
Remote Mobile Patient Monitoring using Diffuse Optical
Transmissions
Pascal Toumieux, Stéphanie Sahuguède and Anne Julien-Vergonjanne
XLIM UMR 7252, University of Limoges, Limoges, France
Keywords: Wireless Optical Communication, Mobile Communications, Infrared Transmission, Remote Monitoring.
Abstract: In the context of remote patient monitoring, we propose in this paper a radio free solution based system to
transmit health related data. We investigate wireless optical technology based on diffuse infrared links,
which presents the advantage to be secure regarding electromagnetic interference, low-cost and easy to
deploy. Two different monitoring scenarios are considered, both composed of an emitter worn by a mobile
patient and receivers fixed in the environment. The first scenario is the continuous remote monitoring of
heart rate and temperature and the second one involves accelerometer data. To evaluate the wireless mobile
link reliability for the two scenarios, we have developed custom made systems using commercially available
components. The experimental performance is established in terms of packet loss to evaluate the potentiality
of wireless optical technology.
1 INTRODUCTION
Nowadays, there is a rapid growth in medical
devices that incorporate wireless Radio-Frequency
(RF) technology. By eliminating the cables
restricting patient mobility during stay in hospital,
wireless devices contribute to improve patient health
outcomes. However, because of an increasingly
crowded RF environment, the risk of
electromagnetic interferences with other medical
devices has to be considered (Periyasam, 2013). In
addition, the question of prospective health effects
of RF signals in particular long exposure impact is
still open (Benson, 2013). Thus, the deployment of
RF devices can be risky and thus limited in sensible
environments such as hospitals or healthcare
organizations, where high data security and high
immunity against interference with other existing RF
and electronic devices are required.
To overcome this limitation, Wireless Optical
Communication (WOC) based systems can be used
as alternative or complement to RF ones for wireless
monitoring in hospitals (Torkestani, 2012). This
technology has the potential of reducing the amount
of RF effects in patient vicinity because WOC
wavelength range ensures that there is no
interference with existing RF and electronic
equipment. In addition, WOC systems have many
advantages over RF ones such as being free of
license, compact, low cost and having a great level
of security because light cannot pass through walls.
Communicate by using optical beams is one of
the oldest solutions. Since (Gfeller, 1979) WOC in
infrared range have been standardized and with the
development and maturity of optoelectronic devices,
this technology has experiencing a renewed interest.
Indeed, for many years, systems based on infrared or
visible wavelength range have been studied for
indoor and outdoor applications (Carruthers, 1997,
Elgala, 2011; Arnon, 2012; Borah, 2012;
Ghassemloy, 2013).
Two main link configurations are commonly
investigated: Line of Sight (LOS) scheme and
diffuse one. In LOS configuration, the transmitter is
directly pointed towards the receiver. This scheme is
easy to implement and offers high performance, but
it is highly sensitive to misalignments and blocking
effects. Diffuse schemes are more robust because
they exploit multiple reflections of optical beams
over the surface environment to establish non-
directed links between emitter and receiver. The
potentialities of using WOC for healthcare
monitoring have been already investigated
(Torkestani, 2011; Torkestani, 2012; Noonpakdee,
2013). In our previous works the theoretical
performance has been established by determining
553
Toumieux P., Sahuguede S. and Julien-Vergonjanne A..
Remote Mobile Patient Monitoring using Diffuse Optical Transmissions.
DOI: 10.5220/0005275505530557
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2015), pages 553-557
ISBN: 978-989-758-068-0
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
link outage probability for both LOS and diffuse
systems considering emitter mobility.
In this paper, we investigate the feasibility of
practical WOC based system using diffuse optical
transmissions to remotely monitor health data. We
have developed a custom made system dedicated to
a realistic monitoring scenario in a medical unit of
Limoges University Hospital Center (CHU)
concerning post-stroke patients. The objective is to
remotely transmit physiological and physical activity
data during the first weeks of rehabilitation and re-
training effort, which is a critical phase for patients.
During this phase, the patients move in a life
experimental set up of Physical Medicine and
Rehabilitation unit of Limoges hospital. They are
placed in a real situation to assess their capacity to
exercise in different situations of everyday life such
as getting out of bed or cooking for example. It is
therefore extremely important to monitor the patient
throughout this phase and to take into account
patient mobility.
In such context, our contribution in this paper
concerns the experimental evaluation of the wireless
optical technology to transmit health data between
an emitter worn by a mobile patient and receivers
fixed in the environment. We investigate two
different monitoring scenarios, the first one is the
continuous remote monitoring of heart rate and
temperature and the second one involves
accelerometer data.
2 SYSTEM DESCRIPTION
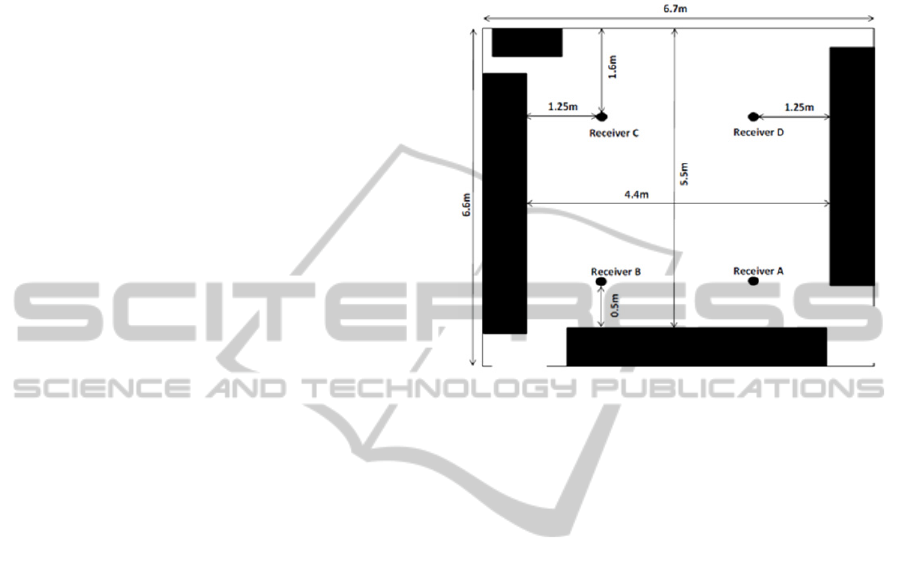
The experiments are performed in a test room of
dimension (6.6m x 6.7m x 3m) as shown in figure 1.
Black areas in the figure correspond to elements of
the furniture. Scratched area corresponds to a
window placed over the entire length of the wall.
In this environment, we consider a patient
equipped with sensors connected to a wearable
hardware unit attached on the body and
communicating by using an optical source which is
an eye safe Infrared (IR) Light Emission Diode
(LED).
Data are sent using Intensity Modulation and
Direct Detection (IM/DD). Four receivers composed
of photo-detectors (named A to D on figure 1) are
fixed on the ceiling and oriented towards the floor.
They are connected to a distant computer
allowing remote access to the data. In such
configuration, because of patient mobility and
source position on patient body, the communication
link is mainly a Non – LOS one, established by
exploiting diffuse reflections over the environment.
A receiver collects beams from all the reflective
surfaces, and thus the total received power is the
sum of all reflective room elements contributions.
Figure 1: Indoor test environment.
2.1 Transmitter
The optical source is a high power infrared diode
(TSAL5100) emitting around 940nm, having a half-
power angle of 10° and generating a maximal optical
intensity of 130 mW/sr.
In the first scenario, we have designed a jacket
worn by the patient equipped with two sensors: a
chest belt for cardiac frequency and a thermistor as
temperature sensor, located under the arm. The LED
is inserted in a plastic part and located on the jacket
shoulder by snaps (figure 2). A cable connection is
realized between the LED and a control unit. In this
configuration, the optical source is mainly oriented
towards the ceiling but it may also point to the walls
and obstacles in the environment according to body
movements.
For the second scenario, the wearable device is
composed of tri-axial accelerometer (MMA7631LC)
and attached on the patient arm (figure 3). The
optical source is mainly oriented towards the ceiling
as in scenario 1, but the orientation can be also
varying according to arm movements.
In both scenarios, the control unit of the device
is composed of a microcontroller based on
Atmega328, battery pack and electronic LED driver.
The signal is emitted with an On-Off Keying (OOK)
modulation, at a baud rate of 4.8 kbps and with a
subcarrier at 38 kbps.
HEALTHINF2015-InternationalConferenceonHealthInformatics
554

Figure 2: Wearable device for scenario 1 (cardiac
frequency and temperature).
Figure 3: Wearable device for scenario 2 (accelerometer
data).
2.2 Receiver
The receivers consist of infrared modules composed
of photo-detectors and preamplifiers (TSOP34338)
with FOV of 45° and a minimal irradiance of
100W/m². They are located in the corner of the
false ceiling tiles with a plastic part to ensure that
they are pointing towards the floor (see figure 4).
Moreover, they are arranged uniformly on the
ceiling as presented in figure 1. They are all
powered by Ethernet modules and connected to a
switch transmitting the received data to a remote
computer connected to a standard RJ45. The
computer analyses the received data and fills a table
containing the sensor information so that it can be
exported at the end of the measurement, and then
plots the measured parameters on a scrolling graph
as data arrive.
Figure 4: Optical receiver module.
2.3 Data Packets
The two types of health data are transmitted,
following a common scheme represented in figure 5.
In both cases, we consider a frame delimiter, a
patient identifier (4 digits: P
3
P
2
P
1
P
0
), a verification
code obtained by summation of information data (9
digits: V
8
V
7
V
6
V
5
V
4
V
3
V
2
V
1
V
0
) and a measure
increment (3 digits: I
2
I
1
I
0
) to identify the information
once when it is received from different receivers.
The verification data and the redundant transmission
of patient identifier are two different ways to check
the integrity of the data.
Figure 5: Packet description.
Depending on the scenario, data packets are not
transmitted at the same period. Let’s denote T
e
this
time duration. In addition, the packet duration T
p
depends also on the scenario as presented in the
following. According to the value of T
p
/ T
e
ratio, the
maximal forward current through the photodiode is
not the same. In each scenario, we adjust the
emission circuit so that we maximize the current and
thus the resulting emitted power.
For the cardiac frequency plus temperature
transmission, data are transmitted at the rhythm of
heart rate, so T
e
is of the order of the second. The
information data are carried over N
d
=2 bytes and
the verification code is obtained by summation of
temperature, cardiac frequency, patient identifier and
measure increment. This scheme leads to T
p
≈ 10 ms
so that T
p
/ T
e
is of the order of 1%. In this case the
forward current is fixed to 325mA. Considering the
temporal occupancy, the average emitted power is
less than 0.5 mW.
For the accelerometer data transmission, there
are N
d
= 6 bytes containing accelerometer values
RemoteMobilePatientMonitoringusingDiffuseOpticalTransmissions
555
over the three dimensions (x, y, z) from the 10-bits
analog to digital converter. The verification code is
in this case obtained by summation of the first five
MSB of accelerometer data over the three axes,
patient identifier and measure increment. This
scheme leads to T
p
≈ 20 ms. In addition, data are
transmitted each 0,1s so that T
p
/ T
e
is around 20%.
The forward current in this case is fixed to 150 mA,
and the average emitted power is less than 4 mW.
3 EXPERIMENTAL RESULTS
To evaluate the wireless optical technology
performance, we have measured packet loss during
mobile transmission within the room presented in
figure 1, for the two scenarios previously described.
We have performed several measurements with
different persons equipped with the two kinds of
devices and different conditions of lighting from sun
and neon lights at room ceiling. Moreover, during
the test, persons moved regularly throughout the
environment.
A packet can be lost for two reasons: the signal is
not received or it is bad received. The signal is not
received if its amplitude is too low to be detected by
the photo-detector, for example when an obstacle
blocks the optical beam. A packet is bad received
when it contains an error so that the receiver rejects
it. An error is detected as soon as the redundant
patient identifier or the verification code is wrong.
Performance is presented in terms of packet loss
rate determined by the number of lost packets over
the total number of packets sent.
We have evaluated the transmission performance
for one active receiver, two and four. The obtained
results are reported on table I, averaged from 10
measurements for each scenario. The measurements
were carried out over a period of 30 min in order to
detect at least 10 packet losses which are necessary
to have reliable paquet loss rate information. For one
active receiver, measures have been performed for
each receiver A to D. For the case with two receivers
we have considered the couples A-C and B-D
corresponding to room diagonals.
As expected, we can see that the performance
improves when the number of receivers increases.
When there are only one or two receivers,
scenario 2 leads significantly to more packet losses
than scenario 1. This can be explained by the fact
that due to the higher ratio T
p
/ T
e
in scenario 2, the
forward current in the photodiode is lower than in
scenario 1, which means a lower peak optical
emitted power. In addition, the emitter position is
not the same on the patient body so that the body can
be more blocking in scenario 2.
Table 1: Packet Loss Rate.
Number of
receivers
Scenario 1 Scenario 2
4 1,3.10
-3
1,3.10
-3
2 4.10
-3
1,5.10
-2
1 4.10
-2
0,11
When the number of receivers increases, we first
remark for scenario 2 that the performance is
significantly enhanced. Indeed, the packet loss rate
has been improved by one decade by comparing the
results obtained from 1 to 2 receivers and also from
2 to 4. On the other hand, we can note that for
scenario 1 this improvement is not so important: the
packet loss rate from 2 to 4 receivers is only divided
by 3. In addition it can be noticed that with 4
receivers, performance between both scenarios tends
towards a similar value. These observations can be
explained by the fact that, in scenario 1, as the peak
optical emitted power is larger, the optimal room
coverage is achieved with fewer receivers than in
scenario 2.
Finally, our experimental results show that it is
important to take into account the data packet
parameters in order to deploy the right number of
receivers allowing a given quality of service in terms
of packet loss while optimizing the emitted power.
Besides, we can say that the value obtained with
4 receivers, which is 10
-3
, is a typical one in wireless
transmission system and permits concluding that the
wireless optical transmission reliability is ensured.
4 CONCLUSIONS
In this paper, we have presented the experimental
performance of an alternative solution to radio
frequencies for healthcare mobile monitoring that is
wireless optical technology. We have used as a
criterion the packet loss of the transmitted data for
two health-related monitoring scenarios having
different constraints.
For both scenarios, we have investigated the
wireless data transmission between a mobile emitter
worn by the patient and receivers fixed in the
environment, by exploiting optical diffuse
reflections over the room surfaces.
The measurement results obtained with two
prototypes made of commercially available and low
cost components have shown that the optical
HEALTHINF2015-InternationalConferenceonHealthInformatics
556

wireless technology constitutes a reliable solution
for health monitoring. In the best coverage
configuration, a packet loss of 10
-3
has been
obtained for both scenarios.
Future work will consist in conducting this
experimentation in the life experimental unit of
Limoges hospital and to evaluate the reliability in
real context of use, especially considering several
monitored patients. In addition, one important point
is to enhance the system by reducing the
consumption and to work on its miniaturization.
ACKNOWLEDGEMENTS
This work is part of SAPHIRALE project supported
by the Limousin regional council (France) and the
AutonomLab living Lab association. (www.limousin
livinglab.fr)
REFERENCES
Arnon, S., Barry, J., Karagiannidis, G., Schober, R., and
Uysal,M., 2012, Advanced Optical Wireless
Communication Systems, Cambridge University Press.
Benson, V. S., K. Pirie, et al., 2013, ‘Mobile phone use
and risk of brain neoplasms and other cancers:
Prospective study’, in International Journal of
Epidemiology 42(3): 792-802.
Borah, K., Boucouvalas, A.C.,Davis, C.C, Hranilovic, S.,
Yiannopoulos, K., 2012 ‘A review of communication-
oriented optical wireless systems’ in EURASIP
Journal on Wireless Communications and Networking,
2012:91.
Carruthers, J.B., Kahn, J.M., 1997 ‘Modeling of
nondirected wireless Infrared channels’ in IEEE
Transaction on Communication, 45, 1260–1268.
Elgala, H., Mesleh, R. and Haas, H., 2011, ‘Indoor optical
wireless communication: potential and state-of-the-
art’, in Communications Magazine, IEEE, vol. 49, no.
9, pp. 56-62.
Gfeller, F.R.; Bapst, U., 1979, ‘Wireless in-house data
communication via diffuse infrared radiation’, in Proc.
of the IEEE, vol.67 ,no.11, pp.1474,1486.
Ghassemloy, Z., Popoola, W., Rajbhandari, S., 2013,
Optical wireless communications, system and channel
modeling with MATLAB®, CRC Press.
Noonpakdee, W., 2013, ‘Adaptive wireless optical
transmission scheme for health monitoring system’ in
Consumer Electronics Berlin (ICCE-Berlin) IEEE
Third International Conference on, pp.161,164.
Periyasam, M.; Dhanasekaran, R., 2013, ‘Electromagnetic
interference on critical medical equipments by RF
devices’, in Communications and Signal Processing
(ICCSP), International Conference on, pp.78-82.
Torkestani, S. S.; Barbot, N.; Sahuguede, S.; Julien-
Vergonjanne, A; Cances, J-P, 2011, ‘Performance and
transmission power bound analysis for optical wireless
based mobile healthcare applications’, in Personal
Indoor and Mobile Radio Communications (PIMRC),
2011 IEEE 22nd International Symposium on ,
pp.2198,2202.
Torkestani, S.S.; Sahuguede, S.; Julien-Vergonjanne, A;
Cances, J.P., 2012, ‘Indoor optical wireless system
dedicated to healthcare application in a hospital’ in
Communications, IET , vol.6, no.5, pp.541,547.
RemoteMobilePatientMonitoringusingDiffuseOpticalTransmissions
557
