
CordiAAL: Enhanced Motivation for Cardiological Ergometer Training
through Virtual Groups in Virtual Worlds
Israfil Akman
1
, Rafael Bielen
1
, Henning Br
¨
ummer
1
, Egor Kudrjaschow
1
, Stefan Tschentscher
1
,
Oliver Dohndorf
1
, Heiko Krumm
1
, Jan-Dirk Hoffmann
2
, Anke Workowski
2
and Detlev Willemsen
2
1
Lehrstuhl Informatik IV, TU Dortmund University, Martin-Schmeißer-Weg 18, 44221 Dortmund, Germany
2
Sch
¨
uchtermann-Schiller’sche Kliniken, 49214 Bad Rothenfelde, Germany
Keywords:
Ambient Assisted Living, Bicycle Ergometer, Cardiac Disease, Preventive Programme, Secondary Cardiac
Prevention, Immersive Virtual Reality.
Abstract:
The project CordiAAL purposes the goal of developing a training system for patients with cardiovascular
diseases. The first aim is to reduce the anxiety of overexertion by using a continuous monitoring of vital
parameters and the second is to increase the patients’ motivation according to a moderate physical activity by
the virtual environment of the system. The training can be done alone or in common with several patients in a
virtual group, regardless of the patients’ location. When grouped together, the performance of the individual
patient is aligned, so that patients with different fitness levels are able to work together. The evaluations
revealed that the increase in motivation could be achieved by training in the virtual environment in virtual
groups.
1 INTRODUCTION
Cardiovascular diseases are the leading causes of
deaths in industrialized countries. In Germany
there are 40.2% of all deaths based on cardiovascu-
lar diseases (CVD) (Statistisches Bundesamt, 2011).
Mainly elderly people, 65 years and more, die be-
cause of these diseases. In 2011 the mortality rate of
over 65 year old people was 92% (Statistisches Bun-
desamt, 2011). Around 15% of medical expenses,
with 37 billion euros, were spent for these morbidities
for the care, treatment, prevention and rehabilitation
in Germany 2008 (Statistisches Bundesamt, 2008).
These facts increase the meaning of primary and sec-
ondary prevention of people with CVD. Up to 90%
of the cardiovascular morbidities are caused by the
cardiovascular risk factors: dyslipidemia, hyperten-
sion, diabetes mellitus, obesity, distress and physical
inactivity (Yusuf et al., 2004). Large epidemiolog-
ical studies and meta-analyzes of randomized, con-
trolled studies (evidence-based medicine, level IA)
have shown that regular physical endurance activity
is associated with a reduction of cardiovascular mor-
bidity and mortality (Nocon et al., 2008). There-
fore physical inactivity is considered the most impor-
tant modifiable risk factor (Bjarnason.Wehrens et al.,
2009). According to results of the National Health
Survey only 41% of German adults (45 up to 65 years
old) are more than 2 hours physically active per week,
about 38% in this age group do not exercise and
around 48% of German people older than 65 years
do not exercise (Gesundheit in Deutschland aktuell
– Telefonischer Gesundheitssurvey (GEDA), 2010).
The fitness level of a person is correlated with the
exercise outcome. The life expectancy of ”Fit Peo-
ple”, people with a high performance, is higher than
for people, who do not perform exercises regularly
(Sattelmair et al., 2011). The risk of a cardiac event
is reduced through regular physical activity by posi-
tive physiological adaptations (Lee et al., 2003) and
the major modifiable risk factor is physical inactivity
(Balady et al., 2007).
Because of this background cardiac patients train
their physical activity during cardiac rehabilitation. It
is largely documented that the traditional rehabilita-
tion after discharge from hospital is efficient and ac-
knowledged generally. Several studies confirm that
the cardiac rehabilitation improves the functional ca-
pacity and psychosocial resources. But this success
is not a long term effect (Kotseva et al., 2009), af-
ter one year, the output level is usually reached again.
This lifts the obligation and responsibility of every in-
dividual to make secondary preventive care. In Ger-
many, the secondary prevention of heart patients pro-
78
Akman I., Bielen R., Brümmer H., Kudrjaschow E., Tschentscher S., Dohndorf O., Krumm H., Hoffmann J., Workowski A. and Willemsen D..
CordiAAL: Enhanced Motivation for Cardiological Ergometer Training through Virtual Groups in Virtual Worlds.
DOI: 10.5220/0004797300780089
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 78-89
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

vides outpatient heart groups only. However, only 13-
40% of all CVD patients do participate (Bjarnason-
Wehrens et al., 2006). Reasons for this lack are that
these groups are temporally inflexible and not nation-
wide available. In addition, there is a high drop-
out rate of new members (Bjarnason-Wehrens et al.,
2006). IT-based systems providing Ambient Assisted
Living functions can be a solution. Therefore the
chair IV of the Technical University of Dortmund
and the Sch
¨
uchtermann-Schiller’sche Kliniken in Bad
Rothenfelde developed a virtual biking application as
a part of a two-semester project, which should moti-
vate patients to do exercises regularly. The CordiAAL
project is an attempt to break the monotony of regu-
lar ergometer training sessions with virtual adventure
components and to sustain the motivation and adher-
ence of CVD patients. Healthcare professionals and
computer science students developed a software for
a bicycle ergometer in combination with a PC and
wireless sensors (ECG, respiration rate, body temper-
ature, oxygen saturation, blood pressure). The system
is integrated into an internet based community, called
RehaWeb, a special website for heart patients, with
a combination of social networking features, edito-
rial contents as well as mobile support and monitor-
ing (Dohndorf et al., 2012). The user can go by bike
through a virtual environment with a movable control
and a virtual reality head-mounted display (HMD),
that the session is as real as possible. The bike con-
sists of a heart-rate controlled load system. The car-
diologist can define individual corridors for each vi-
tal parameter and can set the optimal load for each
user to prevent overexertion and underexertion. The
training can be fulfilled online in a group of up to six
users with different performances or alone in a single
modus. Users can virtually train together without ac-
tually being together. Thereby heart patients will be
motivated through the advanced sensor-based gaming
environments to do exercise. With the defined limits
of the vital data, the users can loose their anxiety of
exercise and get more body awareness. For the do-
cumentation of the training and vital data a report of
each session is generated. The CordiAAL system can
support a sustained prevention and rehabilitation of
people with CVD. The CordiAAL project is based on
the results of ”OSAMI - Open Source Ambient In-
telligence Common”, which was funded by the Fed-
eral Ministry of Education and Research in Germany
(ITEA2) (Busch et al., 2009). This paper will intro-
duce with related works, discuss the requirements and
possible solutions to the system afterwards. The fol-
lowing section will describe the architecture of the
system in detail. Finally, first evaluation results of the
system will be presented.
2 RELATED WORK
IT-based systems, that motivate persons to do sports,
can be categorized according to their nature as immer-
sive and non-immersive systems, and regarding to the
kind of environment where they are used. Some sys-
tems can be used at home, but others are made to be
used in physical therapy.
One non-immersive system usable in every envi-
ronment is the Geosocial Network (Boulos and Yang,
2013). This system requires a GPS and an internet-
capable mobile phone. The application defines a tar-
get in the local area, where the user should travel to.
At an easy level the target is clearly defined by GPS
coordinates, but at a more difficult level the coordi-
nates are hidden by small puzzles. When the user
reaches the target, it is recorded in his profile and
more challenges are unlocked. The profile of each
user is also available in a web portal and is visible
for other players. The training aspect of the Geoso-
cial Network is based on the hiking of the users,
whereas the achievement of objectives and the com-
parison with other players serve an enhanced motiva-
tion. Other examples of such systems are CodeRun-
ner
1
or Dokobots
2
.
The Wiihab system (Anderson et al., 2010) is im-
mersive and made for physical therapy. It is designed
for patients who have restricted moving abilities. This
system requires a Personal Computer, a Wii Balance
Board and a Wii Mote. The Wii Mote is a video
game controller with a built-in motion sensor, the Wii
Balance Board measures the weight and the balance
of the patient. The Wiihab system has five built-in
games. Every game trains a different aspect, like the
balance of the body or the accuracy of the hand’s
movements. During a game session the training is au-
tomatically adapted to the patient’s health status. Af-
ter every session, the patient gets feedback about his
training success. So, the Wiihab system increases mo-
tivation for rehabilitation training by playing games
and the comparison with other players.
Furthermore, the Kinect system realizes a sensor-
based gaming environment. Similar to the Wii, the
Kinect system motivates the users playfully to per-
form physical activities. This system is immersive
and can be used in every environment. The Kinect
is basically a camera which detects movements of
the body. The user itself is the input device for a
video game. That is unique and increases the im-
mersive factor and hence the motivation. Examples
of immersive and physical activity promoting video
1
http://www.coderunnergame.com/
2
http://www.dokobots.com/
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
79

games are Your Shape
3
or UFC Personal Trainer
4
.
These games have certain exercises, training different
parts of the body and recording vital data during the
training.
A very prominent example of an immersive
system, only usable in hospital-like environments, is
the game Re-Mission (Lampert et al., 2009). It is di-
rected to children, who have cancer and aims at in-
fluencing the behavior and attitude of young patients
positively to their disease. The game was created by
Games for Health
5
. This organization has the objec-
tive to motivate patients’ physical activities and hence
prevent illness and disease with the help of video
games. In this game the patient fights against the dis-
ease cancer, in particular against tumors and similar
signs of cancer using various weapons.
3 REQUIREMENTS AND
SOLUTION APPROACHES
In order to serve its purpose as an aid in the prophy-
lactic and rehabilitation phase the envisaged project
CordiAAL has to meet following social, technical and
medical requirements:
Social Requirements
Easy usage of the Application: Because the pri-
mary target user group consists of elderly patients
which usually have little experience in dealing
with modern media, the user-friendliness is of
great significance. We take up this challenge
by sticking to the five rules as described in
(Caprani et al., 2012, p. 101). In respect of these
rules, we firstly ensure a fast running system
and secondly realize a very intuitive operation of
the application, where, for example choices are
limited in order not to confuse the user. Thirdly,
the guidance through the application is very clear
so that no ambiguities are given. Not least of all,
the usage is evaluated intensively. An easy usage
of the modified RehaWeb website is guaranteed,
since it was evaluated for the original version
(Dohndorf et al., 2012), and the extensions are
maintaining the original RehaWeb principles and
styles.
Building Trustfulness: In the sensitive area of me-
dical applications, the mediation of trust is a nec-
essary prerequisite with respect to a high user ac-
3
http://www.ubi.com/DE/Games/Info.aspx?pId=10769
4
http://www.golem.de/1104/82633.html
5
http://gamesforhealth.org/
ceptance. For that purpose, the users are informed
about the relevant issues of data security, safety
and data privacy. In the medical field the analy-
sis of training sessions by medical professionals
increases trust.
Increasing Motivation to Secure Long-term Use:
Patients use to neglect their training in case of
a motivation lack (Shahsavari et al., 2012). We
focus on that with the main feature of CordiAAL,
the group training mode, which keeps the mo-
tivation on a high level. Boredom is prevented
through a common training with like-minded
patients. Not least of all, the HMD and the voice
chat are conducive to this. Moreover monotony
does not arise due to the existence of several
maps.
Reduction of Fears: As it is generally known, pa-
tients with a cardiac disease commonly have to
cope with fears (Eifert et al., 2000). Thus, the
software CordiAAL pursues the goal of reducing
these fears in several ways. Technically, thresh-
olds for the heart rate, defined by medical profes-
sionals with respect to the health level of the pa-
tients, are used in each training session. Further-
more the training load during a training session
is adapted instantly according to the current heart
rate so that the risk of a further cardiac event dur-
ing the training is minimized.
Socially, the user gets in contact with like-minded
patients that suffer from a similar health issue,
which helps to distract the user’s fears. Further-
more, the training is not felt to be a training, in-
stead it is felt to be a game.
Technical Requirements
Achievement of Data Security and Privacy: We
extend the RehaWeb project which already en-
sures these requirements. Our extension contains
the web interface for the cardiologist where he
can define and adjust vital thresholds for a patient
and a detailed web statistic for each training. The
statistics can only be accessed by authorized per-
sons.
Recording of Vital and Load Parameters: The vi-
tal data have to be delivered from the body sensors
to the client software. These data are the basis
for the dynamic ergometer load control system.
The vital data used in CordiAAL comprise the
ECG, the respiration rate, the body temperature,
the SpO2 level and the blood pressure.
Controlling Functions and Dynamic Group
Control: The load and the RPM of the ergometer
HEALTHINF2014-InternationalConferenceonHealthInformatics
80
define the speed of the virtual bike. The load is in
turn influenced by the virtual world environment,
e.g. the gradient or the ground character. During a
group training, patients must have the possibility
to continue the training within their group even
if they have a lower fitness level compared to
other group members. Therefore we developed
a corresponding load controlling algorithm: the
dynamic group control. During a group training
this provides a regulation of the ergometer load
of a patient in a way that the patient is capable
to work with a higher RPM, since the load is
decreased when his health status turns critical.
Thus, the patient is able to stay virtually near to
the group cycling with a lower load but a higher
RPM, and therefore a higher velocity, whereas
other patients’ load and RPM may vary.
Real-time: In order to create a sufficiently realis-
tic virtual environment during the cycling within
CordiAAL we have to meet real-time constraints.
The rendering during a training shall not introduce
significant delays, even during a group training,
where the other bicycles of the participating pa-
tients have to be rendered also. So, the connection
must not slow down the virtual training. These
constraints also have to enable the mentioned con-
trolling functions. Therefore we use Unity3D for
rendering which works well with modern comput-
ers. In addition the position data of group mem-
bers is communicated periodically using small
UDP-messages.
Medical Requirements
Prophylactic and Rehabilitation Measure: A suf-
ficient training effect must be guaranteed. We
achieve this goal by providing several maps for
virtual training environments, where each of them
is categorized by a difficulty level. This leads to
an optimal training for the patients with respect
to their fitness level. Moreover the load control
supports efficient and risk-reduced training. This
results in improving the patients’ sporting perfor-
mance as well as their state of health.
Recording of Vital Data: For the acquisition of
physical constitution in the course of cardiac re-
habilitation and prophylaxis a broad spectrum of
medical sensors is supported. They monitor the
most important medical data, the heart rate, the
respiration rate, the body temperature, the SpO2
level and the blood pressure.
Analyzing and Visualizing Vital Data: The record-
ed vital data have to be analyzed by the
application in order to control the ergometer load.
The data have to be visualized on the screen.
In addition, the vital data are also visualized in
RehaWeb in a much more detailed way. This en-
ables the cardiologist to examine these data during
the training phase of each patient and therefore
plan the next training sessions.
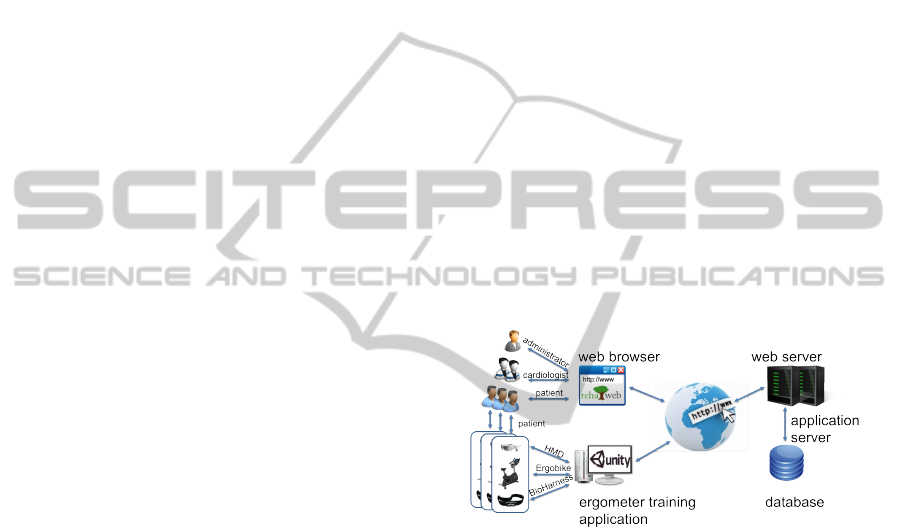
4 ARCHITECTURE
The project CordiAAL is based on a typical
client/server system (see figure 1). On the one hand
a web server with database access runs on the server-
side. This server is responsible for the requests of the
RehaWeb community while the data access is realized
via a RESTful-API (Pautasso et al., 2008). On the
other hand an application server acts as a communica-
tion interface between the different ergometer training
applications. On this application server the vir-
tual group information is processed via the position-
tracking application as well as the real-time commu-
nication via the voice chat application.
Figure 1: System architecture of the project CordiAAL.
The client-side consists of three different groups
of actors that interact with the system. Firstly the
administrator realizes both the administration of each
patient and the maintenance of the RehaWeb website.
The cardiologists are able to define or to adjust vital
parameters of their patients. Moreover, in RehaWeb
they can supervise the recorded statistics. The pa-
tients immerse in the virtual world by using the
ergometer and the HMD and are able to perform
a virtual group training. Furthermore they can use
RehaWeb’s social network function in order to find
out virtual routes or arrange a virtual group training.
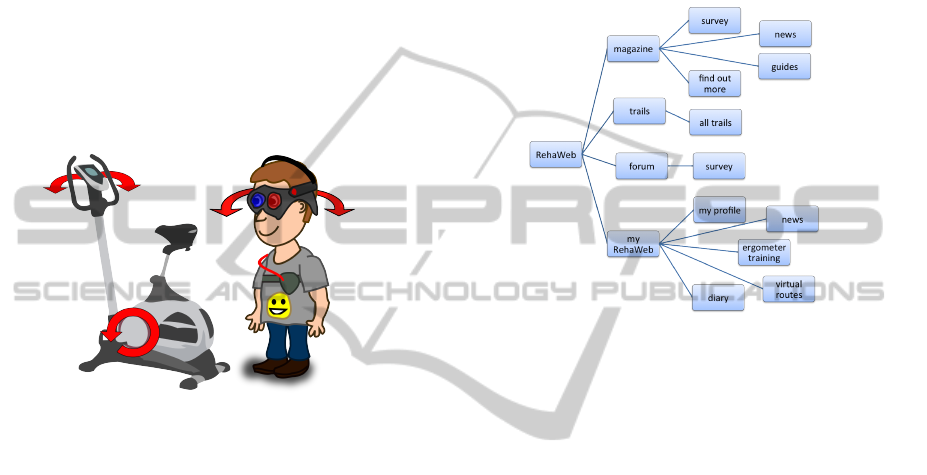
The integrated devices comprise the virtual reality
headset for displaying the immersive 3D world as
well as a bicycle ergometer for controlling the load
and a harness for recording the vital data (see fig-
ure 2). All of these components define a cyber-
physical system (CPS) (Lee, 2008). In such systems
the strict separation between the real and virtual world
becomes neutralized. The physical environment gets
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
81
recognized by the introduced sensors and is mixed
with parameters of the virtual reality. The obtained
information is processed and thus the physical envi-
ronment is influenced correspondingly. For instance
the revolutions of the pedals and the movement of the
steering wheel control the velocity and the direction
of the player respectively. On the other hand a moun-
tain or bad ground covering in this world causes a
higher adjustment of the ergometer’s load, but always
in consideration of the defined thresholds. The vital
parameters ensure medically appropriate adjustments.
Thus, this CPS combines the patient, the ergometer
control and the Unity3D game engine to a virtual en-
vironment, that facilitates a group training and adjusts
the individual performance levels.
Figure 2: Sensors environment of the system CordiAAL.
4.1 Social Network
The RehaWeb system pursues the goal of motivat-
ing cardiac patients for sustainable training. Virtual
group trainings on selected virtual 3D worlds can be
planned in the RehaWeb community together with
friends. The collected data are transmitted to the
RehaWeb server and are reviewable there in the form
of a training diary for both the patient and the medi-
cal staff. The patient is able to talk with other patients
about the development of his own performance and
other prevention-relevant topics in the forum.
The Architecture of the social network RehaWeb
consists of two layers. The first one comprises the
server-side. The server component has been designed
with a service-oriented and layered architecture. The
Tomcat application server contains the community
software as a Web2.0 user interface which is con-
nected to a MySQL database. The server provides
central storage and processing of all data. The access
is provided via a RESTful-API. The second layer con-
sists of the user’s web browser. Java-ServerFaces 2.0
is used in order to generate dynamic HTML code.
The Structure of the web portal RehaWeb is con-
ceived hierarchically as a tree structure. The top level
of the web portal is called the root. It is followed by
the level of the main navigation and its subnavigation.
In RehaWeb the level of the main navigation is repre-
sented as a horizontal bar above the green strip. The
further sublevels are displayed as a subnavigation in
the left column (see figure 3).
Figure 3: Portal structure of the website RehaWeb.
4.2 Communication
The CPS CordiAAL shows three types of communi-
cation. These are described in the following.
The first one is the web communication. The com-
munication between the web browser and the server is
based on HTTP/HTML.
The second type is the access to the services of the
server. These services are composed of the access,
processing and storage of all necessary data before
and after the training. The services are designed in
respect of REST principles (Fielding, 2000). They are
stateless and encapsulate every communication with
the database. Each service class is responsible for one
type of resource and provides methods according to
the CRUD principle (Novick, 2008). JSON messages
as the transport format are transmitted over HTTP.
The third type regards the time critical commu-
nication between the ergometer training applications.
For the realization of a virtual group training, the
current data concerning each patient’s current state
within the virtual world has to be exchanged via the
position-tracking application. For instance the pa-
tient’s ID and his position vector are transmitted. An-
other aspect concerns the audio communication be-
tween the patients of a group, realized by the voice
chat application. On the application-side the open
source .NET Audio and Musical Instrument Digital
HEALTHINF2014-InternationalConferenceonHealthInformatics
82
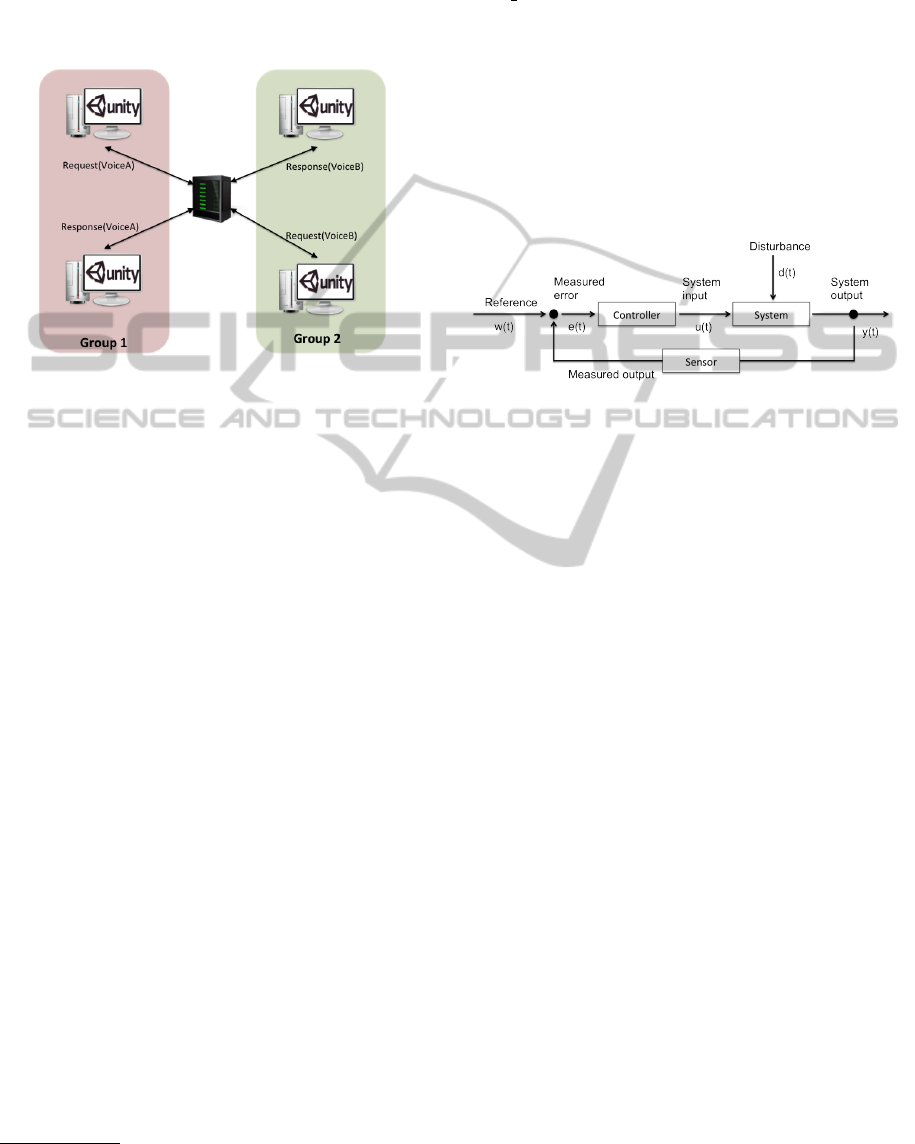
Interface (MIDI) library NAudio
6
has been used to fa-
cilitate a data stream. The audio samples are transmit-
ted to the voice chat application over UDP messages
and forwarded to the members of the group (see fig-
ure 4).
Figure 4: Voicemail distribution in different groups.
4.3 Training
The training is executed either as a single training or
as a group training. The challenge of this work is to
perform a training in virtual groups and the medical
load control of different patients. These aspects are
explained in the following.
Medical Monitoring
The following data are collected for the medical su-
pervision:
• ECG
• Respiration rate
• Body temperature
• SpO2
• Blood pressure
For the analysis of the SpO2 and blood pressure
data we make use of the Corscience NiBP2010 sen-
sor. The sensor communicates via an USB interface
with our system. Moreover the Zephyr BioHarness3
sensor, which enables a precise recording of the vital
parameters is used. The BioHarness3 communicates
via a Bluetooth interface.
Load Control
Enabling the individual control of each patient’s load
within a group training needs to deal with several sen-
sors and a load control algorithm.
6
http://naudio.codeplex.com
Sensors & Actors: The ergometer is the central en-
tity for controlling the intensity during the training.
Within our system we have used the ergometer
Ergo bike2000 of the company Daum Electronics.
Via a RS232 interface data can be exchanged between
the ergometer and the PC. These data are the cur-
rent speed, the RPM and the load data to control the
ergometer. The handle bars are modified in a way that
they are rotatable and a realistic steering is achieved.
Controlling One Person: The load control for one
person is based on a typical control loop (Schulz,
2007) (see figure 5).
Figure 5: Control circuit of the load control.
The regulation monitors the current heart rate
value (y(t)) and compares it with the desired value
(w(t)). Thus, disturbances (d(t)), for example slopes
and overloads of the patient, are recognized and com-
pensated (u(t)). The compensation is achieved by re-
ducing or increasing the load.
Controlling a Virtual Group: In order to support
virtual groups of patients with different fitness levels,
the group control reduces the load of low fitness level
patients. In detail, this means that a group member
is not outpaced by the others due to his own lower
fitness level. He has the possibility to cycle virtually
near to the others. The load (d(t)) of a patient whose
heart rate gets into the threshold area is reduced so
that this patient is able to train with a higher RPM
under less effort to retain the group velocity within
the virtual world.
Therefore patients who have undergone a load re-
duction are able to cycle with the same RPM as be-
fore. Thus, this mechanism enables the weaker pa-
tients and the ones with a lower fitness level to stay
virtually near the other group members.
Immersive Game Environment
For the purpose of realizing an immersive world we
make use of a virtual reality head-mounted display as
well as of a game engine for displaying the 3D world.
Designing the application as a distributed system en-
ables multiplayer games over the internet.
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
83
Virtual Reality Head-mounted Display: To serve
its purpose as a motivational tool and to improve the
display quality of the 3D world a virtual reality head-
mounted display is integrated into the system, in de-
tail the Oculus Rift (developer version) is used. The
head-mounted display has got a large field of vision
and fast head-tracking sensors. The Oculus Rift pro-
vides a DVI and a HDMI input interface as well as
an USB interface for transferring tracking data to the
ergometer training application.
Unity3D: Unity3D is a complete development en-
vironment, designed to develop video games and
rendering. The target platforms are Windows,
Mac OS X, video game consoles and mobile phones.
The development environment includes a visual edi-
tor, the C# editor Mono and different modules.
The main task of the visual editor is to create and
manipulate 3D objects. The 3D objects can be created
in programs such as Blender or Maya 3D. For details,
logic and behavior components can be attached to 3D
objects. Components define objects’ properties like
sound, look, material, texture, behavior and physical
properties. Own components can be written in C#,
JavaScript and Boo.
For the display of 3D objects Unity3D makes use
of its own 3D engine. The 3D engine also handles
the optimization of the scene so that the drawing is
efficient.
For music and sounds Unity3D uses the FMOD li-
brary. Input devices such as mouse, keyboard and
joystick can be integrated directly into Unity3D.
Unity3D is free, but there is also a pro version. The
pro version allows to write components in C++ and
has some additional improvements in the 3D engine,
the pro version supports dynamic light, shadow ef-
fects and more efficient rendering.
With Unity3D version 3.0 comes an Asset Store
in which resources uploaded by other users, for in-
stance 3D models, textures and sounds, can be bought
or downloaded for free.
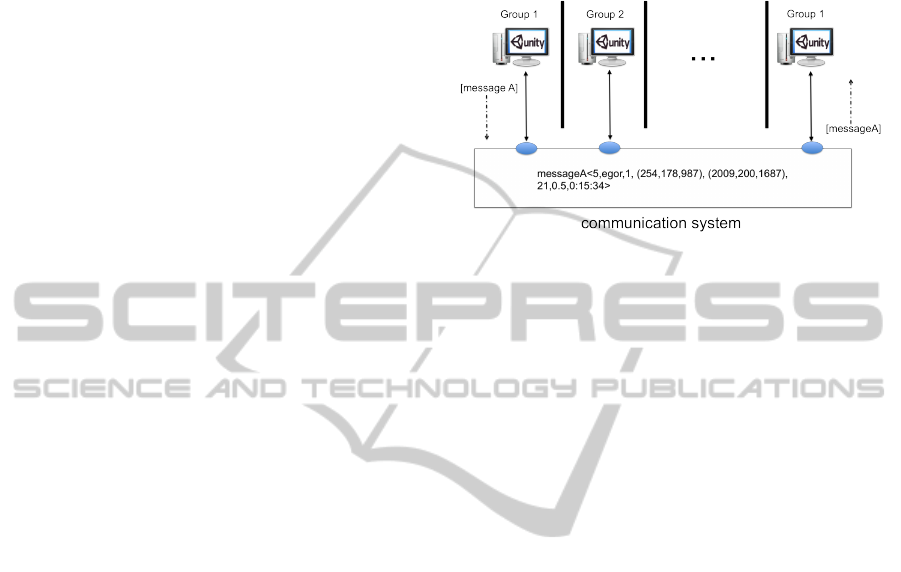
Virtual Group Dynamics: In the single training
mode we have local access to the static 3D world.
This mode requires no further information about other
players. There is only communication to the server
before and after the training. Before the training the
information for the lobby, i.e. the currently training
virtual groups or the planned training groups, is re-
trieved. After a training session the statistic data of
the current session is sent to the server and stored in
the database. In the group training mode each pa-
tient’s local computer computes an own 3D-scenario,
namely the view of the respective patient. How-
ever, the different scenarios are coordinated with each
other. They use the same map and the positions of the
players are communicated continuously. The corre-
sponding distributed system is presented in figure 6.
Figure 6: Behavior of the group dynamics on a distributed
system.
The 3D world is maintained on each computer, the
other players are displayed dynamically according to
the information about each group member. In order
to obtain this information, the application exchanges
messages in the following form:
• Patient ID
• Patient name
• Group ID
• Position vector (x, y, z)
• Direction vector (x, y, z)
• Velocity
• Position of the steering wheel
• Training time
The distribution of the messages to the corresponding
group members is based on the group ID within the
position-tracking application. The further data con-
tained in the message are needed for displaying 3D
objects locally on the ergometer training application.
5 APPLICATION
CordiAAL consists of two main applications:
the RehaWeb website and the ergometer training
application. The ergometer training application is re-
sponsible for the whole training sessions of the pa-
tients and the RehaWeb website for user administra-
tion and community functions.
5.1 RehaWeb
During the development of the CordiAAL project
the existing RehaWeb application was extended
and adapted, so that it is now possible to combine
both applications. The RehaWeb website provides
HEALTHINF2014-InternationalConferenceonHealthInformatics
84

Figure 7: RehaWeb Home Surface.
functionality for three types of user groups: patient,
cardiologist and administrator. Every group has got
different permissions within RehaWeb.
Patient: Patients can log in after registering on
RehaWeb. After log in they can look at their last
workout statistics.
They can arrange to meet with other patients for
a virtual group workout within the CordiAAL
ergometer training application. Furthermore it is
possible to communicate in a forum to exchange
information and experiences with other patients.
Moreover they can exchange private messages
with friends inside the RehaWeb community.
Figure 8: Vital Parameters Surface.
Cardiologist: Cardiologists can use RehaWeb to
manage the vital parameters of their patients
(see fig. 8). This is a very important function,
so that an individual and best possible workout
is guaranteed for each patient. It helps to avoid
overloads of the patients. The cardiologists are
able to set the values for the heart rate, respiration
rate, body temperature and SpO2. Initial values
have to be set for each patient after examination
by the clinic.
Additionally they have permissions to view
Figure 9: Detailed Statistic Surface.
and supervise detailed training statistics of all
their patients. Figure 9 shows an excerpt from a
sample statistic which has been recorded during a
training session.
Administrator: The administrator has got the per-
missions to manage all the users of RehaWeb.
Only he is able to add a new virtual route which
the patients can choose for their virtual training
within the ergometer training application.
5.2 Ergometer Training Application
The ergometer training application is the main
application of the CordiAAL system and responsible
for the training sessions. It controls the workout,
manages the sensors and takes care of the health
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
85

status of the training members. A training session can
be divided into three main sections: Training Prepa-
ration, Training Execution and Training Conclusion.
Training Preparation: First of all after starting the
application, the patients log in to the ergometer
training application with their user data from
RehaWeb. After a successful login the patients are
able to view their last workout statistics or they
can choose between a single and a group training
session. By selecting a group training it is pos-
sible to start a workout together with up to six
other patients at the same time using the same vir-
tual route. In this training mode all patients can
see each other like in a multiplayer game. The
other participants are covered in different colors
and they are able to communicate via voice chat.
After pushing the training start button, the patients
are asked to connect all sensors and devices. The
system waits until the patients have connected all
sensors. In an overview all connectable sensors
and devices are displayed with their connection
status.
Before the workout starts, the patients have to
Figure 10: Training Settings.
configure the settings of the training. They can
select a virtual route which they want to drive
in, set the duration of the workout and in group
training mode they can set the maximum number
of other patients driving with them (see fig. 10).
It is also possible to join an existing training in-
stead of creating a new one. By clicking on a dis-
played training from the list, a short status infor-
mation is shown. It gives information about the
remaining time, which virtual route is used and
how many other patients participate in this work-
out. The patients get only training sessions dis-
played they are able to join. Either the training is
a public one or the patient has previously arranged
it on RehaWeb. If they want to join one of the cur-
rent training sessions they simply have to select
one and click on the start button. The workout
starts immediately. As well there is a menu item
reachable from the main menu, where the patients
get an overview list of training sessions which will
start in the future.
Figure 11: Workout Screen.
Training Execution: From beginning to end of a
training session the application records all sen-
sor data like heart rate, SpO2, temperature, speed,
distance, time and rpm in an interval of one sec-
ond. Some of this information is displayed on the
screen during the training. So the patients can
see directly what the current load in watt is, the
speed in km/h, meters of the altitude profile and
the driven distance. On the left side of the dis-
play the names of the other group members and
their colors are shown. But the most important
information displayed is the heart rate status bar.
It is a big status bar in top of the screen, which
is corresponding to the current heart rate of the
patient (see fig. 12). Thus the patients can eas-
ily see if they perform their training in the right
way. The status bar is colored from green to red.
These scale correlates to the settings the cardiolo-
gist managed on the RehaWeb website. Training
inside the green range is optimal. The yellow and
red range indicate to drive faster or slower to get
back into the green area. Additionally a message
occurs on the screen with instructions. If the phys-
ical load is still too high, the system will regulate
the load of the ergometer down, until the heart rate
of the patient will be out of the red area. After the
predefined time span the workout will finish au-
tomatically, but the patient is capable to abort the
training session by clicking an exit button before
the training time is elapsed.
Figure 12: Heart Rate Status Bar.
Training Conclusion: After the workout, the pa-
tients are asked to specify a Borg value (Borg,
HEALTHINF2014-InternationalConferenceonHealthInformatics
86
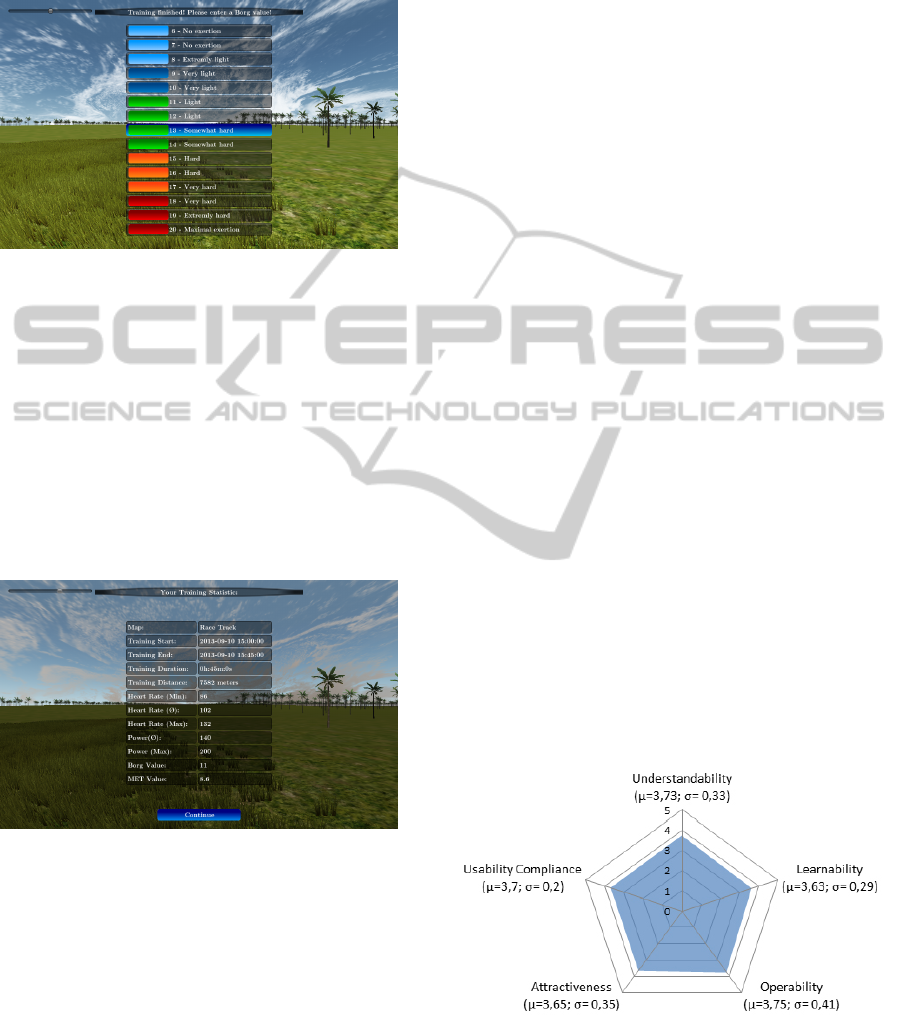
1970) for the training, which is an important clue
for the cardiologist about the subjective inten-
sity of the training (see fig. 13). Thereafter all
Figure 13: Surface to enter the Borg Value.
recorded data from the sensors and the application
are transmitted and stored in a database hosted
by the CordiAAL server. If it is impossible to
transmit the data to the server, e.g., because of
a broken internet connection, the recorded data
will be saved on the local hard disk. Next time
the ergometer training application is started the
application tries to submit the data again. Finally
a short summary of the current training session re-
sults together with average values like heart rate,
distance and time are displayed (see fig. 14).
Figure 14: Workout Summary.
6 EVALUATION
The evaluation aims at two different aspects: Analyz-
ing how far the CordiAAL system assists the users in
the execution of a training session and increasing the
motivation for a sustainable training. Secondly, veri-
fying the application in terms of design, usability and
ergonomics of the user interface.
In the evaluation process, the subjects performed
an afore designed scenario, which relates to a normal
use of the software. The scenario comprises a training
session, inspecting the statistics and a review of the
completed session. During the training session, it will
be analyzed how the displayed information affects the
subjects, how they experience the virtual environment
through the virtual reality head-mounted display, and
how far the virtual training affects the increase of mo-
tivation. Here, an important aspect is whether a vir-
tual group training influences the motivation and how
it stimulates the subject’s ambition, so that training
sessions are no longer felt as a liability but more as a
game.
To evaluate the aforementioned aspects, a ques-
tionnaire was presented to the subjects after the
training. The questions were divided into three cat-
egories and rated on a scale from one to five (1 = ”the
statement is not true”, 5 = ”the statement is true”).
First, the subjects were asked to answer questions for
self-assessment, these questions helped to determine
how motivated the subjects are in doing sports. In the
second category of the questionnaire, subjects were
asked to rate the usability of the system. At the end of
the test subjects were asked to rate the virtual training
and specify whether this type of training could in-
crease their motivation.
Overall 10 participants, including 2 women and 8
men were tested in the age range of 25 years up to
36 years. The sequence of execution took about 30
minutes to complete, with two training sessions by 10
minutes.
In order to present the usability evaluation results,
five categories were defined (see figure 15). As you
can see, the software is considered as user-friendly,
an average value of 3,7 out of 5 was achieved. One of
the most important aspects of this case was to make
the software as intuitive as possible, so long learning
phases are avoided and this barrier pulls no reduction
in motivation.
Figure 15: Evaluation of the usability questions by cate-
gories ”Understand Solutions, Learnability, Operability, At-
tractiveness, Usability Compliance”.
To evaluate the training, the subjects self-assessed
their sportiness and their general sport-related moti-
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
87
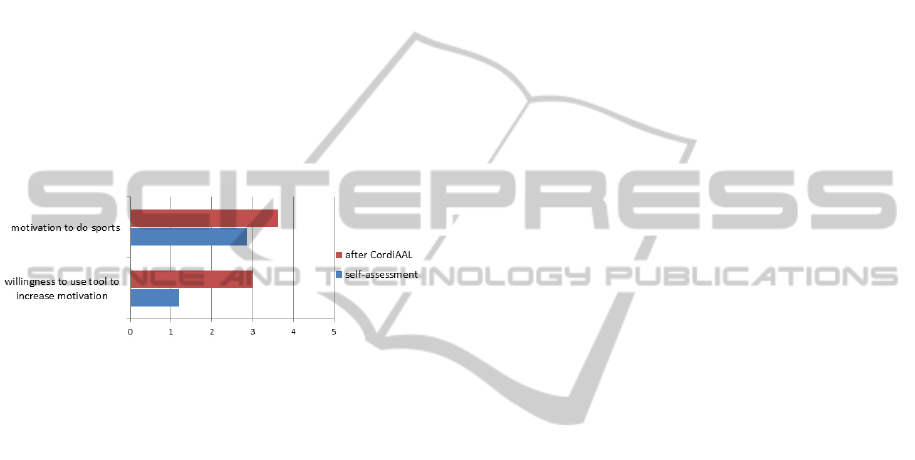
vation to conclude how far the training in the virtual
environment could increase their motivation. To il-
lustrate the influence of the training with CordiAAL
we have taken two aspects into account. The moti-
vation for doing sports with and without any general
technical aids, and the same with CordiAAL as a spe-
cific technical aid. Figure 16 clearly illustrates that
the subjects have difficulty doing sustainable sporting
activities and also the willingness of using aids is low.
In turn, the increasing motivation through the virtual
training is clearly evident. An increased value for the
readiness to use CordiAAL as a technical aid for reg-
ular sport activities was also indicated. The most im-
portant motivation factor was thereby the training in a
virtual group. It was stated that the training and com-
munication with other group members minimize the
effort of training and increase the ambition.
Figure 16: Evaluation of the questions of motivation and
willingness to use the aids, divided according to data ob-
tained from the self-assessment and evaluation after training
with CordiAAL.
7 CONCLUSIONS
The user study clearly demonstrates that the main ob-
jectives of the CordiAAL system were achieved, real-
izing a playfully ergometer training which motivates
users to a regular physical activity, bringing users
with different fitness levels together and to give them
safety at the same time.
This is done by a permanent monitoring of vital
data and an adjustment of the ergometer load based
on these data. Since the study was not conducted
with subjects with heart disease, for ethical reasons,
the question of the decrease of anxiety remains open.
The next stage in the evaluation would be a long-
term study to check if the motivation stays high-
leveled in a long-term use.
REFERENCES
Anderson, F., Annett, M., and Bischof, W. F. (2010). An-
nual Review of Cybertherapy and Telemedicine 2010.
Studies in Health Technology and Informatics.
Balady, G., Williams, M., Ades, P., Bittner, V., Comoss, P.,
Foody, J., Franklin, B., Sanderson, B., and Southard,
D. (2007). Core components of cardiac rehabili-
tation/secondary prevention programs. Circulation,
115(20):2675–82.
Bjarnason-Wehrens, B., Held, K., and Karoff, M. (2006).
Herzgruppen in Deutschland: Status quo und Perspek-
tiven. Herz, 31:559–565.
Bjarnason.Wehrens, B., Drsch, M., Gielen, S., Halle, M.,
Hambrecht, R., and Kindermann, W. (2009). Leitlinie
krperliche aktivitt zur sekundrprvention und therapie
kardiovaskulrer erkrankungen. Clinical Research in
Cardiology Supplement (CRICS), pages 1–44.
Borg, G. (1970). Perceived exertion as an indicator of so-
matic stress. Scandinavian journal of Rehabilitation
Medicine, 2:92–98.
Boulos, M. N. K. and Yang, S. P. (2013). Exergames for
health and fitness: the roles of GPS and geosocial
apps. Technical report, International Journal of Health
Geographics.
Busch, C., Litvina, A., and Willemsen, D. (2009). Kar-
diale Telerehabilitation auf Basis einer flexiblen Platt-
form f
¨
ur verteilte Systeme - das OSAmI-D Projekt.
e-Health, pages 218–221.
Caprani, N., O’Connor, N. E., and Gurrin, C. (2012). Touch
Screens for the Older User. In Cheein, D. F. A., editor,
Assistive Technologies, chapter 5. InTech.
Dohndorf, O., G
¨
oring, A., Krumm, H., Schneider, A., Som-
mer, A., Sladek, S., Busch, C., Hoffmann, J.-D., and
Willemsen, D. (2012). RehaWeb – An information
system for cardiologic rehabilitation assistance in the
third phase. Technical report, TU Dortmund Univer-
sity.
Eifert, G. H., Thompson, R. N., Zvolensky, M. J., Edwards,
K., Frazer, N. L., Haddad, J. W., and Davig, J. (2000).
The cardiac anxiety questionnaire: development and
preliminary validity. In Behaviour Research and Ther-
apy, volume 38, pages 1039–1053. Elsevier Ltd.
Fielding, R. T. (2000). Architectural styles and the design
of network-based software architectures. PhD thesis,
University of California. AAI9980887.
Gesundheit in Deutschland aktuell – Telefonischer Gesund-
heitssurvey (GEDA) (2009/2010). Gesundheit in
Deutschland aktuell – Telefonischer Gesundheitssur-
vey (GEDA): Durchschnittliche sportliche Aktivit
¨
at
pro Woche (Anteil der Befragten in Prozent).
Kotseva, K., Wood, D., Backer, G. D., Bacquer, D. D., Py-
oeraelae, K., and Keil, U. (2009). Cardiovascular pre-
vention guidelines in daily practice: a comparison of
euroaspire i, ii, and iii surveys in eight european coun-
tries. The Lancet, 373(9667):929 – 940.
Lampert, C., Schwinge, C., and Tolks, D. (2009). Der
gespielte Ernst des Lebens: Bestandsaufnahme und
Potenziale von Serious Games (for Health). Zeitschrift
f
¨
ur Theorie und Praxis der Medienbildung, 15/16:1–
16.
Lee, C., Folsom, A., and Blair, S. (2003). Physical activity
and stroke risk: a meta-analysis. Stroke, 34(10):2475–
81.
HEALTHINF2014-InternationalConferenceonHealthInformatics
88

Lee, E. A. (5-7 May 2008). Cyber Physical Systems:
Design Challenges. Object Oriented Real-Time Dis-
tributed Computing (ISORC), 2008 11th IEEE Inter-
national Symposium on, pages pp.363–369.
Nocon, M., Hiemann, T., M
¨
uller-Riemenschneider, F., Tha-
lau, F., Roll, S., and Willich, S. N. (2008). Association
of physical activity with all-cause and cardiovascular
mortality: a systematic review and meta-analysis. Eur
J Cardiovasc Prev Rehabil, 15:2239–246.
Novick, A. (2008). Implementing crud operations using
stored procedures: Part 1.
Pautasso, C., Zimmermann, O., and Leymann, F. (2008).
Restful web services vs. ”big”’ web services: mak-
ing the right architectural decision. In Proceeding of
the 17th international conference on World Wide Web,
WWW ’08, pages 805–814, New York, NY, USA.
ACM.
Sattelmair, J., Pertman, J., Ding, E., Kohl 3rd, H., Haskell,
W., and Lee, I. (2011). Dose response between physi-
cal activity and risk of coronary heart disease: a meta-
analysis. Circulation, 124(7):789–95.
Schulz, G. (2007). Regelungstechnik 1 Lineare und
Nichtlineare Regelung, Rechnergesttzter Regleren-
twurf. Oldenbourg Wissenschaftsverlag GmbH.
Shahsavari, H., Shahriari, M., and Alimohammadi, N.
(2012). Motivational factors of adherence to cardiac
rehabilitation. Iranian Journal of Nursing and Mid-
wifery Research, 17:7.
Statistisches Bundesamt (2008). Herz-
/Kreislauferkrankungen verursachen die h
¨
ochsten
Krankheitskosten. Wiesbaden.
Statistisches Bundesamt (2011). 2011: Todesf
¨
alle 2011
leicht r
¨
uckl
¨
aufig – h
¨
aufigste Todesursache Herz-
/Kreislauferkrankungen. Wiesbaden.
Yusuf, S., Hawken, S., Ounpuu, S., Dans, T., Avezum, A.,
Lanas, F., McQueen, M., Budaj, A., Pais, P., Varigos,
J., and Lisheng, L. (2004). Effect of potentially mod-
ifiable risk factors associated with myocardial infarc-
tion in 52 countries (the interheart study): case-control
study. Lancet, 364(9438):937–52.
CordiAAL:EnhancedMotivationforCardiologicalErgometerTrainingthroughVirtualGroupsinVirtualWorlds
89
