Knowledge Management Systems:
Conceptual Foundations and Research Issues’, MIS
Quarterly, vol. 25, no. 1, pp. 107-136
Blumenberg, S., Wagner, H. and Beimborn, D. (2009)
‘Knowledge transfer processes in IT outsourcing
relationships and their impact on shared knowledge
and outsourcing performance‘, International Journal
of Information Management, vol. 29, no. 5, pp. 342-
352.
Corbin. J. and Strauss, A. (1990) Basic of Qualitative
Research: Grounded Theory Procedures and
Techniques, Newbury Park: Sage Publications.
Creswell, J.W. (2007) Qualitative Inquiry and Research
Design: Choosing Among Five Approaches,
California: Sage Publications.
Dalkir, K. (2005) Knowledge Management in Theory and
in Practice, London, UK: Butterworth-Heinemann
Publisher.
Eisenhardt, K.M. (1989) ‘Building Theories from Case
Study Research’, Academy of Management Review,
vol. 14, no. 4, pp. 532-550.
Eppler, M.J. (2007) ‘Knowledge communication problems
between experts and decision makers: an overview and
classification‘, The Electronic Journal of Knowledge
Management, vol. 5, no. 3, pp. 291-300.
Ferlie, E., Crilly, T., Jashapara, A. and Peckham, A.
(2012) ‘Knowledge mobilization in healthcare: A
critical review of health sector and generic
management literature‘, Social Science & Medicine,
vol. 74, no. 8, pp. 1297-1304.
Ferriani, S., Corrado, R. and Boschetti, C. (2005)
Organizational Learning under Organizational
Impermanence: Collaborative Ties in Film project
Firms‘, Journal of Management and Governance, vol.
9, no. 3-4, pp. 257-285.
Glaser, B. and Strauss, A.L. (1967) The Discovery of the
Grounded Theory: Strategies for Qualitative
Research, Chicago: Aldine.
Gold, A.H., Malhotra, A. and Segars, A.H. (2001)
‘Knowledge Management: An Organizational
Capabilities Perspective’, Journal of Management
Information Systems, vol. 18, pp. 185-214.
Greig, G., Entwistle, V.A. and Beech, N. (2012)
‘Addressing complex healthcare problems in diverse
settings: Insights from activity theory’, Social Science
& Medicine, vol. 74, no. 3, pp. 305–312.
Grover, V. and Davenport, T.H. (2001) ‘General
perspectives on knowledge management: Fostering a
research agenda’, Journal of Management Information
Systems, vol. 18, pp. 5-21.
Hall, A. and Walton, G. (2004) ‘Information overload
within the healthcare system: a literature review‘,
Health Information and Libraries Journal, vol. 21, pp.
102-108.
Hanvanich, S., Sivakumar, K. and Hult, G.T.M. (2006)
‘The relationship of learning and memory with
organizational performance: The moderating role of
turbulence‘, Journal of the Academy of Marketing
Science, vol. 34, no. 4, pp. 600-612.
Heckerman, D. (1996) A tutorial on learning with
Bayesian networks, Redmond: Microsoft Research
Advanced Technology Division.
Hernández, J.G. and Noruzi, M.R. (2010) ‘How
intellectual capital learning organization can foster
organizational competiveness?‘, International Journal
of Business and Management, vol. 5, pp. 183-193.
Hill, K.S. (2010) ‘Improving quality and patient safety by
retaining nursing expertise’, The Online Journal of
Issues in Nursing, vol. 15, no. 3.
Hsiao, H-C. and Chang, J-C. (2011) ‘The role of
organizational learning in transformational leadership
and organizational innovation‘, Asia Pacific Education
Review, vol. 12, no. 4, pp. 621-631.
Huber, G.P. (1991) ‘Organizational learning: The
contribution processes and the literatures‘,
Organization science, vol. 2, no. 1, pp. 88-115.
Iwai, S. and Ishino, F. (2009) ‘Translating tacit medical
knowledge into explicit knowledge’, Journal of
Knowledge Management Practice, vol. 10, no. 2.
Joan, R. and Pastor, A. J. (2007) ‘Applying Grounded
Theory to Study the Implementation of an Inter-
Organizational Information System‘, Electronic
Journal of Business Research Methods, vol. 5, no. 2,
pp. 71-82.
Kohonen, T. (1989) Self-Organization and Associative
Memory, Berlin: Springer-Verlag.
Kohonen, T. (1995) Self-Organized Maps, Berlin:
Springer-Verlag.
Koskinen, J. (2010) ‘Phenomenological view of health and
patient empowerment with personal health record’,
Proceedings of the Well-being in the information
society (WIS) conference, Turku: University of Turku,
pp. 1-13.
Lahtiranta, J. (2009) ‘Current challenges of personal
health information management‘, Journal of Systems
and Information Technology, vol. 11, pp. 230-243.
Latour, B. (1991) Materials of Power, Technology is
society made durable. A Sociology of Monsters:
Essays on Power, Technology, and Domination,
Sociological Review Monograph, vol. 38, pp. 103-
131.
Lauder, W., Reynolds, W. and Angus, N. (1999) ‘Transfer
of knowledge and skills: Some implications for
nursing and nurse education‘, Nurse Education Today,
vol. 19, no. 6, pp. 480-487.
McGrath, J.E. and Argote, L. (2000) ‘Group Processes in
organizational contexts‘, in Hogg, M. and Tindale,
KnowledgeManagementConceptsandProcessesinHealthcare-ResearchPlanforDoctoralThesis
9

R.S. (ed.) Blackwell’s Handbook of Social
Psychology, vol. 3, London: Blackwell Publishers.
Morr, C.E.L. and Subercaze, J. (2010) ‘Knowledge
Management in Healthcare‘, in Cunha, M.M.C.,
Tavares, A.J. and Simões, R. (ed.) Handbook of
Research on Developments in eHealth and
Telemedicine: Technological and Social Perspectives
(pp. 490-510), NY: IGI Global.
Mustonen-Ollila, E. and Heikkonen, J. (2003)
‘Information System Process Innovation knowledge
acquisition and information distribution mechanisms‘,
Proceedings of the UKAIS2003 conference, Warwick,
England, pp. 1-16.
Mustonen-Ollila, E. (2005) Information system process
innovation adoption, adaptation, and unlearning: A
longitudinal case study, Doctoral Dissertation,
Lappeenranta University of Technology: Digipaino.
Mustonen-Ollila, E. and Heikkonen, J. (2008a) ‘IS process
innovation evolution in organisations‘, Academy of
Information and Management Sciences Journal, vol.
11, no. 1, pp. 65-88.
Mustonen-Ollila, E. and Heikkonen, J. (2008b)
‘Information System process innovation evolution
paths‘, Proceedings of the 10th International
Conference on Enterprise Information Systems,
Barcelona, Spain, pp. 171-178.
Mustonen-Ollila, E. and Heikkonen, J. (2009) ‘Historical
research in information system field: from data
collection to theory creation‘, in Cater-Steel, A. and
Al-Hakim, L. (ed.) Information Systems Research
Methods, Epistemology, and Applications. pp. 140-
160, Hersey, New York: Information Science
reference (an imprint of IGI Global), Hersey.
Nonaka, I. (1994) ‘A dynamic theory of organizational
knowledge creation’, Organization Science, vol. 5, no.
1, pp. 14–37.
Nonaka, I. and Takeuchi, H. (1995) The knowledge-
creating company: how Japanese companies create
the dynamics of innovation, New York: Oxford
University Press.
Nonaka, I. and Konno, N. (1998) ‘The concept of “Ba”:
Building a foundation for knowledge creation‘,
California Management Review, vol. 5, no. 1, pp. 14-
37.
Nyerwanire, H. and Mustonen-Ollila, E. (2012)
‘Knowledge management concepts in healthcare
environment‘, Proceedings of World Conference on E-
Learning in Corporate, Government, Healthcare, and
Higher Education, Montreal, Canada, pp. 1660-1668.
Oinas-Kukkonen, H., Räisänen, T. and Hummastenniemi,
N. (2008) ‘Patient Relationship Management: An
Overview and Study of a Follow-Up System‘, Journal
of Healthcare Information Management, vol. 22, no.
3, pp. 24-30.
Oinas-Kukkonen, H., Räisänen, T., Leviskä, K., Seppänen,
M. and Kallio, M. (2009) ‘Physicians’ user experience
of mobile pharmacopoeias and evidence based medical
guidelines‘, International Journal of Healthcare
information Systems and Informatics, vol. 4, no. 2, pp.
57-68.
Pawluch, D. and Neiterman, E. (2010) ‘What is Grounded
Theory and Where Does is Come from?’, in
Bourgeault A., Dingwall, R. and De Vries. R. (ed.)
The SAGE Handbook of Qualitative Methods in
Health Research, London: Sage Publications, pp. 174-
192.
Paoli, M. and Prencipe, A. (2003) ‘Memory of the
organization and memories within the organization‘,
Journal of Management and Governance, vol. 7, no. 2,
pp. 145-162.
Polanyi, M. (1966) The Tacit Dimension London:
Routledge.
Raitoharju, R., Aarnio, E., Oinas-Kukkonen, H., Räisänen,
T. and Suomi, R. (2007) ‘Management of Medication
Knowledge in Six Finnish Primary Healthcare
Centers‘, Proceedings of the 2nd International
Symposium on Medical Information and
Communication Technology, Oulu, Finland.
Räisänen, T., Oinas-Kukkonen, H., Leiviskä, K.,
Seppänen, M. and Kallio, M. (2010) Managing Mobile
Healthcare Knowledge: Physicians’ Perceptions on
Knowledge Creation and Reuse, in Rodrigues, J. (ed.)
Health Information Systems: Concepts,
Methodologies, Tools, and Applications (pp. 733-749).
Turc, E. and Baurnard, P. (2007) ‘Can organizations really
unlearn? ‘, in Mcinerney, C.R. and Day, R.E. (ed.)
Rethinking Knowledge management, Berlin
Heidelberg: Springer-Verlag, pp. 125-146.
Venable, J.J., Pries-Heje, J., Bunker, D. and Russo, N.L.,
(2010) ‘Creation, transfer and diffusion of innovation
in organizations and society: Information systems
design science research for human benefit‘, in Pries-
Heje, J., Venable, J.J., Bunker, D., Russo, N.L. and
DeGross, J.I. (ed.) Human Benefit through the
Diffusion of Information Systems Design Science
Research (1-10), Berlin Heidelberg: Springer-Verlag.
Wang, W. and Lu, Y. (2010) ‘Knowledge transfer in
response to organizational crises: An exploratory
study‘, Expert Systems with Applications, vol. 37, no.
5, pp. 3934-2942.
Wegner, D. M. (1986) ‘Transactive memory: A
contemporary analysis of the group mind‘, in Mullen,
B. and Goethals, G.R. (ed.) Theories of group
behavior, New York: Springer-Verlag, pp. 185-208.
Whelan, E., Donnellan, B. and Golden, W. (2009)
‘Knowledge diffusion in contemporary R&D groups:
Re-examining the role of the technological
gatekeeper‘, in King, W.R. (ed.) Knowledge
Management and Organizational Learning (3-13),
USA: Springer-Verlag.
Williams, A.M. and Baláž, V. (2008) ‘International return
mobility, learning and knowledge transfer: A case
Study of Slovak Doctors’, Social Science and
Medicine, vol. 67, no. 11, pp. 1924–1933.
Yin, R.K. (2003) Case study research: design and
methods, California: Sage Publications.
IC3K2014-DoctoralConsortium
10
