
The International Classification of Functioning,
Disability of Health as a Conceptual Framework for the
Design, Development and Evaluation of AAL Services for
Older Adults
Alexandra Queirós
1
, Joaquim Alvarelhão
1
, Anabela Silva
1
, António Amaro
1
, António
Teixeira
2
and Nelson Pacheco da Rocha
1,3
1
Escola Superior de Saúde, Universidade de Aveiro, Aveiro, Portugal
2
Dep. Electrónica Telecomunicações e Informática / IEETA, Universidade de Aveiro
Aveiro, Portugal
3
Secção Autónoma de Ciências da Saúde, Universidade de Aveiro, Aveiro, Portugal
Abstract. The paper presents the International Classification of Functioning,
Disability of Health (ICF) as a comprehensive model for a holistic approach for
the design, development and evaluation of Ambient Assisted Living (AAL)
services for older adults. ICF can be used to systemize the information that
influence individual's performance and to characterize users, theirs contexts,
activities and participation. Furthermore, ICF can be used to structure a
semantic characterization of AAL services and as a basis to develop
methodological instruments for the services evaluation.
1 Introduction
1.1 Active Ageing
Accordingly to World Health Organization (WHO) population ageing is one of
humanity’s greatest triumphs [1]. It is also one of our greatest challenges: the global
ageing is putting increased political, economic and social demands on all countries.
To overcome these pressures, WHO argues that governments, international
organizations and civil society should promote active ageing policies and
programmes.
The main goal of active ageing is the promotion of older adults in social,
economic, cultural, spiritual and civic affairs, while providing them with adequate
protection, security and care. The implementation of active ageing requires a strategic
planning based on a rights-based approach that recognizes the rights of people to
equality of opportunity and treatment in all aspects of life as they grow older and also
a positive thinking about enablement instead of disablement. We must be aware that a
disabling perspective increase the needs of older people and lead to isolation and
dependence, while an enabling perspective focuses on restoring functions and
expanding the participation of older adults in all aspects of society [1].
Queirós A., Alvarelhão J., Silva A., Amaro A., Teixeira A. and Pacheco da Rocha N..
The International Classification of Functioning, Disability of Health as a Conceptual Framework for the Design, Development and Evaluation of AAL
Services for Older Adults.
DOI: 10.5220/0003341700460059
In Proceedings of the 1st International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications (AAL-2011), pages 46-59
ISBN: 978-989-8425-39-3
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Active ageing depends on a variety of influences or determinants that surround
individuals, families and nations related with personal characteristics, culture and
gender, but also with societal characteristics and infra-structures (e.g. physical
environments, support services, economical and social determinants) [1]. In terms of
individual perspective, the three basic pillars of active ageing are [1]: full
participation in socioeconomic, cultural, spiritual and civic affairs, according to basic
human rights, capacities, needs and preferences; access to the entire range of health
and social services that address the needs and rights of older adults; and protection,
dignity and care in events that older adults are no longer able to support and protect
themselves.
The framework of the International Classification of Functioning, Disability of
Health (ICF) [2] is aligned with the enabling perspective of the active ageing and it
focuses on the individual participation independently of theirs health state.
1.2 International Classification of Functioning, Disability of Health
The ICF offers a framework for conceptualizing functioning associated to health
conditions [3] and it considers that are many factors that affect and have influence on
the individual’s performance and thereby on the decisions made on what type of
service is needed either delivered by care staff, relatives, aid appliances and
technology.
The ICF structure separates between the body, activities, participation and
contextual factors [2] as part of the individual's functioning. Additionally, it considers
the context (environmental factors and personal factors) as components that can
enhance or limit the performance, depending on how the individual experiences
limitations (e.g. due to possible weakness, illness and/or handicap). The structure is
illustrated in the Figure 1 [2].
Health Condition
(disorder / disease)
Body
(impairment)
Activities
(limitation)
Participation
(restriction)
Environmental
Factors
Personal
Factors
Health Condition
(disorder / disease)
Body
(impairment)
Activities
(limitation)
Participation
(restriction)
Environmental
Factors
Personal
Factors
Fig. 1. Interaction of ICF concepts.
Following there is a description of each of the ICF elements [2]:
− Activities - Activities are the individual’s recital of assignments and tasks.
Difficulties with these activities are noted as activity limitations. Limitations are
47

usually due to function depreciation of bodily functions but also due to
environmental hindrances.
− Participation - Participation covers the individual’s involvement in daily life and
society. Difficulties in participation are classified as participation restrictions.
− Body - The body's functions entail the individual’s physiological functions. ICF
defines disability as any problem of the individual with his/her bodily functions.
Physical functions depreciations can, in principle, have no consequences for the
individual's ability to do activities, especially if there are help aids that compensate
particular functions depreciation (e.g. an individual with weak eyesight wearing
glasses would not have a limitation.
− Contextual factors - The contextual factors are the environmental and personal
factors which either enhance or limit the individual's functioning. These factors are
indirectly understood in the sections of evaluation of activities and participation;
however, they are important to explain certain situations (e.g. two individuals with
the same diagnosis/ physical function depreciation may have different limitations
when it comes to activities and participation). The environmental factors are the
physical, social or attitudinal world ranging from the immediate to more general
environment. The personal factors entail elements that make people different and
unique, such as life style, education level, sex, race, life events or psychological
characteristics.
Differences in mastering capacity are a possible explanation to why individuals
with the same physical function depreciations do not have the same limitations when
performing various activities. For example, when it is windy outside, some
individuals will put up wind shelters, whilst others put up windmills. Dependent on
whether one looks upon changes as strenuous or as a challenge which contains new
options.
The environmental factors can have a positive (i.e. be facilitators) or negative
impact (i.e. be barriers) on the individual’s performance as a member of society, on
the individual’s capacity to execute actions or tasks, or on the individual’s body
function or structure. When coding an environmental factor as a facilitator, issues
such as the accessibility of the resource, and whether access is dependable or variable,
of good or poor quality, should be considered.
In the case of barriers, it might be relevant to take into account how often a factor
hinders the person, whether the hindrance is great or small, or avoidable or not. It
should also be kept in mind that an environmental factor can be a barrier either
because of its presence (e.g. negative attitudes towards people) or its absence (e.g. the
unavailability of a needed service).
The classification has individual items or codes defined within each chapter. The
ICF contains 1,424 codes organized according to an alphanumeric system. Each code
begins with a letter that corresponds to its component domain: b (Body Functions), s
(Body Structures), d (Activities and Participation) or e (Environmental Factors). The
letter is followed by between one and five numeric digits. Items are organized as a
nested system so that users can telescope from broad to very detailed items depending
upon the needs presented by particular applications of the ICF.
48

1.3 Living Usability Lab Project
Over the last decade, considerable research efforts have been pursued by the
European Commission, national governments and relevant industries to provide an
adequate technology response to the challenges of an ageing society [4]. In terms of
technology uses, the so called independent living or Ambient Assisted Living (AAL)
domain today comprises a heterogeneous field of applications ranging from quite
simple devices such as intelligent medication dispensers, fall sensors or bed sensors to
complex systems such as networked homes and interactive services. Some are
relatively mature and some are still under development.
Considering the growing importance of AAL services, the Living Usability Lab
(LUL) intends to develop AAL services to fulfill some needs that are common to
older adults: full participation in society, health and quality of life or living with
security.
Dependency is strongly related with the ability to perform Activities of Daily
Living (ADL). There are two groups of ADL: the basic ADL consist of those skills
needed in typical daily self care, namely personal hygiene, dressing and undressing,
eating or moving around; and instrumental ADL are skills that let an individual live
independently in a community, beyond basic self care, and that may include typical
domestic tasks, such as driving, cleaning, cooking, and shopping, as well as other less
physically demanding tasks such as operating electronic appliances or handling
budgets.
Basic ADL are out of the scope of the LUL since most of the times require the
caregiver intervention. The impossibility of perform instrumental ADL like
housekeeping (e.g. cleaning, cooking, shopping, or ironing) usually implies that the
individual needs help and although, in some circumstances, he/she can live alone,
although in border of the dependency. It is clear that AAL services can not supply
these needs completely but they can mitigate the effects by means of specialized
service (e.g. an e-commerce solution for shopping or a well managed external
housekeeping service) [5].
Additionally, AAL services can contribute to increase the older adults’
performance in a broad spectrum of activities and participation [5]: personal care,
planning of the weekly menu, nutritional advisor, maintenance of house and garden,
self administration or agenda; support in finding and carrying out work, establishing
and maintaining contacts with other people, and, in general, in spending the day
(through the participation in different leisure activities) and social integration
participation.
Furthermore, AAL services can contribute to the reorientation in health systems
that are currently organized around acute, episodic experiences of disease, namely, by
allowing the development of a broad range of services such as care prevention and
care promotion and home-caregiver support.
Some of the AAL services for older adults consider their users as people who are
weak and passively assisted by others [6, 7]. The position should be the opposite:
those services should help encourage the older adults to actively participate in society
(i.e. the enabling perspective of the active ageing paradigm). However, older adults
are usually scared by the application of new technology. Therefore, we should
construct user friendly interfaces, and also provide appropriate trainings to their users.
49

Developing adaptive, natural and multimodal human computer interfaces is the main
challenge of future interfaces in AAL [8]. This is the main goal of the LUL project.
2 Our Position
Taking in consideration the needs of the target users for the AAL services aimed by
our Living Lab and the state of the art, we defend that integration of a holistic view of
the individuals and their context is needed and has the potential for advantages in
terms of the adequacy of the services being developed.
The existence of a conceptual framework based on standardized concepts can
provide a common language between strategic planners, technological innovators,
care providers and users for the development of new services in general and, in
particular, new AAL services. We argue that ICF can be used as a conceptual
framework to systemize the information that can influence individual's performance,
not only in terms of health conditions or physiological functions, but also in terms of
contextual (both personal and environmental) factors and it can be used as
comprehensive model for a holistic approach to characterize users, theirs contexts,
activities and participation:
− The ICF body (physiological functions) and personal factors (e.g. life style,
education level, sex, race, life events or psychological characteristics) can be used
to model the final users and theirs specific needs.
− The ICF contextual (environmental and personal) factors either enhance or limit
the individual’s functioning and, clearly, must have an important role in AAL
services for older adults, considering that one of their main goal is to maintain
older adults activities and participation in society. In particular, ICF environmental
factors (e.g. physical, social or attitudinal) must be considering when modeling the
immediate or more general environment.
ICF fundamental concepts are related with functioning and performance in activities
and participation. On the other hand, the goal of AAL services for older adults is the
development of technological solutions to enhance theirs activities and participation
in all aspects of society. Therefore, it should be possible, and desired, to use ICF for:
− The specification, development and characterization of AAL services.
− The development of suitable instruments for the evaluation of the AAL services
and their impact on the daily life of older adults (i.e. activities and participation).
Potential advantages of ICF usage in several aspects of the AAL services for older
adults will be addressed in the following sections, namely: user modeling and
profiling, essential for adaptable and intelligent services; development of complex
AAL services; and AAL services evaluation.
50

3 Users Modeling and Profiling
Users modeling and profiling provides the methodology to enhance the effectiveness
and usability of services and interfaces in order to: tailor information, predict user's
future behavior, help the user to find relevant information, adapt interface features to
the user and the context in which it is used, and indicate interface and information
presentation features for their adaptation to a multi-user environment.
As a variety of users may operate with AAL services, a users’ model serve as a
description of the users of a system and a prediction of how they will behave and
perform tasks. These goals are achieved by constructing, maintaining and exploiting
user models and profiles, which are explicit representations of individual user’s
preferences.
Different models have been considered for the development of applications and
information systems for support in activities based on new paradigms that promote
the human ability to solve problems. These models differentiate the users in terms of
information processing capabilities, according to individual differences of a physical
nature, according to individual differences of a psychological nature, and also
considering environmental and cultural factors. As a result of this research a set of
meaningful international usability standards were defined.
One of this international usability standards (the ISO/IEC 24756 [9], which
defines a framework for specifying a Common Access Profile of needs and
capabilities of users, computing systems, and their environments) was used together
with ICF by the Vaalid [10] project as an attempt to characterize the user profile [10,
11], namely to qualify the abilities of the older adults that have direct impact on
successful use of ICT product and services, following the recommendations of the
ETSI EG 202 116 [12]: sensory, physical and cognitive abilities.
The abilities were classified using body functions and structures and some
concepts related with activities and participation of ICF. However, we argue that a
step forward is possible due to the fact that other individual factors, such as
anthropological characteristics or preferences can be considered using the ICF
framework. ICF, as a model that offers a balance between a purely medical and a
purely social approach, contains essential information for the profile characterization
of body functions and structures, personal factors and activities and participation:
body functions and structures allow the definition of the type of access to services, as
well as, the definition and configuration of its interfaces; personal factors allow the
characterization of personal preferences in the definition and configuration of services
and interfaces; and activities and participation allow the characterization of the
services that best fit the person’s functioning.
Detailed information associated with these components determines the type of
AAL service access, the need for assistive technology and appropriate adaptation of
its interfaces.
From the point of view of users, we can not forget that their models have to be
dynamic in order to adjust to the context in which they operate. Context can be
considered as any information that can be used to characterize the situation of an
entity. An entity is a person, place, or object that is considered relevant to the
interaction between a user and an application, including the user and application
themselves [13]. Additionally, it is also clear that not all types of contextual
51

information can be easily sensed. Some types of contextual information (e.g. the
mood of the individuals) can only be derived by intelligent combination of other
information or by human inputs [13].
The ICF model is consistent with these requirements as a person’s performance
can be characterised as the result of a complex relationship between health conditions
and personal and external factors. External factors represent the circumstances in
which the person lives, i.e. the functional performance of a person in the activities and
participation is influenced by his/her individual characteristics and participation, and
the environmental factors can be considering a facilitator or barrier to his/her
functioning.
Therefore, concerning the user model, the individuals are a combination of body
functions and structures, activities and personal and environmental factors. Personal
factors include gender, age, coping styles, social background, education, profession,
past and current experience, overall behaviour pattern, character and other factors that
influence how disability is experienced by the individual [2]. Additionally,
environmental factors can be grouped in the following classes: products and
technology; natural environment and human-made changes to environment; support
and relationships; attitudes; services, systems and policies.
However, we must be aware that the development of ICF is still work in progress
what may pose some challenges:
− Personal factors still need an in depth study to avoid the need to use concepts
outside the ICF for the complete definition of the user model.
− In the context of AAL services, it is urgent to identify habits and routines. These
are the recurring patterns of a person’s behavior, usual activities performed and
resources used. These concepts are not explicit in the ICF, but they are highly
relevant to the classification of environmental factors.
− The capture and systematization of environmental factors is one of the biggest
challenges [14]. Measure the impact of the environmental factors on human
functioning is becoming an important subject to optimize interventions and reduce
participations restrictions [14]. In recent years different instruments have been
developed for assessment of impact of environmental factors in human
functioning, reflecting the concern about the inclusion of this component of ICF in
a comprehensive assessment.
Despite the difficulties listed, we believe that the ICF can help modulate users and
theirs contexts from a holistic viewpoint. Additionally, we believe that the difficulties
mentioned must be seen as opportunities and challenges: the use of ICF beyond the
restricted field of health will bring interesting contributions to its own development
and will help the ICF to meet all the requirements identified for user model within the
AAL services.
4 Development of Complex AAL Services
The System Architecture proposed for the LUL follows the paradigm of service
orientation, which allows developing software as services that are delivered and
consumed on demand. The benefit of this approach lies in the loose coupling of the
52

software components that make up an application. Discovery mechanisms can be used
for finding and selecting the functionality that a client is looking for. Many protocols
already exist in the area of service orientation.
The architecture components are divided into three layers: the base middleware
layer contains the functionality that is needed to facilitate the operation of the
networked environment; the intelligent middleware layer contains the functionality
that is needed to facilitate the usability and acceptance of the services (it provides
users modeling and profiling, user interface management and context awareness and
notification); and the application layer allows dynamic services composition, which is
essential to allow the congregation of different services to build domain specific
applications.
Therefore, the application services have a hierarchical structure in which a
particular service is made up of components. Each one of these components could be
composed by more elementary services.
Furthermore, the interactions between the assistive devices, human services and
end users, must be under a service oriented management perspective. Assistive
devices and human services interactively work together to express potentials from
both sides providing high quality services to the people with needs [6]. Effective and
efficient solutions to meet the AAL challenges should combine the forces from both
the technological part and the societal ones. The participations of human beings could
help fully express the potential of smart devices, and maintain the social awareness of
the older adults. Although informal caregivers may help reduce the needed social
resources, and increase the social connections, they are inherently very dynamic: the
availabilities of the caregivers are continuously changing.
A scenario is a specific context where the activities and participation, features and
resources are well defined. It gives us the information about which AAL, human and
technological support services are necessary to assist older adults in social, economic,
cultural, spiritual and civic affairs.
Considering this services organization, an efficient infrastructural support for
building AAL services aggregation is needed [15]. It consists of the following
infrastructure services which act as basic service components: service registration;
semantic service descriptions; semantic match service; and service binding.
The services must be described based on a standard, commonly declarative,
service description language to enable service discovery and invocation independently
of its implementation details. An example of a suitable service description language is
the XML-based WSDL language, used to describe web services. Additionally, there
must be an ontology able to classify the different AAL services and thus facilitate
their re-use.
There are a huge number of possibilities in terms of possible classifications of
AAL services:
− Persona [5] project defines usage scenarios (these provide a basis for subsequent
specification and evaluation of services and basically define specific contexts and
how users carry out their tasks in these contexts. Since the number of available
scenarios is rather big, the end users have been asked to identify the most
interesting scenarios. This led to the selection of the following eight scenarios [5]:
peer to peer exchange; meeting other people; enhanced activity assistant; personal
53

safety; behavior detection; health status management; neighborhood assistant; help
in planning and conducting a journey using public transportation.
− In a different approach [16] AAL application are considered as composed of a set
of services that can be grouped into two categories: health-oriented services and
comfort services. Health-oriented services (e.g. health and activity monitoring)
allow the older people to access to medical and emergency services, and facilitate
collaboration among medical staff. Comfort services are services that allow the
older adults to maintain social and familiar contacts or that allow them to access
information to which they are interested or shopping assistance.
− Different services do not require the same properties of the execution environment
such as security, confidentiality or urgency. This could lead to another type of
classification [16, 17] based on three type of assistance: emergency assistance (e.g.
assistance detection, prediction and prevention); autonomy enhancement services
(e.g. drinking, eating, clearing, dressing, medication, shopping assistance or
traveling assistance); and comfort services (e.g. logistical services, services for
finding things, infotainment services transportation services or orientation
services).
− The European Ambient Assisted Living Innovation Alliance focuses on the needs
of older adults to categorize all products and research activities [11]: social
interaction (i.e. all kinds of products, services and research projects that enable
older adults to stay in touch with the world beyond their domestic environment);
health and home care (i.e. combination of supporting assistive technologies and
rather conventional health or home care solutions might be best suited to provide
the framework necessary for autonomous living conditions of older adults that can
be further divided into prevention, assistance or therapy); supply with daily goods
and chores; and safety (i.e. for fulfilling the safety, privacy and security needs of
older adults).
Considering the broad range of sub domains used to classify AAL services (which
is natural taking in consideration the maturity level of this technology) is not an easy
task to identify an appropriate semantic knowledge base to precisely describe the
advertised services. The question of how to automatically map the available/requested
services is still a big challenge in AAL.
We consider that the conceptual framework of ICF could be useful to solve critical
issues related with the services organization. Since the activities and participation, i.e.
involvement of the person in real life situation, is what justifies the use of AAL
services, we can and we should used ICF for the structuring and classification of AAL
services.
The component activities and participation is a neutral list of domains indicating
various activities and areas of life (learning and applying knowledge, general tasks
and demands, communication, mobility, self-care, domestic life, interpersonal
relationships and interactions, major life areas, community, social and civic life),
which are subdivided into three levels increasing the accuracy of the classification.
The list of areas of activities and participation covers the full range of functioning
that can be coded at the individual and social level. This component can have
different uses, considering the concepts of activities and participation. The ICF
defines four ways to use this list of domains: different groups of domains of activities
and domains of participation (not allowing overlap), partial overlap between the
54

groups of domains of activities and participation, the existence of detailed categories
of activities and broad categories of participation, with or without overlap and use the
same fields for both activities and participation with complete overlap of the fields
[2].
For the definition of an ontology to categorize the AAL services we proposed the
ICF participation domains. This implies that we have to define a border line between
activities and participation [18]: we consider the first two activities and participation
domains (learning and applying knowledge, general tasks and demands) as activities
(used to define the user profile, as they qualify the user abilities to perform activities)
and the remainder five domains (communication, mobility, self-care, domestic life,
interpersonal relationships and interactions, major life areas, community, social and
civic life) as participation because they are more related with the individual’s
performance [19].
Figure 2 represents a layer organization’s services for a specific scenario (peace of
mind), using the example of a choreography of AAL services conceptualized by the
Persona [5] project in attempt to maintain peace of mind of adult child concerning the
well-being of their parents [20].
AAL services highlight the technology as a facilitator of the person’s performance
improving functioning. This means that the results associated with the development of
AAL services are strongly oriented to technology, i.e. services are conceptualized and
developed considering the potential of technology. This can cause problems when
trying to classify, according to ICF, services already developed or being developed.
However, it is clear that a structured classification of AAL services should not be
oriented to technology, but to individuals. This is a strong argument to use the ICF as
the basis for an otology for the AAL services and its components.
5 AAL Services Evaluation
The AAL services evaluation is an approach to the technology design and
development process that can be divided in two main phases: anticipation of impacts
and consequences and performance assessment.
The publication, in 1999, of the ISO 13407 standard (Human-centered Design
Processes for Interactive Systems) [21] was an international recognition that the
human factors have processes which can be managed and integrated with the project
processes. According to this ISO standard the first steps within the user centered
design process are [22]: understanding and specifying the context of use; and
collecting and analyzing users’ needs and requirements.
However, the usually approach for involving users throughout the whole R&D
process is typically followed by the development of prototypes by experts. By doing
this, decisions about the conceptual design, i.e. what kind of functions are to be
developed and what the interaction should be like, are made by experts. The
prototypes, based on those conceptual design ideas, are then evaluated by users.
Therefore, the initial design ideas are not based on the mindsets, experiences and
mental models of the users but on the experts. The user can intervene only through the
user based assessment [23].
55
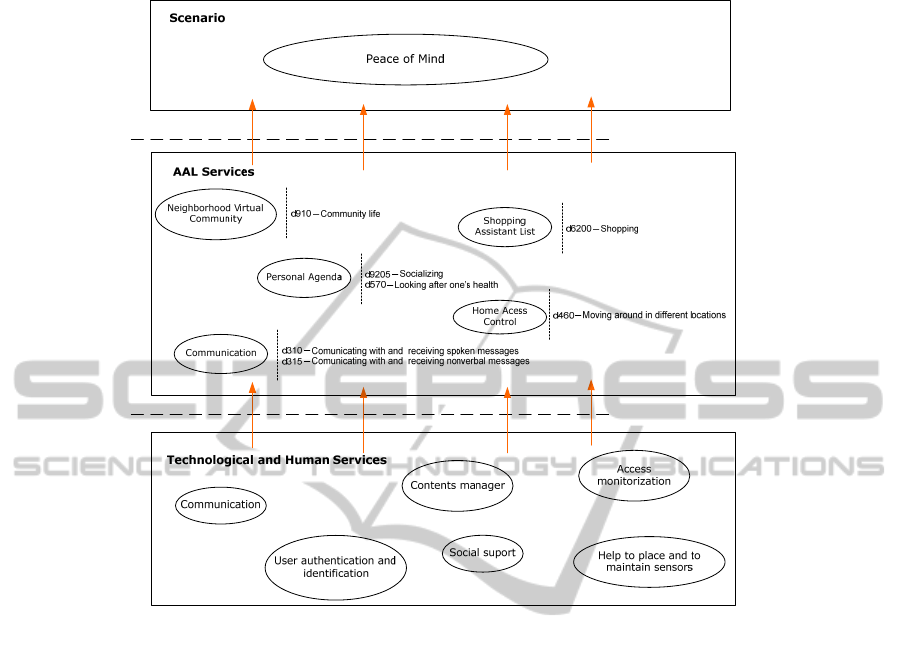
Fig. 2. Peace of Mind scenario.
A central idea of the Living Lab concept is a strong involvement of the users in all
the development phases, including the conceptual design and, later, the prototypes.
Therefore, new methodologies are required to allow the generating of new design
solutions and the evaluation of design solutions derived from the first phases of user
involvement. Focused design discussions, theatre and multilevel prototyping [23].
Although the process is cyclic, it should be flexible enough to move forwards,
backwards, and crosswise between phases. Notably, practice and use are tightly
interwoven by these phases, since the output from one becomes the input for another.
In particular, the prototypes that that evolve from empirical studies may become part
of the Living Lab infrastructure for use in future studies. These prototypes together
with the evaluation results are additionally useful for future model and tool building,
and they lead to further cycling though the Living Lab [23].
The evaluation has several goals: evaluate process/ways of working changes;
measure hard data of the improvements/changes; evaluate fit between software
concepts and users real way of working; evaluate acceptance, satisfaction, motivation
and individual performance of users; evaluate usability, bugs, functionality of
software; and create ideas about improvements and new features.
For the performance assessment the technological developments have been based
on a fairly limited view and, in particular, the evaluation methodologies focus on
56

instrumental factors, such as mobility, physical and sensory deficit and ability to
perform activities of daily living and rarely on advanced activities of daily living and
social roles. There’s an imperative for changing this paradigm as the result of higher
levels of performance that health and social interventions demands. In fact, we also
need to understand how the technology influences the (re)motivation and the
(re)organization of the human performance within a particular context. Humans as
open systems can accomplish changes over time through the engagement in
meaningful activities with the propose of fulfill the sense of achievement and control
of own life. As we state before this level of functioning is a dynamic interaction
between the person and the environment where the personal causation, values,
interests, habits and routines play a very important role. To this dynamic interaction
we call it meaning.
An ecological model focused on practical aspects of everyday activities of the
person, highlighting opportunities for technology and design solutions to support
these activities is a useful framework for guiding the evaluation process. The
activities that comprise a person’s everyday life are shaped by a range of different
factors, including attributes of the person (e.g. functional ability, cognitive ability or
psychological factors) and attributes of the immediate and wider socio-cultural
contexts (e.g. formal support network, social network, physical environment or
cultural and political determinants) [11].
Assuming that AAL services intend to highlight environmental factors referring to
technology to improve participation and quality of life, such services should be
evaluated taking into account theirs impact on activities and participation of the user,
particularly on his/her quality of life, which includes the meaning and the satisfaction
of the performance.
Therefore, it is extremely important to develop new methodological approaches to
include not only the performance of the individual but also the meaning and
satisfaction with their performance.
ICF model contemplates some of the factors previously listed and also considers
that environmental factors and the individual cannot be conceptually separated. The
ICF ecological perspective are reasons strong enough to use this conceptual model to
develop methodological instruments to evaluate in a holistic perspective the impact of
AAL on older adults quality of life, including the meaning and the satisfaction of the
performance. On the other hand, it is of utmost importance to adopt the ICF as this is
a WHO classification internationally used.
6 Conclusions
In the previous sections we had presented arguments that sustain the possibility of
using ICF in different aspects of design, development and evaluation of AAL services
for older adults. ICF can be used as a universal framework to characterize users’
profiles and theirs environments, to structure a semantic characterization of AAL
services and to develop methodological instruments for the AAL services evaluation.
Therefore, we believe that ICF can be used as a conceptual framework for the
design, development and evaluation of AAL services. Within the LUL project we
57

intend to demonstrate that such a conceptual framework can overcome some of actual
difficulties related with AAL services design, development and evaluation.
One of the problems of using technology and information systems for care
provision is the communication difficulties between technology professionals and
caregivers. Different professionals with different backgrounds and needs but who
speak a common language increase the efficiency of teamwork. This leads to a better
performance when developing new services or when improving existing services. In
particular, the use of a conceptual framework from WHO, as is ICF, facilitates the
work of multidisciplinary teams.
Additionally, although it may be needed to complete ICF with additional models,
it can help to overcome a recurring problem that is the lack of data to create robust
user’s models. Properly safeguarding ethical issues, the ICF can allow almost
unlimited access to appropriate information properly encoded.
Last but not least, using the ICF to enhance the semantic interoperability
facilitates the generation of knowledge: the existence of universally accepted
conceptual models, and its terminology, concepts and coding of information allows
the aggregation and consolidation of the available information, which will be essential
for the strategic planners, technological innovators, care providers and users involved
in the development of AAL services.
Acknowledgements
This work is part of the COMPETE – Program Operacional Factores de
Competitividade and the European Union (FEDER) under QREN Living Usability
Lab for Nest Generation Networks (hrrp://www.livinglab.pt).
References
1. World Health Organisation: Active Ageing: A policy framework (2002)
2. World Health Organization: The International Classification of Functioning, Disability and
Health (ICF). Geneva, Switzerland (2001)
3. Peterson, D. B.: International Classification of Functioning, Disability and Health: An
Introduction for Rehabilitation Psychologists. Rehabilitation Psychology, Vol. 50, No. 2,
(2005) 105–112
4. O’Grady, M. J., Muldoon, C., Dragone, M., Tynan, R., O’Hare, G. M. P.: Towards
evolutionary ambient assisted living systems. Journal of Ambient Intelligence and
Humanized Computing, Vol 1, Number 1, Springer-Verlag (2009) 15-29
5. Ochoa, E. [et al]: PERSONA - PERceptive Spaces prOmoting iNdependent Aging -
Deliverable 2.1.1 - Report describing values, trends, user needs and guidelines for service
characteristics in the AAL Persona context (2008)
6. Hong Sun, V. F., Ning Gui, C. B.: Promises and Challenges of Ambient Assisted Living
Systems, Sixth International Conference on Information Technology: New Generations
(2009)
7. Hong Sun, V. F., Ning Gui, C. B.: Towards Longer, Better, and More Active Lives -
Building Mutual Assisted Living Community for Elder People. In the Proceedings of the
47th European FITCE Congress, FITCE, London (2008)
58

8. Kleinberger T., Becker M., Ras E., Holzinger A., Muller P.: Ambient Intelligence in
Assisted Living: Enable Elderly People to Handle Future Interfaces, Universal Access in
Human-Computer Interaction. Ambient Interaction, Part II, HCII (2007)
9. Janse, M. (ed.), Ramparany, F., Kladis, B., Rozendaal, L., Broens, T., Eertink, H.: IST
Amigo Project Deliverable D2.3 Specification of the Amigo Abstract System Architecture
(2005)
10. Mocholí, J. L., Sala, P., Navarro, A.: VAALID - Accessibility and Usability Validation
Framework for AAL Interaction Design process. D2.2 - Concept & Services ontology
description, VAALID Project (2010)
11. Broek, G. [et al]: Ambient Assisted Living Roadmap. Alliance – The European Ambient
Assisted Living Innovation Alliance (2009)
12. ETSI EG 202 116 v1.2.1 (2002-09): Human Factors (HF); Guidelines for ICT products and
services; “Design for All” (2002)
13. Ramparany, F. [et al]: IST Amigo Project. Deliverable D2.2 - State of the art analysis
including assessment of system architectures for ambient intelligence (2005)
14. Lemberg, I., Kirchberger, L., Stucki G., Cieza A.: The ICF Core Set for stroke from the
perspective of a physicians: a worldwide validation study using the Delphi technique.
European Journal of Physical and rehabilitation Medicine, 46 (2010)
15. Hong Sun, V. F., Ning Gui, C. B.: Towards Building Virtual Community for Ambient
Assisted Living. 16th Euromicro Conference on Parallel, Distributed and Network-Based
Processing, IEEE Computer Society (2008)
16. Segarra, M. T., André, F., Building a Context-Aware Ambient Assisted Living Application
Using a Self-Adaptive Distributed Model. ICAS 2009 : Fifth International Conference on
Autonomic and Autonomous Systems , Valencia (2009)
17. Avil´es-L´opez, E., Villanueva-Miranda, I., García-Macías, J. A., Palafox-Maestre, L. E.:
Taking Care of Our Elders Through Augmented Spaces. LA-WEB '09: Proceedings of the
2009 Latin American Web Congress (la-web 2009) (2009)
18. Kostanjsek, N.: Semantic Interoperability – Role and Operationalization of the International
Classification of Functioning, Disability and Health (ICF), International Journal of
Integrated Care, Vol 9 (2009)
19. Jette, A., Tao W., Haley, S.: Blending activity and participation sub-domains of the ICF.
Disability and Rehabilitation (2007) 1742 – 1750
20. Rowan, J. T.: Digital Family Portraits: Support for Aging in Place, in partial fulfillment of
the requirements for the degree Doctor of Philosophy, College of Computing, Georgia
Institute of Technology (2005)
21. DIN EN ISO 13407: Human-centred design processes for interactive systems (1999)
22. Storf, H., Becker, M., Riedl, M.: Rule-based Activity Recognition Framework: Challenges,
Technique and Learning. Pervasive Computing Technologies for Healthcare, 2009.
PervasiveHealth 2009. 3rd International Conference on In Pervasive Computing
Technologies for Healthcare, 2009. PervasiveHealth 2009. 3rd International Conference on
(2009) 1-7
23. Muller, S., Santi, M., Sixsmith,A.: Eliciting user requirements for ambient assisted living:
Results of the SOPRANO project, eChallenges Conference 2008, Stockholm (2008)
59
