
IT-Structures and Algorithms for Quality Assurance in the
Medical Advisory Service Institutions in Germany.
Step 2: To err is Human. Consensus-Conferences
Vera Ries
1,*
, Klaus-Peter Thiele
1
, Bernhard van Treeck
2,†
, Sarah Schroeer
1
,
Christina Witt
1
and Reinhard Schuster
2
1
Medical Advisory Service Institution in North Rhine (MD Nordrhein), 40212 Duesseldorf, Germany
2
Medical Advisory Service Institution in Northern Germany (MD Nord), 23554 Luebeck, Germany
Keywords: Quality Assurance, Statutory Health Insurance, Medical Advisory Service Institution, Communication
Structures Between Different IT-Systems, Server Data Structures, Data Protection, Script Programming,
Client Office Answers Using Perl Modules, Integer Linear Programming, Consensus, Quality Benchmark,
Positive Criticism, Pseudonym-Protected Knowledge Transfer.
Abstract: 16 Regional Medical Advisory Service Institutions perform medical expertise assessments upon German
in- and out-patient care. Assessments have to accomplish a nationwide quality assurance plan with mandatory
public reporting. We developed strategies to resolve conflicting quality measurement evaluations in the same
item by different peers without unveiling the identity of the criticised medical expert or peer in the processes.
All workflows are completely digitalized using mathematical IT-based procedures for randomized sampling
and for an equal distribution of the medical expertise assessments to be reviewed. We even allow for smaller
sample sizes, so regional heterogeneity and the heterogeneity of the types of medical expertise assessment
pose a constraint satisfaction problem. We discuss models addressing this kind of problem type and present
possible solutions. Our technical framework for peer review distribution, data collection and final result
analysis includes a completely IT-based workflow not only masking the origin of the medical expertise
assessments discussed, but routing the peer review processes in a way that independent and impartial review
sheets are produced by peers that were previously not yet involved in the reviewing process. Finally, the
statistical distribution and outcomes of the review results are analysed.
1 INTRODUCTION
To err is human and occurs among medical experts as
well. Our aim is to establish a continuous mutual
learning situation within a benchmark framework for
a nationwide quality assurance plan covering all
medical expertise assessments performed by the
Medical Service Institution. We present a valuable
tool creating maximum transparency of outcomes but
founded on positive criticism without blaming
individual institutions or individual medical experts.
This quality initiative is unique in Europe by
creating nationwide outcome quality assurance
standards within the legal institutions that advise the
German health care insurance funds in declaring cost
*
https://md-nordrhein.de
†
https://md-nord.de
assumption for health care service. The health care
providers deserve that the legal institution appraising
quality benchmarks its own performance.
This innovative project was initiated in November
2016 by the head physicians' board of the 16 Regional
Medical Advisory Service Institutions (MD). In 2018,
a mutual agreement was reached regarding the quality
objectives, the criteria applied and the central IT
platform conception, its architecture and technical
workflow implementation (Ries et al., 2021). The
nationwide implementation started from November
2019 and will be accomplished by April 2023.
Meantime, the self-initiated nationwide quality
assurance became mandatory by a law amendment of
the German Social Code in December 2019 (Merkel
and Spahn, 2019).
Ries, V., Thiele, K., van Treeck, B., Schroeer, S., Witt, C. and Schuster, R.
IT-Structures and Algorithms for Quality Assurance in the Medical Advisory Service Institutions in Germany. Step 2: To err is Human. Consensus-Conferences.
DOI: 10.5220/0011632600003414
In Proceedings of the 16th International Joint Conference on Biomedical Engineering Systems and Technologies (BIOSTEC 2023) - Volume 5: HEALTHINF, pages 271-278
ISBN: 978-989-758-631-6; ISSN: 2184-4305
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
271

2 LEGAL FRAMEWORK
The 16 Regional Medical Advisory Service Institu-
tions performing medical health care expertise are
legally established by the German social legislation
(Gaertner and Gnatzy, 2011). A pre-existing peer
review based quality assurance system was mandated
by law in 2004, but restricted on long term care as-
sessments (Schmacke, 2016). The current nationwide
quality assurance plan's initiative started in 2016
(Ries et al., 2021) and was mandated by law ex post
in 2019 (Merkel and Spahn, 2019), adding a supple-
mentary advisory service institution.
2.1 Getting Started
In analogy to industrial quality standards for pro-
duction, quality is defined to measure the degree of
correspondence between the service provided by a
supplier and the service expected by the customer
(Masaaki, 1986; Gerlach, 2001; Kamiske and Brauer,
2011; Institute of Medicine, 1990 and 2001; Interna-
tionale Organisation fuer Normung, 2015).
The aim here was to review the kaleidoscope of
singular quality assurance measures regionally
performed and to merge it into one mutual commit-
ment based nation-wide quality perspective. Based on
this conception, a new quality assurance plan for
medical expertise assessments started in 2019, ad-
dressing the two main topics for medical expertise
assessments:
In-patient care:
hospital quality and billing control on behalf
of the health care insurance funds (Thiele et
al., 2018; Kreuzer et al., 2022);
Incapacity for work in out-patient care:
case management consultancy and medical ex-
pertise assessment in insurance questions aris-
ing in the area of incapacity for work service
(Nuechtern, 2008; Nuechtern und Mittelstaedt,
2015; Ries et al., 2022);
By choosing those two assessment topics, more
than 70 % of all medical expertise assessments were
covered within the pilot phase.
2.2 Rollout Schedule
By April 2024, the quality assurance plan covers all
medical expertise assessments performed on all
medical topics (Gostomzyk and Hollederer, 2022):
factual or putative medical treatment errors;
dental medicine / oral maxilla-facial surgery;
prevention and rehabilitation;
medical assistance supplies and prostheses;
plastic surgery, bariatric surgery, gender reas-
signment surgery;
psychotherapy, occupational therapy, speech
therapy, physiotherapy, intermittent home
nursing, palliative home care, hospice care;
new and unconventional diagnostic and thera-
peutic methods or medical devices, drug pre-
scription and drug treatment.
3 CHALLENGES
We had to solve challenging distributional problems.
3.1 Regional Heterogeneity
Germany is characterised by a huge regional and
sociodemographic heterogeneity of the 16 federal
states, leading to 20 % of the population agglomerate-
ing in North Rhine Westphalia, but five other institu-
tions in federal states representing less than 4 % of the
population, either due to their historically profiled
tiny regional size (Saar, Bremen) or to their rather
scarce population density (former Eastern Germany).
This creates institutional size variations from 100 to
up to 1.500 employees per regional institution.
3.2 Structural Heterogeneity
Our innovative workflow validates the internal quali-
ty assurance within the regional advisory service in-
stitutions in a double-check way by the external quali-
ty assurance of another advisory service institution,
creating a new and nationwide perspective.
Putting this challenging aim into reality was
further complicated by the heterogeneity of the IT-
systems. To tackle this problem, we implemented a
web-based portal that can be reached by any software
solution, processing data from different assessment
databases.
Conflicting regional legal regulations on data
protect-tion are posing a constant challenge for
cooperation on a nationwide level.
4 ACCOUNTING FOR INEQUITY
4.1 Adaption of Sample Size
The quantity structure of the nine topics of health care
benefits leads to more than 70 % of all assessments
performed in the single field of in-patient care, being
2.5 million medical expertise assessments per year.
HEALTHINF 2023 - 16th International Conference on Health Informatics
272
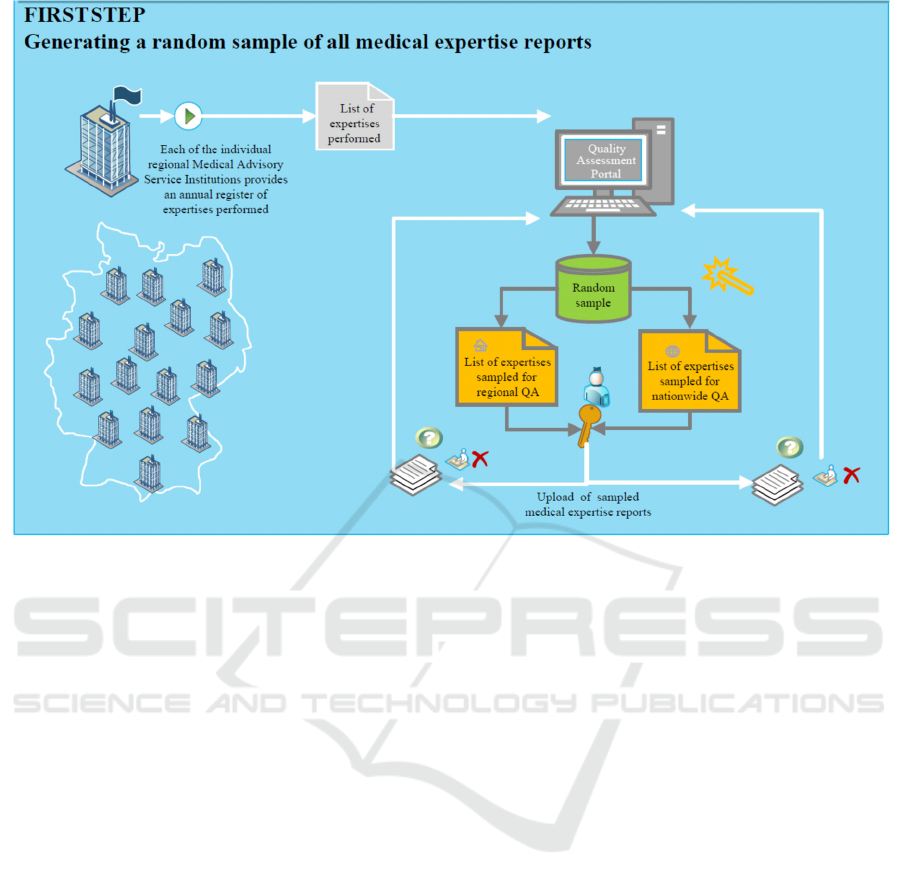
Figure 1: IT-architecture: Performing two quality reviews for a 10 % subset of the 0,5 % sample of all expertise assessments
performed by each of the 16 Medical Advisory Service Institutions.
A random sample of 0.5% is chosen for re-
gional quality assurance using peer reviews.
10 % of the previously chosen assessments are
randomly chosen for a double check peer re-
view by another regional institution genera-
ting the nationwide perspective.
This sampling leads to 12,500 regional peer reviews
and 1,250 nationwide peer reviews for in-patient care.
The remaining medical treatment topics generate
only a total of 650.000 assessments per year. For
reliability, we fixed minimal random sample sizes to
112 per year for regional quality assurance;
56 of the previously chosen assessments for a
double check peer review.
Since the peer review process is organized quarterly,
this provides every participant with a review by any
of the other participants in a quarterly rhythm,
validating internal quality assurance results.
4.2 Positive Criticism
Even this rigorous reduction was not yet feasible for
the five federal states representing less than 4 % of
the population, so we had to further reduced it to
56 per year for regional quality assurance and
28 randomly chosen for double check review.
From a psychologic point of view, it was
revealing that this concern was concealed by the
participants in the regular meetings of the quality
assurance working group, but proclaimed "out of the
blue" by the executive board.
This incident acted as an eye-opener to us. Quality
assurance management is a communication process,
first and foremost. Obviously, we had not yet
managed to create that situation of mutual trust and
learning within our working group that is crucial to
allow individual participants to raise word to focus on
important short-comings of the process.
Background analysis initiated by quality outcome
discussions reveal structural variations or even space
for clarifying procedural questions. Therefore, at least
one member of the corresponding medical expert
committee for the topic takes part in the consensus
conference, as well as at least one member of the head
physicians' board.
4.3 Pseudonym-Protected Knowledge
Transfer
Nobody wants to get passed on the red lantern, so it
is crucial to create an environment of positive
criticism and trustful mutual learning preventing the
participants of feeling embarrassed by raising
concerns or outing important short-comings (Beau-
champ and Childress 2001;
Varkey, B. 2021). A user-
friendly and trustful shaping of the quality assurance
IT-Structures and Algorithms for Quality Assurance in the Medical Advisory Service Institutions in Germany. Step 2: To err is Human.
Consensus-Conferences
273
communication process remains a constant quest
(Woodward, 2019). The nationwide quality assurance
plan conceals the identity of the peer reviewer and the
provenance of the medical expertise assessment.
Quality measurement and validation takes place
comparing all double-check review sheets, i. e.:
The internal review sheets: self-evaluation
review by an experienced peer within the
regional medical advisory service institution of
provenience.
The external review sheets: impartial
evaluation by an experienced peer belonging to
another regional medical advisory service
institutions.
5 IT PROCESSES FOR THE
CONSENSUS CONFERENCE
5.1 Structured Quality Review
The review sheets are composed of 20 core quality
criteria for all topics of health insurance benefits.
Several topics add specific quality criteria to check in
depth for medical accuracy in complex medical
assessment procedures like drug administration,
transsexualism or dental surgery.
Quality criteria ratings are colour-coded as
"adequate" green, "potential for improvement"
yellow and "inadequate" red. Synoptic review sheets
contrasting "green" with "red" in the same quality
criterion are eligible for a joint meeting of medical
experts designated by all regional institutions to
resolve conflicting views (consensus-conference).
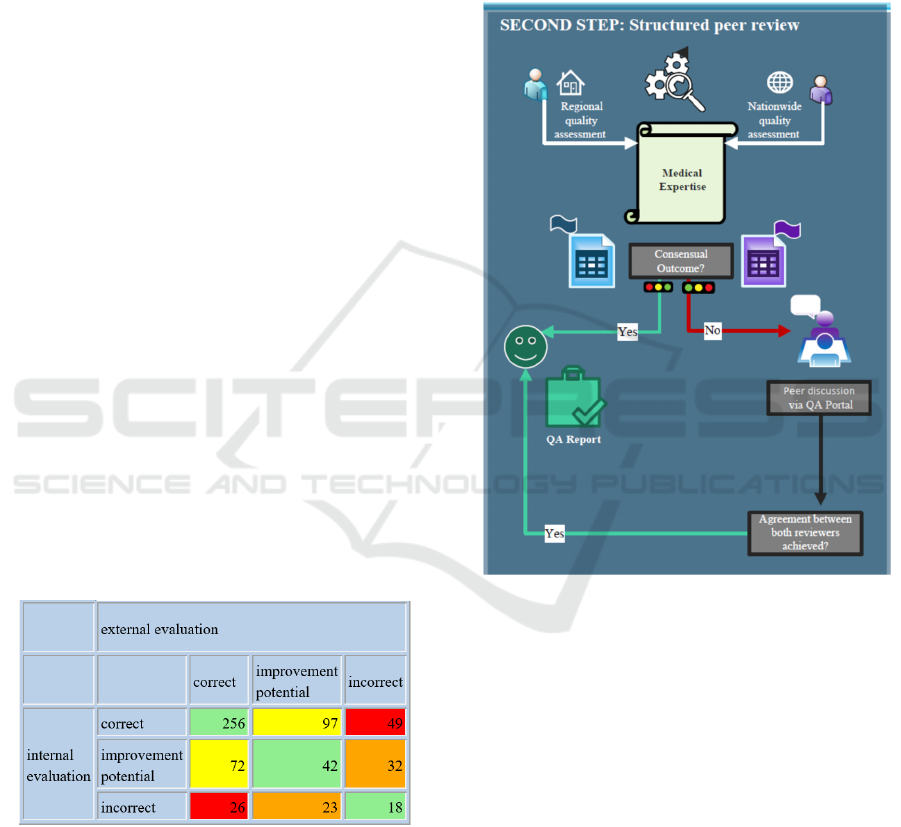
Table 1: Validating internal quality assessment outcomes
by comparing with the outcomes by mutual peer review for
the same expertise assessments. In the topic shown above,
49 + 26 = 75 reviews are eligible for consensus.
5.2 Structured Peer Review
Communication
We consider the random sample of medical expertise
assessments from each of the nine topics for a period
of six months in three steps:
1. internal review by the author's peer (1° peer)
2. external review by a second peer, belonging
to another regional institution (2° peer),
3. possible modification of the internal
evaluation by the first peer in regard to the
external evaluation, creating the synoptic
review outcome sheet.
Figure 2: Peers gathering assessments to be treated in the
consensus-conference by discussing conflicting reviews via
the QA-Server.
5.3 Resolving Conflicting Reviews
To facilitate joint decision making, they are randomly
distributed into four groups with four parti-cipants
each. To guarantee objective judgements, no
participant can be involved in discussing reports ge-
nerated by himself (only third-party peers admitted).
Usually, we discuss 16 or 32 expertise assess-
ments per conference day. In order to solve the alloca-
tion problem, we start with a random order, followed
by group assignment to the first possible position in a
cyclic order. If there are no valid assignments left, we
search from top to bottom for possible replacements.
Opting for a few more candidate expertise assess-
ments to choose from, will facilitate the exchange
process. Other options are to change the initial
HEALTHINF 2023 - 16th International Conference on Health Informatics
274
random order of the expertise assessments or the
random group assignment of the institutions.
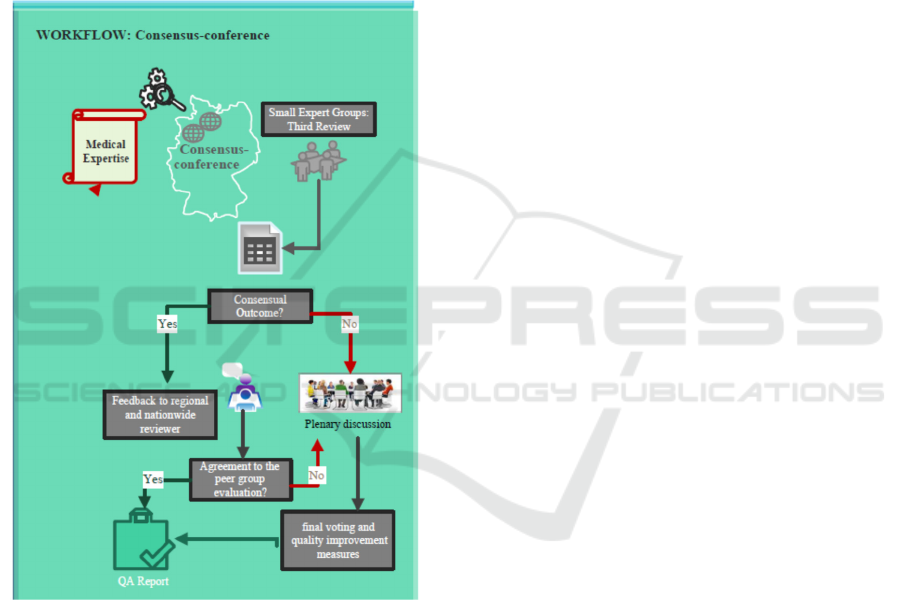
During the consensus conference, controversial
review sheets are processed by third party review. If
a common judgement within the third party peers
remains disputed, this expertise assessment will be
routed into the plenary discussion.
As soon as the third party groups have fixed their
group voting, persisting conflicting reviews are open
to discussion, leading to a final plenary voting in each
conflicting quality criterion, involving all 16 medical
experts. The final review results of the consensus-
conferences are stored as part of the public reporting.
Figure 3: IT implementation of the consensus process.
5.4 Logistic Framework
The red/green differences showed to be unevenly
distributed as well among the regional institutions as
across the quality criteria, so unveiling the prove-
nance of the reports and of the reviewer proved to be
of capital importance to maintain an objective, factual
and open exchange among the peers in order to revisit
critical process checkpoints in passing an expert
opinion, creating a common ground of agreement.
We usually started resolving the conflicting
reviews by establishing third party groups.
Alternatively, polarizing expertise reviews showing a
high load of red/green differences can be prepared for
individual live evaluation by every peer to discuss the
range of opinions openly during the consensus-
conference. To select the most polarizing reviews, we
performed a ranking by summing up the evaluation
differences between the internal and external review
(from green to red distance 2, otherwise 1). We advise
to check for the kind of assessment problem in order
to exclude reports addressing the same problem
repeatedly but in different criteria.
All previously described points are automatically
implemented via the QA-server, presenting to each
medical expert only those decisions he has to discuss
with his peers. If votes are necessary, they are carried
out live on the QA-server. Each peer sees the results
and the documented remarks in real time, which are
then transferred to the database to be available for
quality assessments reports.
6 PUBLIC REPORTING
The provident decision of the head physicians' board
in 2016 happened to gain the attention of the German
health politics. The Health Care Act in 2019 intro-
duced mandatory reports of the activities of the
regional Medical Advisory Service Institutions every
two years, including the nationwide quality assurance
plan's evaluation, starting in 2024.
We will now present preliminary statistical results
for some paramount quality dimensions we analysed
so far. The following figures show the outcomes
concerning the medical assessment topic "incapacity
for work" displaying the first nine months in 2021.
6.1 Quality Dimensions
The quality assurance results were investigated
within several dimensions:
Cumulative internal quality assurance results
benchmarked against cumulative external
quality assurance results, using both a visuali-
sation as a bar plot and a secondary diagram
showing confidence intervals for differing
results.
Comparing the mutual peer review results on a
descriptive level in a table, indicating reliable
differences found by confidence values initiat-
ing quality improvement measures.
Focussing on quality outcomes within the own
institution for all criteria applied on all med-
ical topics addresses systematic weak points as
comprehensible language avoiding needless
IT-Structures and Algorithms for Quality Assurance in the Medical Advisory Service Institutions in Germany. Step 2: To err is Human.
Consensus-Conferences
275
technical terms, deploying medical facts and
recommendations in a well-structured way.
6.2 IT-Server Assisted Access
For training purposes, the expertise assessments are
shown in the QA-Server sorted by bad scores,
selecting for the highest number of criteria marked as
incorrect. Clicking on a cell on table 1 takes you
directly to a synoptic view of the internal and the
external reviews, provided both online and as file
export. A link to the original expertise assessment is
embedded in the synoptic review sheet, so all peers
can check for appropriate rating in every criterion.
All institutions can export the charts with the
individual results highlighted on a daily accurate
basis as a freely configurable graphic from the QA-
server, selected for quality criterion and for medical
assessment topic.
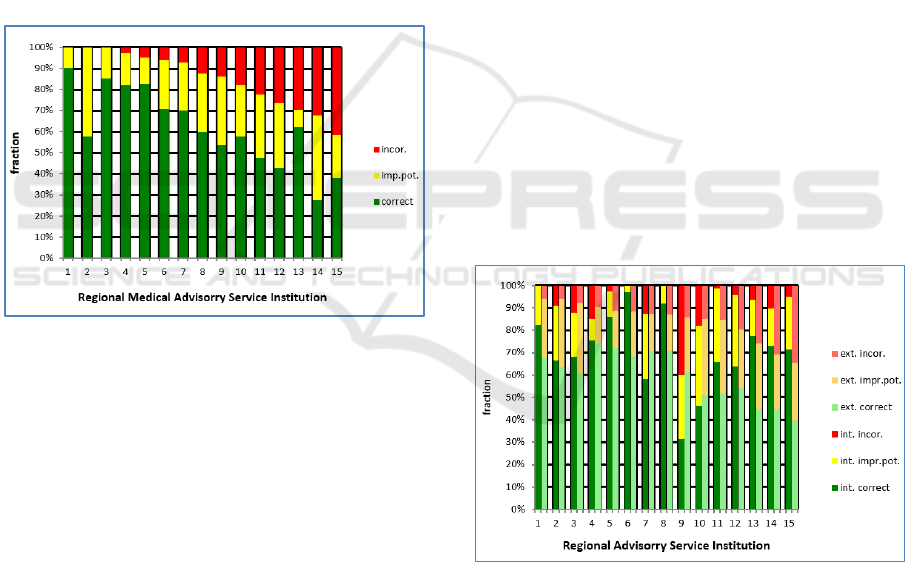
Figure 4: Individual quality assurance results of all regional
Institutions in one criterion for topic "incapacity for work".
6.3 Preliminary Quality Assurance
Results for Internal Peer Review
The benchmark of the cumulative internal results
shows varying results between the regional
institutions (MD), "MD 1" stating no incorrect
assessments and "MD 15" stating more than 40
percent of incorrect expertise assessments. The
criterion checks if all the medical information was
available. The divergent evaluation results judging
the same assessments highlights the need to reach a
uniform understanding of the quality standards,
initiated by the consensus conference discussions.
Each peer can see the position of his own
institution in the benchmark telling him whether he
acts particularly strictly or tolerantly (and possibly
inaccurate) as compared to the peers of the other
regional institutions. The other MD are concealed, the
number ID changing from chart to chart since the
position is sorted by growing amount of red ratings.
6.4 Benchmarking the Individual
Quality Assessment Results:
Outcome Validation by Mutual
Peer Review
Validation of individual internal quality assurance by
external review by a second peer focusses mainly on
the quality of the expertise assessments. The external
review is a representative mix of all other MDs over
a sufficiently long period of time. The left part of the
column graphic below always shows the internal
assessment and the right part the external review. In
"MD 9" the external evaluation is much more critical
than the internal. For "MD 15" the situation is
reversed.
Evaluation differences in a criterion spring to the
eye instantly, making analyses easy for the peers.
Additionally, confidence intervals are displayed:
In case the intervals are disjoint, there is a
statistically significant difference calling for action,
either inside the institution or even on a nationwide
level.
A critical reappraisal of the quality criteria
concerned will be proposed as subject for the
consensus conference discussion to discuss the need
for nationwide improvement measures.
Figure 5: Validation of quality assurance results by direct
comparison of the individual quality assurance vs. the
external mutual peer reviews for the same expertise
assessments (author peer vs. external second peer).
The confidence intervals of the external assessment in
Figure 6 are disjunct even in a horizontal perspective
for "MD 1" and "MD 15", additionally indicating a
significant difference in the quality of medical
expertise assessments between "MD 1" as compared
HEALTHINF 2023 - 16th International Conference on Health Informatics
276

to "MD 13", "MD 14" and MD15", an intriguing find-
ing of regional disparity.
Figure 6: Checking the variations found in a quality
criterion for statistically significant differences render
possible quality improvement measures.
6.5 Scope of Individual Improvement
It is of paramount importance for each regional
institution to gain this innovative perspective in order
to realise new improvement potential.
Quality assurance results vary a lot between the
criteria and are an ample monitoring tool to focus on
potentials for improvement in several topics, profiling
a general improvement measure like special trainings
for the medical experts authoring the assessments.
Figure 7: Specific charts for each individual regional
institution display all quality criteria within a medical
expertise assessment topic.
6.6 Future Prospects
The results of quality assurance will be published in
great detail in accordance with the recently adopted
statistics guideline. Thousands of real-time tables and
graphics are created by the QA-server processing
huge amount of data (Schuster, 2022).
Our next quality assurance tools to be developed are:
Time series including statistical significance
will monitor the effects of quality improve-
ment measures and possible confounders.
Monitoring the inter-rater-reliability within an
institution helps to identify internal evaluation
bias, benchmarking the nine medical
assessment topics against each other.
Analysing quality assurance outcome data
within a medical topic in regard to the nation-
wide inter-rater-reliability will enable us to
assess the process for differences in review
behaviour between the institutions involved as
a possible confounder.
7 CONCLUSIONS
The German health care insurance funds rely on
institutionalised medical experts to allocate the
appropriate health care service. The nationwide
quality assurance plan will empower the Medical
Advisory Service institutions to consolidate quality
performance on a nationwide level, strengthening the
legal task as an unimpeachable healthcare advisor.
We hope that this powerful tool will ease the
improvement processes, fostering a mindful dialogue
within the 16 Medical Advisory Institutions involved.
Consensus-conferences are meant to be a very
satisfactory and efficient quality assurance tool to
ascertain high quality in the peer review process.
REFERENCES
Altenstetter
, C., Busse, R. (2005). Health Care Reform in
Germany: Patch Change Within Established Governan-
ce Structures. J. Health Politics Policy Law, 30(1-2):
121–42.
Beauchamp, T.L., Childress, J.F. (2001)
Principles of Bio-
medical Ethics.
Oxford University Press.
Buehn,
S.,
Mathes,
T.,
Prengel,
P. ,
Wegewitz,
U.,
Ostermann,
T., Robens, S., Pieper, D. (2017). The risk of bias in
systematic reviews (ROBIS) tool showed fair reliability
and good construct validity to assess the risk of bias in
systematic reviews. J. Clin. Epidemiol., pages 121–128.
Cortina, J. (1993). What Is Coefficient Alpha? An Exami-
nation of Theory and Applications. J. Appl. Psychol., 78
(1):98–104.
Deming, W. E. (1982). Out of the crisis. Cambridge:
Massachusetts Institute of Technology.
DRV
(2018).
Qualitaetssicherung
der
sozialmedizinis
chen
Begutachtung. Manual zum Peer Review-Verfahren.
Berlin: Deutsche Rentenversicherung
Bund.
Eisinga, R., Grotenhuis, M., Pelzer, B. (2012). The relia-
bility of a two-item scale: Pearson, Cronbach or Spear-
man-Brown? Int J Public health, 58 (4): 637–642.
Gaertner, T., Gnatzy, W. (2011) Zum Sachverstaendigen-
status im Medizinischen Dienst der
Krankenversiche-
rung am Beispiel MDK Hessen. GuP 2011(5): 166-173.
IT-Structures and Algorithms for Quality Assurance in the Medical Advisory Service Institutions in Germany. Step 2: To err is Human.
Consensus-Conferences
277

Gerlach,
F.
M.
(2001).
Qualitaetsfoerderung
in
Praxis
und
Klinik:
eine
Chance
fuer
die
Medizin.
Stuttgart:
Thieme.
Gostomzyk, J. G., Hollederer, A. (2022) Angewandte So-
zialmedizin. Ecomed Medizin.
Institute of Medicine (2001). Crossing the Quality Chasm:
A New Health System for the 21st Century. Washington,
DC, National Academy Press.
Institute of Medicine (1990). Medicare: A Strategy for
Quality Assurance. Volume II: Sources and Methods,
Washington, DC, National Academy Press.
Internationale
Organisation
fuer
Normung
(2015).
DIN EN
ISO
9001:2015-11.
Qualitaetsmanagementsysteme.
An-
forderungen. Beuth Verlag.
Kamiske, G. F. and Brauer, J.-P. (2011). Qualitaetsmanage-
ment
von
A
bis
Z
.
Carl Hanser Verlag.
Kreuzer, C., Thiele, K.-P., Ries V. (2022) Krankenhaus-
Abrechnungspruefungen und Qualitaetskontrollen. in:
Hartweg, H. R., Knieps, F, Agor, K (Eds.) Kranken-
kassen- und Pflegekassenmanagement. Springer Gab-
ler. Wiesbaden.
Machnik, W. (2009). 20 Jahre MDK Nordrhein. Ju
bilae-
umsschrift
.
MDK
Nordrhein.
Masaaki, I. (1986). Kaizen: The Key To Japan’s Competiti-
ve Success. McGraw-Hill Education.
Merkel, A., Spahn, J (2019) Gesetz fuer bessere und unab-
haengige Pruefungen (MDK-Reformgesetz) vom
14.12.2019. BGBl. I 2019 (51):2789-2816.
Newman, M. (2006). Finding community structure in net-
works using the eigenvectors of matrices. Physical
Review E, 74.
Normand, S.-L., Mcneil, B., Peterson, L., Palmer, R.
(1998). Eliciting expert opinion using the Delphi tech-
nique: identifying performance indicators for cardio-
vascular disease. IJQHC, 10:247-260.
Nuechtern,
E.
(2008).
Das
professionelle
Gutachten.
Beson-
derheiten in der gesetzlichen Krankenversicherung.
MedSach, 105 (3):96–98.
Nuechtern, E., von Mittelstaedt, G. (2015) Sozialmedizin:
Unabhaengig und fair in der Beurteilung. Dtsch Arztebl
112 (1-2): A-24 / B-20 / C-20.
Polak, U. W. (2018). Evaluation von Durchgangsarztbe-
richten mithilfe eines Peer-Review-Verfahrens. Trau-
ma Berufskrankh, 20 (Suppl. 4):237–240.
Ries, V., Thiele, K., Schuster, M. und Schuster, R. (2021)
IT-structures and Algorithms for Quality Assurance in
the Health Insurance Medical Advisory Service Institu-
tions in Germany. In: Biomedical Engineering Systems
and Technologies, pages 353-360. Springer Nature.
Ries V., Thiele, K.-P., Garbrock, K., Hassa, R. (2022)
Medizinische Dienste und Medizinischer Dienst Bund
in der Krankenversicherung. In: Hartweg, H. R.,
Knieps, F, Agor, K (Eds.) Krankenkassen- und Pflege-
kassenmanagement. Springer Gabler, Wiesbaden.
Schuster, R. (2022) Strukturelle Beratung der Kranken-
kassen durch den Medizinischen Dienst in der Pharma-
kotherapie. Die Verwendung epidemiologischer und
gesundheitsoekonomischer Analysen im Zeitalter von
Digitalisierung und Big Data. In: Hartweg, H. R.,
Knieps, F, Agor, K (Eds.) Krankenkassen- und Pflege-
kassenmanagement. Springer Gabler, Wiesbaden.
Sawicki, P., Bastian, H. (2008). German Health Care: A
Bit
of Bismarck Plus More Science. BMJ, 337:a1997.
Schmacke, N. (2016). Zur Positionierung des MDK in der
gesetzlichen Kranken- und Pflegeversicherung, Gutach-
ten im Auftrag des AOK-BV. In:
Bolte,
G.,
Goe
rres,
S.
Gerhardus,
A. (Eds.) IPP-Schriften
,
Uni
Bremen.
Shewhart, W. A. (1931). Statistical Method from the view-
point of quality control. (Reprint in1986 of a publication
of the
Department
of
Agricultuire
Mil
waukee 1931).
New York: Dover Publication.
Shinano, Y., Fujie, T., Kounoike, Y. (2003). Effectiveness of
Parallelizing the ILOG-CPLEX Mixed Integer Optimi-
zer in the PUBB2 Frame-work. In Euro-Par 2003 Paral-
lel Processing; 451-460. Springer Berlin Heidelberg.
Strahl, A., Gerlich, C., Alpers, G., Ehrmann, K., Gehrke,
J.,
Mue
ller-Garnn,
A.,
Vogel,
H.
(2018).
Devel
opment and
evaluation of a standardized peer-training in the context
of peer review for quality assurance in work capacity
evaluation. BMC Medical Education, 18:135–145.
Strahl,
A.,
Gerlich,
C.,
Wolf,
H.-D.,
Gehrke,
J.,
Mue
ller-
Garnn,
A.,
Vogel,
H.
(2016).
Qualitaetssicherung
in der
Sozialmedizinischen Begutachtung durch Peer Review.
Pilotprojekt der DRV. Gesundheitswesen, 78:156–160.
Thiele, K.-P., Kreuzer, C., Mengel, R. (2018).
MDK-Prue-
fung: Fluch
oder
Segen?
In: Janssen, D., Augurz-ky, B.;
Krankenhauslandschaft in Deutschland: 89–94. Stutt-
gart: Kohlhammer.
Varkey B. (2021) Principles of Clinical Ethics and Their
Application to Practice. Med Princ Pract 2021, 30(1):
17-28.
Wirtz, M. and Caspar, F. (2002).
Beurteileru¨bereinstimmung
und
Beurteilerreliabilitaet:
Methoden
zur
Bestimmung
und
Verbesserung der
Zuverlaessigkeit
von
Einschae-
tzungen
mittels Kategoriensystemen
und
Ratingskalen
.
Goe
ttingen:
Hogrefe.
Woodward, S. (2019). Sign up for safety campaign. In: NHS
resolution. Being fair. resolution.nhs.uk.
HEALTHINF 2023 - 16th International Conference on Health Informatics
278
