
Knowledge Creation in Technology Evaluation of 4-Wheel Electric
Power Assisted Bicycle for Frail Elderly Persons
A Case Study of a Salutogenic Device in Healthcare Facilities in Japan
Miki Saijo
1
, Makiko Watanabe
2
, Sanae Aoshima
3
, Norihiro Oda
3
,
Satoshi Matsumoto
4
and Shishin Kawamoto
5
1
Graduate School of Innovation Management, Tokyo Institute of Technology, Tokyo, Japan
2
Graduate School of Science and Technology, Tokyo University of Science, Chiba, Japan
3
Kakegawa Kita Hospital, Shizuoka, Japan
4
Corporate Planning Division, Yamaha Motor Engineering Co., Ltd, Shizuoka, Japan
5
Faculty of Science, Hokkaido University, Sapporo, Japan
Keywords: Knowledge Creation, Tacit Knowledge, Health Care for Frail Elderly Persons, AT Devices, Technology
Evaluation.
Abstract: As societies age, it is anticipated that we will see a sudden increase in the number of frail elderly persons.
New assisted-technology (AT) devices to facilitate the activities of daily life (ADL), especially of walking,
are essential for the healthy life of these people. However, frail elderly people suffer a variety of physical
and mental weaknesses that tend to hinder their ability to make use of AT devices in the intended manner.
Because of this, it is important that new AT devices undergo technology evaluation within the context in
which they are to be used, but there is very little research in this area. In this study, frail elderly people in
Japanese daycare centers and rehabilitation facilities were given a 4-wheel, power-assisted bicycle, called a
“Life Walker” (LW), to ride, and technology evaluations were carried out based on functionality, usability,
and experience as perceived by the frail elderly riders. The LW is considered to be best suited for those age
75 and older assessed at level 1 to 3 under Japan’s long-term care insurance program, but the data for the 61
people at the rehabilitation facility who tried out the bicycle under the supervision of a resident physical
therapist (PT), indicated that there was considerable individual deviation on the continued use of the AT
device. The LW is also meant to enable frail elderly users who have difficulty walking to go outside and
enjoy themselves more. It was found, however, that this effect was achieved only when the physical
therapist intervened, gave encouragement, adjusted the bicycle settings as needed for the user, and otherwise
created new knowledge. It was also found that in order for this kind of knowledge creation to take place, the
bicycle must be used in an appropriate setting, the user needs to have a proactive attitude, and organizational
support to ensure that therapists are appropriately assigned is necessary.
1 INTRODUCTION
Between 2000 and 2050, the proportion of the
world’s population over 60 years will double from
around 11% to 22%. The absolute number of people
aged 60 years and over is expected to increase from
605 million to 2 billion over the same period (WHO,
2014). Japan is aging rapidly also. The population of
people 75 years or older will double over the next
two decades (Fukutomi et al, 2013), and the national
cost for medical care for those 70 years or older will
account for 45% (MHLW, 2011) of all medical cost.
Health promotion for this large cohort of aging
population is indispensable for building a
sustainable society.
Our perception of health has gradually changed
from a dichotomous to a salutogenic perspective. In
the former, health and disease are treated separately
and health is defined as being “low on risk factors”.
The latter, however, focuses on “keeping people
well”. From this perspective, health is viewed as an
ease/dis-ease continuum (Antonovsky, 1996). The
1986 Ottawa Charter for Health Promotion marks
one of the starting points of this change. Before the
87
Saijo M., Watanabe M., Aoshima S., Oda N., Matsumoto S. and Kawamoto S..
Knowledge Creation in Technology Evaluation of 4-Wheel Electric Power Assisted Bicycle for Frail Elderly Persons - A Case Study of a Salutogenic
Device in Healthcare Facilities in Japan.
DOI: 10.5220/0005136100870097
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2014), pages 87-97
ISBN: 978-989-758-050-5
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

charter was drafted, it was considered the
individual’s responsibility to maintain a healthy
lifestyle, but under the Ottawa Charter, health is
something to be achieved through a collaboration of
environment, community, personal skills, and public
policies. The Ottawa Charter initiated a redefining
and repositioning of institutions, epistemic
communities and actors within the disease-health
continuum (Kickbusch, 2003).
Frail elderly persons, especially those aged over
75 years, who tend to be the main users of aged care
services live in a dis-ease condition. Frailty is highly
prevalent in old age and poses a high risk of falls,
disability, hospitalization, and mortality (Fried et al,
2001). Falls are common and often devastating
among older people (Rubenstein, 2006). Walking is
a risk factor for falling, and yet walking is a basic
salutary factor in an individual’s life. Therefore, in
order to promote health among frail elderly persons,
optimal approaches involving interdisciplinary and
inter-agency collaboration are required to build an
environment in which such people can go out
without worry about falling.
While some people may have difficulty in
walking, they may still be able to ride a bicycle.
Already there are electric power-assisted bicycles on
the market that will allow the rider to climb steep
hills with ease, even if they do not have much foot
power. The power-assisted bicycles were originally
developed by the Yamaha Motor Company. The 4-
wheel assisted bicycle is a newly developed vehicle
which is safer than walking for frail elderly persons,
and is actually allowed on public roads as a
wheelchair. Its controls are set so that it will not
exceed a speed of 6 km per hour when going
downhill. With this vehicle, a person who cannot
walk can climb a hillside at the same pace as
someone walking at normal speed. Though
technically it is already available, this vehicle is not
yet on the market because there remain concerns of
its safety for frail elderly users.
In order to find salutogenic benefits in lifestyles
of the frail elderly, we undertook action research on
frail elderly people’s use of this 4-wheel electric
power assisted bicycle in a rehabilitation hospital in
the city of Kakegawa, Japan. As Antonovsky (1996)
said, we must start with the question, “How can this
person be helped to move toward greater health?”
This kind of effort must relate to all aspects of the
person, and the frail elderly adult is no exception.
We tackled this question through interdisciplinary
and inter-agency collaboration among manufacturer,
hospital, municipal government, and university.
2 LITEATURE REVIEW
2.1 Assessing Frailty in Elderly Persons
In order to provide appropriate care for frail elderly
persons covered by long-term care insurance (LTCI)
the Japanese Ministry of Health, Labour and
Welfare (MHLW) drew up a Kihon Checklist, a
basic health checklist, for those aged 65 and older, to
be used as a frailty index to predict the risk of
requiring care under LTCI. The checklist consists of
a 25-item, self-reported questionnaire, covering
seven categories including physical strength,
nutritional status, and oral function, as well as
houseboundness, mobility, cognitive function, and
depression risk (Fukutomi et al, 2013). Using this
checklist, municipal governments classify the frail
elderly persons in their communities according to
their need for preventive care. Kakegawa City
covers all 25 items on the questionnaire as well as
medical certificates to identify the frail elderly.
Figure 1 is a partial view of the checklist and its
screening criteria.
Municipal governments use the basic checklist as
a guide to decide their own criteria and procedures
for preventive care and care services, the dispatch of
helpers, the lending of wheelchairs, and the need to
provide rehabilitation. Care services are provided in
accordance with the degree to which acitivities of
daily life (ADL) have deteriorated. Table 2 shows
the assesement levels for LTCI. Persons classfied as
Support Level 1 and Support Level 2 are eligible for
preventive care. Table 2 was drawn up by the first
author as a simplified illustration of Japanese LTCI
assessment levels.
A few researchers have evaluated the validity of
this checklist to predict the risk of requiring care
(Fukutomi et al, 2013; Tomata et al, 2011).
Fukutomi, 2013, in particular, has suggested that
physical strength and cognitive function are more
useful indices for detecting the risk of future
deterioration of ADL. However, there is no
consideration of intervention to prevent future risk.
Frailty is defined as a clinical syndrome in which
three or more of the following criteria are present:
unintentional weight loss, self-reported exhaustion,
weakness (grip strength), slow walking speed, and
low physical activity (Fried, 2001). Geriatric
interventions have been developed to improve
clinical outcomes for frail older persons (Applegate
et al, 1990; Rubenstein, 2006). Maki et al, 2012, also
evaluated the efficacy of intervention by examining
a municipality-led walking program for the
prevention of mental decline in the elderly aged
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
88
72.0±4.0, in a randomized controlled trial. This
study introduced a 90-minute intervention program
consisting of 30 minutes of exercise and 60 minutes
of group work, and concluded that this intervention
program may provide benefits for some aspects of
cognition. Though their research target was not the
frail elderly, from the criteria in Table 1 and the
assessment level of LTCI we can easily surmise that
the frail elderly requiring LTCI are unable to
participate in this kind of walking intervention.
In these studies, some interventions were
implemented to evaluate the efficacy for improving
clinical outcome through randomized controlled
trials (RCT). Though RCT is a traditional evidence-
based methodology to examine the efficacy of
medical treatments or interventions in medicine, it
does not address the fact that frailty involves
multiple deteriorations, or that an elderly person’s
ability to take part in an intervention will vary
according to the context in which they live.
We need other methodologies to assess the
frailty of the elderly and to mitigate the
inconveniences in their daily life.
Table 1: Screening criteria for providing preventive care
(partial view of MHLW check list).
Mobility (those with top score of 3 points are candidates for preventive care) 0 point 1 point
Q6. Can you climb stairs without holding onto a handrail or wall? Yes No
Q7. Can you stand up from a sitting position without holding on to anything? Yes No
Q8. Can you walk continuously for 15 minutes? Yes No
Q9.Have you fallen within this one year? No Yes
Q10. Do you worry about falling down? No Yes
Cognitive functions (1 point or more required) 0 point 1 point
Q18. Do people around you say you repeat the same thing and have become forgetful? No Yes
Q19. Do you make phone calls by yourself? Yes No
Q20. Do you find yourself not knowing today’s date? No Yes
Depression (2 points or more required) 0 point 1 point
Q21. I do not feel any fulfillment in my daily life during the last two weeks. No Yes
Q22. I cannot enjoy things I used to enjoy during the last two weeks. No Yes
Q23. During the last two weeks, I am not willing to do what I could do easily before. No Yes
Q24. During the last two weeks, I do not feel I am useful to anyone. No Yes
Q25. During the last two weeks, I feel I am exhausted without any reason. No Yes
Table 2: Japan’s long-term care insurance assessment
levels (
△
○Yes, Partial, ×No).
Level Self-sufficient Body care Comprehension Behavior controlMobil
e
Support
Level 1
○
ᇞ
○ ○ ○
Level 2
○ ᇞ
ᇞ
○ ○ ○
L
TC
Level 1
ᇞ ᇞ
○ ○ ○
Level 2
ᇞ ᇞ
○ ○
ᇞ
Level 3
× ×
ᇞ ᇞ ᇞ
Level 4
× × × ×
ᇞ
Level 5
× × × × ×
2.2 Health Care in Tacit Knowledge
Since the 1970s, people have been given more room
to take the initiative in roles where they provide
expertise and participate in informing, ideating, and
conceptualizing activities in the early design phases
(Sanders and Stappers, 2008). This movement is
called user-centered design. For frail elderly people,
there are various assisted-technology (AT) devices
such as canes, walkers, and bath benches, as well as
wheelchairs, that could be considered to be user-
centered designs. As Mann et al (1999) notes, many
elderly persons rely on these devices.
NHS (the UK department of health) advocates
patient-led care and urges health care teams to move
from a service that does things to and for its patients
to one which is patient-led and which works with
patients to support them with their health needs
(Pickles, J., Hide, E., and Maher, L., 2008). AT
devices are provided to frail elderly people on the
assumption that the devices will promote their
independence and lower costs (Mann et al, 1999),
but there is little research on how much and what
kinds of frailty are mitigated by AT devices and
what kind of support is needed to make full use of
such devices. As some of the studies have pointed
out, an important part of health care consists of tacit
knowledge.
A significant part of health-care knowledge
exists in tacit form, for instance the working
knowledge of health care experts (Abidi, Cheah,
Curran, 2005). Abidi, Cheah, Curran, 2005, classify
tacit knowledge into 1) basic tacit knowledge or
routine experiential knowledge, and 2) complex tacit
knowledge or intuitive experiential knowledge. The
latter is “progressively accumulated as the expert
responds to atypical and high acuity clinical
problems–it is deeply embedded and, hence, not
easily articulated, yet manifests as the expert’s
intuitive judgment in challenging clinical situations.”
According to this classification, a health care
professional’s judgment of the usability of an AT
device for the frail user is inherent in the
professional’s tacit knowledge. The question is:
How can we extract this individual knowledge and
create new knowledge for patient-led care?
2.3 Knowledge Creation and
Technology Evaluation of AT
Devices
Knowledge creation starts with socialization, which
is the process of converting new tacit knowledge
through shared experiences in day-to-day social
interaction (Nonaka and Toyama, 2003). Nonaka
and Toyama also state that “knowledge creation is a
synthesizing process through which an organization
interacts with individuals, transcending emerging
contradictions that the organization faces”, and “one
can share the tacit knowledge of others through
shared experience” (Nonaka and Toyama, 2003). In
order to transform tacit knowledge to shared new
knowledge, socialization and efforts to transcend
KnowledgeCreationinTechnologyEvaluationof4-WheelElectricPowerAssistedBicycleforFrailElderlyPersons-A
CaseStudyofaSalutogenicDeviceinHealthcareFacilitiesinJapan
89

contradictions are needed. In professional health
care work places, medical doctors, nurses,
physiotherapists, and occupational therapists work
together. In this sense their routines consist of an
inter-agency, interdisciplinary collaborative
experience (Saijo et al, 2013). Also the main
contradictions in elderly health care are inherent in
the care itself. All human beings must eventually die,
but the care professional’s work is to challenge this
destiny. The need to transcend emerging
contradictions and shared experience are embedded
in their routines. The problem is how to elucidate
their tacit knowledge and reconstruct it to create new
knowledge. In this study, we describe this process
through a technology evaluation of a newly
developed 4-wheel electric power-assisted bicycle,
called a Life Walker or LW vehicle, for frail elderly
persons. This requires, however, that the health care
professional collaborate with outsiders, engineers
and researchers, to undertake the technology
assessment of the newly developed AT device.
Collaboration with outsiders requires socialization of
their mind or manners. We assume that this shared
new experience will extract their tacit knowledge to
create new knowledge in the methodology of caring
for frail elderly persons.
Technological evaluations of manual and
powered wheelchairs have already been made in the
field of anthropometry, the measurement of physical
characteristics and abilities of people (Paquet and
Feathers, 2004; Das and Kozey, 1999), with the
objective of acquiring information that is essential
for the appropriate design of a wheelchair. There is
little study, however, of the usability of a wheelchair,
or how it is actually used in real-world health care
circumstances. And there is no user-centered
technology evaluation of newly developed AT
devices for supporting the frail elderly on outings in
real-life circumstances with inter-agency and
interdisciplinary cooperation.
McNamara and Kirakowski (2005, 2006)
propose three aspects that need to be considered
from the viewpoint of user-centered technology
evaluation, namely, functionality, usability, and
experience. They state that these are unique but
independent aspects of usage. Functionality focuses
on the product and is evaluated by answering the
question, “What will the product do?” Usability is
defined by the ISO 9241-11 definition of usability as,
“the extent to which a product can be used by
specified users to achieve specified goals with
effectiveness, efficiency and satisfaction in a
specified context of use” (ISO 9241). Experience is
the individual’s personal experience of using the
device. The question asked here should perhaps be,
“How do I relate to this product?”
In this study of the Life Walker (LW), we apply
these aspects of technology evaluation to the
framework of knowledge creation. The aim of this
study is to elucidate the process of knowledge
creation among inter-agency and interdisciplinary
health care professionals, engineers, and researchers
in evaluating AT technology meant to promote
patient-led care among frail elderly persons.
3 RESEARCH METHODOLOGY
3.1 Research questions
In introducing the Life Walker (LW), a
microcomputer-controlled, 4-wheel, electric power-
assisted bicycle, to frail elderly persons certified as
requiring care in a rehabilitation hospital and a
daycare center for the elderly, we began with two
questions: (1) What conditions are necessary to have
an LW used in a hospital or daycare setting in such a
way that there will be knowledge creation, and (2)
How can the functionality, usability, and experience
of the LW be measured quantitatively and
qualitatively? The three categories in the second
question were further broken down into additional
questions as follows:
Functionality: What are the distinguishing
characteristics of the LW and what kind of
elderly person is it best suited for?
Usability: What kind of elderly person will ride
the vehicle and for how long?
Experience: What do the elderly persons and
care professionals experience through riding the
LW?
3.2 Case Study Method
We loaned the LW for two months to a rehabilitation
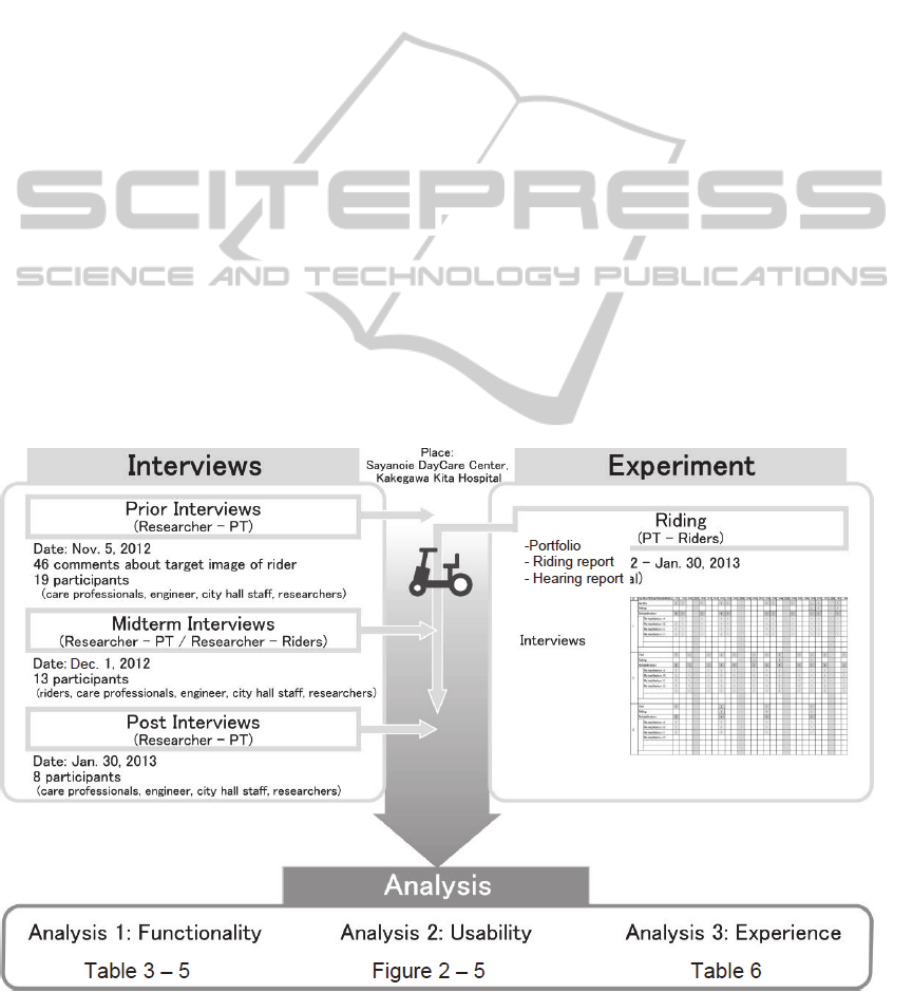
hospital and a daycare center for the elderly. Figure
1 shows the flow of data collection for this study.
• Period: Nov 5, 2012 to Jan 30, 2013
• Targets: 1) Frail elderly people (hereafter
“facility users”) in the Kakegawa Kita Hospital
and the Kakegawa City Sayanoie daycare facility
for the elderly. Facility users were rated at
Support Level 1 through LTC 4 level ; and
2) Hospital and daycare care professionals:
physiotherapists (PT), occupational therapists
(OT), care managers (CM), care workers (CW),
and social workers (SW)
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
90

• Methods: Questionnaire survey, test riding of
LW, and interviews of care professionals
The questionnaire for this study included the
following kinds of information. The authors
prepared a form that was filled out by the care
professionals (as it turned out, only PTs in the
rehabilitation hospital filled out the form). Also we
interviewed care professionals at both hospital and
daycare center.
Personal portfolio: Age, sex, care rating, dates at
facility, experience riding LW, type of
rehabilitation, continuing or interruption of LW
experience: PT’s predictions of whether each
facility user will become a continuing rider or
not.
Riding report: Rider’s basic checklist (if there
were multiple test rides, only changes from the
first ride were recorded), reason for test rides,
evaluation of driving skills
Recording of interview: The authors carried out
focus group interviews (FGI) of the care
professionals just before or after the loan of the
LWs and during the loan period.
The sub-categories of the research questions
were handled as follows.
3.2.1 Functionality
Functionality is a concept related to the technical
aspects of a product, and involves answering the
question, “What does the product do?” (McNamara
and Kirakowski, 2005, 2006)
The specifications of the LW vehicle used in this
study are as follows.
・Overall length x Overall width x Overall height:
1.190 mm x 655 mm x 990 mm
・Dry weight (with battery): 36 kg (38 kg)
・Tires: Sponge-type; do not blow out
・Drive system: dual electric-assisted run and full-
electric run
・ Control system: Microcomputer control with
motor controlled automatic brake
・Max forward speed: 6.0 km/h
・Max reverse speed: 0.5 km/h
When the rider is a healthy adult, the functions of
the vehicle are dependent on its specifications; while
there may be small divergences, the functions of the
vehicle do not change drastically among different
riders. The functionality of this vehicle as judged by
its specifications would be described thus:
With the electric-assist function, the vehicle can
be made to move forward with just light pressure on
the pedals. The vehicle can be stopped with
handbrakes or by simply removing one’s feet from
the pedals. Reversing is also possible. The vehicle is
pre-set so that it cannot go forward at a speed greater
than 6 km/h or reverse any faster than 0.5 km/h.
However, the users who are the subjects of this
study are all certified as requiring some level of
nursing care in their ADLs, as shown in Table 2, and
the functionality of the LW in the case of a facility
user greatly depends on the physical and mental
condition of the rider. Therefore, the question needs
to be revised to, “What kind of rider can move this
vehicle?” It must also be pointed out that since the
LW is not yet available on the commercial market,
facility users have no analogy with their past
experiences to refer to.
In FGIs carried out prior to the test riding of the
LW, we asked the health care professionals routinely
caring for the facility users what kind of person they
felt was suitable for this vehicle. During the loan
period of LW vehicles, we asked for volunteers
among the care professionals who would be willing
to encourage facility users to ride the LW. We then
asked them to predict whether each rider would
continue to ride the LW or not. Later, we included
these predictions in the personal portfolio.
3.2.2 Usability
Usability, according to ISO is defined as “the extent
to which a product can be used by specified users to
achieve specified goals with effectiveness,
efficiency, and satisfaction in a specified context of
use.” In this study, we created a histogram and
accumulated data chart comparing the riding rates of
continuous riders and those who discontinued riding,
a histogram of riding rates (number of rides / days at
facility) by attributes (sex, age cohort, care level) to
clarify what kind of people rode the LW at what
frequency. The effectiveness of the rides should also
be measured in terms of physical and mental effects,
but that is not within the scope of this study.
3.2.3 Experience
According to McNamara and Kirakowski (2005,
2006), judging experience requires answering the
question, “How do I relate to this product?” The
facility users who tried out the LW required
assistance in their ADLs, but they nevertheless made
the decision to ride the LW, tried it out several times,
and then decided to either continue or discontinue
riding during the period in which the vehicle was on
KnowledgeCreationinTechnologyEvaluationof4-WheelElectricPowerAssistedBicycleforFrailElderlyPersons-A
CaseStudyofaSalutogenicDeviceinHealthcareFacilitiesinJapan
91
loan to the facility. By keeping a record of their
reasons (for deciding to continue or discontinue use),
it was possible to learn what they found appealing,
or conversely, what they found to be a problem,
about the LW. Likewise, it was possible to find out
how they were influenced to try out the experience
of riding the LW. This data was collected by the
authors from the riding survey tables and through
interviews carried out after the vehicle loan period.
This study was carried out only after it had been
reviewed and approved by the ****************
research ethics committee. (authorization NBR:
2012021)
4 RESULTS
4.1 Circumstances which Elucidate
Knowledge Creation
In this experiment, not one facility user at the
daycare center attempted to ride the LW. At the
rehabilitation hospital, there were 61 users who rode
the vehicle. This result indicates that, without
exception, there was no knowledge creation
generated by the loan of the new AT device to the
daycare center. The following is an excerpt from an
interview related to this.
(D: Daycare Center Director; 1st: First Author;
2nd: Second Author; Ci: City Hall staff; En: LW
Engineer)
PT: When the vehicle was demonstrated, there
were two people who expressed interest, but they
never tried to ride the vehicle themselves.
D: They were told it was OK to ride the vehicle,
but the one person who we thought might be a
good candidate to try it out became sick and that
made a trial difficult.
1st: Yes, it may be difficult without an
atmosphere that this might become popular
within the facility.
PT: There was no word-of-mouth encouragement.
1st: If at least one person had tried it out, and
said it was fun....
PT: Yes, if that sort of thing had happened we
might have seen different results. But it didn’t
turn out that way, I’m sorry.
D: Persons who are undergoing rehabilitation are
working hard to resume their normal life, so for
someone like that a vehicle that they can pedal
on their own is appealing. There is a difference
between simply wanting to maintain your current
lifestyle such that, for example, even if you can’t
drive a car yourself, you can use a wheelchair or
your family will drive you, or you can have
groceries delivered, and being motivated to go
Figure 1: Flow of Data and Analyses.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
92
out on your own to do something. There is a
difference of drive and energy between the
two. ...
2nd: Apparently, people were reluctant to try out
the vehicle because they were told they could not
ride it outside. But even though they were
allowed to use it within the facility, no one tried,
so we were not able to find out how they might
have used the vehicle.
D: Given the size of the vehicle, it is not
surprising that people were reluctant to ride it
inside the facility. It is hard to imagine riding on
the LW through the same hallways in which
people are in wheelchairs, or walking, or even
just standing because they can’t walk. It doesn’t
seem reasonable to expect people to ride
smoothly inside a hospital.
Ci: I think it would be embarrassing, too. You
would have to have courage.
1st: You would stand out and you would feel
constrained to have to sweep by the other people.
D: A wheelchair would feel more natural. Two-
wheelers and 3-wheelers are what feel out of
place.
Ci: But if you get used to it, it wouldn’t be so
bad.
En: In America, people ride mobility scooters
[called “senior cars” in Japan] inside hospitals.
Ci: [It would be nice] if everyone could get used
to it that way.
(2013 Jan 30, Post interview FGI: Sayanoie
Daycare Center)
The daycare center is a place where elderly
persons certified as requiring care can spend time
during the day. They do not come to the center with
a specific purpose in mind, such as those who go to
the rehabilitation hospital, and there are no specified
activities for each individual. Still, just like at the
rehabilitation hospital, the daycare center PTs and
OTs did demonstrate the vehicle, riding the LW
themselves and inviting the facility users to do the
same. No one took them up on the invitation,
however. This indicates how important it is to have
someone try out the vehicle first in order to
disseminate use of the new AT device. Also, as
indicated in the interview excerpt above, the
conditions for health care knowledge creation in this
particular case are that facility users are highly
motivated to go outside, are proactive in their
lifestyles, and are not embarrassed to use the vehicle
inside the facility.
4.2 Functionality
4.2.1 The Type of Frail, Elderly Person for
Whom the LW Is Best Suited
Table 3 shows the characteristics that emerged from
the prior interview that best describe the type of
elderly person who would be able to make use of the
LW. As was shown in Figure 1, we collected 46
comments from interviews with care professionals.
Comments that were basically the same were
combined into one.
Table 3: Target image of frail elderly persons who are best
suited to use the LW vehicle.
Occupation ID Target image
CM S Forward-looking person
CM
S Candidate for secondary preventive care
CM
S
Person requiring preventive care or support as opposed to a
regular daycare user
CM
S
Person who is being taken care of by a general support
center (preventive care)
CM
S Person who wants to undergo rehabilitation
CM
S Person who can walk using a cane
CM
S
Person who thinks they can still ride a bicycle or who uses a
bicycle like a cane, but who others do not believe is actually
capable of riding a bicycle
CM
S
A relatively healthy elderly person who still farms (such as
in mountain valley areas or in tea fields)
CM
S Person who has not yet ridden a mobility scooter
CM
T
Person with relatively strong legs who can pedal (including
those with dementia)
PT A
Person who is mobile near the home using a cane or walker
but who has difficulty going further afield
PT
SW
Person who uses machines or bicycles for physical training
and rehabilitation
PT
A
Person who thinks they will be able to go outside if they
have this kind of vehicle
CW M Anyone who shows interest; anyone who likes vehicles
SW N
Person who is still riding bicycles but is losing confidence
in their ability to do so
Facility
director
IN
Person who doesn’t want to depend totally on a mobility
scooter
While no quantitative analysis has been made,
the comments shown in Table 3 contrast the target
image held by PTs and care managers. The PTs
speak of the facility user’s behavior and
psychological factors while the care managers tend
to base their target image on external markers such
as the facility user’s level of care, AT device, and
even occupation. Nevertheless, as will be
demonstrated in the next section on usability, these
kinds of external markers are not effective measures
of a user’s suitability for riding the LW.
4.2.2 PT’s Predictions of Whether a User
Will Continue or Discontinue Riding
Table 4 shows the PT’s predictions and actual
results of facility users’ continuity of riding. The rate
of accuracy of the PT’s predictions was around 50%.
KnowledgeCreationinTechnologyEvaluationof4-WheelElectricPowerAssistedBicycleforFrailElderlyPersons-A
CaseStudyofaSalutogenicDeviceinHealthcareFacilitiesinJapan
93
In Table 4, the “Neither” category indicates those
who rode only sporadically and for whom the PT
had difficulty deciding which category (continue or
discontinue) they belonged to.
Table 5 indicates the reasons for the PT’s
predictions. The numbers above the double line are
the PT’s predictions and the numbers below, the
actual results. The figure under “Prompt” indicates
the number of users the PT believed would respond
to or not respond to prompting. The criteria
“Prompt”, “Proactive”, and “Initiative” proved to be
effective measures for deciding whether a user was
likely to continue using the LW or not, but it was
found that the other criteria, “Willingness”
(willingness to try anything new), “Interest” (interest
in the LW vehicle), “Medical/physical condition”
(today’s condition), were not very effective
measures for judging a person’s reaction to the LW
vehicle. The reasons were recorded in the personal
portfolios, with each reason categorized in the 8
categories shown in Table 5. The PT sometimes
gave several reasons for a prediction, so the total
number of reasons is not the same as the total
number of riders.
Table 4: Rate of accuracy of PT’s prediction.
Result
Prediction
Continued Discontinued Total
Continue 31.1% 19.7% 50.8%
Neither 9.8% 14.8% 24.6%
Discontinue 6.6% 18.0% 24.6%
Total 47.5% 52.5% 100.0%
Table 5: Reasons for prediction by category.
Category
Prompt
Willingness
Proactive
initiative
Interest
Fear
Bicycle
Medical /
Physical
condition
All 10 11 12 7 19 3 5 9
Continue 7 6 8 5 5 0 1 2
Neither 3 1 2 1 7 0 2 1
Discontinue 0 4 2 1 7 3 2 6
4.3 Usability
The breakdown of the users who tried out the LW
vehicle in the rehabilitation hospital is as follows:
Age: 65-74: 22; 75-above: 39. Men: 36; Women: 25.
Care level: Support Level 1– LTC Level 4.
The number of days that a user came to the
facility varied according to the individual’s care
level and medical condition. In order to determine
what kind of persons rode the LW vehicle and to
what extent, it was necessary to calculate the rate of
riding by dividing the number of rides by the
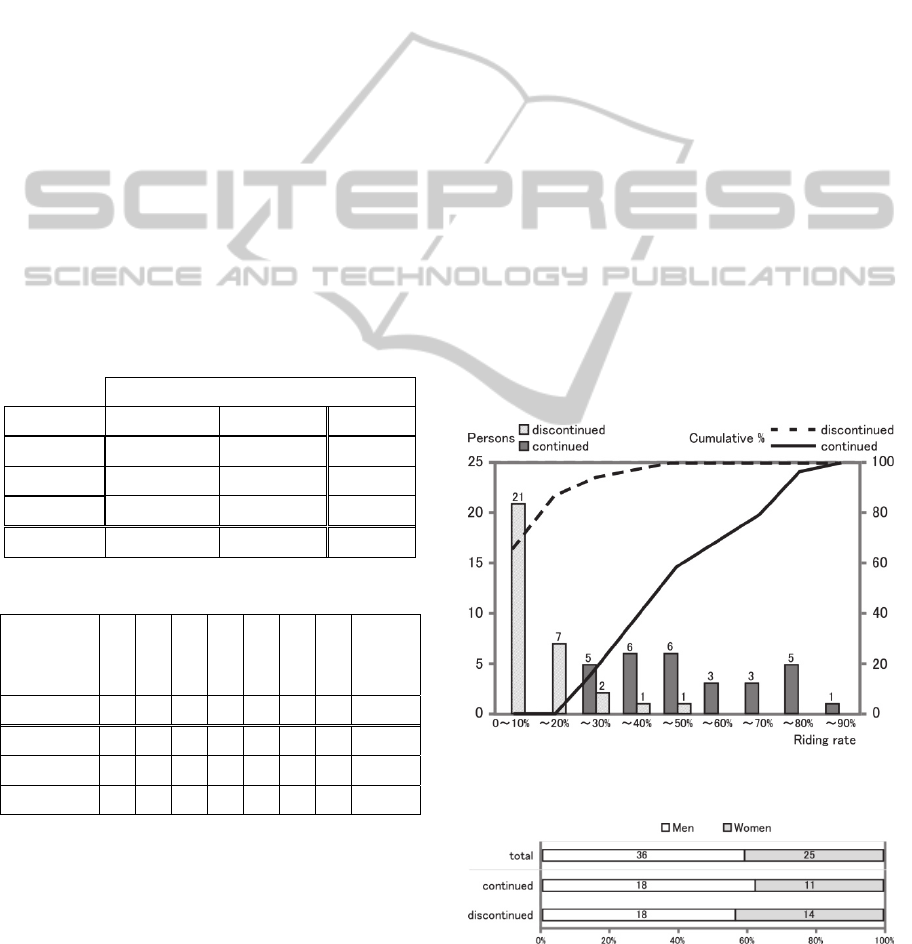
number of days at the facility. Figure 2 compares the
riding rates and accumulated riding rates of those
who continued to ride against those who
discontinued. Those who continued where persons
who may have taken several breaks, but who
nevertheless continued to ride the LW vehicle
throughout the period it was on loan to the
rehabilitation hospital. Those who discontinued were
persons who tried out the vehicle a few times but
then stopped riding. There were only 4 riders in the
“Neither” category so we traced their record of
riding and re-categorized them in “continued” or
“discontinued”.
Looking at Figure 2, you can see that most of
those who discontinued riding generally did so after
they had reached a riding rate of around 20% (4
times). This indicates that the users were able to
judge by their fourth ride whether or not the LW
vehicle suited them. Those who continued to ride are
distributed between 20% to 90%, and half exceeded
a riding rate of 50%, indicating that they rode the
LW vehicle at least half of the days that they came
to the hospital.
Figure 2: LW riding rate and accumulated riding rate by
continued / discontinued category.
Figure 3: Rates by sex.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
94
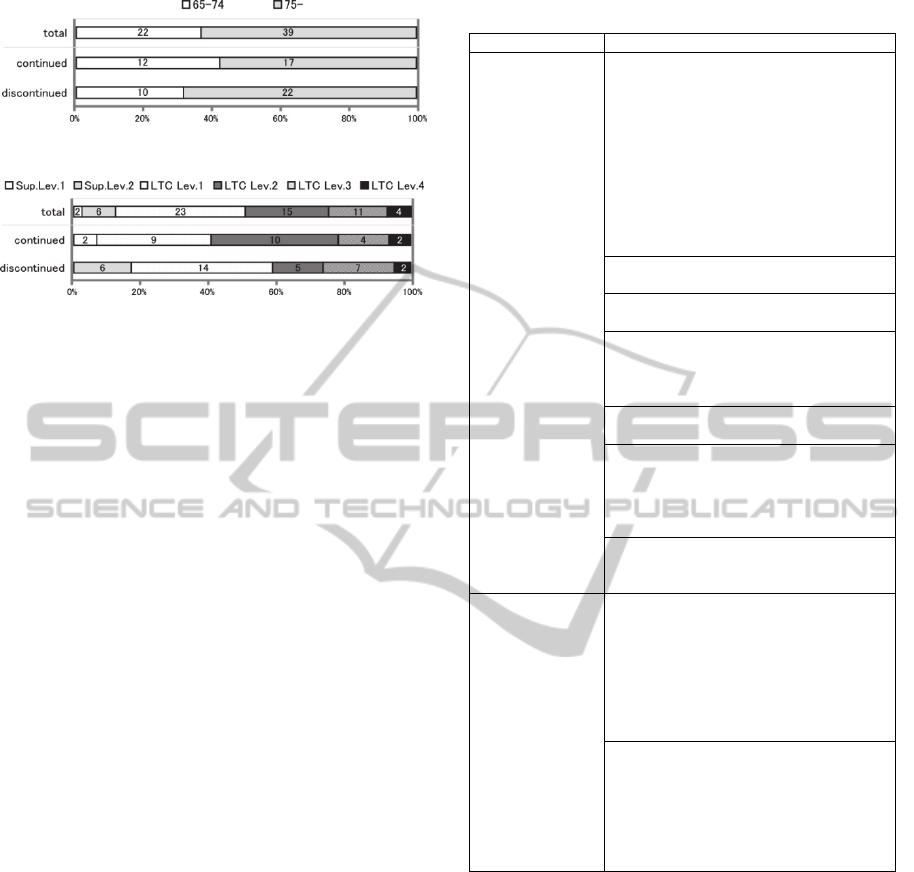
Figure 4: Rates by age cohort.
Figure 5: Rates by care level.
Figures 3 through 5 indicate that more men than
women, and those older than 75 as compared to
those age 65 to 75, were likely to continue riding. In
terms of care levels, the greatest number of
continuing riders spans LTC Levels 1, 2 and 3, while
most of those at the less demanding care levels of
Support Levels 1 and 2 did not attempt to ride the
vehicle.
4.4 Experience
The most common reasons cited by users in their
personal portfolios for riding the LW vehicle were:
because I was encouraged to do so by the PT,
because it looked like fun, because I want to build
up some muscle, because I saw or heard about
someone riding, and because I want to be able to
ride a bicycle. Those who continued riding gave as
their reasons for doing so: able to go outside, fun,
encouraged to do so, condition was good, etc. Those
who discontinued riding gave as their reasons: hard
to ride, tiring, too slow, condition was poor, etc. As
was noted earlier, almost all of the 61 riders at the
rehabilitation hospital rode the LW vehicle at least
four times, suggesting that the PT’s encouragement
was a major factor in securing so many riders.
Below are some of the comments made in an FGI of
the rehabilitation hospital PTs during the experiment.
What these comments tell us is that the
rehabilitation hospital assigned staff specifically to
help with the trial rides, repeatedly encouraged users
to try out the vehicle, made adjustments as necessary
to ensure a smoother ride, called out a beat to give
the rider a rhythm by which to pedal, and otherwise
made proactive efforts to act as an interface between
the rider and the LW vehicle.
Table 6: PTs’ comments in midterm interview.
Topics Comments
Trial rides Start by gathering everyone together,
saying “Would you like to ride it? Let’s try
it.” Have a person get on the vehicle, show
them how to operate it and walk by them
as they go a few rounds. On the first ride,
the rider goes a few turns and tries out all
the vehicle’s functions. Each individual is
asked if they want to give it a try, and a
staff person accompanies each person who
decides to try riding. Once one person is
done, the next person is brought forward.
Those who want to try a second ride are
contacted by the facility staff.
Those who ride two or three times tend to
continue riding.
A common characteristic of those who
continue riding is that they are self-
sufficient at home but have difficulty
going out on their own.
These were mostly persons at support
level 1 and nursing care level 2.
There were some care level 3 people who
tried out the vehicle, but they generally
needed assistance in controlling the
vehicle, and some had to have help to keep
their feet on the pedals.
Those who had disabilities of their hands
or feet had difficulty controlling the
vehicle.
Encouragement
from hospital staff
during the
trial ride
Progress is uneven during the trial rides,
but we tried to encourage the rider by
helping them with rhythm, for example,
calling out, “One, two, one, two” each
time they stopped pedalling. The usual
staff worked with the riders [so they had
people they were familiar with helping
them out]
After the rider got on the vehicle, the seat
was adjusted (height, etc.) to ensure a
comfortable ride. It was slightly different
from adjusting a bicycle seat, but the staff
kept communicating with the rider, asking
“How does it feel?” and so on, and making
minor changes as needed.
(2012 Dec 1, Midterm FGI interview, Kakegawa Kita
Hospital)
5 CONCLUSIONS
As a new AT device, we found that the LW vehicle
could be fun and highly satisfactory to frail elderly
users who had difficulty walking on their own or
going outside. But this was an experience that could
not have been achieved without the interaction
between the PTs and the users. The PTs provided
encouragement, helped in adjusting the vehicle
settings, made judgments as to who might be suited
to ride the vehicle, and otherwise created new
knowledge to guide frail elderly persons to using the
KnowledgeCreationinTechnologyEvaluationof4-WheelElectricPowerAssistedBicycleforFrailElderlyPersons-A
CaseStudyofaSalutogenicDeviceinHealthcareFacilitiesinJapan
95

vehicle. In order for this kind of knowledge creation
to take place, it is imperative that the organization
provide an environment suitable for the use of the
device, that the user be proactive, and that dedicated
staff be appropriately assigned to assist as necessary.
In the setting of the rehabilitation hospital where
PT supervision was available, it was found that the
LW vehicle was best suited to users at LTC Levels 1
to 3 who were over the age of 75. At the same time,
there was considerable discrepancy among
individuals as to whether they would continue or
discontinue use of the vehicle. It was also found that
it was difficult for PTs to predict who would or
would not continue riding, and in this regard there is
a need for new knowledge creation.
The primary focus of the salutogenic perspective
on health is the individual’s ability, right up to the
time of death, to adapt to his or her own condition as
necessary to stay in good health. Today, there are a
variety of devices that support this ability. The more
devices that are made available to frail elderly
persons, the easier it will be to realize the kind of
health that is the focus of this perspective.
Unfortunately, major manufacturers are reluctant to
develop new products for the over-75 market
because of the fear of accidents and the probability
of being sued as a result. Still, the market for devices
for the over-75 age cohort is certain to expand and
there is ample room for innovation based on new
knowledge creation. As this study has shown, having
a new device evaluated within the context of a care
facility serves as an impetus to transform the tacit
knowledge of professional caregivers to explicit
knowledge. This requires, however, close
collaboration among the device maker, researchers,
and caregivers. In the current study, the city hall
staff also played an important role as intermediaries
bringing together diverse professionals and the staff
of the care facilities.
There are three topics that this study must
undertake in the future.
(1) Accurate measurement of effectiveness which
is a critical index for judging usability. We
need to elucidate the psychological and
physical effects of continuous use of the LW
vehicle.
(2) We need to provide a method, such as a
rehabilitation menu, by which care managers,
who are not as knowledgeable as PTs about
nursing care, can judge who is best suited to
use the LW vehicle.
(3) We need to consider what kind of knowledge
creation is needed to enable users to ride the
LW vehicle outside of the facilities.
REFERENCES
Abidi, S. S. R., Cheah, Y. N., Curran, J., 2005. A
knowledge creation info-structure to acquire and
crystallize the tacit knowledge of health-care experts.
Information Technology in Biomedicine. IEEE
Transactions, 9(2), 193-204.
Antonovsky, A., 1996. The salutogenic model as a theory
to guide health promotion. Health Promotion
International, 11(1), 11-18.
Applegate, W. B., Miller, S. T., Graney, M. J., Elam, J. T.,
Burns, R., Akins, D. E., 1990. A randomized,
controlled trial of a geriatric assessment unit in a
community rehabilitation hospital. The New Journal of
Medicine, 1572-1578.
Das, B., Kozey, J. W., 1999. Structural anthropometric
measurements for wheelchair mobile adults. Applied
Ergonomics, 30(5), 385-390.
Fried, L. P., Tangen, C. M., Walston, J., Newman, A. B.,
Hirsch, C., Gottdiener, J., Seeman, T., Tracy, R., Kop,
W. J., Burke, G., McBurnie, M. A. for the
Cardiovascular Health Study Collaborative Research
Group, 2001. Frailty in older adults: evidence for a
phenotype. Journal of Gerontology Medical Sciences,
56 A (3), M146-M156.
Fukutomi, E., Okumiya, K., Wada, T., Sakamoto, R.,
Ishimoto, Y., Kimura, Y., Kasahara, Y., Chen, W.,
Imai, H., Fujisawa, M., Otuka, K., Matsubayashi, K.,
2013. Importance of cognitive assessment as part of
the Kihon Checklist developed by the Japanese
Ministry of Health, Labour and Welfare for prediction
of frailty at 2-year follow up. Geriatrics and
Gerontology International, 13(3), 654-662.
ISO 9241, 1998., Ergonomic Requirements for Office
Work with Visual Display Terminals: Part 11:
Guidance on Usability.
Kickbusch, I., 2003. The contribution of the world health
organization to a new health and health promotion.
American Journal of Public Health, 93, 383–388.
Maki, Y., Ura, C., Yamaguchi, T., Murai, T., Isahai, M.,
Kaiho, A., Yamagumi,T., Tanaka, S., Miyamae, F.,
Sugiyama, M., Awata, S., Takahashi, R., Yamaguchi,
H., 2012. Effects of intervention using a community-
based walking program for prevention of mental
decline: A randomized controlled trial. Journal of the
American Geriatrics Society, 60(3), 505-510.
Mann, W. C., Ottenbacher, K. J., Fraas, L., Tomita, M.,
and Granger, C. V., 1999. Effectiveness of assistive
technology and environmental interventions in
maintaining independence and reducing home care
costs for the frail elderly: A randomized controlled
trial. Archives of Family Medicine, 8(3), 210-217.
McNamara, N., Kirakowski, J., 2005. Defining usability:
quality of use or quality of experience? In
International Professional Communication Conference
Proceedings, IEEE. 200-204
McNamara, N., Kirakowski, J., 2006. Functionality,
usability, and user experience: three areas of concern.
Interactions, 13(6), 26-28.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
96

Ministry of Health, Labour and Welfare, 2011. Act for
partial revision of the Long-Term Care Insurance Act,
Etc., in order to strengthen long-term care service
infrastructure; 2011. Available at: http://www.mhlw.
go.jp/english/policy/care-welfare/care-welfare-elderly/
dl/en_tp01.pdf.
Nonaka, I., Toyama, R., 2003. The knowledge-creating
theory revisited: knowledge creation as a synthesizing
process. Knowledge Management Research and
Practice, 1(1), 2-10.
Paquet, V., Feathers, D., 2004. An anthropometric study
of manual and powered wheelchair users. International
Journal of Industrial Ergonomics, 33(3), 191-204.
Pickles, J., Hide, E., Maher, L., 2008. Experience based
design: a practical method of working with patients to
redesign services. Clinical Governance: An
International Journal, 13(1), 51-58.
Rubenstein, L. Z., 2006. Falls in older people:
epidemiology, risk factors and strategies for
prevention. Age and Ageing, 35(S2), 37-41.
Saijo, M., Suzuki, T., Watanabe, M., Kawamoto, S., 2013.
An analysis of multi-disciplinary & inter-agency
collaboration process: case study of a Japanese
community care access center, KMIS 2013, 66, 470-
475.
Sanders, E. B. N., Stappers, P. J., 2008. Co-creation and
the new landscapes of design. CoDesign, 4(1), 5-18.
Tomata, Y., Hozawa, A., Ohmori-Matsuda, K., Nagai, M.,
Sugawara, Y., Nitta, A., Kuriyama, S., Tsuji, I., 2011.
Validation of the Kihon Checklist for predicting the
risk of 1-year incident long-term care insurance
certification: the Ohsaki Cohort 2006 Study. Nippon
Koshu Eisei Zasshi, 58(1), 3-13. (In Japanese)
World Health Organization, 2014. Ageing and Life Course,
Available at: http://www.who.int/ageing/en/.
KnowledgeCreationinTechnologyEvaluationof4-WheelElectricPowerAssistedBicycleforFrailElderlyPersons-A
CaseStudyofaSalutogenicDeviceinHealthcareFacilitiesinJapan
97
