
Spatial Patterns in Neurodegenerative Disease’s Hospitalizations in
Portugal (2000-2016)
Mariana Oliveira
1,2 a
, Alberto Freitas
1,2 b
, Ana Cláudia Teodoro
3,4 c
and Hernâni Gonçalves
1,2 d
1
Center for Health Technology and Services Research (CINTESIS@RISE), Faculty of Medicine, University of Porto,
Rua Doutor Plácido da Costa, s/n 4200-450 Porto, Portugal
2
Department of Community Medicine, Information and Health Decision Sciences (MEDCIDS), Faculty of Medicine,
University of Porto, Rua Doutor Plácido da Costa s/n, 4200-450 Porto, Portugal
3
Department of Geosciences, Environment and Land Planning, Faculty of Sciences, University of Porto,
Rua do Campo Alegre 687, 4169-007 Porto, Portugal
4
Earth Sciences Institute (ICT), Pole of the FCUP, University of Porto, 4169-007 Porto, Portugal
Keywords: Neurodegenerative Diseases, Spatial Epidemiology, Hospitalization Rates.
Abstract: Neurodegenerative diseases, usually arising from the death of nervous system cells, are a rising concern in
the worlds’ population increasing life expectancy. More precisely, the Portuguese population, along with that
of other developed countries, is ageing at a fast rate. The understanding of such diseases’ patterns is of utmost
relevance to help manage the burden it represents in the health system. In this retrospective study, we analysed
over 500 thousand hospitalizations with discharges between 2000 and 2016. We computed age-standardized
hospitalization rates for each neurodegenerative disease. The most prevalent disease in our sample was
Dementia with 43.4% of cases, and the least prevalent was Basal with only 0.2% of cases. The spatial analysis
shows that Santarém and Portalegre (neighbour) districts in central Portugal, have the highest rates. The
increase in hospitalization rates over the study period is also clear when looking at the spatio-temporal
analysis. Although limited by the usage of secondary health data, this study represents a background for other
studies on the field of neurodegenerative diseases, presenting with relevant insight into the spatio-temporal
patterns of each and every neurodegenerative disease in Portugal at the moment.
1 INTRODUCTION
Global life expectancy has been increasing, from 66.8
in 2000 to 73.3 years in 2019 (WHO, 2022) , raising
the concern on neurodegenerative diseases, since age
is one of the main contributing factors to developing
these pathologies. Neurodegeneration often occurs
due to the pathological changes in the human brain
arisen from aging (Spencer et al., 2016), which result
in the death of cells either by necrosis or delayed
apoptosis (Brown et al., 2005).
Among these diseases are Alzheimer’s and other
dementias, which contribute to 12% of the burden in
disability-adjusted life years (DALYs), worsened by
the fact that it is the most common form of late onset
a
https://orcid.org/0000-0001-7313-9749
b
https://orcid.org/0000-0003-2113-9653
c
https://orcid.org/0000-0002-8043-6431
d
https://orcid.org/0000-0001-6558-8966
dementia globally (Rabinovici, 2019). Along with
Parkinson’s disease, they are the most common
neurodegenerative diseases (de Lau & Breteler, 2006;
Jankovic, 2008). Patients with these diseases are more
susceptible to longer lengths of stay and represent a
higher mortality rate, as well as a higher likeliness to
be discharged to long-term care (Timmons et al.,
2015). Other neurodegenerative diseases include
Multiple Sclerosis, Huntington’s, Basal Ganglia and
Pick’s.
Some risk factors to these diseases have been
already discussed. For instance, atop from age as
presented earlier, gender, hereditarianism and
environmental exposure to pollution are all
established risk factors for many of the
neurodegenerative diseases. For instance, in
Oliveira, M., Freitas, A., Teodoro, A. and Gonçalves, H.
Spatial Patterns in Neurodegenerative Disease’s Hospitalizations in Portugal (2000-2016).
DOI: 10.5220/0011990100003473
In Proceedings of the 9th International Conference on Geographical Information Systems Theory, Applications and Management (GISTAM 2023), pages 79-86
ISBN: 978-989-758-649-1; ISSN: 2184-500X
Copyright © 2024 by Paper published under CC license (CC BY-NC-ND 4.0)
79

literature, one third of Alzheimer’s patients are
female, while with Parkinson’s the prevalence is
greater in male patients (de Lau & Breteler, 2006). On
the other hand, Huntington’s disease is entirely
acquired through hereditarianism, and some forms of
Alzheimer’s, mainly early-onset, are also transmitted
through genetics (Price et al., 1998).
Furthermore, several studies have showed the
significance of spatially analysing neurodegenerative
disorders, displaying spatial patterns that uncover
new correlations with variables such as latitude and
environmental pollutants (Oliveira et al., 2020).
Mapping such diseases and understanding the
distribution and characteristics of the patients is of
ultimate importance to plan and mitigate for such
disorders.
To the authors’ best knowledge, this is the first
study developed in Portugal which describes the
hospitalizations by neurodegenerative disorders, both
statistically and spatially. With this retrospective
study with data from 2000 to 2016, we hope to help
provide insight on the distribution of these diseases.
2 MATERIALS AND METHODS
2.1 Study Area
This study was conducted with data from Portugal
mainland, located in the southwest of Europe, with an
area of approximately 89.000 km
2
and an aging
population of around 10,000,000 inhabitants, 21% of
which are 65 years old or older (INE, 2020). Figure 1
shows the distribution of age groups population for
each district of Portugal, using 10 years-old
categories. Population is also very heterogeneously
distributed, as visible in Figure 2.
2.2 Data Acquisition
2.2.1 Health Data
Hospitalizations of patients with at least one
neurodegenerative pathology coded as a diagnosis,
both principal or secondary, were obtained from
secondary hospitalization data, with discharges
between 2000 to 2016. No further years were
included since the provided data frame included only
hospitalizations from 2000 to 2018, but both 2017 and
2018 were incomplete and would thus result in non-
comparable results. Each record contains the year,
patient’s sex, age and residence (coded up to the
parish), entry and leave dates, length of stay and
coded diagnosis.
Figure 1: Population age distribution per groups of 10 years
for each district (2000 to 2021 mean).
Neurodegenerative pathologies codes were
retrieved from literature review (Kim et al., 2019; Lee
et al., 2019; Min et al., 2020; Rochoy et al., 2019; St
Germaine-Smith et al., 2012; Wetmore et al.,
2019),along with counselling with coding experts. All
resulting International Classification of Diseases
(ICD) codes used are listed in Table 1.
GISTAM 2023 - 9th International Conference on Geographical Information Systems Theory, Applications and Management
80

Figure 2: Population percentage per district.
2.2.2 Population Data
Population data was retrieved from National Institute
of Statistics (INE) Population Census for the years of
2001, 2011 and 2021, for each Portuguese mainland
parish. These data were then linearly interpolated to
obtain an approximate value of population by year,
further used to normalize health data. District and
municipality population was also computed from the
sum of the contained parishes. Only integer values
were used, due to the nature of the population
variable.
2.3 Data Processing
All data pre-processing, descriptive analysis and
mapping was done using Python programming
language.
Table 1: ICD codes used to retrieve hospitalization data.
Dia
g
nosis ICD 9 ICD 10
Alzheime
r
331.0 G30
Pick's 331.1
G31
Lewy 331.8
Creutzfeldt 046 A81.0
Huntington 333.4 G10
Parkinson 332 G20
Motor neuron disease 335 G12.2
Multi
p
le sclerosis 340 G35
Basal ganglia 333.0 G23
Dementia
Vascula
r
290.4
F01
F02
F03
Uns
p
ecifie
d
294
Senile 331.2
Cerebral de
g
eneration 331.7
Presenile 290.1
Senile with delusion 290.2
Senile with deliriu
m
290.3
Alcohol induce
d
291.2
Dru
g
induce
d
292.82
Other 331.9
G32
Health data was loaded and diagnosis codes were
extracted and recoded as the disease they referred to.
For example, ICD-9 code 331.0 and ICD-10 code
G30 were both recoded as ‘Alzheimer’. The category
“Other”, as stated in the ICD, represents the other
neurodegenerative diseases not described elsewhere
by the alternative codes. Age was grouped into three
categories: under 20 years old, 20 to 70 years old, and
over 70 years old. These categories were chosen to
adapt to the available population categories, as well
as to accommodate the distinction between paediatric,
early onset and late onset neurodegenerative diseases
(Fatima et al., 2022).
Afterwards, general descriptive statistics was
computed. Then, data was grouped by either district,
municipality or parish to proceed to mapping, and
population in each administrative area, as well as the
percentage of each age group, were used to compute
age-standardized hospitalization rates (ASHR), using
equation 1 (Curado et al., 2007). This rate allows data
to be normalized and therefore enables comparison of
the rates, both across space and time, with a lower
degree of error.
𝐴𝑆𝐻𝑅 =
𝑁
𝑃𝑜𝑝𝑢𝑙𝑎𝑡𝑖𝑜𝑛
×%
(1)
In equation 1, N
AgeGroup
represents the number of
hospitalizations in each age group, Population
represents the total population in the area
corresponding to each age group (for example, each
district) and %AgeGroup the percentage of the age
group in the population. The resulting data was
therefore mapped to establish spatio-temporal
patterns.
Spatial Patterns in Neurodegenerative Disease’s Hospitalizations in Portugal (2000-2016)
81

3 RESULTS
3.1 Descriptive Statistics
A total of 502 245 hospitalizations were included in
this study. As represented in the graphic in Figure 3,
the most prevalent disease was Dementia (43.4%),
followed by Other (22.7%) and Alzheimer (20.2%).
Basal was the least prevalent disease (0.2%).
Figure 3: Number of hospitalizations and respective
percentage per neurodegenerative disease, relative to the
total number of hospitalizations.
Most patients were female (56.3%) and 81.3% of all
patients were over 70 years old, with only 0.4% of the
cases representing paediatric disorders (under 20
years old). Of these, Motor Neuron was by far the
most prevalent neurodegenerative disease with 748
cases (Table 2).
3.2 Spatial Analysis
As expected, mapping the available data provided
frther insight on the spatio-temporal distribution,
otherwise difficult to grasp from algebraic statistical
methods.
Although the descriptive statistics pointed the
Centre as the area with the most prevalence of overall
neurodegenerative diseases, mostly coded as
“Dementia”, the map of the hospitalization rates
(Figure 4) shows that the most incidence is found in
the district of Bragança, located in the north of
Portugal. Furthermore, Porto district, where a main
metropolis of Portugal is located, has lower
hospitalization rates, contrarily to Lisbon, the other
major metropolis of Portugal. Each individual disease
is also mapped in Figure 5.
Figure 4: Age-standardized hospitalization rates by
neurodegenerative diseases per district for the years 2000 to
2016.
Another relevant aspect to be mapped is the temporal
series. In this, the results clearly show that most
districts exhibited a consistent increase throughout
the years, particularly Portalegre in the southeast
(Figure 6).
4 DISCUSSION
To the best of the authors’ knowledge, this is the first
population based spatio-temporal descriptive study of
neurodegenerative pathologies in Portugal. This work
relies on the availability of nationwide hospitalization
data from public hospital for 17 years, thus
representing a significant sample of patients with
neurodegenerative diseases in Portugal. Furthermore,
the availability of each patient’s residence allows for
a spatial analysis not available as standard practice.
GISTAM 2023 - 9th International Conference on Geographical Information Systems Theory, Applications and Management
82

Table 2: Descriptive statistics of each neurodegenerative disease included in this study, as well as their total. Categorical data
(sex, age group and residence) is described by its absolute frequency and percentage, while continuous data (age and length
of stay, which are both asymmetrically distributed), is described by its median and interquartile range. The total row describes
the total frequency of each disease and their respective percentage. yo: years old.
As expected, elders were the most prevalent age
group, representing over 81% of the overall patients.
Only for Creutzfeldt, Huntington, Motor Neuron,
Multiple Sclerosis and Pick was the age mean lower
than 65 years old. Most patients were women (56%)
and patients were hospitalized for a median of 8 days.
As for the spatial patterns found, the centre showed a
slightly higher incidence of neurodegenerative
diseases although the rates are similar throughout the
country.
Porto didn’t show especially high rates of
hospitalizations, even though it is one of the most
populated cities of Portugal. This may be due to easier
access to health, which may allow for the better
management of the diseases, avoiding
hospitalization. On the opposite side, the higher rate
of hospitalizations in the interior of the country where
isolation and aging population are combined to hinder
health access may be thus explained. Other reason
may involve lower literacy, which is a known risk
factor for developing neurodegenerative diseases, and
highly inequal between the interior and the coast of
the country (Ávila, 2006).
Furthermore, the aging of the population is well
represented in the higher rates of hospitalizations
along the time period of the study.
4.1 Limitations
One of the major limitations in our work is the fact
that the hospitalizations dataset does not include a
unique patient identifier, to allow us to attempt to
identify patients unequivocally. As such, if a patient
with a neurodegenerative disease
has been
hospitalized more than once, it will appear repeated
in our database, without us being able to realize it and
filter it out. For this reason, data here represented may
be oversampling some disease that would naturally
require more hospitalizations than other. Ideally,
datasets should include a unique patient identifier to
advert this issue.
Alzheimer
Basal
Creutzfeldt
Dementia
Huntington
Lewy
Motor Neuron
Multiple Sclerosis
Parkinson
Pick
Other
Total
Sex
Female
62349
(61.4)
659
(55.8)
1209
(34.1)
127694
(58.6)
736
(47.1)
3458
(49.9)
3272
(45.5)
12062
(67.2)
56977
(50.0)
722
(45.1)
13775
(47.4)
282913
(56.3)
Male
39256
(38.6)
521
(44.2)
2332
(65.9)
90087
(41.4)
828
(52.9)
3474
(50.1)
3919
(54.5)
5898
(32.8)
56877
(50.0)
879
(54.9)
15260
(52.6)
219331
(43.7)
Age (yo)
81
[76, 85]
72
[61, 79]
48
[38, 68]
82
[76, 87]
58
[47, 70]
78
[70, 84]
65
[53, 73]
43
[33, 54]
79
[73, 84]
68
[60, 77]
76
[66, 83]
80
[74, 86]
A
g
e Grou
p
< 20 yo
16 (0.0) 39 (3.3)
116
(3.3)
157
(0.1)
29 (1.9)
130
(1.9)
748
(10.4)
403
(2.2)
59 (0.1) 2 (0.1)
187
(0.6)
1886
(0.4)
20-70 yo
9018
(8.9)
511
(43.3)
2649
(74.8)
25241
(11.6)
1169
(74.7)
1656
(23.9)
4087
(56.8)
16775
(93.4)
20052
(17.6)
956
(59.7)
9740
(33.5)
91854
(18.3)
> 70 yo
92571
(91.1)
630
(53.4)
776
(21.9)
192383
(88.3)
366
(23.4)
5146
(74.2)
2356
(32.8)
782
(4.4)
93744
(82.3)
643
(40.2)
19108
(35.8)
408505
(81.3)
Length of
stay (days)
8
[4, 13]
8
[4, 15]
15
[7, 34]
8
[5, 14]
9
[4, 16]
9
[5, 16]
7
[3, 13]
5
[2, 9]
8
[4, 14]
12
[6, 24]
9
[5, 17]
8
[4, 14]
Residence
North
37116
(36.5)
513
(43.5)
973
(27.5)
79156
(36.3)
437
(27.9)
2687
(38.8)
2396
(33.3)
5411
(30.1)
35190
(30.9)
554
(34.6)
22274
(76.7)
186707
(37.2)
Centre
49750
(49.0)
518
(43.9)
1897
(53.6)
114337
(52.5)
882
(56.4)
3642
(52.5)
3621
(50.4)
9487
(52.8)
61947
(54.4)
901
(56.3)
5225
(18.0)
252207
(50.2)
South
14739
(14.5)
149
(12.6)
671
(18.9)
24288
(11.2)
245
(15.7)
603
(8.7)
1174
(16.3)
3062
(17.0)
16718
(14.7)
146
(9.1)
1536
(5.3)
63331
(12.6)
Total
101605
(20.2)
1180
(0.2)
3541
(0.7)
217781
(43.4)
1564
(0.3)
6932
(1.4)
7191
(1.4)
17960
(3.6)
113855
(22.7)
1601
(0.3)
29035
(5.8)
502245
(100)
Spatial Patterns in Neurodegenerative Disease’s Hospitalizations in Portugal (2000-2016)
83

Figure 5: Neurodegenerative diseases’ spatial distribution per district.
Reusing data is not always as accurate as
desirable. Nevertheless, it is the best available option
when studying a large population throughout a large
time frame, without the implications of collecting
data prospectively.
4.2 Implications and Future Work
This study may be used as a base for further studies
concerning neurodegenerative pathologies, as it gives
insight on the spatial patterns expected, as well as to
anticipating the statistical distribution of Portuguese
public hospitalization data.
GISTAM 2023 - 9th International Conference on Geographical Information Systems Theory, Applications and Management
84
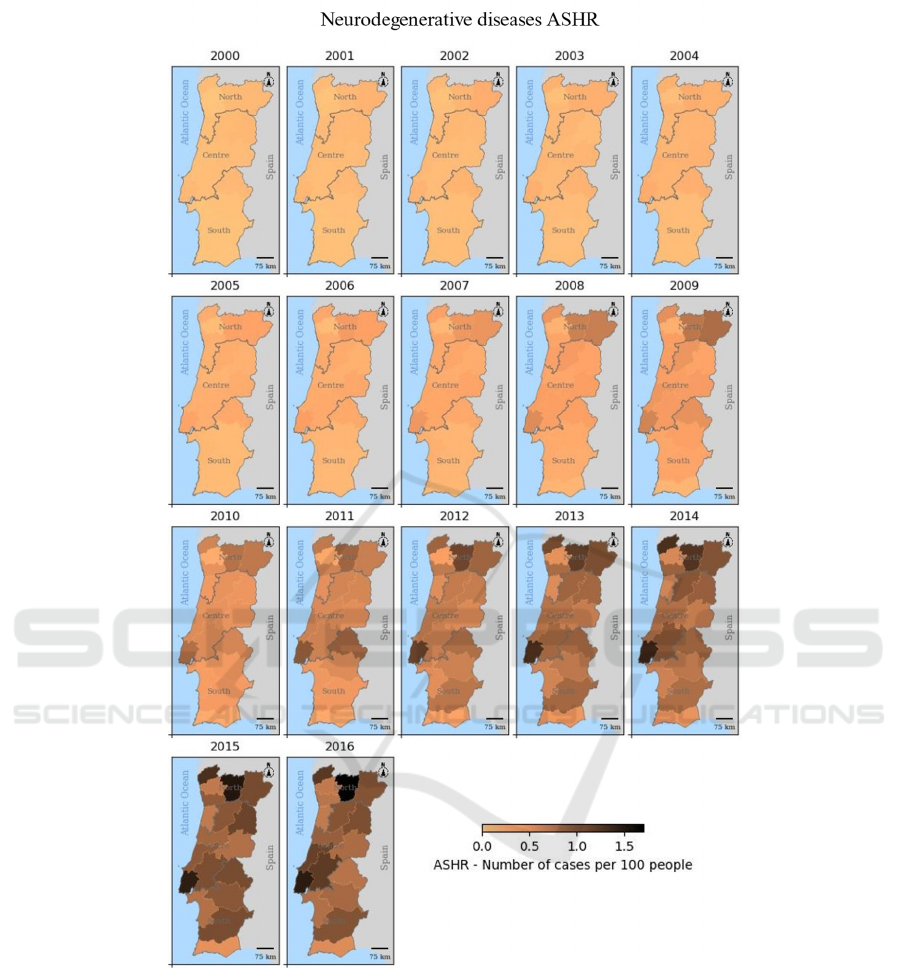
Figure 6: Spatio-temporal age-standardized hospitalization rates by neurodegenerative diseases per district for each year, from
2000 to 2016.
5 CONCLUSION
This work describes the spatio-temporal patterns of
age-standardized hospitalization rates of
neurodegenerative diseases, in Portugal mainland,
from 2000 to 2016. The most prevalent disease was
Dementia, and the least prevalent was Basal.
The
aging Portuguese population is notorious on
the temporal analysis, where it becomes clear that
neurodegenerative diseases incidence is increasing.
Also, disparities in health access become clear as
interior districts have higher hospitalization rates than
littoral ones and, mostly, than the larger metropolis.
With this work, we hope that the established
patterns may be of use when working with similar data
sources.
Spatial Patterns in Neurodegenerative Disease’s Hospitalizations in Portugal (2000-2016)
85

ACKNOWLEDGEMENTS
This research was funded by FCT – Fundação para a
Ciência e Tecnologia, grant number SFRH/BD/
147324/2019 and national MCTES funds and
supported also by National Funds through FCT –
Fundação para a Ciência e a Tecnologia, I.P., within
CINTESIS, R&D Unit (reference UIDB/4255/2020).
Hospitalization data was provided by the Central
Administration of the Health System, I.P. (ACSS).
REFERENCES
Ávila, P. D. (2006). A literacia dos adultos: competências-
chave na sociedade do conhecimento.
Brown, R. C., Lockwood, A. H., & Sonawane, B. R. (2005).
Neurodegenerative diseases: an overview of
environmental risk factors. Environ Health Perspect,
113(9), 1250-1256. https://doi.org/10.1289/ehp.7567
Carvalho, R., Lobo, M., Oliveira, M., Oliveira, A. R.,
Lopes, F., Souza, J., Ramalho, A., Viana, J., Alonso, V.,
Caballero, I., Santos, J. V., & Freitas, A. (2021).
Analysis of root causes of problems affecting the quality
of hospital administrative data: A systematic review and
Ishikawa diagram. Int J Med Inform, 156, 104584.
https://doi.org/10.1016/j.ijmedinf.2021.104584
Curado, M.-P., Edwards, B., Shin, H. R., Storm, H., Ferlay,
J., Heanue, M., & Boyle, P. (2007). Cancer incidence in
five continents, Volume IX. IARC Press, International
Agency for Research on Cancer.
de Lau, L. M., & Breteler, M. M. (2006). Epidemiology of
Parkinson's disease. Lancet Neurol, 5(6), 525-535.
https://doi.org/10.1016/s1474-4422(06)70471-9
Fatima, K., Mehendale, A. M., & Reddy, H. (2022). Young-
Onset Dementia and Neurodegenerative Disorders of
the Young with an Emphasis on Clinical
Manifestations. Cureus, 14(10).
INE, N. S. I. (2020). Projections of resident population in
Portugal. Retrieved 25/01/2023 from https://www.
ine.pt/xportal/xmain?xpid=INE&xpgid=ine_destaques
&DESTAQUESdest_boui=406534255&DESTAQUE
Smodo=2&xlang=en
Jankovic, J. (2008). Parkinson's disease: clinical features
and diagnosis. J Neurol Neurosurg Psychiatry, 79(4),
368-376. https://doi.org/10.1136/jnnp.2007.131045
Kim, S. Y., Min, C., Oh, D. J., & Choi, H. G. (2019). Risk
of neurodegenerative dementia in asthma patients: a
nested case–control study using a national sample
cohort. BMJ Open, 9(10), e030227. https://doi.org/
10.1136/bmjopen-2019-030227
Lee, S. Y., Lim, J. S., Oh, D. J., Kong, I. G., & Choi, H. G.
(2019). Increased risk of neurodegenerative dementia in
women with migraines: A nested case-control study
using a national sample cohort. Medicine (Baltimore),
98(7), e14467. https://doi.org/10.1097/md.00000000000
14467
Min, C., Bang, W. J., Kim, M., Oh, D. J., & Choi, H. G.
(2020). Rheumatoid arthritis and neurodegenerative
dementia: a nested case-control study and a follow-up
study using a national sample cohort. Clinical
Rheumatology, 39(1), 159-166. https://doi.org/10.1007
/s10067-019-04769-x
Oliveira, M., Padrão, A., Ramalho, A., Lobo, M., Teodoro,
A. C., Gonçalves, H., & Freitas, A. (2020). Geospatial
Analysis of Environmental Atmospheric Risk Factors in
Neurodegenerative Diseases: A Systematic Review.
International Journal of Environmental Research and
Public Health, 17(22), 8414. https://www
.mdpi.com/1660-4601/17/22/8414
Price, D. L., Sisodia, S. S., & Borchelt, D. R. (1998). Genetic
Neurodegenerative Diseases: The Human Illness and
Transgenic Models. Science, 282(5391), 1079-1083.
https://doi.org/doi:10.1126/science.282.5391.1079
Rabinovici, G. D. (2019). Late-onset Alzheimer Disease.
Continuum (Minneap Minn), 25(1), 14-33. https://
doi.org/10.1212/con.0000000000000700
Rochoy, M., Bordet, R., Gautier, S., & Chazard, E. (2019).
Factors associated with the onset of Alzheimer's
disease: Data mining in the French nationwide
discharge summary database between 2008 and 2014.
PLoS One, 14(7), e0220174. https://doi.org/10.1371/
journal.pone.0220174
Santurtún, A., Delgado-Alvarado, M., Villar, A., &
Riancho, J. (2016). Patrón geográfico de la mortalidad
por enfermedad de Parkinson en España y su asociación
con los niveles de plomo en el aire [10.1016/
j.medcli.2016.07.022]. Medicina Clínica, 147(11), 481-
487. https://doi.org/10.1016/j.medcli.2016. 07.022
Spencer, P. S., Palmer, V. S., & Kisby, G. E. (2016). Seeking
environmental causes of neurodegenerative disease and
envisioning primary prevention. Neurotoxicology, 56,
269-283. https://doi.org/10.1016/j.neuro.2016.03.017
St Germaine-Smith, C., Metcalfe, A., Pringsheim, T.,
Roberts, J. I., Beck, C. A., Hemmelgarn, B. R.,
McChesney, J., Quan, H., & Jette, N. (2012).
Recommendations for optimal ICD codes to study
neurologic conditions: a systematic review. Neurology,
79(10), 1049-1055. https://doi.org/10.1212/WNL.0b013
e3182684707
Timmons, S., Manning, E., Barrett, A., Brady, N. M.,
Browne, V., O’Shea, E., Molloy, D. W., O'Regan, N. A.,
Trawley, S., Cahill, S., O'Sullivan, K., Woods, N.,
Meagher, D., Ni Chorcorain, A. M., & Linehan, J. G.
(2015). Dementia in older people admitted to hospital:
a regional multi-hospital observational study of
prevalence, associations and case recognition. Age and
Ageing, 44(6), 993-999. https://doi.org/10.1093/
ageing/afv131
Wetmore, J. B., Li, S., Yan, H., Irfan, M., Rashid, N., Peng,
Y., Gilbertson, D. T., & Shim, A. (2019). Increases in
institutionalization, healthcare resource utilization, and
mortality risk associated with Parkinson disease
psychosis: Retrospective cohort study. Parkinsonism
Relat Disord, 68, 95-101. https://doi.org/10.1016/
j.parkreldis.2019.10.018
WHO, W. H. O. (2022). World Health Statistics 2022.
GISTAM 2023 - 9th International Conference on Geographical Information Systems Theory, Applications and Management
86
