
Digitalization of Healthcare Processes Through BPMN for Clinical
Risk Monitoring and Management
Vincenzo Cartelli
1
, Leonardo Longo
2
, Orazio Tomarchio
2a
and Natalia Trapani
2b
1
Allincloud s.r.l, Catania, Italy
2
Department of Electrical Electronic and Computer Engineering, University of Catania, Italy
Keywords: Digitalization, Healthcare, Business, Process, Management, Risk, BPMN.
Abstract: Several recent studies have provided alarming data regarding the occurrence of errors in healthcare in all
OECD (Organization for Economic Co-operation and Development) countries, including, to a significant
extent, also Italy. Many of these errors seem to be largely due to failure to comply with company operating
procedures, which are typically based on ministerial directives and international standards. In this context, the
paper describes the work carried out in an Italian research project where a more structured approach to the
healthcare sector has been proposed, focusing on clinical risk management. Clinical processes have been
modelled by using BPMN (Business Process Modelling and Notation) standard notation and then interfaced
with the hospital information system to monitor and manage clinical risks. Digitalization of operating
procedures also allowed the definition and computation of several KPIs (Key Performance Indicators) for
long-term monitoring. The work carried out in the experimental phase of the project, through the developed
system, highlighted the areas most affected by operational non-conformities, to address actions aimed at
safeguarding the patient's health and, indirectly, providing considerable economic savings.
1 INTRODUCTION
The rapid technological progress of recent years,
accompanied by the growing use of information
systems suitable for supporting their implementation
in complex business and organizational contexts, has
favoured the adoption of increasingly structured, safe,
and standardized approaches for modern production
processes, making them also more efficient and
monitorable. Latest trends in business automation and
digitalization, and the transformation of production
contexts enabled by Industry 4.0, have also
accelerated the adaptation process to new
organizational requirements to cope with the global
market, which requires products of ever-increasing
quality, in a short timeframe and suited to the needs
of the customer. In such a context any non-conformity
translates into an enormous cost, both from an
economic and image point of view. This need was not
confined to the industrial production sector, but also
has extended to the services market and operations,
thanks above all to the ever-increasing diffusion of
a
https://orcid.org/0000-0003-4653-0480
b
https://orcid.org/0000-0001-6221-5355
the IoT and cloud computing, which make it possible
to overcome the old infrastructural barriers that
represented an obstacle to the high level of
customization, scalability and resilience required by
the clients.
The concept of Smart Hospital also fits into this
promising context, thanks to the advent of modern
technologies and IT infrastructures, a different
approach in healthcare, guaranteeing more accurate
results, the reduction of errors, as well as greater
efficiency, speed, and agility of all medical
procedures, necessary above all for clinical risk
management. This also indirectly translates into a
reduction of costs related to compensation for damage
caused to patients who are victims of medical errors
or medical malpractice, resulting in a higher quality
of produced output, and therefore in greater patient
trust.
This work was carried out within the Italian
project “Mo.Ri.San Monitoring and management of
clinical risk in the social and health care sector”,
whose main objective was to provide useful tools for
Cartelli, V., Longo, L., Tomarchio, O. and Trapani, N.
Digitalization of Healthcare Processes Through BPMN for Clinical Risk Monitoring and Management.
DOI: 10.5220/0011850300003476
In Proceedings of the 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health (ICT4AWE 2023), pages 151-158
ISBN: 978-989-758-645-3; ISSN: 2184-4984
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
151

the reduction of clinical risk and risk management,
using Information Technology and process
management as enablers to guarantee patient safety
and, indirectly, economic savings in the long term.
To reach these objectives a structured approach to
a healthcare context was applied, which is strongly
characterized by operations and human interactions,
really difficult to control and standardize by their
nature, with the aim of monitoring operational non-
conformities within their processes.
Within the project, the basic approach was to
adopt the Business Process Management
methodology to build executable models of the care
pathways provided within some healthcare facilities.
More specifically the standard notation BPMN 2.0
was used to model structured and repeatable
processes (OMG (2013)).
The results and the evaluations carried out in our
study will be used by the private clinics partners of
the project, concerned with implementing operations’
restrictions or constraints within the software used,
thus guaranteeing the adherence of the work of
physicians and nurses to the medical and
organizational operating procedures, according to the
current legislative framework and the standards of
reference.
The rest of the paper is organized as follows.
Related work is reported in Section 2. In Section 3 the
process modelling phase is described together with
some details on a specific process. Then Section 4
reports the risk analysis performed, while system
integration with the existing hospital information
system is described in Section 5. Section 6 describes
the experimental phase and discusses about the
obtained results. Finally, we conclude the work in
Section 7.
2 RELATED WORK
Clinical risk management, which is a requirement of
current legislation in the healthcare sector, represents
an important factor in modern healthcare systems.
According to research conducted by Kohn et al.
(2000), of the IOM - Institute of Medicine, clinical
risk can be defined as the "probability that a patient
is victim of an adverse event, that is, suffers any
damage or discomfort attributable, even if
involuntarily, to treatment provided during the period
of hospitalization, a worsening of health conditions
or fatality"; its inadequate management represents
one of the main causes of legal actions against health
structures in OECD countries, as well as, according
to the Institute for Healthcare Improvement, has
become the third leading cause of death in the United
States.
The ever greater technological, regulatory, and
organizational changes in the healthcare sector have
therefore required the adoption of increasingly in-
depth analysis, aimed at identifying the causes of
adverse events, and intervening even before they can
occur. In this regard, Cagliano et al. (2011)
demonstrated the advantages deriving from the
application of a structured and systemic approach in
identifying risks for the patient, by the Reason theory,
within health contexts characterized, by their nature,
by a strong variability linked to human decision-
making processes.
Wingate (2003) highlighted the possible impact
of computerized systems within healthcare and
pharmaceutical companies, to support daily
operations, evaluating regulatory compliance through
IT validation systems.
In Crotti Junior et al. (2020) an Access Risk
Knowledge (ARK) platform has been presented and
used in clinical risk management. The ARK platform
uses Semantic Web technologies to model, integrate,
and classify risk and socio-technical system analysis
information from both qualitative and quantitative
data sources into a unified risk graph. A clinical
safety management taxonomy to annotate qualitative
risk data has been developed, in order to support
automated analysis.
Furthermore, several recent studies have
proposed the implementation of Business Process
Management in the healthcare sector. Among these,
Emanuele and Koetter (2007) analyzed a case study
of integration between BPM (Business Process
Management) and corporate information systems
within a healthcare facility, highlighting the
advantages related to the support it can give to
processes.
A further study by Reichert (2011) analyzed the
possibility of adopting PAIS (Process Aware
Information Systems), which have healthcare
business processes implemented within them,
highlighting the need of flexibly to adapt them to the
variability that characterizes the healthcare pathways,
through all the decision-making processes of which
they are composed.
Gomes et al. (2018) proposed a case of integration
between models of healthcare processes, created
using the BPMN 2.0 standard, and the electronic
medical record.
However, it should be highlighted that, since
modern health systems are highly interconnected and
dependent on the large amount of data they generate,
patient safety relies not only on the adoption of the
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
152

best medical practices and on the healthcare
pathways, which are as standardized as possible and
established by current and regional regulations but
also from the correct treatment of personal data,
which can guarantee privacy both during
hospitalization phases and in subsequent periods.
In this regard, in recent years new frameworks
mainly focused on ensuring patient cybersecurity
have emerged, such as, for example, the CUREX
conceptual model (Kougka et al., 2021), which offers
a platform-independent integrated environment to
execute cybersecurity and risk assessments, to verify
the security and robustness of information systems
containing sensitive data, as well as providing a
useful tool for the correct exchange of patients’
information between different healthcare facilities,
through the adoption of technologies such as the
blockchain and IoT (Internet of Things) devices.
Although the safety and privacy of patients have
been strongly considered in the context of the
proposed study, through the anonymization of the
data provided and processed by the developed model,
it is mainly focused on the analysis and monitoring of
the critical issues related to the adoption of incorrect
medical practices, which could lead to serious
physical harms to patients.
From the preliminary research executed, therefore
emerges the lack of a real-time monitoring system of
the risks that may occur during healthcare pathways
within health facilities, based on a structured and
standardized approach, as proposed by the OMG
Healthcare Domain Taskforce (2020), which is the
scope of the study.
As anticipated, the modern context, strongly
influenced by digital transformation, together with
the greater awareness and attention of the institutions
towards the clinical risk, have provided the main
input and the possibility of developing the project,
thanks to the tools they make available, as well as the
cultural changes taking place.
3 PROCESS MODELLING
Through the process models, the study aimed to
create a digital representation of the healthcare
procedures, which could be performed in
background, through the recordings reported on
Healthcare ERP software, with which they exchange
data and information, allow to instantiate a new
process, complete a certain task, or exchange
messages necessary for their execution.
Through this approach, it was possible to trace
daily operations performance, evaluating the
operational differences, also with respect to the
procedures established by the companies, by a status
code returned by the system.
To model the processes the Signavio platform was
used. This tool allows you to create business process
models using the BPMN 2.0 standard and allows
different users to collaborate on the same process
modeling in real time. By using this platform, it was
possible to highlight all the decision-making
processes, the involved actors, the documents, and
information exchanged within the identified
processes.
The built models can be traced back to Petri nets,
in which a transition of the state associated with the
system occurs upon predetermined conditions.
For the preliminary study phase, the operating
procedures in use at the clinics involved were used,
thanks to which it was possible to identify three main
processes for the subsequent modeling and analysis
phases:
- Laboratory analysis processes;
- Surgical room processes;
- Drug management and administration processes.
After the preliminary study phase and the
collection of essential information and operating
procedures by the healthcare facilities, a first version
of the process models was created as closely as
possible to the operations carried out by healthcare
personnel within the companies.
For the surgical room processes, the following
sub-processes were identified and built:
− Hospitalization phase, execution of the pre-
operative medical examinations and planning of
the surgical intervention.
− Pre-surgical phase, concerning the preparation of
the patient and his transport and access to the
surgical block, verification of the completeness
of the documentation supplied with the patient.
− Surgical phase, including the records relating to
the surgical and anaesthetic medical practices
adopted.
− Post-surgical phase, concerning the recordings
made on Healthcare ERP software concerning
the monitoring of the patient's vital parameters in
the phase immediately following the surgical
operation.
The modelling of laboratory analysis processes
involved the following sub-processes:
− Pre-analytical phase, which begins with the
request for laboratory analysis by the physician,
continuing with the preparation of the patient and
the collection of the sample by the nursing staff,
Digitalization of Healthcare Processes Through BPMN for Clinical Risk Monitoring and Management
153

and with the subsequent sorting of the samples,
identified and labelled, to the analysis laboratory.
− Analytical phase, in which the actual analysis of
the samples provided by the department takes
place, according to different paths for the
examinations that can be performed with
instrumentation interfaced with healthcare ERP
software and those that can be performed
manually or with non-interfaced instrumentation.
− Post-analytical phase, which concerns the
communication of the results to the department
and their reporting.
The models of drug management and administration
processes have been divided into the following sub-
processes:
− Phase of medical examination, during which the
patient's condition is re-evaluated, then the
therapy is prescribed or updated. In the case of
first access, pharmacological recognition is also
carried out, as well as the patient's anamnesis, to
identify the therapies already in act, allergies,
and pathologies of the patient that must be taken
into consideration for subsequent prescriptions
and administrations.
− Phase of preparation and administration of the
drug, in which the nursing staff proceeds to the
correct identification of the patient, preparation
of the drug, and subsequent administration.
− Monitoring phase, in which any abnormalities or
adverse reactions in patients due to
administration are recorded.
− Pharmacological reconciliation, at the time of
discharge, in which the medical staff delivers the
SUT (Single Therapy Card) to the patient,
providing him/her with the necessary
information regarding the therapy to be followed
after discharge.
The adherence of these models (as-is configuration)
to the standards identified in the preliminary study
phase and to the current legislation was considered, to
evaluate a possible redesign and a to-be
configuration.
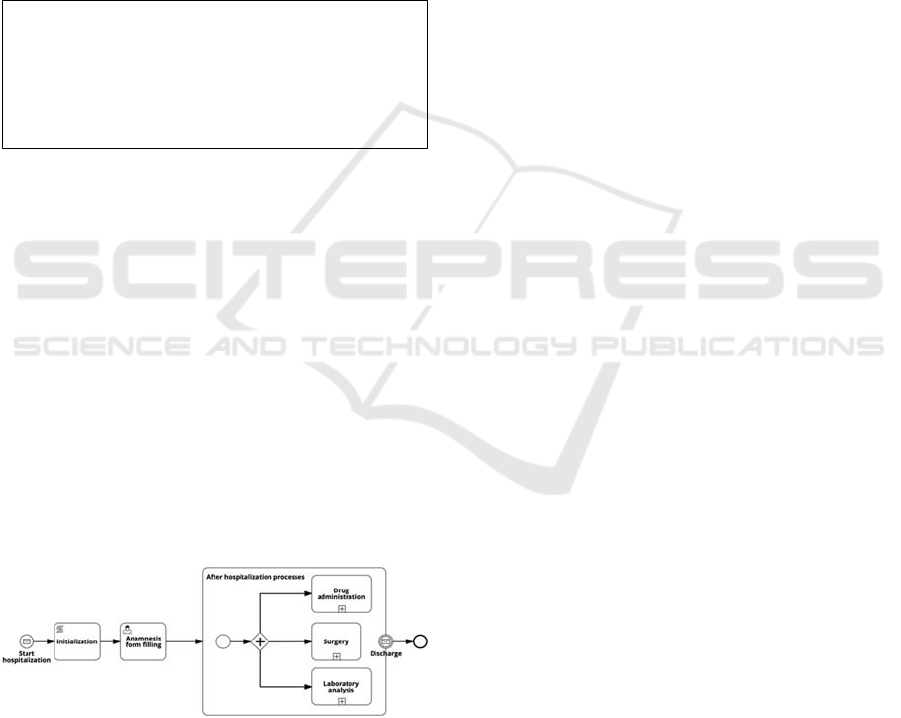
As an example, the workflow concerning the
patient's hospitalization booking sub-process is
shown in Figure 1. In it, many of the elements that the
BPMN 2.0 standard makes available for modelling
have been used.
Figure 1: A simple process model representing the patient
hospitalization booking.
The elements of the workflow represented
through circles represent start events, intermediate
events or end events, while the tasks, i.e. the
elementary operations which compose the model, are
represented through rectangles.
As shown in Listing 1, the initial start event,
which represents the receipt of a new booking, is
started as soon as the management software, through
the prepared REST (Representational State Transfer)
web-service, sends the JSON (Javascript Object
Notation), containing all the booking information, to
the appropriate endpoint.
Listing 1: JSON for the new-booking request.
The system, in turn, sends a response to the
management software, shown in Listing 2.
Listing 2: JSON for the new-booking response.
The JSON is addressed by the management
software on an endpoint of type / message / start,
which allows, upon receipt, to start a new instance of
the process.
The next manual task is automatically performed
by the process engine upon receiving the JSON
shown.
The next task, created by a script task, contains a
Groovy script which is executed by the process
engine when the task itself is instantiated. Through
this script, the execution variables of the “Sanitary
acceptance” process are set with the value received
through the JSON, while the “initiator”, i.e. the user
who started the process instance, is assigned to the
“evaluator” variable.
The next gateway, of the XOR type, allows the
flow to continue along only one of the outgoing
branches. If the condition
${SanitaryAcceptance ==
"hospitalization"}
is verified, meaning that the
patient's hospitalization has been arranged, then the
{
"key": "new-booking",
"businessKey": "<booking ID>",
"payload": {
"initiator": "<user ID>"
}
}
{
"key": "new-booking",
"businessKey": "<booking ID>",
"correlation": object,
"payload": {
"started": [ {
"processId": string,
"businessKey": "<booking ID>",
"initiator": "<user ID>"
} ]
},
"errors": [string]
}
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
154
flow will continue towards the subsequent tasks,
while it will be directed to an end event otherwise.
The flow will therefore await the receipt of the
JSON corresponding to the subsequent user
registration on the management software, containing
the "key" field: "assignment-id-shelter", and a
structure like the JSON previously illustrated. In each
of the JSONs, there is the “businessKey” field,
having the reservation ID as a unique value, through
which it is possible to correlate all subsequent
requests to the correct process instance.
The next script task, containing the Groovy script
shown in Listing 3, is started and executed
immediately upon receipt of the hospitalization ID
assignment message.
Listing 3: Example of a script task.
Through the previous script, key, businessKey and
payload variables are defined, within which the
values of the previously illustrated process variables
are entered, such as HospitalizationId and initiator.
Through the method
messageService.createMessage(), to which the
previously defined variables are passed as
parameters, a message is created addressed to the
subprocess shown below, allowing to start a new
instance.
The message sent by the previous script task
allows to start the start event of the hospitalization
sub-process (shown in Figure 2), followed by a script
task, with which the variable containing the
information of the initiator of the process is set.
Figure 2 Start hospitalization subprocess.
The next human task is performed upon receipt,
by the management software, of the respective JSON,
in which the "key" field: "compilation-file-
anamnesis" allows you to refer it to the correct task,
while the "businessKey" field allows you to correlate
it the process instance of the patient for which
registration on the software is being carried out. In
this case, a / task / complete web-service REST was
used to interface the two systems.
Downstream of the human task, the period of stay
of the patient inside the structure was modelled
through the use of a subprocess, through an AND
gateway, which allows the process instance to
continue on the three outgoing branches, for each of
which a collapsed subprocess has been inserted,
which refers to the relative models created for the
processes of drug administration, surgery, and
laboratory analysis.
The boundary event of receipt of the
communication message is instantiated upon
registration on the management software of the
patient's discharge from the facility, entered by the
physician or nurse, which corresponds to the sending
of a JSON containing the "key":"Discharge", and
with a structure like those previously illustrated.
Upon receipt of the discharge message, the relative
process instance is closed.
4 RISK ANALYSIS
After the modeling phase, a risk analysis was
conducted with the H-FMEA methodology
(Healthcare Failure Mode and Effect Analysis),
reaching for each of them the identification of the
risks and the calculation of the relative RPN (Risk
Priority Number), the identification of possible
consequential damages and the adopted prevention
measures. To determine the RPN, the following
parameters were used:
− S = Severity of the injury or damage that the
patient may suffer.
− L = Likelihood or probability that the event
happens.
− D = Detection, the ease and difficulty of
detecting the error before it causes damage.
The calculated RPN made it possible to
hypothesize an order of priority of intervention for the
various risk factors, as well as to build statistics on
the phases most affected by errors within the same
process, also allowing the identification of causes and
containment factors.
Based on the results of the H-FMEA analysis and
the Ministerial evidence, a set of indicators was built
referring to the processes that were modelled in the
previous phases and suitably integrated with other
indicators already in use in nursing homes.
def key = "sanitary acceptance";
def businessKey =
HospitalizationIdAssignment.get("HospitalizationId");
def payload = commonService.payloadBuilder().put
("initiator",execution.getVariable("evaluator")).build
();
def message = messageService.createMessage(key,
businessKey, null, payload);
messageService.start(message);
Digitalization of Healthcare Processes Through BPMN for Clinical Risk Monitoring and Management
155

This set has the purpose of monitoring the
progress of the processes, the correct execution of the
various phases, and avoiding errors related to the
deviation from the company procedures established
for the execution of the same. To do this, the
indicators have been designed to be measured over
different time horizons.
A subset of them, once implemented in respective
digital dashboards, will provide constantly updated
information, to promptly identify any anomalies with
respect to what is established by the work plans or by
the evaluation criteria, thus representing a tool
capable of reducing the incidence or severity of the
risk factors found within the processes in the previous
stages.
The remaining part of the indicators has been
designed to constitute medium to long-term
monitoring, measuring and certifying the effective
reduction of clinical risk resulting from the
implementation of the project itself, which can be
found in the reduction of significant events.
This set of indicators was used to create a new
software module, made available to clinics, which
allows you to extract its value based on the data
contained in the respective databases, then evaluate
its temporal trend, as well as any abnormal variation.
5 SYSTEM INTEGRATION
To interface the models created within the project to
the management software in use at the facilities, as
anticipated, three different types of REST web-
services were used (as shown in
Figure
3):
• Message/start, when received by the engine
corresponds to the start of an instance of a
specific process.
• Message/send, through which data is
exchanged between the engine and
management software.
• Task/complete, the receipt of which by the
engine corresponds to the completion of a
specific instance of a thread.
Figure 3: System integration.
The exchange of information between the process
engine, which is responsible for executing the models
of the developed processes, and the Healthcare ERP
software the operators are interfaced with, allows to
complete of certain tasks (elementary actions)
belonging to the model created, therefore to be able
to continue their execution, monitoring their status in
real time, by triggering the specific task and instance
connected to the sent message, elaborated by the Web
Services (integrated layer) component of the Process
Engine.
The implementation and interfacing with the
process models have been designed in such a way as
to operate in the background, resulting in minimal
impact compared to the normal working conditions of
the medical and nursing staff, and carried out in such
a way as not to return alerts or error messages,
ensuring the normal functioning of the software used
by companies.
These implementations involved not only the
development, digitalization and execution of the
process models but also the revision of the software
code used by the structures, in such a way as to
provide for interfacing with the previously indicated
cloud process engine.
Through the execution in the process engine,
based on the messages exchanged with the ERP
software, it was possible to collect information about
the most critical processes with respect to the
operating procedures established by the management
of the structures involved, as well as to keep track of
the major process non-conformities, whenever a
different task than the one scheduled in the developed
models has been performed, which could represent a
risk for the patient during his stay in the clinics.
This execution information has been stored in a
process execution Database.
The objective of the subsequent test phase was to
ensure the correct functioning of the developed
system, both limited to the workflows implemented,
and as regards their interfacing with existing systems,
as well as ensuring their stability over time and
effective maintenance conditions of any overload of
data transferred and communications exchanged.
After having validated the correct functioning and
interfacing between the software and the developed
processes and after having tested the reliability and
stability of the updated system, the test environment
was replicated within the servers of the two clinics,
by updating the pre-existing software version within
them and the installation and configuration of a new
server exclusively dedicated to the BPMS (Business
Process Management Suite) system.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
156
6 EXPERIMENTAL PHASE AND
RESULTS
After training the personnel involved, the last project
phase concerned the final experimentation, which had
the aim of collecting data on the actual functionality
in the field of the new system interfaced with the
process engine, operationally evaluating the
adherence of the assistance activities provided within
the clinics with the operating procedures and with the
ministerial standards and directives, identifying any
bottlenecks or discrepancies in their execution, which
could represent a risk for the patient.
The experimental phase was then conducted on
the job for all the processes and sub-processes
identified, analyzed, and modelled in the previous
phases of the project, through the normal registration
operations on software by the medical and nursing
staff of the clinics.
Downstream of the experimental phase, it was
possible to extract the data stored in the appropriate
process execution database, which recorded, for each
process instance executed, a code relating to the state
of completion of the same, as well as any error codes,
which identify differences in execution with respect
to the models prepared.
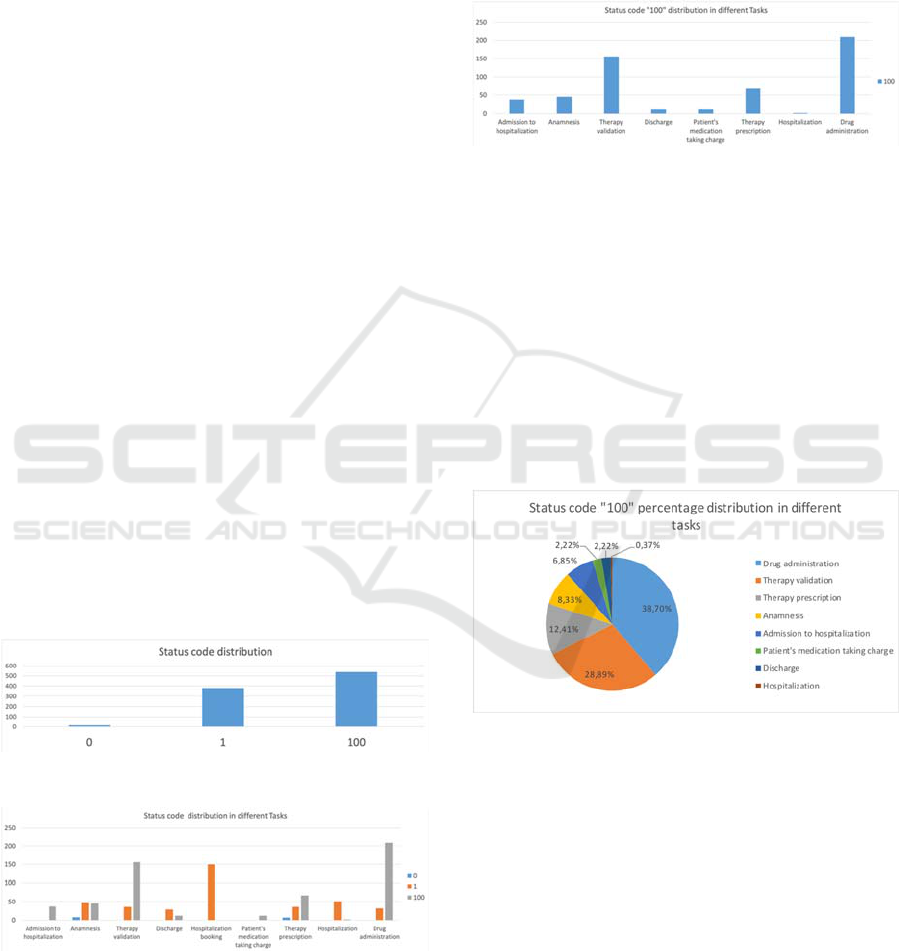
The distribution of the return codes for the
process instances have been collected in the
histogram shown in Figure 4, where code 0 represents
a communication error between software and the
BPMS server, code 1 represents the correct execution
of the single process instance, while code 100
represents discrepancies with respect to the operating
procedures established by the companies.
Figure 4: Status code distribution.
Figure 5: Status code distribution in different tasks.
This histogram was also replicated with reference
to the individual sub-processes of each of the three
main identified ones, of which, by way of example,
the data relating to the administration of drugs within
the departments are reported in Figure 5.
The histogram in Figure 6, on the other hand,
shows the distribution of status code 100, which
therefore represents an operational difference, with
respect to the different phases of the drug
administration process, taken as an example.
Figure 6: Distribution of status code 100.
This graph made it possible to focus attention on
the sub-processes most affected by procedural errors,
therefore potentially having the greatest impact on the
success of the care pathways and the safety of the
patient during the period of stay in the facility.
However, as shown in Figure 7, it is necessary to
consider the percentage distribution of the onset of
the status code 100 between the different phases, to
have a clearer idea about the possible containment
measures and the constraints that could be
implemented in the future within the management
software.
Figure 7: Status code “100” distribution in different tasks.
7 CONCLUSIONS
The use of a structured approach within a context
strongly characterized by human work, therefore also
by the decisions that the healthcare worker is called
to make, has allowed to highlight all the discrepancies
and anomalies that may emerge in the normal
carrying out the daily activities that characterize it.
BPM technology, and in this specific case the
BPMN 2.0 notation, proved to be a valid choice to
guarantee and monitor the compliance of processes
with current legislation and international standards.
Digitalization of Healthcare Processes Through BPMN for Clinical Risk Monitoring and Management
157

In particular, the integrated system developed
appeared to be able to monitor all deviations from the
operating procedures established at the company
level, and based in turn on ministerial standards and
recommendations, which may represent a risk factor
for the patient, which could result in serious damage
to the image and economic for the structure, as well
as physical damage for the patient. The tool to
calculate KPIs is also useful especially for medium
and long-term monitoring, to evaluate any
improvements following future implementation of
constraints and alerts within the management
software, which can instantly report the operational
differences to the operator, in the same registration
phase on the software in use.
Future development of the study could involve the
introduction of constraints within the software, based
on the structure of the process model in execution,
which prevents the operator from completing the
tasks for which the foreseen operations have not been
performed upstream, or that return error messages in
case of discrepancies with the operating procedures.
The modelling could also be extended to other
fields of operational procedures, not directly
reproducible digitally through the BPMN 2.0
standard, due to their unstructured nature, such as
complex decision-making operations or unstructured
procedures. The latter could be modelled using other
Business Process Management tools, such as the Case
Management Model and Notation (CMMN) for
unstructured processes, and Decision Model and
Notation (DMN) for decision-making processes.
Finally, once the effects of the proposed
implementations have been assessed, should they
prove useful for the objective of safeguarding the
safety of the patient and the work of the healthcare
personnel, it could be useful to extend this approach
to all other healthcare processes that have not been
subject of the present study. This would also make it
possible to classify the latter based on their need for a
more or less structured approach, adapting the models
and systems developed to the cases analysed from
time to time.
Furthermore, this approach would follow the
latest trends and propensities of Industry 4.0, oriented
towards the introduction of automated processes and
innovative technologies, to improve working
conditions in terms of productivity and safety.
ACKNOWLEDGEMENTS
This work has been partially financially supported by
the funding programme PO FESR Sicilia 2014/2020,
research project Mo.Ri.San.: Monitoring and
management of clinical risk in the social and health
care sector.
REFERENCES
Joint Commission International. (2007) – “Guidelines for
the implementation of the STANDARDS for the
Management of Clinical Risk in the health structures of
the Sicilian Region Standards for" HOSPITALS”.
Kohn LT, Corrigan JM, Donaldson MS (Institute of
Medicine) (2000). "To err is human: building a safer
health system". Washington, DC: National Academy
Press.
Cagliano AC, Grimaldi S, Rafele C (2011) A systemic
methodology for risk management in healthcare sector.
Safety Sci 49 (5): 695–708.
Wingate G, (2003). Computer Systems Validation: Quality
Assurance, Risk Management, and Regulatory
Compliance for Pharmaceutical and Healthcare
Companies (1st ed.). CRC Press.
Emanuele J, Koetter LE. (2007) "Workflow opportunities
and challenges in healthcare". BPM & Workflow
Handbook 1: 157.
Reichert M. (2011) What BPM Technology Can Do for
Healthcare Process Support. In: Peleg M., Lavrač N.,
Combi C. (eds) Artificial Intelligence in Medicine.
AIME 2011. Lecture Notes in Computer Science, vol
6747. Springer, Berlin, Heidelberg. https://doi.org/
10.1007/978-3-642-22218-4_2
João Gomes, Filipe Portela, Manuel Filipe Santos, (2018).
“Introduction to BPM approach in Healthcare and
Case Study of End User Interaction with EHR
Interface” Procedia Computer Science, 141: 519-524.
Kougka, Georgia, Gounaris A, Papadopoulos A, Vakali A,
Navarro Llobet D, Dumortier J, Veroni E, Xenakis C,
and Gonzalez-Granadillo G. "A Conceptual Model for
Assessing Security and Privacy Risks in Healthcare
Information Infrastructures: The CUREX
Approach.". Knowledge Modelling and Big Data
Analytics in Healthcare: Advances and Applications:
(2021) 285-297.
Nifakos, Sokratis, Chandramouli K, Nikolaou CK,
Papachristou P, Koch S, Panaousis E, and Bonacina S.
"Influence of human factors on cyber security within
healthcare organisations: A systematic review."
Sensors 21, no. 15 (2021): 5119.
Crotti Junior A, Basereh M., Abgaz Y, Liang J, Duda N,
McDonald N. and Brennan R (2020) The ARK
platform: enabling risk management through semantic
web technologies. In: 11th International Conference on
Biomedical Ontologies (ICBO 2020), 17 Sept 2020,
Bolzano, Italy (Online).
OMG Healthcare Domain Taskforce (2020). “Field Guide
to Shareable Clinical Pathways. BPM + in
Healthcare”, Version 2.0
Object Management Group (2013): “Business Process
Model and Notation (BPMN)”, version 2.0.2.
ICT4AWE 2023 - 9th International Conference on Information and Communication Technologies for Ageing Well and e-Health
158
