
Designing an Effective Social Media Platform for Health Care
with Synchronous Video Communication
Young Park
1
, Mohan Tanniru
1
and Jiban Khuntia
2
1
College of Business Administration, Savannah State University, Savannah, GA 31404, U.S.A.
2
School of Business Administration, Oakland University, Rochester, MI 48309, U.S.A.
3
Business School, University of Colorado Denver, Denver, CO 80238, U.S.A.
Keywords: Social Network, Synchronous Video Communication, Healthcare, Multi-tier Application Architecture.
Abstract: Online social networks are evolving as platforms for health communication among the public, patients, and
health professionals. Existing health social network based portals do not provide synchronous -video-based
communication features; and are restricted to only text and picture based content sharing. Arguably,
healthcare focused online social networks need video based communication for active knowledge sharing
between providers and patients, peer-patients, or sharing disease related information through visual media.
This study provides a technological framework and design architecture to develop a customizable online
healthcare social media network that can incorporate synchronous video communication capability. The
design principles and layers that support different types of functionality are described. An evaluation in the
context of Rheumatology and back pain patients is underway and will not be discussed in this paper due to
page constraints.
1 INTRODUCTION
Use of online social health networks is increasing
with the understanding that online communication
and support is highly effective to manage own health
(Giustini 2006; Heidelberger 2011; Thackeray et al.
2008). In addition, online social media platforms
are providing conduits for providers to increase
clinical competence of healthcare practitioners
through constant monitoring and support
mechanisms (Green and Hope 2010; McNab 2009).
The emerging use of social media in healthcare is
centered around interactions between individuals
and health organizations, and the nature and speed at
which these interactions support communication of
health related issues (Frost and Massagli 2008;
Hawn 2009; Landro 2006). In the United States,
61% of adults search online and 39% use social
media such as Facebook for health information (Fox
and Jones 2009). Globally, the adoption rate is
similar, such as 45% of Norwegian and Swedish
hospitals are using LinkedIn, and 22% of Norwegian
hospitals use Facebook for health communication,
and Facebook is emerging as the fourth popular
source of health information in UK (Heidelberger
2011). Moreover, with the focus on decreasing the
growing healthcare costs, social media is posited to
provide a cost-effective means to support patient-
doctor interactions (Hillestad et al. 2005).
Irrespective of the increased use of social media
sites in healthcare, design issues pose a significant
challenge for effective use of these media in
diagnosis, treatment, and intervention. Specifically,
the lack of synchronicity among these sites is a
major issue for both patients and providers. For
example, a patient cannot get an expert opinion, as
opposed to unreliable opinions from friends and
family, to his current breathing issues (say, due to
asthma) just by logging into a social network site
given that most of these are designed to access
archived information. Several existing healthcare
social networking portals use communication
methods such as emails, published articles or
discussion forums (see Table 1 for a detailed list and
features of social networking portals). They lack
scalability to support synchronous communication
for online consultation, which would greatly
contribute to improving communication between
health professionals and patients. To our knowledge,
no social network portal has the capability to make a
doctor available to a patient through a video
communication instantly. Furthermore, as healthcare
434
Park Y., Tanniru M. and Khuntia J..
Designing an Effective Social Media Platform for Health Care with Synchronous Video Communication.
DOI: 10.5220/0004905204340441
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 434-441
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

Table 1: Sample Healthcare Web Portals and Social Media Sites.
Website Name & URL Focus
Communication
Methods
Content Categories
Steady Health
www.steadyhealth.com
How to live healthily under
different categories. Covers
disease treatments and diets.
Information Center;
Articles; Discussions;
Videos; Slideshows;
Medical Answers;
Applications
Categorized by: Well Beings
(purposes); Health Conditions
(disease types); Family Heath
( Sex and Age); Therapies &
Treatments; Emotional & Mental
Health
Wellness
www.wellness.com
How to live healthy under
different categories. Covers
disease treatments and diets. Also,
information about fitness and
beauty.
Blogs; Forum;
Articles
Popular Topics; Facilities; Fitness
& Beauty; Dental Care; Stores;
Insurances; Doctors; Mental
Health; Counseling; Provider
Program; Community
Everyday Health
www.everydayhealth.com
Diseases, drug information, living
healthily (food & diet).
Articles; Videos;
Twitters; Facebook;
Blogs; Applications
Conditions (diseases); Drugs;
Health Living; Food & Recipes;
Advices & Support
Find a doc
www.findadoc.com
Devised a unique proprietary
rating system that helps patients
choose from among the 720,000
practicing physicians in the U.S.
NA
Contact Information Search by
Categories
My doc hub
www.mydochub.com
Offers doctors' information,
hospital information and diseases
information.
Articles; Discussions;
Blogs; Applications
Doctors; Reviews; Dentists; Blog;
Answers; Chiropractors;
Hospitals; Vets; Health; News;
Health A-Z; Articles
Spark People
www.sparkpeople.com
Focused on living healthily
depending on food and exercises.
Information Center;
Articles; Discussions;
Videos; Boards;
Applications
Eat Better; Feel Better; Look
Better
Physician Data Query
www.cancer.gov/cancerto
pics/pdq
PDQ (Physician Data Query) is
NCI's comprehensive cancer
database.
Search Engine NA
Health grades
www.healthgrades.com
Doctors' information, hospital
information and dentists'
information.
NA
Find Doctors; Find Dentists; Find
Hospitals
Vitals www.vitals.com
Find and review doctors, make an
appointment and prepare for the
doctor visit.
NA
Patient Education; Write a
Review
RatMD.com
www.ratemds.com
Find and review doctors and
hospital information.
FAQ; Forums;
Tweeters
Find a Doctor; Find a Doctor;
Browse Doctors; Hospitals; Top
Local Doctors; FAQ; Forums
Drscore.com
www.drscore.com
Find doctors information. Email
Find a doctor; Score your doctor;
For Patients
Doctortree.org
www.doctortree.org
Find doctors information. NA Search Engine by Categories
Suggest a doctor
www.suggestadoctor.com
It helps to find doctors
information.
Customers'
Evaluations
Search Engine by Categories
Healthcare.com
www.healthcare.com
Information about health
insurances.
NA NA
Vimo
www.vimo.com
Information about health
insurances.
NA NA
depends on the evidence base of a set of visual
diagnostics; and plausibly, in this scope,
synchronous video communication can be used to
establish an effective link that supports service and
care delivery in healthcare system.
The study uses the design science approach,
which emphasizes that any new information
technology artifact, developed to address a key
problem, should be evaluated in a real world setting
to demonstrate its purposefulness (Hevner et al.
2004). We provide a technological framework and
design architecture to develop a customizable online
DesigninganEffectiveSocialMediaPlatformforHealthCarewithSynchronousVideoCommunication
435

healthcare social media network that can incorporate
synchronous video communication capability. Next
section will provide some background and research
context and the third section will discuss the features
needed to support the video communication portal.
The fourth section illustrates the functioning of the
portal, along with the design principles and layers
that support different types of functionalities. The
last section makes some comments on the evaluation
underway and provides concluding remarks.
2 PRIOR RESEARCH
Existing literature points out that there are several
limitations of social media for health
communications. In a recent review, Moorhead et al
(2013) point out that quality concerns, lack of
reliability of information, and blurred lines between
content producer are three major concerns about the
reliability of these platforms. However, beyond
these concerns, the most important one is the
“information overload” and “lack of validity of the
information,” and this poses a bigger challenge to
the use of the social media for meaningful purposes
(Adams 2010a; b). Lack of guidelines may
misinform the public on how to correctly apply
information found online to their personal health
situation, thus posing a danger in promulgating
adverse health impact or consequences (Freeman
and Chapman 2007). These reasons also deter
providers not to participate in a social network site,
especially when there is a higher likelihood that the
text based information may result in a greater risk.
Thus, limited evidence on to what extent online
communities are effective in positively impacting
people’s health (Colineau and Paris 2010), and how
effective social media is in communicating health
related information to patients, are some inhibiting
factors for providers from actively participating in
online social health networking portals (Kim 2009).
Against these concerns, existing studies have
suggested three plausible alternatives for greater
provider engagement (Lagu, et al., 2010). First,
similar to traditional Internet sites, there is a need for
greater interactivity in the social media for patients
to upload information regardless of quality. The
information posted will be at least more realistic and
meaningful to the patients (Adams 2010b) and this
might help providers glean useful insights into
patients’ needs and concerns. Mikki Nasch, the co-
founder of AchieveMint recently discussed their use
of social medial platform to let patients voluntarily
interact with either, so healthcare providers can gain
useful information on patient adherence to certain
desired behaviour, using Mashup technologies (Polz
et al. 2013). Second, reliability concerns can be
mitigated if the social media communication and
relevant information extraction can be given to third
party agencies (Sneha and Varshney 2009), thus
allowing healthcare providers to focus on
developing appropriate strategies based on this data.
In the above example, AchiveMint is the third party
used by Sanofi-Aventis, a pharmaceutical firm. The
third, and the most important, suggestion is to
improve “media richness” by making the
information communicated contextually relevant to
the situation at hand (Kaplan and Haenlein 2010).
In support of the third suggestion, a novel artifact
that supports synchronous video communication
(SVC) is proposed in this research paper. Table 1
summarizes many social media interaction
environments that support health care related
interactions and none of these, to our knowledge,
have the provision for such synchronous video
communication functionality.
Synchronous video communication (SVC) is not
new concept in the emerging Web 2.0 context.
Indeed there are a number of applications that
provide SVC services, albeit not within social media
platforms. Applications such as Skype, Voodoo,
Google Chat with Video do facilitate multi-party
video conferencing features. While it may be argued
that, the social media users can always use these
“external third party” solutions for synchronous
communication. However, in the health care
context, knowledge base diagnostic or information
sharing approach requires an integrated platform as
switching between different applications is
cumbersome to users. Both in the patient-physician
context as well as patient-patient context, the
requirement of a well-integrated system to support
secure communication, search capabilities to find
topics of interest, connect with others, and to allow
for business work-flow integration will facilitate
efficient and effective care management. To
summarize, although social media applications and
use are growing in healthcare, but a significant
design gap remains in the existing social media sites.
They are not focused on synchronous video based
communication, and that perhaps is posing a
challenge for a provider-side adoption of the social
media to deliver care. We suggest a design and
demonstrate implementation of synchronous video
communication (SVC) in a social media portal. In
this regard, the next section develops design features
needed to support the SVC application in a
healthcare setting using social media environment.
HEALTHINF2014-InternationalConferenceonHealthInformatics
436

3 USER REQUIREMENTS
The synchronous video communication (SVC),
designed to support health related discussions in a
social media context, uses features along three
layers: input (front-end), application (middle) and
database (back-end layers) (see Figure 1). The front-
end layer is designed to support two types of
stakeholders: (1) users, consisting of patients, friend
and family and (2) providers, consisting of
physician, nursing staff, provider organization
employees. The goal here is to provide easy and
secure access to the video content, and support the
associated social media interaction between patients
and providers. The middle layer is designed to
support the workflow management necessary for the
distribution of the content to meet care provider’s
policy needs and interaction of the content to meet
the healthcare needs of the patient. The back-end
layer is designed to support the creation,
customization and search functionalities of the SVC.
3.1 User Interface Requirements
The user interface requirements of the front-end
layer focus on two access related features: ease of
access and secure access. The ease of access in SVC
calls for both effectiveness of information and
mobility for users. The interface needs to be simple
and intuitive, as many healthcare sites are accessed
by elderly people. The interface needs to limit the
degree of scrolling and allow the patients to preview
the content and community they are interacting with
before they enter the site. In addition, the system
needs to support many typical communication
features such as discussion forums, instant
messaging and others such as those discussed in
physician rating sites (Lagu et al. 2010).
The mobility feature in this context is the user
access at any time and from any place to the portal,
irrespective of geographical location, technology
platform and medium of internet access. Patient
access to the system is critical as this is key to the
synchronous communication. The focus should be
ubiquitous access and patient-centric, so that patient
can connect with his/her friends for chat, review
health care data, connect with - and engage in -
consultation with a physician, etc. In other words,
the technology should support access from any
platform (desktop to mobile devices), and from any
location (work place, home, and outside of home).
Secure access to the site should include authentic
login features and other controls needed when
information is shared with others in public or private
interaction mode. There is negative relationship
between privacy concerns and willingness to
disclose information when requests come from
government/public health agencies vis-à-vis
hospitals or pharmaceutical companies (Anderson
and Agarwal 2011). In addition, patients trust non-
profit hospitals more than for-profit organizations.
Therefore, it is critical that appropriate
privacy/access control features are incorporated and
screens/views are limited based on the role the group
or an individual user (patient, physician, face book
involved in the discussion, etc.) may play.
Moreover, social media sites with chatting or
blogging capability have to detect and prevent the
use of profanity or obscene words. Thus, the
proposed system should support a robust set of
secure access mechanisms, including password
controls, role based access, and administration
privileges upon authentication. Finally, Secure
Sockets Layer (SSL) technology for encrypted link
between a server and a client may be needed, given
that the social media platform will operate from
different server locations.
3.2 Database Requirement
The back end layer includes a database engine that is
designed to support content creation or
development, content customization and content
search. The health care content in healthcare is
changing rapidly and physicians and other health
care providers may update the content used by
patients at a more frequent rate. Thus, ease of update
of content becomes critical to maintain the
effectiveness of the site. Furthermore, given that the
context of patient inquiry will change with time,
there should be provisions for customization by
patients, so that patients can select the right
healthcare domain to share it with others and
consult/pose questions to physicians. Finally, as the
content stored grows over time, ability to quickly
and effectively search and select the content that
patients need becomes an important criteria for the
design of the system.
3.3 Application Requirements
The application layer is designed to address three
needs: (1) alignment/support with organizational
workflows, (2) accommodation of domain diversity,
and (3) scale up to meet the increase of users.
First, alignment with organizational workflows is
crucial since the system should be flexible enough to
support the needs of healthcare providers to
DesigninganEffectiveSocialMediaPlatformforHealthCarewithSynchronousVideoCommunication
437
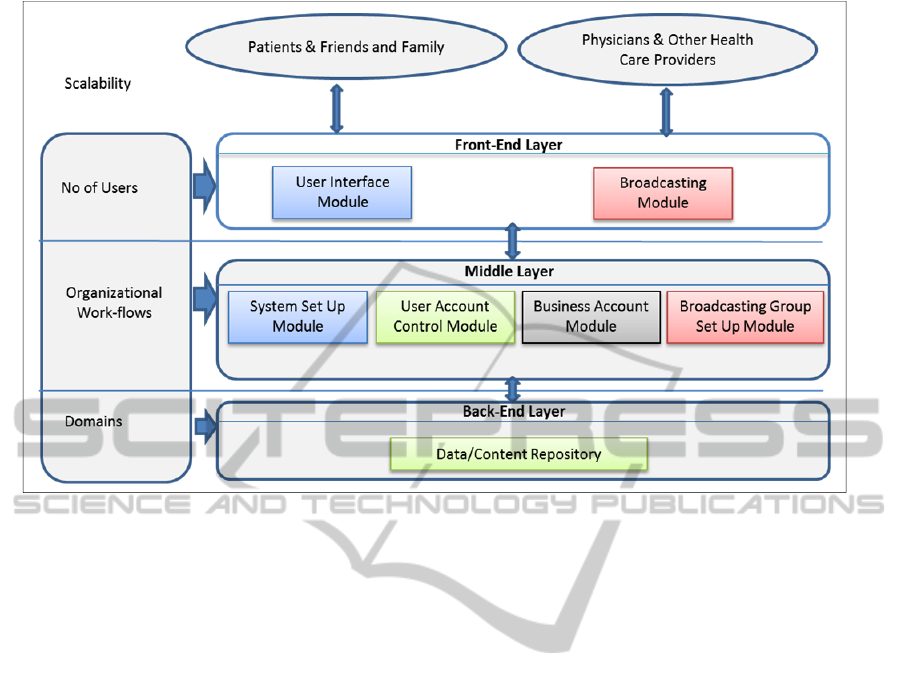
Figure 1: Design Features of the SVC-Social Media Framework.
support care consultation and knowledge
dissemination. Providers may want to schedule
weekly broadcasting time for certain type of care
related communication, or simply make physicians
available for consultation at a certain time, for
patients to interact with the physicians. The platform
should provide flexibility and customizability so that
it is used by physicians from differing streams with
distinct needs. Apparently, a common theme
amongst care delivery is the need of synchronous
consultation or synchronous discussion, relying on a
repository of evidence based knowledge system.
We try to implement the synchronous discussion
part, and make use of pre-recorded videos for
creation of the knowledge system along with text
based repositories.
Second, although the end goal is to develop a
synchronous video conference (SVC) portal for
health domain, the platform should provide
opportunity to support communication for various
other domains than healthcare. For example, in
addressing pain management issues and related care,
the system may support synchronous interaction
between patients and physician, while in the case of
patients with obesity and diabetes related illnesses,
the system may focus on social interaction among
patients groups to support behavior modification.
Yet, in other cases such as heart patients in a nursing
home, the system may provide patient-family
interaction with only an asynchronous display of
care related information provided by the physician.
For smoking cessation management programs, the
system may rely on both group and incentive based
interventions. While the requirements for these
health related issues may be different, but a
generalizable application layer that can support
dynamically the interface protocol and content
changes with minimal programming should be the
objective of the system. For example, adding videos
and indexing these for easy use, as well providing
content-providers the ability to promote these to
different groups is useful.
Finally, as demonstrated in many social media
sites, the data and the number of users on any social
media typically start small but may soon grow
exponentially depending on the popularity of the
site. In addition, any site that uses videos requires a
great deal of bandwidth and storage to handle a large
amount of data being transmitted. Although
organizations go through a rigorous capacity
planning or other pre-estimation process, it is very
common to start small and expand as demand
increases. In this regard, it is important to design the
architecture to support the scalability; that we have
accommodated in the design for scalability.
Thus, to summarize, we user interface
requirements of a synchronous video communication
feature design for a social media platform need to
accommodate some salient features in its front-,
middle- and back- end layers. While addressing the
HEALTHINF2014-InternationalConferenceonHealthInformatics
438

design parameters for these features, the next section
will provide elements embedded in the system
architecture to support the SVC and illustrate its use
with some sample screen shots of the implemented
design in an alpha-developed social media site.
4 DESIGN ARCHITECTURE
The system design architecture has the objective to
support the design features discussed in the previous
section. Figure 1 provides, under each layer,
specific system design elements to support the
synchronous video communication in social media.
The architecture consists of several components in
the three layers: (1) front-end layer, (2) middle layer
and (3) back-end layer.
4.1 Front-end Layer
The front-end layer consists of two major modules:
(a) user interface module and (b) broadcasting
module. The user interface module is responsible
for providing easy-to-use interface, user
authentication for secured access or search options.
The user interface module allows the users to log in
and browse, search for friends, or invite a group to
join through web browsers. The client’s user
interface is automatically rendered by the changes
made to the system set up module in the middle
layer. Through the access control mechanism built
in, the user account control module of the middle
layer displays different set of menus depending on
the type of user account: broadcast owner or
broadcast recipient. To build dynamic and
interactive user interfaces, a combination of
Javascript and AJAX on top of HTML and CSS
have been used. The home screen consists of three
panels: top menu panel, left menu panel, and
outcome display panel in the middle.
The broadcasting module is responsible for
creating and customizing the broadcasting contents.
This module is only available for the account
registered as a broadcast owner. Once the
broadcasting feature is set up by the middle layer,
the owner - health professional - can customize
broadcasting settings. The system is designed to
leave zero-foot print on the client site by having the
console program download from the back-end server
the needed information, wherever it is needed. Once
it is downloaded, the console program indicates
whether it is on air or not, and displays the same
screen users see on their website.
Using the console program in the broadcasting
module, health professionals can easily set up
weekly live video schedules and customize the
contents by uploading any recoded video or image
materials they want to share with others. Once the
broadcast is made to the public, all interested can
interact with the health professional and engage in
public chat or even private chat. By clicking a user
name on the user list, users can see the profile of the
person of interest or send a private chat request for a
confidential communication. If the person accepts it,
they can have a private chat that others cannot see.
This feature is extremely critical in healthcare
environment that deals with confidential information
on many occasions. This broadcasting module uses
Adobe’s Flash to stream videos and audios at the
user site as it uses less bandwidth to stream videos.
4.2 Middle Layer
The middle layer has four major modules: (a) the
system set up module, (b) the user account control
module, (c) the business account module, and (d) the
broadcasting group set up module.
The system set up module is responsible for
defining parameters that will be passed to the
browser to control the behavior of the application. It
also provides a mechanism to set up the interface
including the search menu. All the changes made
through this module are saved into the data/content
repository of the back-end layer.
The user account control module provides a
mechanism for users to set up accounts. It also
provides a way to block an account that violates
established policies set up by the SVC portal. It also
communicates with the broadcasting set up module
to determine the access control of the broadcaster
account.
Business account module helps to implement
organizational workflows and business processes.
For example, business activities are recorded to
track the status of recruiting or contacting potential
broadcasters or any issues related to broadcasting,
etc.
The broadcasting group set up module interacts
with the video streaming service and builds a
container that includes all necessary functionalities
including live video broadcasting, scheduling, off-
line recoded video, and other training material
management. Once the broadcasting group is set up
through this module, the container is created and
stored into data/content repository with a unique
identifier. Because this identifier is associated with
the broadcaster (owner) account, the broadcaster can
DesigninganEffectiveSocialMediaPlatformforHealthCarewithSynchronousVideoCommunication
439

easily retrieve the container from anywhere to
broadcast or change parameters through the
broadcasting module implemented into the
broadcasting console program. This module
contains the steps needed to build a chat module and
link a chat window to the designated video
broadcasted window.
4.3 Back-end Layer
This layer is a repository that stores all the data and
the containers made by modules in the front-end
layer and the middle layer. This repository is
designed and structured so that the stored scripts,
templates, or objects can be shared and reused
especially by the broadcasting group set up module
of the middle layer and the broadcasting module of
the front-end layer. When a new broadcasting group
is created, a separate container for the group is
created in this repository. In addition, when
parameters are changed in the front-end layer, these
changes are updated into the flash script stored in the
corresponding container. Most of the data in this
repository are represented by the relational data
model and built on MySQL program. The chat
content and user list of each group are also stored
into the repository, and constantly updated by the
broadcasting module of the front-end layer.
5 CONCLUSIONS
An evaluation of this framework in support of pain
management is underway. The proposed system
provides several key benefits that go beyond one
provider or one disease setting. First, the system can
provide information sharing platform with real-time
interactivity between the parties. Second, the system
design is centered around providing flexibility of
building communities or targeted markets amongst
parties based on their interests, while providing
control to the information disseminated. Third, the
portal can make expert information available in
public or in private, depending on the modalities of
operation. Because the information will be provided
by expert’s live video rather than simple blogging or
email communication, the patients or information
recipients’ satisfaction and trust will increase, as the
systems allows for two-way real-time
communication between the parties through live
chat. Besides evaluation, future work will continue
to look at leveraging the benefits of synchronous
vide communication system on a broad scale.
REFERENCES
Adams, S. A. 2010a. "Blog-Based Applications and
Health Information: Two Case Studies That Illustrate
Important Questions for Consumer Health Informatics
(CHI) Research", International Journal of Medical
Informatics (79:6), pp. e89-e96.
Adams, S. A. 2010b. "Revisiting the Online Health
Information Reliability Debate in the Wake of “Web
2.0”: An Inter-Disciplinary Literature and Website
Review", International Journal of Medical Informatics
(79:6), pp. 391-400.
Anderson, C. L., and Agarwal, R. 2011. "The Digitization
of Healthcare: Boundary Risks, Emotion, and
Consumer Willingness to Disclose Personal Health
Information", Information Systems Research (22:3),
pp. 469-490.
Colineau, N., and Paris, C. 2010. "Talking About Your
Health to Strangers: Understanding the Use of Online
Social Networks by Patients", New Review of
Hypermedia and Multimedia (16:1-2), pp. 141-160.
Fox, S., and Jones, S. 2009. "The Social Life of Health
Information," pp. 2009-2012.
Freeman, B., and Chapman, S. 2007. "Is “Youtube”
Telling or Selling You Something? Tobacco Content
on the Youtube Video-Sharing Website", Tobacco
Control (16:3), 2007, pp. 207-210.
Frost, J. H., and Massagli, M. P. 2008. "Social Uses of
Personal Health Information within Patientslikeme, an
Online Patient Community: What Can Happen When
Patients Have Access to One Another’s Data",
Journal of Medical Internet Research (10:3).
Giustini, D. 2006. "How Web 2.0 Is Changing Medicine",
BMJ (333:7582), pp. 1283-1284.
Green, B., and Hope, A. 2010. "Promoting Clinical
Competence Using Social Media", Nurse Educator
(35:3), pp. 127-129.
Hawn, C. 2009. "Take Two Aspirin and Tweet Me in the
Morning: How Twitter, Facebook, and Other Social
Media Are Reshaping Health Care", Health Affairs
(28:2), pp. 361-368.
Heidelberger, C. A. 2011. "Health Care Professionals’ Use
of Online Social Networks, Available at:
http://cahdsu.wordpress.com/2011/04/07/Infs-892-
Health-Care-Professionals-Use-of-Online-Social-
Networks/ " Retrieved 13 October 2013.
Hevner, A. R., March, S. T., Park, J., and Ram, S. 2004.
"Design Science in Information Systems Research",
MIS Quarterly (28:1), pp. 75-105.
Hillestad, R., Bigelow, J., Bower, A., Girosi, F., Meili, R.,
Scoville, R., and Taylor, R. 2005. "Can Electronic
Medical Record Systems Transform Health Care?
Potential Health Benefits, Savings, and Costs", Health
Affairs (24:5), pp. 1103-1117.
Kaplan, A. M., and Haenlein, M. 2010. "Users of the
World, Unite! The Challenges and Opportunities of
Social Media", Business Horizons (53:1), pp. 59-68.
Kim, S. 2009. "Content Analysis of Cancer Blog Posts",
Journal of the Medical Library Association : JMLA
(97:4), pp. 260-266.
HEALTHINF2014-InternationalConferenceonHealthInformatics
440

Lagu, T., Hannon, N., Rothberg, M., and Lindenauer, P.
2010. "Patients’ Evaluations of Health Care Providers
in the Era of Social Networking: An Analysis of
Physician-Rating Websites", Journal of General
Internal Medicine (25:9), pp. 942-946.
Landro, L. 2006. "Social Networking Comes to Health
Care", Wall Street Journal (27).
McNab, C. 2009. "What Social Media Offers to Health
Professionals and Citizens, URL: http://
www.who.int/Bulletin/Volumes/87/8/09-066712/En.".
Moorhead, S. A., Hazlett, D. E., Harrison, L., Carroll, J.
K., Irwin, A., and Hoving, C. 2013. "A New
Dimension of Health Care: Systematic Review of the
Uses, Benefits, and Limitations of Social Media for
Health Communication", Journal of Medical Internet
Research (15:4) pp 11-25.
Polz, M., Sanofi-Aventis, and Mikki Nasch, A. 2013.
"Smart Data Is the Key to Scaleable Healthcare
Solutions," in: Big Data Symposium. Eller College of
Management, Arizona.
Sneha, S., and Varshney, U. 2009. "Enabling Ubiquitous
Patient Monitoring: Model, Decision Protocols,
Opportunities and Challenges", Decision Support
Systems (46:3), pp. 606-619.
Thackeray, R., Neiger, B. L., Hanson, C. L., and
McKenzie, J. F. 2008. "Enhancing Promotional
Strategies within Social Marketing Programs: Use of
Web 2.0 Social Media", Health Promotion Practice
(9:4), pp. 338-343.
DesigninganEffectiveSocialMediaPlatformforHealthCarewithSynchronousVideoCommunication
441
