
Reliability and Usability of the eChez-Soi In-home Telerehabilitation
Platform: A New Internet-based Communication and Real-time
Monitoring Software Solution Combined with Interactive Exercises
Results of a Longitudinal Pilot Study in Four Patients with Lung Cancer
Hélène Moffet
1,2
, Didier Saey
1,3
, Valérie Coats
3
, Claude Vincent
1,2
,
Fanny Choinière
2
and François Comeau
2
1
Department of Rehabilitation, Faculty of Medicine, 1050 avenue de la Médecine, Université Laval, Québec (QC), Canada
2
Center for Interdisciplinary Research in Rehabilitation and Social Integration,
Institut de Réadaptation en Déficience Physique de Québec, 525 Boulevard Hamel, Québec (QC), Canada
3
Research Center of the Institut Universitaire de Cardiologie et Pneumologie de Québec,
2725 Chemin Sainte-Foy, Québec (QC), Canada
Keywords: Telehealth, Technology, User Perception, Exercise, Video Games.
Abstract: This longitudinal pilot study aims to describe the components and functionalities of the eChez-Soi home-
based telerehabilitation platform, and present preliminary results on its technological reliability and
usability. Four patients receiving chemotherapy treatments for lung cancer followed an 8 week home-based
telerehabilitation program using the new eChez-Soi platform. All 60 planned sessions supervised by a
clinician occurred with few technological problems. Only one session had to be rescheduled because of
unresolved audiovisual communication problems. In 20 sessions, temporary problems were experienced,
mostly related to the audiovisual signal (n=16), while few technical problems were associated with the
sensors (n=1) and the interactive exercise software (n=1). The usability of the platform was very good, with
an overall satisfaction rating of 4.63±0.43 (max. score=5) for all aspects evaluated, namely its dimension,
safety, effectiveness, ease of use and game environment. These preliminary results support the reliability
and usability of our new platform as a whole but highlight the challenges encountered in ensuring a stable
audiovisual signal when delivering services via a standard home-based Internet connection.
1 INTRODUCTION
Implementation of home-based telerehabilitation is
challenging. In combination with the development of
user-friendly and economical platforms that provide
quality audiovisual communication between
clinician and client, it may also be necessary to
allow real-time measurement of biomechanical and
physiological parameters (Theodoros and Russell,
2008). This is particularly essential in prescribing
safe, individually adapted exercises, as well as in
progressively increasing the intensity of exercises to
reach the goal of the intervention, especially in at-
risk populations.
Moreover, there is growing scientific evidence
that a gaming environment, and/or interactive
exercises, adaptable to the needs of users promote
better adherence to prescribed exercises
(Baranowski et al., 2008, Plow et al., 2011). To our
knowledge, however, few telerehabilitation
platforms combining one or more of these
functionalities have been developed; moreover, they
were not widely implemented (Kairy et al., 2009).
They were designed to meet specific rehabilitation
needs of various populations and mainly to retrain
balance and upper limb motor function of patients
with neurodegenerative diseases, acquired brain
injury or post-surgical deficits (Gonzalez-Fernandez
et al., 2010, Parmanto et al., 2010, Gil-Gómez et al.,
2011, Bento et al., 2012, Cikajlo et al., 2012, Kuusik
et al., 2013, Krpic et al., 2013, Eguiluz-Perez and
Garcia-Zapirain, 2014).
This pilot study provides preliminary results
concerning the reliability and usability of the eChez-
137
Moffet H., Saey D., Coats V., Vincent C., Choinière F. and Comeau F..
Reliability and Usability of the eChez-Soi In-home Telerehabilitation Platform: A New Internet-based Communication and Real-time Monitoring Software
Solution Combined with Interactive Exercises - Results of a Longitudinal Pilot Study in Four Patients with Lung Cancer.
DOI: 10.5220/0005476701370142
In Proceedings of the 1st International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AgeingWell-
2015), pages 137-142
ISBN: 978-989-758-102-1
Copyright
c
2015 SCITEPRESS (Science and Technology Publications, Lda.)
Soi platform in the rehabilitation of patients with
lung cancer. The eChez-soi platform is a new
platform for home-based telerehabilitation which
combines interactive exercises with real-time
biomechanical and physiological parameter
acquisition and transmission to the clinician during
telerehabilitation sessions.
The aims of this study were: 1) to describe the
components and functionalities of the eChez-Soi
platform; 2) to describe the reliability of its
technological components and its software solution
designed for real-time acquisition, transmission and
visualization of biomechanical and physiological
signals, and for the creation of a gaming
environment with interactive exercises; and 3) to
collect four patients' perceptions of the usability of
this new platform.
2 METHODS
This pilot study was conducted at the Institut
universitaire de cardiologie et de pneumologie de
Québec (IUCPQ), in collaboration with the Centre
for Interdisciplinary Research in Rehabilitation and
Social Integration in Quebec City. The research
protocol was approved by the institutional ethics
committees. All participants provided written
informed consent before enrollment in the study.
2.1 Participants
Potentially eligible patients (men or women),
between 40 and 80 years of age, diagnosed with lung
cancer and receiving chemotherapy treatments, were
recruited from the Clinique d’oncologie thoracique
de l’IUCPQ. Patients had to have an ECOG
functional status (Scale of the Eastern Cooperative
Oncology Group, see Oken et al., 1982) of 0
(Asymptomatic) or 1(Symptomatic but completely
ambulatory); have a sufficient understanding of
verbal and written instructions; and live in a
geographic region served by a high speed Internet
connection. Exclusion criteria were as follows:
oxygen-pulsed saturation (SpO
2
) <80% during the
cardiopulmonary exercise test; contraindications to
exercise testing according to the American Thoracic
Society and American College of Chest Physicians
Exercise Testing Guidelines (2003); cerebral or bone
metastasis, a history of significant cardiovascular
disease, hypertension, diabetes or musculoskeletal
concerns that might limit their ability to perform
active exercises; and severe psychiatric illness
compromising adherence to the rehabilitation
training routine.
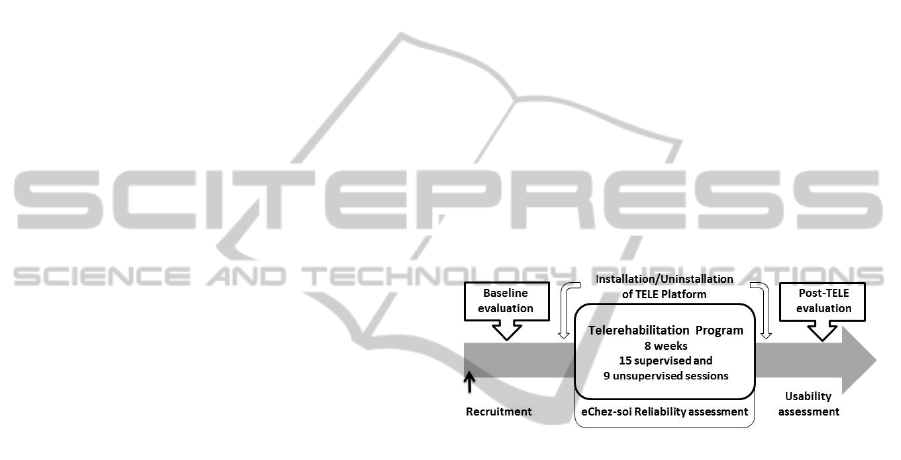
2.2 Study Design
Following their inclusion in the study and a baseline
evaluation, a technician installed the eChez-Soi
platform in the patient's home, and the eight-week
telerehabilitation program was initiated. The
proposed telerehabilitation program included
strengthening exercises for upper and lower body
and cardiovascular exercises, as well as
recommendations to increase the daily physical
activity level. Following the eight-week
telerehabilitation program, participants were
evaluated again and the telerehabilitation platform
was uninstalled. Clinical tests were performed at
both pre- and post-program evaluation times.
Usability of the eChez-Soi platform was assessed
during the post-program evaluation while its
reliability was evaluated throughout the program
delivery period (Figure 1).
Figure 1: Time Line of the Study.
2.3 Telerehabilitation Platform
Through a unique software interface, the eChez-Soi
telerehabilitation platform allows for the
combination of the following three technological
aspects: 1- continuous data acquisition and recording
from commercial biometric sensors and other
instruments used by patients during rehabilitation
sessions; 2- continuous transmission of the collected
data via the Internet to the clinician's computer,
allowing the clinician to visualize the biomechanical
and physiological parameters in real time; and 3- a
challenging gaming environment with interactive
exercises performed on musical rhythms using a
dance mat and a Wii Balance Board. This gaming
environment permits the clinician to create exercise
routines adapted to the patient's condition and to
export them remotely to the patient's platform. At
the end of each routine, a score is provided to the
patient, offering immediate feedback on their
performance in order to encourage them to improve.
Biometric sensors used were: a wrist-worn pulse
oximeter (Nonin WristOx
2
™
, Model 3150), wireless
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
138
wearable accelerometers (LEGSys
™
, BioSensics),
and a Wii Balance Board (Nintendo
®
Wii Fit
™
), all
using Bluetooth-based communication, as well as an
Xbox Dance Mat connected by a USB cable. The
following parameters were also collected regularly
with these instruments: blood pressure (A&D
Medical Blood Pressure Monitor), weight (Aria
™
Wi-Fi Smart Scale) and daily physical activity
(Fitbit Flex
™
). These sensors and devices were
chosen because of their proven technology, ease of
use, and portability, as well as the availability of
Bluetooth or wireless communication.
The audiovisual communication between the
patient and the clinician was supported by the
videoconferencing solution Vidyo (Vidyo
™
Desktop
Software). This solution was chosen as a
videoconferencing platform for its ease of
deployment, its security, and its quality in a standard
network environment.
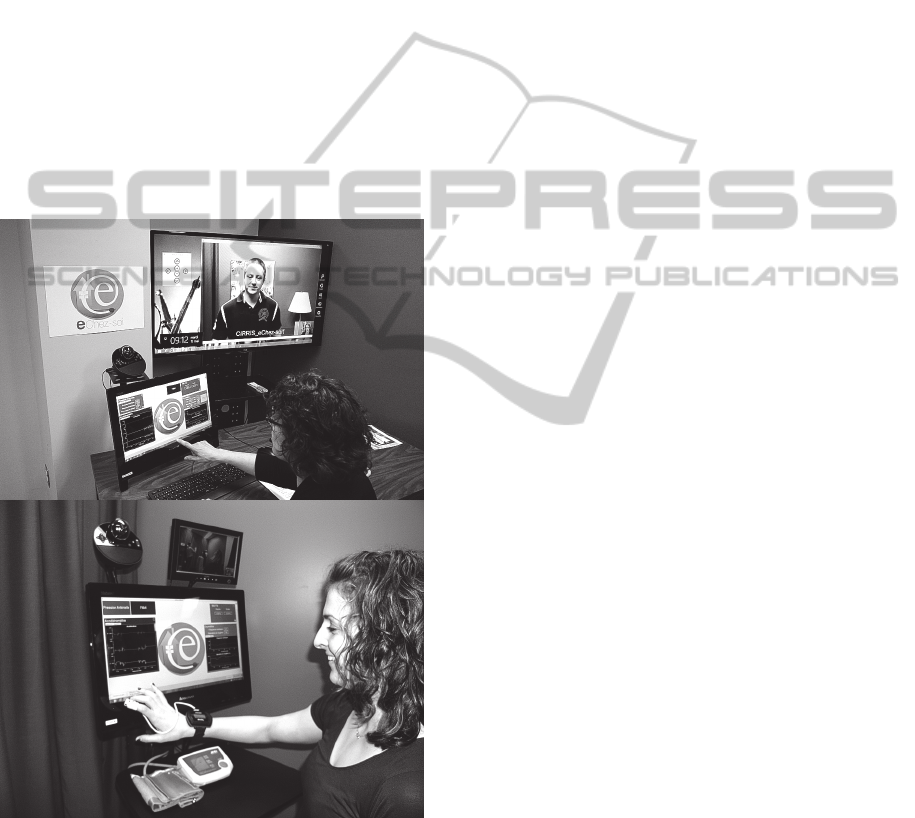
Figure 2: eChez-Soi Telerehabilitation Platform on the
Clinician side (top) and Patient side (bottom).
The home-based telerehabilitation station for the
patients includes an "all-in-one" computer with a
touch screen and Windows 8 friendly user interface,
as well as a small external screen, a webcam, all
sensors and instruments for biomechanical and
physiological measurement and the software
solution. The clinician’s technological station
includes an "all-in-one" computer with a touch
screen and Windows 8 friendly user interface,
combined with a webcam and a large LCD screen
for a good view of the patient (Figure 2).
2.4 Outcome Measures
2.4.1 Clinical Assessment
In order to provide a safe individualized exercise
prescription, a complete clinical evaluation was
made at baseline. It included assessments of
pulmonary functions, body composition, muscle
strength, functional exercise capacity and a
screening for abnormal cardiovascular and
pulmonary response to exercise. Clinical effects of
the program are reported elsewhere.
2.4.2 Reliability and Usability Assessment
Reliability of the eChez-Soi platform was assessed
by documenting the number, type, duration and
transient or permanent nature of the technological
problems encountered during supervised
telerehabilitation sessions. In addition, recordings’
reliability, with respect to the parameters observed
in real time by the clinicians during prescribed
routines of interactive exercises, was verified.
Usability was evaluated using a questionnaire
adapted from the Québec User Evaluation of
Satisfaction with Assistive Technology
questionnaire (QUEST 2.0) that calculates both
satisfaction scores for technological aspects and
services, and the overall scores. It consists of 12
items rated on a scale from 1 to 5 (1: not satisfied at
all to 5: very satisfied) (Demers et al., 2002). The
QUEST has good construct validity (factorial: two
dimensions), good to very good test-retest reliability
(ICC = 0.82, 0.82 and 0.91) and good internal
reliability (alpha: 0.76 to 0.82) (Demers et al., 1999,
Demers et al., 2000). For the present project, five
original technological aspects were preserved (items
1 to 5, Table 2) and seven new aspects (items 6 to
12, Table 2) were added.
2.5 Intervention
The planned intervention was an 8-week supervised
home-based program (3sessions per week with an
average duration of 75 minutes each). Over time, the
ratio of supervised/unsupervised training sessions
was progressively reduced from 3 supervised
ReliabilityandUsabilityoftheeChez-SoiIn-homeTelerehabilitationPlatform:ANewInternet-basedCommunicationand
Real-timeMonitoringSoftwareSolutionCombinedwithInteractiveExercises-ResultsofaLongitudinalPilotStudyin
FourPatientswithLungCancer
139

sessions per week to one, in order to develop the
patient’s autonomy. In total, 15 supervised sessions
and 9 unsupervised sessions were planned for a total
of 24 exercise sessions.
Throughout the program, training modalities and
intensity were adapted to the patient's condition. The
training included: 1) warm-up and stretching
exercises; 2) cardiorespiratory training and 3)
resistance training of the upper and lower limbs.
Exercises were executed using the Xbox Dance Mat
and the Wii Balance Board via a game software
environment developed for this purpose.
Before each supervised session, a short
assessment was conducted to detect any significant
changes in the participant’s health condition. In
addition, the participant's weight and blood pressure
were measured using the platform instruments.
Throughout the exercise session, participants used
the pulse oximeter to assess the components of the
physiological response (heart rate and
oxyhemoglobin saturation). Data were transmitted in
real time to the caregiver by the eChez-Soi platform.
In order to ensure the security of the intervention,
saturation should remain higher than 88%
throughout the session.
3 RESULTS
3.1 Subject Characteristics
Four subjects were recruited between May and
November 2014. Their personal and clinical
characteristics are presented in Table 1.
Table 1: Subject Characteristics.
ID Sex Age
(years)
BMI
(Kg/m
2
)
Stage Tumor
Type
01 Male 56 26.3 IV ADK
02 Female 60 20.6 IIIA ADK
03 Female 64 22.1 IV ADK
04 Male 57 24.2 IV ADK
*ADK: Adenocarcinoma
All patients received chemotherapy treatment during
the intervention period, and two had concomitant
radiotherapy during this period.
3.2 Compliance with the Intervention
All patients completed 100% of the supervised
prescribed exercise sessions (15/15 sessions). No
adverse event occurred during the entire
intervention. Only one training session had to be
postponed following the pre-training evaluation.
(The patient had a high level of psychological
distress and fatigue.) Also, the prescribed intensity
had to be adjusted for one patient who showed a
significant drop in oxyhemoglobin saturation during
a supervised training session. The mean duration of
supervised sessions was 67.5±12.9 minutes, and the
total duration of all 61 sessions was 68.6 hours.
Given some familiarity with the telerehabilitation
platform, due to its previous use in some supervised
sessions, all four patients were able to easily use it
during unsupervised sessions, following brief
instructions from the clinician.
3.3 Reliability of eChez-Soi Platform
3.3.1 Reliability of the Technology
Of the 60 sessions of telerehabilitation offered to the
four patients, only one session had to be delayed due
to an inability to establish audiovisual
communication between the patient and the
clinician. Three other sessions were cut short
because of technical problems.
Temporary problems (n=20) were observed and
resolved during 13 sessions. Most of these problems
were related to audiovisual communication (n=16).
The other difficulties were due to the poor
functioning of a sensor (n=1, pulse oximeter, and
n=1, Wii Balance) or the software solution
(synchronization of a sensor, n=1; interactive
exercises, n=1). 186 minutes in total (4.5% of the
entire duration of the sessions) were used to resolve
these temporary problems. Half of the sessions with
technical problem and the time spent resolving them
occurred during the follow-up care of the first
patient in this study (patient 01; 7 sessions with
temporary technical problems and 91 minutes spent
resolving them).
3.3.2 Real-time Measurements and
Recordings
Data from the pulse oximeter (heart rate and
oxyhemoglobin saturation), the accelerometers and
the Wii Balance were recorded for all interactive
exercise routines (n=331) performed during the 61
supervised sessions without problems, with the
exception of 24 routines (7% of the routines) where
data from at least one sensor, mainly the oximeter
(n=10), were not recorded.
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
140

3.4 Usability of eChez-Soi Platform
All four patients were quite satisfied (score of 4) or
very satisfied (score of 5) with all aspects of the
home-based telerehabilitation platform, for a mean
score of 4.63 (Table 2). No 1 to 3 scores were
reported for any of the assessed items. Ease of use
and effectiveness of the telerehabilitation platform,
and audiovisual communication between the client
and the clinician were identified by the patients as
the three most important elements related to the
usability of the platform.
Table 2: Usability of the Telerehabilitation Platform (TP)
measured with an adaptation of the Quebec User
Evaluation of Satisfaction with assistive technology.
1.
Item How satisfied are you with the… Score
1
1.
dimension of your TP?
4.75 (0.50)
2.
safety of your TP?
4.75 (0.50)
3.
durability of your TP?
4.50 (0.58)
4.
* ease of use of your TP?
4.50 (0.58)
5.
* effectiveness of your TP?
4.75 (0.50)
6.
biometric sensors of the TP for taking
data in real time (e.g. Nonin
oximeter)?
4.25 (0.50)
7.
devices used by the patient for reading
automatic data (e.g. Fitbit Flex)?
4.75 (0.50)
8.
visualization in real time of biometric
data collected by sensors on the client
workstation and transferred to the
clinician’s computer?
4.75 (0.50)
9.
game environment, enabling
customers to perform exercises
tailored to their condition?
4.75 (0.50)
10.
* audiovisual communication between
the client and the clinician?
4.75 (0.50)
11.
touch screen and user-friendly
interface (Windows 8)?
4.50 (0.58)
12.
illustrated procedures accompanying
the user of the TP?
4.50 (0.58)
Overall score (SD): 4.63 (0.43)
1
Mean QUEST score (standard deviation) for the 4 patients (1:
not satisfied at all; 2: not very satisfied; 3: more or less satisfied;
4: quite satisfied; 5: very satisfied)
* 3 items reported as most important.
4 CONCLUSIONS
These preliminary results support the technical
reliability and usability of the eChez-soi
telerehabilitation platform. During the entire period
of this pilot study, relatively few technical problems
were experienced by the users (4.5% of the time).
Almost all technical difficulties were transient and
addressed rapidly within the same session. Lastly,
most of the problems (50%) were experienced by the
first participant, thus demonstrating our capacity to
prevent the repetition of previous technical
problems. However, some problems with the
audiovisual connection or signal quality were
experienced by all participants, thereby illustrating
the challenges of delivering services at home
through a standard home-based Internet connection.
All users were satisfied with the different aspects
of the new platform, with the highest score (4.75/5)
being found for dimension, safety, effectiveness,
devices, visualization in real time of biometric data
collected by sensors, the game environment and the
audiovisual communication between the client and
the clinician, even though most of the technical
problems (80%) were related to this last aspect.
Future studies are needed to confirm the present
results obtained with only four patients, although the
platform was tested during a significant number of
sessions and periods of time (61 sessions lasting 68
hours). This platform's potential should also be
tested in other contexts and populations.
ACKNOWLEDGEMENTS
The authors thank all participants. They also would
like to acknowledge the Clinique d’oncologie
thoracique de l’IUCPQ, including Dr. Lise
Tremblay, for their help in recruiting participants,
and Mr Steve Forest for his technical support with
the eChez-Soi Platform. This pilot study was
supported by the Canadian Lung Association and the
Québec INTER Research Network.
REFERENCES
American Thoracic Society; American College of Chest,
Physicians. 2003. ATS/ACCP Statement on
cardiopulmonary exercise testing. Am J Respir Crit
Care Med, 167, 211-77.
Baranowski, T., Buday, R., Thompson, D.I., Baranowski,
J. 2008. Playing for real: video games and stories for
health-related behavior change. Am J Prev Med, 34,
74-82.
Bento, V. F., Cruz, V. T., Ribeiro, D. D., Colunas, M. M.,
Cunha, J. P. 2012. The SWORD tele-rehabilitation
system. Stud Health Technol Inform, 177, 76-81.
Cikajlo, I., Rudolf, M., Goljar, N., Burger, H., Matjacic, Z.
ReliabilityandUsabilityoftheeChez-SoiIn-homeTelerehabilitationPlatform:ANewInternet-basedCommunicationand
Real-timeMonitoringSoftwareSolutionCombinedwithInteractiveExercises-ResultsofaLongitudinalPilotStudyin
FourPatientswithLungCancer
141

2012. Telerehabilitation using virtual reality task can
improve balance in patients with stroke. Disabil
Rehabil, 34(1), 13-18.
Demers, L., Ska, B., Weiss-Lambrou, R. 1999. Stability
and reproducibility of the Quebec User Evaluation of
Satisfaction with Assistive Technologie (QUEST). J
Rehabil Outcomes Measures, 3, 42-52.
Demers, L., Weiss-Lambrou, R., Ska, B. 2000. Item
analysis of the Quebec user evaluation of satisfaction
with assistive technology (QUEST). Assist Technol,
12(2), 96-105.
Demers, L., Weiss-Lambrou, R., Ska, B. 2002. The
Quebec user evaluation of satisfaction with assistive
technology (QUEST 2.0): An overview and recent
progress. Technol Disabil, 14, 101-5.
Eguiluz-Perez, G., & Garcia-Zapirain, B. 2014.
Comprehensive verticality analysis and web-based
rehabilitation system for people with multiple sclerosis
with supervised medical monitoring. Biomed Mater
Eng, 24(6), 3493-3502.
Gil-Gómez, J.A., Lloréns, R., Alcñiz, M., Colomer, C.
2011. Effectiveness of a Wii balance board-based
system (eBaViR) for balance rehabilitation: A pilot
randomized clinical trial in patients with acquired
brain injury. J Neuroeng Rehabil, 8, 30.
Gonzalez-Fernandez, M., Gil-Gomez, J. A., Alcaniz, M.,
Noe, E., Colomer, C. 2010. eBaViR, easy balance
virtual rehabilitation system: a study with patients.
Stud Health Technol Inform, 154, 61-66.
Kairy, D., Lehoux, P., Vincent, C., Visintin, M. 2009. A
systematic review of clinical outcomes, clinical
process, healthcare utilization and costs associated
with telerehabilitation. Disabil Rehabil, 31, 427-47.
Krpic, A., Savanovic, A., & Cikajlo, I. 2013.
Telerehabilitation: remote multimedia-supported
assistance and mobile monitoring of balance training
outcomes can facilitate the clinical staff's effort. Int J
Rehabil Res, 36(2), 162-171.
Kuusik, A., Sarna, K., & Reilent, E. 2013. Home
rehabilitation system supported by the safety model.
Stud Health Technol Inform, 189, 145-151.
Oken, M.M., Creech, R.H., Tormey, D.C., Horton, J.,
Davis, T.E., McFadden, E.T., Carbone, P.P. 1982.
Toxicity and response criteria of the Eastern
Cooperative Oncology Group. Am J Clin Oncol, 5,
649-655.
Parmato, B., Saptono, A., Pramana, G., Pulantara, W.,
Schein, R. M., Schmeler, M. R., Mccue, M. P.,
Brienza, D. M. 2010. VISYTER: versatile and
integrated system for telerehabilitation. Telemed J E
Health, 16, 939-44.
Plow, M.A., McDaniel, C., Linder, S., Alberts, J.L. 2011.
A scoping review of exergaming for adults with
systemic disabling conditions. J Bioengineer
Biomedical Sci, S1-002.
Theodoros, D. & Russell, T. 2008. Telerehabilitation:
current perspectives. Stud Health Technol Inform, 131,
191-209.
ICT4AgeingWell2015-InternationalConferenceonInformationandCommunicationTechnologiesforAgeingWelland
e-Health
142
