
PROCESS-ORIENTED INCIDENT REPORTING IN HEALTH CARE
ORGANIZATIONS
Web Application Architecture and Modeling Experiences
Martin Schmollinger
1
, Eric Stricker
2
, Tibor Bazlen
1
, Thomas Eßlinger
1
, Christopher R
¨
ohl
1
and Brian Walter
1
1
School of Informatics, Reutlingen University, Reutlingen, Germany
2
Department of Anaesthesiology and Intensive Care Medicine, University Hospital T
¨
ubingen, T
¨
ubingen, Germany
Keywords:
Process-oriented system architecture, Medical incident reporting, BPMN 2.0, REST web services.
Abstract:
In Germany more than 17,000 people die per year because of ”medical errors”, in the USA it is about 98,000.
The number of avoidable malpractice cases or major complications is about tenfold higher. Nearly everyone
will be a patient in a hospital sooner or later. A key concept to improve patient safety are modern, anonymous
adverse event reporting systems in hospitals. These are known as incident reporting systems. The introduction
of modern process-oriented technologies optimizes the efficiency of such systems and increases patient safety.
IT saves lives, if it is possible to improve the analysis of medical incidents and to accelerate the detection of
the underlying causes by optimizing the IRS processes. In this paper we present a generic process-oriented ar-
chitecture and its application for incident reporting systems in health care organizations. Further, we formulate
lessons learned concerning business process modeling and implementation for process-oriented architectures.
1 INCIDENT REPORTING IN
HEALTH CARE
Since the report ”to err is human” published by the
Institute of Medicine (IOM) (Institute of Medicine,
1999), it is well known that up to 98,000 people die
each year because of medical errors. In many coun-
tries medical errors are among the ten leading causes
of death (Kohn, 2006). The number of avoidable
major complications is about tenfold higher. Cases
with injury to the patient are only the tip of the ice-
berg. The avoidance of medical errors increases pa-
tient safety. Unfortunately, there is little knowledge
about the error mechanisms in health care. A main
reason for errors in medicine is the failure to ap-
ply medical knowledge in imperfect, real world con-
ditions of patient care and not the missing medical
knowledge itself (Rall and Gaba, 2005).
Incident reporting systems (IRS) facilitate the
continuous collection of data for a systematic analy-
sis. Presently available systems do not collect the nec-
essary amount and quality of data. The amount of un-
reported and therefore not systematically analyzed in-
cidents is estimated to be between 50% and 96% (In-
stitute of Medicine, 1999; Leape, 1994; Cullen et al.,
1995).
Furthermore, ten years after the before-mentioned
IOM report, medical IRS still have major problems to
induct a fast realization of useful recommendations.
Because the analysis of the incidents is not compre-
hensive enough, decisions are often made without suf-
ficient knowledge of environmental conditions and
various other factors. These quick fixes can have un-
intentional side effects and even worsen the situation
(O’Reilley, 2009). Reported incidents are a window
to the surrounding health care system (Vincent, 2006).
Looking into this window gives the chance to de-
tect dangerous constellations which may be the root
causes of the reported incidents. Sometimes such fac-
tors do not actually correspond directly to the reported
incident, but without this reporting no one would have
ever questioned the detected nuisance. Eliminating
the deeper problem behind the incident means to im-
prove the situation for the given incident and more-
over, for similar or dependant situations. In order to
reduce the risk of adverse events all underlying fac-
tors and their relations have to be observed (Leape
et al., 1991). The World Health Organization (WHO)
published guidelines for adverse event reporting and
learning systems (WHO, 2011). The most important
aspects are organizational integration, data security,
219
Schmollinger M., Stricker E., Bazlen T., Eßlinger T., Röhl C. and Walter B..
PROCESS-ORIENTED INCIDENT REPORTING IN HEALTH CARE ORGANIZATIONS - Web Application Architecture and Modeling Experiences.
DOI: 10.5220/0003775602190224
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 219-224
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

implementation of change requests and the establish-
ment of some type of learning system. Some char-
acteristics of successful reporting systems can also be
derived from Leape (Leape, 2002) and Cohen (Cohen,
2000): e.g. non-punitive, confidential, professional
analysis, timely, systems-oriented and responsive.
1.1 Patient Safety Information System
The T
¨
ubingen Center of Patient Safety and Simula-
tion (T
¨
uPASS) at the university hospital T
¨
ubingen de-
velops and administrates the interprofessional IRS Pa-
SIS (Patient Safety Information System) (Dieckmann
et al., 2006). PaSIS is widely accepted with more than
70 participating hospitals and about 30 rescue heli-
copter bases in Central Europe. More than 3000 inci-
dents have been reported. All reports undergo a four-
eye anonymization process by neutral domain experts
trained in incident reporting and using checklist pro-
tocols to prevent any lapses. After that the reports are
professionally analyzed in order to find the causes and
factors for the medical error. Within this process, it is
possible to pose questions to the anonymous reporter.
The result is prepared for the different user groups and
recommendations are derived from the analysis. The
implementation of the recommendations is supported
and evaluated throughout the system.
PaSIS is a classical web application based on
Apache, PHP and MySQL. The complete incident re-
porting process for each hospital beginning with re-
porting step, anonymization, posing questions to re-
porters, analyzing and suggesting recommendations
is hard wired in the program code. Each customiza-
tion of the system is associated with time-consuming,
error-prone manual programming. Moreover, it is not
possible to execute processes of different versions at
the same time. Changes to the process are very com-
plex, because the data of all pending processes have
to be adapted to the new one.
2 PROCESS-ORIENTATION IN
INCIDENT REPORTING
SYSTEMS
The success of an incident reporting system depends
on the optimal cooperation of all its stakeholders.
Stakeholders are all kinds of users (medical person-
nel, domain experts, quality managers of hospitals),
developers and administrators. Long-running pro-
cesses are common in medical incident reporting sys-
tems. Ideally, the process behind an incident report is
adapted to the corresponding hospital, because they
differ in size and organization. A precondition for
that is the cooperation between clinical personnel or
managers and IT specialists responsible for the IRS.
Business process management (BPM) technologies
and methodologies are the key to successfully ful-
filling this task. BPM is a systematic approach to
capture, arrange, document, measure, monitor and
steer automatic and non-automatic processes in order
to reach the goals of the organization (van der Aalst
et al., 2003; European Association of Business Pro-
cess Management, ). A business process management
system (BPMS) supports the BPM life cycle, which
consists of the four major steps: process design, sys-
tem configuration, process enactment and diagnosis
(van der Aalst et al., 2003). The life cycle supports
continual improvement of business processes. Mod-
ern approaches provide methods and technologies to
get business people naturally involved in the BPM life
cycle. First of all, graphical notations like OMG’s
Business Model an Notation (BPMN) (Object Man-
agement Group, 2011; White and Miers, 2008) can
be used to design process models without program-
ming skills. The resulting business process models
can be augmented by technical details ideally using
the same notation. The execution of the detailed pro-
cess model is done by a process engine that coordi-
nates user interaction with the running processes by
a web application (Ouyang et al., 2009). Although,
there is an increasing need in health care to support
patient-oriented processes, BPM technology is rarely
used. Especially for IRS web applications, the em-
bedding of process-oriented technologies has several
advantages over conventionally implemented web ap-
plications. Namely, improved transparency of IRS
processes, complete involvement of all IRS partici-
pants in the processes’s life cycle, easier maintenance
and extendibility, faster ”time to market” for individ-
ual IRS processes of new participating hospitals, flex-
ible change management, support of several process
versions per hospital and enhanced process monitor-
ing capabilities that help improving reaction times.
In (Schmollinger et al., 2011), we proposed a gen-
eral methodology to systematically incorporate pro-
cess oriented technologies into web applications. Fur-
thermore, we sketched a process-oriented target ar-
chitecture based on open source products and showed
how to implement processes with an adequate tool
chain using a simplified incident reporting process.
The used modeling strategy provides three types
of models. First, the strategic model. It describes the
main participants (user roles and systems) and the or-
der of their main activities. It disregards all the special
cases and exceptional or error conditions of the real
process. Second, the operative process model is much
HEALTHINF 2012 - International Conference on Health Informatics
220

more detailed than the strategic process model. It de-
scribes all operative tasks of all process participant
(human beings, as well as systems) and their relations
and dependencies. Third, the technical process model
contains all technical details and can be executed on
a process engine that is embedded in the web appli-
cation. As proof of concept, we realized a simplified
process (”happy path”) that gave us precious insights
and confirmed the proposed methodology.
Practical use showed two main drawbacks of the
proposed architecture. First, the integration of the
process engine into the web application is too com-
plex. The PHP application communicates with a
JEE web application using HTTP. The JEE applica-
tion uses the Java API of the process engine (JBOSS
jBPM (JBoss, 2011)) to communicate with the pro-
cesses. Further frameworks were necessary to realize
a seamless integration e.g. W3C’s XForms standard
was used to describe web forms and Orbeon was used
to render these forms. One objective of the process-
oriented approach is to simplify maintenance and ex-
tensibility. But the architecture we sketched was too
complex to meet this objective. The effort in man-
aging the architecture is too high and too many skills
are necessary to create new processes or to update the
current versions.
Another problem with the architecture is the use of
different process modeling notations for the design of
the business process and for executable technical pro-
cess model. jBPM works best with the native jPDL
notation. Hence, there is always an additional step of
translation, because the common process design with
the users is done with BPMN. In order to improve the
overall architecture, we propose the following two ac-
tions: first, use ”light-weight” integration of the pro-
cess engine into the web application using REST web
services (Fielding, 2000); second, use BPMN 2.0 for
the design and for the execution on the process en-
gine.
Concerning process modeling, the remaining
tasks were to turn the strategic model into an accu-
rate operative model. Then, the operative model itself
has to be turned into a technical process model that
can be executed on the process engine of choice.
In the following two sections, we show improve-
ments of the process architectures and lessons learned
in the area of process modeling in health care.
3 A PROCESS-ORIENTED WEB
APPLICATION
ARCHITECTURE
The Activiti-Project (Activiti, 2011) is an open source
BPM platform with a BPMN 2.0 process engine for
Java as its core. Furthermore, Activiti includes a
REST web service API to the engine that can easily
be used by web applications and therefore reduces the
complexity of the BPM integration into web applica-
tions dramatically. No additional user interface tech-
nology is necessary, it is completely up to the web
application how to display the process information.
This reduces the effort in customizing the application
for new modeled processes. The resulting new archi-
tecture for PaSIS is sketched in Figure 1. Besides
the engine, Activiti contains several tools supporting
the BPM life cycle, especially for modeling technical
(Eclipse designer) as well as non-technical business
processes (Activiti Modeler). Two databases are used.
The first one stores all information of the web appli-
cation such as login data. The Activiti database stores
process information and user data of running process
instances. After completing a process instance the
user data is transferred back to the PaSIS database for
archiving purposes.
Figure 1: A process-oriented web application architectue
using a process engine and REST web services.
As already mentioned, Activiti implements a
REST interface, which offers extensive possibilities
for controlling the engine. These include the start-
ing of processes, completing tasks and reading of data
from the process engine. Information is transferred
in the JavaScript Object Notation (JSON), which is
much simpler than XML and has a smaller grammar.
JSON objects were transferred into multidimensional
PHP arrays by native implemented PHP functions.
Vice versa, we used cURL functions to wrap informa-
tion, entered by the user of the web application, for
sending them to Activiti. For future reusability new
PHP functions were implemented, which simplify the
invocation of the built-in REST methods.
PROCESS-ORIENTED INCIDENT REPORTING IN HEALTH CARE ORGANIZATIONS - Web Application
Architecture and Modeling Experiences
221
4 MODELING EXPERIENCES
In this section, we want to address the task of model-
ing processes for the sketched architecture. It is out
of scope of this paper to discuss the process content
itself e.g. the details/tasks of incident reporting. Our
focus lies on the modeling methodology.
Due to the strategic model (see (Schmollinger
et al., 2011)), we have created a common understand-
ing of incident reporting in health care organizations
among the development team. This model helps to
understand the core of the process by ignoring com-
plex aspect like e.g. realizing 4-eyes principles, sev-
eral iterations of discussions between external experts
and hospital delegates or call backs to the anonymous
reporter. It is the task of creating the operative process
model to address all those details.
In order to model the operative process out of the
strategic model, we had to analyze the actual incident
reporting system and the interaction with the process
participants thoroughly. A successful strategy is to
model the view of each process participant separately
in a single pool. The pool representing the process
engine contains all tasks that are necessary to coor-
dinate the other process participants. In our case, we
defined three pools. One for the participating hospital
and within this pool one lane for the anonymous re-
porter and one lane for the quality manager. One for
the process engine (in the middle) and finally one for
the incident reporting organization with its experts for
deidentification and analysis. The message flows into
the process engine’s pool represent REST web service
calls from the web application to Activiti.
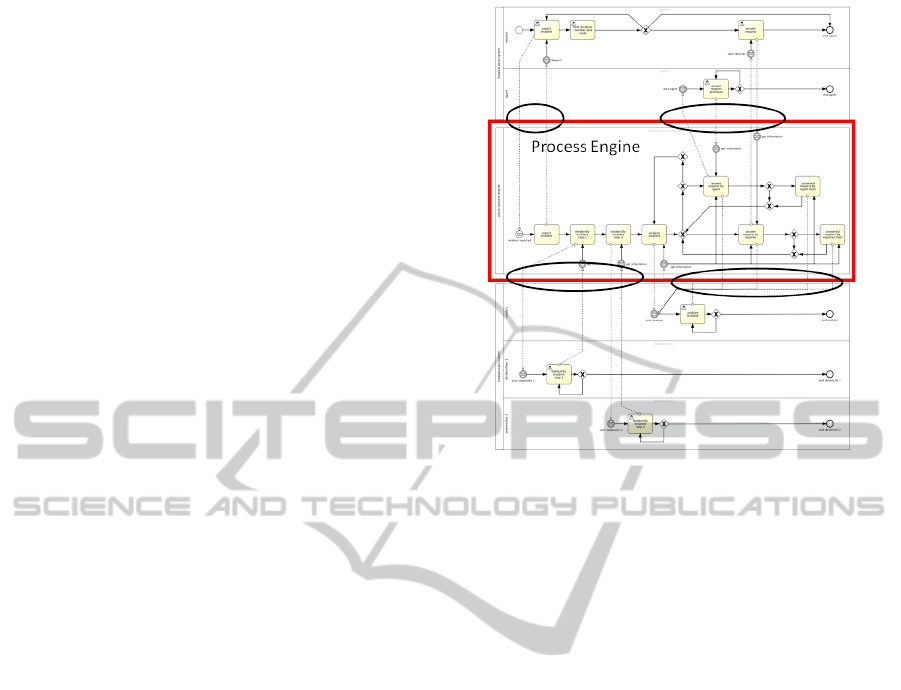
In general, the operative process model is always
huge and complex, because it represents a large part
of the system’s logic. Our resulting operative process
model consists of three pools integrating 6 swimlanes,
15 activities spread over the swimlanes, 11 gateways,
19 events and several sequence and message flows.
A precise description together with a complete illus-
tration is out of scope of this paper. We focus on
the modeling methodology and show the relation be-
tween the operative and the technical process model
(see Figure 2).
Ideally, the process engine pool is very close to
the technical process model that is finally deployed to
the process engine of the process-oriented architec-
ture in order to facilitate the realization of the BPM
round trip. The resulting technical process model is
shown in Figure 3. It can be easiliy seen that in our
case the technical process model really looks simi-
lar to the process engine pool in the operative model.
This model is optimized for execution in the Activiti
BPM engine. Each human task is assigned to a pro-
Figure 2: Overview of the operative process model of the
entire incident reporting process. The pool in the middle
emphasized by the rectangle represents the process engine.
This part of the operative model is the base for the imple-
mentation of the technical process model that is executable
on the target process engine. The ellipses mark message
flows between the process engine pool and the other pools.
The message flows have to be implemented by service calls
from the web application to the process engine.
cess participant as defined in the operative model. In
addition all elements which were not required, such
as notice-elements, were deleted because the engine
does not need them. Gateways within the sequence
flow use process variables (most of their values are
generated by user interaction) in order to decide the
route of the sequence flow. The experiences made led
to the following lessons learned:
1. Optimization and Adaption of the Original
Web Application is Recommended. Although
the original web application might be instrinsi-
cally process-oriented, it is very complex to ex-
tract these processes. In general most applications
grew historically and include several workarounds
or bypasses for special cases and customers.
Sometimes these construct are de facto not used
anymore. Modeling all these constructs would
lead to even more complex models without an ad-
ditional benefit. Hence, we recommend to clean
up and simplify the system while modeling. It is
worth questioning suspicous constructs in order to
otimize the new models.
2. Redefinition of Authorization. Process-oriented
systems need a clear mapping of tasks to process
participants. Tasks are assigned to roles. A role
HEALTHINF 2012 - International Conference on Health Informatics
222
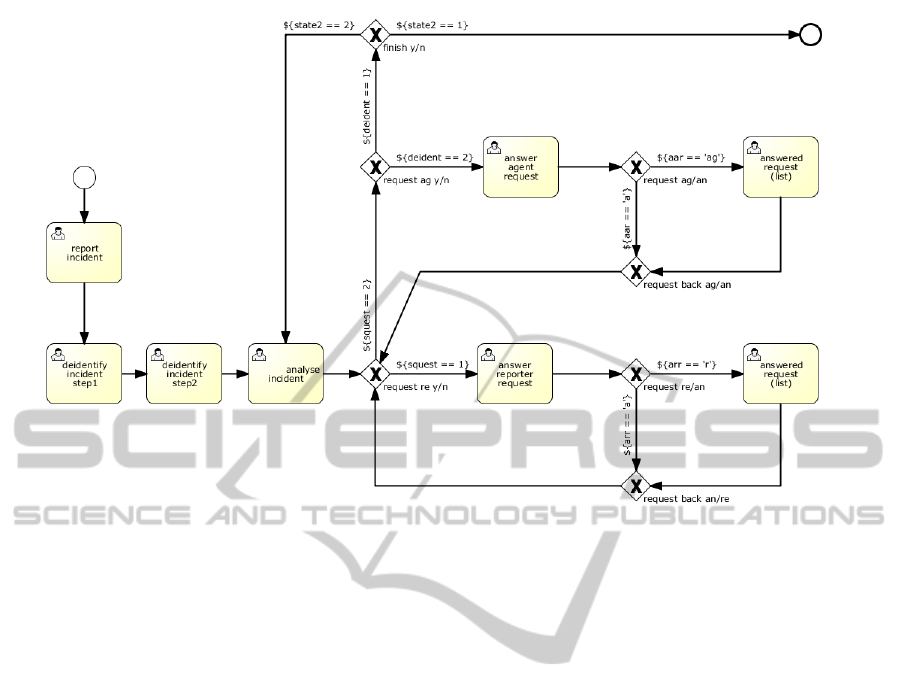
Figure 3: Technical process model that is executable on the process engine of Activiti. The labels at the outgoing sequences
at the gateways are conditions using process variables. The values of these variables are generate by user input during the
process execution. The model mainly consists of human tasks that are executed by service calls from the web application.
The participant’s todo-lists in the web application can be updated by reading the actual state of the process instance.
can be taken by single users or user groups. There
are web application that have a good authentifi-
cation, but a very crude authorization. In these
case, it is not the system that ensures that the
right people do the right things at the right time,
but the organization of the daily work (they know
themselves what they are allowed to do or not).
Without a distinct authorization, the application
is more flexible because nearly everyone can do
everything. But on the other hand side, it is not
possible to manage accurate todo-lists and there
is always the danger of misusage. Therefore, we
recommend to redesign the authorization system
while building up a process-oriented system.
3. Use of Modeling Conventions. During process
modeling it happens that the same construct can
be modeled in several ways. In order to receive
similar models over time it is recommended to de-
fine modeling conventions, use process patterns or
general accepted guidelines like (Mendling et al.,
2010).
4. Know your Process Engine. There are a lot
of process engines around that pretend to be a
BPMN 2.0 compatible engine. BPMN 2.0 is a
very mighty standard with a lot of new constructs
and symbols. If you want to use all its features,
you first have to check whether your engine does
really support them. Furthermore, if it supports
it, you have to check how it is implemented (e.g.
parallel gateway: is it really executed in parallel?).
In theory a BPMN 2.0 model should run on every
BPMN 2.0 process engine. Unfortunatelly, this is
not true. You have to consider the capabilities of
your engine while modeling the operative and of
course technical process model. Otherwise, there
will be a high probability that you can not reuse
your operative model for the design of the tech-
nical model. Although this the wrong way, your
engine defines the BPMN subset you can use for
your models. Hence, we recommend to define this
subset of BPMN before modeling.
5 CONCLUSIONS AND FUTURE
WORK
Intrinsically process-oriented web applications, like
incident reporting systems in health care are usually
implemented conventionally (e.g. LAMP/WAMP).
The processes are implicitly realized in the system.
This leads to major disadvantages concerning trans-
parency, maintainability and extendibility. The cus-
tomization of processes is very time-consuming and
error-prone. Even if the current process engines are
PROCESS-ORIENTED INCIDENT REPORTING IN HEALTH CARE ORGANIZATIONS - Web Application
Architecture and Modeling Experiences
223

not able to handle the full BPMN 2.0 notation, BPM
methodologies and technologies have a high potential
to improve this situation. In this paper, we presented a
process-oriented architecture that integrates a BPMS
into classical web application using REST web ser-
vices and BPMN 2.0. We implemented the architec-
ture for an incident reporting systems in health care.
Further, we showed how to model processes for the
given architecture using incident reporting processes
as an example and derived several lessons learned
from it. The presented approach has great potential,
but has to pass the practice test. Besides the future
lauch of a production system, further open questions
arised.
After establishing process-orientation in our in-
cident reporting system, we want to exploit the new
monitoring capabilities of the process-oriented archi-
tecture. Future work will be about the design of a
management cockpit for incident reporting with the
goal to improve reaction times and the quality of the
analysis.
The exploration of processes in web applications
is a very time consuming task. Process mining is a
research area that surveys methodologies and algo-
rithms with which processes of applications can be
detected out of log-Files. We are about to realize a
software infrastructure that helps collecting process
relevant data of clinical web applications in a con-
venient way over time. Using process mining tech-
niques on this data collection promises to accelerate
the exploration of business processes that are implic-
itly realized by clinical web applications.
Although a predefined incident reporting process
is a good orientation for the process participants, in
some cases it is necessary to extend or modify the
process dynamically. The actual BPM technology ap-
proach does not support these so called ad hoc pro-
cesses. We will survey how social media technology
can improve this aspect.
REFERENCES
Activiti (2011). Bpm platform. http://www.activity.org/.
Cohen, M. (2000). Why error reporting systems should be
voluntarily. BMJ 2000, pages 728–9.
Cullen, D., Bates, W., Small, S., Cooper, J., Nemeskal, A.,
and Leape, L. e. a. (1995). The incident reporting sys-
tem does not detect adverse drug events: A problem
in quality assurance. Joint Commission Journal on
Quality Improvement, (21):521–8.
Dieckmann, P., Stricker, E., and Rall, M. (2006). The role
of incident reporting systems in the evaluation of med-
ical devices. In Proceedings of the Annual Meeting of
the International Ergonomics Association.
European Association of Business Process Management.
Business Process Management Common Body of
Knowledge - BPM CBOK: Guidelines for Business
Process Management. EABPM.
Fielding, R. (2000). Architectural styles and the design of
network-based software architectures. Doctoral dis-
sertation, University of California, Irvine.
Institute of Medicine (1999). To err is human: building
a safety health system. Washington DC: National
Academy Press.
JBoss (2011). jbpm. http://www.jboss.com/products/jbpm/.
Kohn, L. T. (2006). Building a safer health system. Wash-
ington DC: National Acad. Press.
Leape, L. (2002). Health policy report. patient safety. re-
porting of adverse events. NEJM, pages 1633–8.
Leape, L., Brennan, T., and Laird, N. e. a. (1991). The na-
ture of adverse events in hospitalized patients: Results
from the harvard medical practice study i & ii. New
Engl. J. Med., I & II:324, 370–384.
Leape, L. L. (1994). Error in medicine. JAMA 1994, pages
1151–7.
Mendling, J., Reijers, H., and van der Aalst, W. (2010).
Seven process modeling guidelines (7pmg). Informa-
tion and Software Technology, 52(2):127–136.
Object Management Group (2011). Bpmn 2.0 specifica-
tions. http://www.omg.org/spec/BPMN/2.0/.
O’Reilley, K. (2009). Patient safety improving slightly,
10 years after iom report on errors. http://www.ama-
assn.org/amednews/2009/12/28/prsb1228.htm.
Ouyang, C., Dumas, M., van der Aalst, W., ter Hofst-
ede, A. H. M., and Mendling, J. (2009). From busi-
ness process models to process-oriented software sys-
tems. ACM Transactions on Software Engineering
and Methodology, 19, 19(2).
Rall, M. and Gaba, D. M. (2005). Millers’s Anesthesia,
chapter Human Performance and Patient Safety, pages
3021–3072.
Schmollinger, M., Iwanowski, M., Kußmaul, T., Schwart-
ing, D., Stark, J., Stricker, E., and Rall, M. (2011). A
challenge for healthcare web applications: From data-
to process-orientation. In Proceedings of the Inter-
national Conference on Health Informatics HEALTH-
INF 2011. SciTePress.
van der Aalst, W., ter Hofstede, A., and Weske, M. (2003).
Business process management: A survey. In In Pro-
ceedings of the International Conference Business
Process Management 2003. Springer Verlag.
Vincent, C. (2006). Patient safety. Edinburgh: Elsevier.
White, S. and Miers, D. (2008). BPMN modeling and ref-
erence guide. Understanding and using BPMN - de-
velop rigorous yet understandable graphical repre-
sentations of business processes. Future Strategies
Inc., Lighthouse Point.
WHO (2011). World alliance for patient safety: Draft
guidelines for adverse event reporting and learning
systems. http://www.who.int/patientsafety/events/05/
Reporting Guidelines.pdf.
HEALTHINF 2012 - International Conference on Health Informatics
224
