
Look at the Horizon: Evaluation of a Software Solution Against
Cyber Sickness in Virtual Reality Applications
Jonathan Harth
1a
, Christian-Norbert Zimmer
2
and Michaela Zupanic
3b
1
Chair of Sociology, Witten/Herdecke University, 58455 Witten, Germany
2
Mixed Reality and Visualization (MIREVI),
University of Applied Sciences Duesseldorf, 40233 Düsseldorf, Germany
3
Interprofessional and Collaborative Didactics in Medical and Health Professions, Witten/Herdecke University,
58455 Witten, Germany
Keywords: Cyber Sickness, Virtual Reality, Mixed Methods, Software Layer, Evaluation Study.
Abstract: Cyber sickness (CS), a symptom that occurs in 30-80% of users when using virtual environments, is still
considered an obstacle to the spread of virtual reality (VR). The aim of this study is to investigate whether
symptoms of CS can be minimised by software adaptation. A prototype of a layer based on the "Seetroën
Glasses" was used for this purpose. 80 students participated in the study with virtual roller coaster rides. The
results show that the group with the layer was able to increase its performance and that the layer was able to
delay the exit of the participants for about 2 laps. The layer does not provide immunity to CS, but it does delay
the onset of symptoms. The study shows that the virtual test environment is suitable for investigating CS and
that the prototype of the layer may be promising for reducing symptoms of CS.
1 INTRODUCTION
Immersive interfaces such as simulators or virtual
environments enable impressive interactions and
compelling user experiences, but they carry the risk
of severely compromising subjective well-being
(Chang et al. 2021; Mayor et al. 2021). The problem
is known by many names, e.g., simulator sickness or
cyber sickness (Dennison/Krum 2019), and it is an
open debate whether these refer to the same or closely
related aspects of motion sickness (see
David/Nesbitt/Naivaikko 2014; Gavgani et al. 2018;
Zupanic 1993). Modern simulation systems such as
the use of virtual reality (VR) can also trigger the
above-mentioned complaints. However, as long as
these negative effects in the use of virtual reality
cannot be reliably avoided, they will continue to be a
major obstacle to the growth of the VR medium.
Cyber sickness is a condition that can occur
during or after exposure to virtual environments.
Symptoms include headaches, eye strain, nausea or
even vomiting in extreme cases (LaViola 2000). It is
estimated that some degree of cyber sickness occurs
a
https://orcid.org/0000-0002-8433-0896
b
https://orcid.org/0000-0002-7166-5160
in about 30% to 80% of all users (cf.
Rebenitsch/Owen 2016).
Cyber sickness is therefore considered a major
obstacle to the spread of the medium of virtual reality
(VR). Although the phenomenon has been known for
a long time under the names of simulator sickness or
motion sickness and is attributed to conflicts between
the visual and vestibular systems
(Stanney/Kennedy/Drexler 1997), there is still no
generally recognised solution for the prevention of
the disease that is suitable for everyday use
(Saredakis et al. 2020; Yildirim 2020).
2 RELATED WORKS
A large body of research on cyber sickness aims at a
better understanding of the symptoms of the disease
and the factors of its cause (see for an overview
Duzmanska 2018 and Rebenitsch/Owen 2016).
According to the theory of "sensory mismatch", the
most likely cause of cyber sickness is a mismatch
between visual stimuli and the corresponding
vestibular or proprioceptive feedback (see Gavgani et
Harth, J., Zimmer, C. and Zupanic, M.
Look at the Horizon: Evaluation of a Software Solution Against Cyber Sickness in Virtual Reality Applications.
DOI: 10.5220/0012049900003541
In Proceedings of the 12th International Conference on Data Science, Technology and Applications (DATA 2023), pages 13-21
ISBN: 978-989-758-664-4; ISSN: 2184-285X
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)
13

al. 2018). In addition, other factors can also contribute
to the occurrence of motion sickness. These factors
can be divided into hardware-dependent categories
(e.g., tracking problems or input/output delays,
refresh rate of displays, as well as screen tearing) or
content-related categories (such as the visual
representation of the direction of motion or the
presence of linear or angular accelerations).
In addition, the processing of perceptions varies
between people. Field dependence describes the
tendency to which the perception of one's own body
position in space is influenced by contextual
information (Witkin et al. 1954). Individuals with
higher levels of field dependence rely more heavily
on external cues (e.g., reference frames, background
objects), while field-independent individuals rely
more heavily on internal cues (e.g., vestibular,
proprioceptive) to perceive body position. Field
independence is more common in men and associated
with lower susceptibility to motion sickness (Bendall
et al. 2016). Field dependence can affect the
perception of vection (illusory self-motion) in virtual
space when a visual frame is missing and the vertical
of the earth is not clearly displayed (Keshararz et al.
2016).
An innovative and promising solution against the
occurrence of motion sickness while travelling by car
or train has been presented by the car manufacturer
Citroën. The so-called "Seetroën Glasses" (Figure 1)
add a variable horizon to the peripheral field of vision
of the wearer. According to the manufacturer, this
leads to a peripheral and stable focus of the
surroundings, which suppresses the symptoms of
motion sickness (cf. Picot/Wright 2016). The
manufacturer of the glasses advertises a success rate
of 95 %. In addition, the Seetroën glasses are said to
take effect in only 10-12 minutes even if motion
sickness is present and could even be taken off again
afterwards (cf. Citroën 2020). Unfortunately, we
could not find any independent research or evidence
for the effectiveness of these glasses.
Figure 1: Seetroën Glasses (cf. Citroën 2020).
The aim of this study was to investigate whether
and to what extent discomfort in the use of virtual
applications can be minimized by a software-based
adaptation from the motion sickness domain.
3 METHODS
Both the layer and the application were created from
scratch in the Unity Engine for this study. For the
conception of the virtual layer, we adapted the
principle of the "Seetroën glasses" (Figure 1) of the
car manufacturer Citroën. In principle, the layer
should also be easy to use in any VR application. To
test the effect of the layer, we therefore created an
application that can induce cyber sickness in the first
place.
For this purpose, a prototype was developed
together with the University of Applied Sciences
Düsseldorf, which provides the user with peripheral
fixed points in the head-mounted display (HMD) in
the style of the "Seetroën Glasses" (see Figures 2, 3).
The application was realised in the Unity engine
and shows the following features:
Roller coaster ride with a duration of 70
seconds per lap,
Activation / deactivation of endless rides,
Activation / deactivation of VR layer,
Additional offset for layer (0-1),
Options for the virtual distance of the
layer to the user's POV (2m, 1m, 50cm,
30cm, 20cm, 10 cm).
The test environment of the study consists of a
virtual roller coaster ride that goes through a looping
and several steep curves and slopes. The aim of the
design of the roller coaster was to create a suitable
environment that can lead to cyber sickness.
Overhead rides as well as tight curves while travelling
fast are considered good conditions for generating the
symptoms under investigation (Islam et al. 2020).
The Hardware Setup for the study consisted of a
capable VR computer (AMD Ryzen 5600, GeForce
RTX 3080, 32 GB RAM) and a suitable VR Headset
(Valve Index).
By means of a virtual visual layer, which is
modelled on these glasses, the visual-vestibular
conflicts of the users should be eliminated. The main
research question was to what extent the principles of
the anti-motion sickness glasses "Seetroën Glasses"
by the car manufacturer Citroën can be transferred to
the use of VR headsets and to what extent the layer
can help against the symptoms of cyber sickness.
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
14
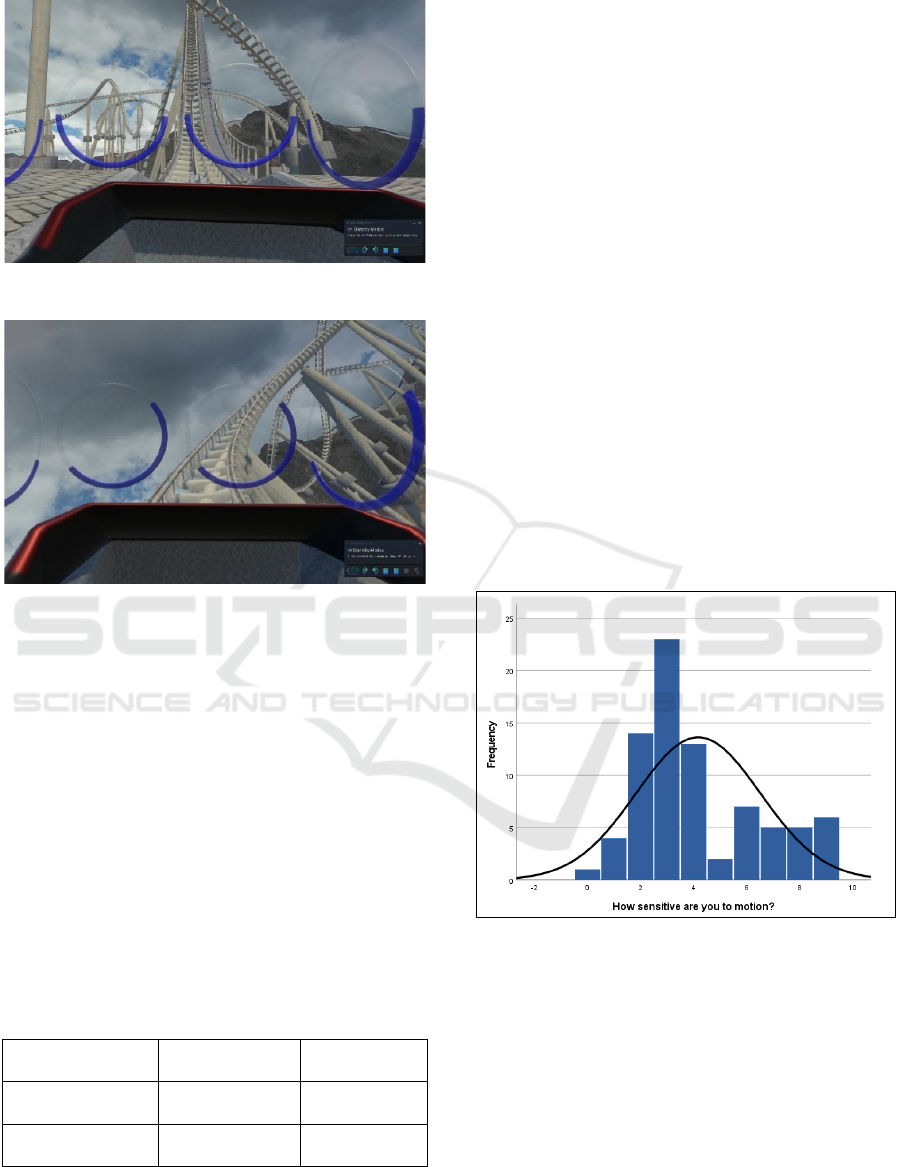
Figure 2: Rollercoaster with activated layer.
Figure 3: Dynamic adaptation of the layer to the virtual
horizon.
3.1 Participants
Eighty students (49 female, 31 male) with an average
age of 23.51 ± 5.89 years (minimum 18, maximum 45
years) participated in the study and were randomly
assigned to one of the two groups: control or layer.
The extent of field dependence was measured with
three visual perception subtests by summing the
individual raw scores and classifying them as norm
scores (c.f., LPS-2; Kreuzpointner/Lukesch/Horn
2013). The average norm score for performance in the
LPS-2 Visual Perception was 101.50 ± 14.73
(minimum 74, maximum 139).
Table 1: Quasi experimental design with perception style
and viewing conditions.
Intervention
with layer
Control
without laye
r
Field dependence
low
N=20
(11 f., 9 m.)
N=21
(10 f., 11 m.)
Field dependence
hi
g
h
N=20
(
15 f., 5 m.
)
N=19
(
13 f., 6 m.
)
After median dichotomization of performance in
the LPS-2 Visual Perception, participants with a score
below the median of 100 were classified as field
dependent, and participants with a score above 100
were classified as field independent. Considering the
perceptual style and the viewing conditions, the
results of the participants are grouped in a quasi-
experimental design (see Table 1.). Female (f.) and
male (m.) participants are evenly distributed across
the four groups.
The participants' experience with motion
stimulation was also asked. About one third of the
sample (N=25, 31.3 %) said they had never ridden a
roller coaster or only once, 25 % (N=20) up to ten
times and most participants (N=35, 43.8 %) more
than ten times. When asked how often they played
computer games, half (N=42, 52.5 %) said they never
played, followed by at least once a month (N=19, 23.8
%), at least once a week (N=15, 18.8 %) and daily
(N=4, 5 %). Only 4 participants (5 %) use VR at least
once a month. The rating of the subjective sensitivity
to motion on a scale of 0-10 resulted in an average
value of 4.18 ± 2.34 (minimum 0, maximum 9) for
the sample. The distribution is right skewed
(skewness = .736) and flattened (kurtosis = -.493),
with many small values. The participants thus tend to
describe themselves as insensitive to motion (Figure
4).
Figure 4: Ratings of subjective sensitivity to motion
(N=80).
3.2 Materials and Procedures
In a mixed methods approach, we conducted a quasi-
experimental study with a questionnaire survey, static
ataxia tests and a subsequent evaluation by qualitative
interviews. While the questionnaires establish
objectifiable coherence between the level of cyber
sickness and the different prototypes, the interviews
primarily served as a subjective assessment and
articulation of the experiences from the subjects'
point of view. Conditions for participation were a
Look at the Horizon: Evaluation of a Software Solution Against Cyber Sickness in Virtual Reality Applications
15

minimum age of 18 years and the exclusion of serious
illnesses (e.g., epilepsy, serious cardiovascular
diseases, diseases of the hearing organ), a pacemaker
or other implanted medical devices as well as acute or
chronic mental illnesses.
The study received a positive vote from the Ethics
Committee of Witten/Herdecke University (S-
142/2021). In addition, the subjects had the option of
discontinuing their participation in the study at any
time, which is pointed out to them in a consent form.
Furthermore, the study complies with the Code of
Conduct on the Ethical Use of Virtual Reality in
Research (cf. Madary/Metzinger 2016).
The Cyber Sickness Questionnaire (CSQ) was
developed based on the Simulator Sickness
Questionnaire (cf. Kennedy 1993; Bimberg et al.
2020) and the Virtual Reality Sickness Questionnaire
(cf. Kim 2018; Sevinc/Berkman 2020). It serves as a
quantifiable survey form and consists of a total of 24
items, with six demographic items (age, gender,
previous VR experience) and nine items on symptoms
of cyber sickness, e.g., nausea, headaches, dizziness.
The CSQ is presented to the test subjects before and
after the roller coaster ride to enable a pre/post
comparison.
The static ataxia tests were also conducted in a
pre/post design to measure possible balance disorders
(disequilibrium; cf. Litleskare 2021) of the subjects
that could be caused by the roller coaster ride. In the
static ataxia tests, a body posture is to be maintained
for a certain duration (30 seconds), first with open and
then with closed eyes. The performance in the tests
SPLEO (stand on preferred leg eyes open) and
SPLEC (stand on preferred leg eyes closed) as well as
SNPEO (stand on non-preferred leg eyes open) and
SNPEC (stand on non-preferred leg eyes closed) is
recorded before and after the roller coaster ride.
The perceptual style field dependence was
recorded with the three subtests of the performance
test system (LPS-2; Kreuzpointner/Lukesch/Horn
2013) for visual perception: Subtest 6: mental
rotation, Subtest 7: area count and Subtest 8: line
pattern (see Table 2). In total, the performance test
system 2 contains eleven subtests in the four factors
crystalline intelligence, fluid intelligence, visual
perception, and cognitive speed. The good to very
good internal consistency of the three subtests is α =
.86 (subtest 7), α =.90 (subtest 8) and α =.93 (subtest
6).
In addition, we applied the Fast Motion Scale
(FMS) during the subject's immersion. The procedure
is as follows: Acquisition of a self-measured,
subjective measure of cyber sickness, which is
continuously queried by the study leader during the
immersion (McHugh et al. 2019). In the FMS, the
subject is asked to verbally communicate the measure
of cyber sickness, e.g., on a scale of 0-20
(Keshavarz/Hecht 2011) or 1-10 (Bock/Oman 1982).
From this, a running chart or graph of the subject's
subjective well-being can be created. This can
identify sections of an application or process that
cause increased levels of cyber sickness (McHugh et
al. 2019). In our approach, the current well-being of
the test subjects was recorded after each lap on a scale
of 0-10.
Total duration time for every single participant in
the study was about one hour.
4 RESULTS
The results of the study include both the basic
technical creation and programming of the virtual
layer in virtual reality inspired by the Seetroën glasses
as well as the test application itself and the evaluation
of the prototype in a randomised control trial.
The creation of the prototype based on the
"Seetroën Glasses" could be carried out successfully.
In VR, a layer could be activated over the visible
image in the options menu. In this way, the test
subjects could be divided into two groups: while the
control group rode the roller coaster without a layer,
the experimental group saw the layer to be tested in
their field of vision.
4.1 Cyber Sickness Questionnaire
(CSQ)
The test-theoretical examination of the questionnaire
is carried out with item analyses in which the mean
value, standard deviation and discriminatory power of
all items are calculated. According to Lienert/Raatz
(1994), the coefficient of selectivity is the correlation
of the item response with the sum value of the scale
and is the characteristic value for the extent to which
the differentiation of the persons by the item
corresponds with that by the scale.
After the intervention, the items 1 (Do you suffer
from nausea?), 4 (Do you suffer from dizziness when
your eyes are closed?) and 7 (Does your head feel
heavy or full?) have the highest agreement in the post-
CSQ, with mean values of M = 2.20, 1.73 and 1.73
respectively. The discriminatory power of the items
in the post-CSQ is in no case below the critical value
of .20, and many are in a good to very good range (r
.60).
To test the scale of the CSQ, the reliability is
calculated according to Cronbach's Alpha. This
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
16

model of internal consistency is based on the average
inter-item correlation. Characteristic values of the
CSQ scales are the scale mean (M), standard
deviations (SD) and the homogeneity coefficients (α).
As expected, the higher agreement is found in the
Post-CSQ_sum scale (1.57 ± 0.40) vs. the Pre-CSQ-
sum (1.13 ± 0.22). Both scales show a high internal
consistency, which can be rated as satisfactory to
good (α > .700).
Statistical testing of differences in the CSQ scales
between the study groups (control vs. intervention,
field-independent vs. field-dependent, quasi-
experimental design) revealed no significant
differences.
Table 2: Descriptive statistics (mean, standard deviation)
for the Post-CSQ_sum scale in the study groups (N = 80
participants).
Intervention
with la
y
er
Control
without la
y
e
r
Field dependence
low
1.54 ± 0.35 1.61 ± 0.39
Field dependence
high
1.54 ± 0.33 1.58 ± 0.53
4.2 Ataxia Tests
The ataxia tests, as well as the CSQ, were performed
before and after the roller coaster for a maximum of
30 seconds. The performance of the participants in the
two tests SOPLEC (stand on preferred leg eyes
closed) and SONPLEC (stand on non-preferred leg
eyes closed) is documented in table 3.
Table 3: Descriptive statistics for performance in the ataxia
tests (N = 80 participants).
Ataxia Tests M SD
P
r
e
_
SOPLEC
_
su
m
13.99 8.97
Post
_
SOPLEC
_
su
m
13.07 9.19
P
r
e
_
SONPLEC
_
su
m
13.46 8.81
Post
_
SONPLEC
_
su
m
13.31 8.12
Statistical testing revealed a significant
difference. While in the control group the
performance in the ataxia test SOPLEC was
significantly less favorable after the roller coaster ride
than in the pre-test, the group with the layer was able
to increase its performance (F = 4.55, p = .036).
4.3 Fast Motion Scale
The Fast Motion Scale (FMS) is an assessment of the
subjective measure of cyber sickness during the
immersion, in this case during the 15 laps of the roller
Figure 5: Error bars for performance in the pre and post
SOPLEC ataxia test before and after the intervention
(N=80).
coaster ride. Participants had the option to end the
immersion early, so only the first two laps were
completed by all. Overall, the FMS shows a large
spread of values (response scale 1 - 10). The average
number of laps is 9.20 ± 4.78 (minimum 2, maximum
15).
Table 4: Descriptive statistics for FMS items in 15 laps (N
= 80).
Fast Motion
Scale (FMS)
M SD
FMS
_
1
1.83 2.11
FMS
_
2
2.63 2.53
FMS
_
3
3.29 2.53
FMS
_
4
3.54 2.44
FMS
_
5
3.67 2.51
FMS
_
6
3.76 2.50
FMS
_
7
3.70 2.41
FMS
_
8
4.07 2.66
FMS
_
9
4.09 2.71
FMS
_
10
3.81 2.67
FMS
_
11
3.66 2.76
FMS
_
12
3.07 2.16
FMS
_
13
3.25 2.27
FMS
_
14
3.41 2.37
FMS
_
15
3.19 2.28
The rapid reduction of the sample is evident in the
survival function (Figure 5) of the Kaplan-Meier
analysis, while the 1-survival function (see Figure 6)
illustrates the growth of cyber sickness over time
described in the literature.
The first third of dropouts are up to lap 5 (N=26,
32.5 %), the middle third up to almost the last lap
(N=28, 35 %) and only one third of participants (N =
26, 32.5 %) complete the intervention with all 15 laps.
0
5
10
15
20
Control(N=40) Layer(N=40)
Pre_SOPLEC_sum Post_SOPLEC_sum
Look at the Horizon: Evaluation of a Software Solution Against Cyber Sickness in Virtual Reality Applications
17
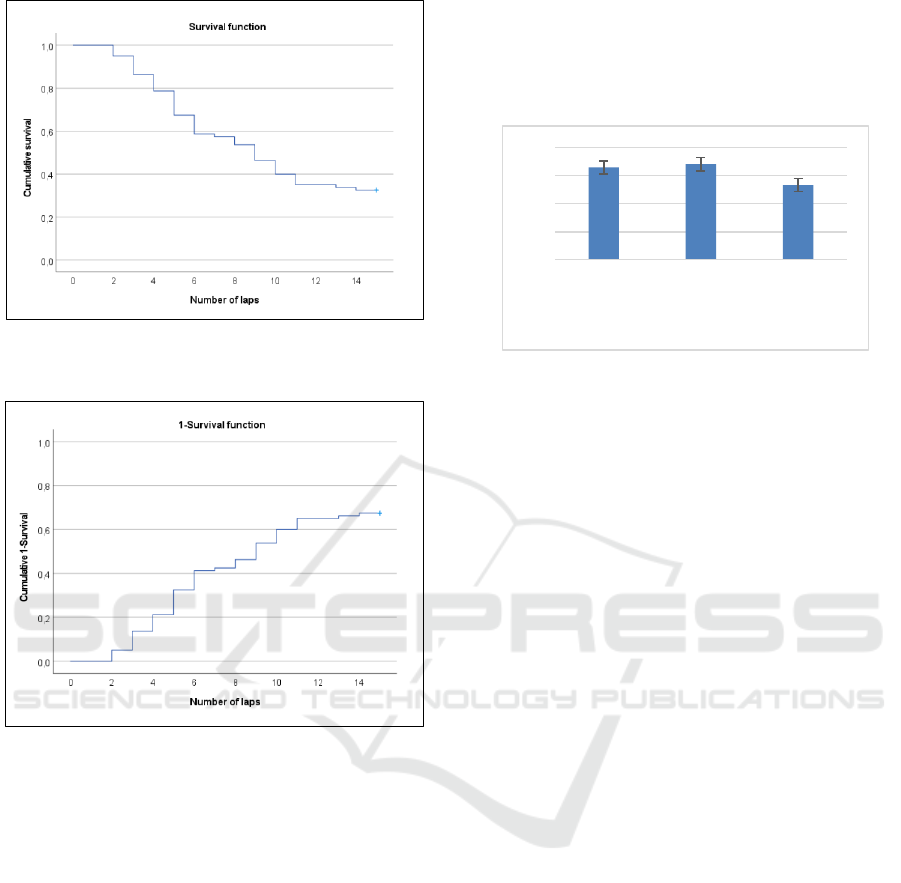
Figure 6: Survival function for the number of laps in the
roller coaster ride (N=80).
Figure 7: 1-Survival function for the onset of cyber sickness
in the roller coaster ride (N=80).
These three groups differ significantly not only in
the number of laps, but also in gender, subjective
sensitivity to exercise and in the Cyber Sickness
Questionnaire (post-CSQ) after the intervention.
There are significantly more females (N = 20) than
males (N = 6) in the early dropout group (Chi-Square
= 6.73, p = .035), who have significantly less
experience with computer games (Chi-Square =
17.24, p < .001) and describe their subjective
sensitivity to exercise at a higher level (Mann-
Whitney-U = 211, p = .018). In the Post_CSQ, the
highest expression in comparison is found in item 1
(Do you suffer from nausea?) with 2.62 ± 0.64
(Kruskal-Wallis-H = 26.21, p = .001) for this group.
In the middle group with a dropout between the
5th - 15th lap, on the other hand, a different symptom
profile emerges. Here, the highest expression in the
Post_CSQ is item 2 (Do you suffer from headaches?)
with 1.64 ± 0.73 (Kruskal-Wallis-H = 10.82, p = .004)
and item 6 (Does your head feel heavy or full?) with
1.96 ± 0.64 (Kruskal-Wallis-H = 13.49, p = .001). The
sum of the CSQ after the intervention shows clear
differences between the three groups (Kruskal-
Wallis-H = 21.72, p < .001).
Figure 8: Results in the Cyber Sickness Questionnaire
(CSQ) after the intervention (N=80).
To better understand these effects statistically, we
formed an FMS score from the sum of the individual
FMS values divided by the number of laps ridden
(transformation to scale). The FMS score is on
average 3.95 ± 1.90 (minimum 0, maximum 8) and
differentiates significantly between the control and
layer groups (Mann-Whitney: U = 566, p = .021),
with less favorable average values for the control
(4.37 ± 1.98) compared to the layer (3.52 ± 1.75).
The difference between the genders is even more
marked (Mann-Whitney: U = 487, p = .007), with
higher scores for females (4.38 ± 2.06) than for males
(3.27 ± 1.39). There is no difference in field
dependence.
5 CONCLUSIONS
Overall, the application is a very suitable test
environment for the emergence of cyber sickness.
Figures 5 and 6 clearly show how the onset of cyber
sickness steadily increases over time (or over the
duration of the roller coaster ride) and how more and
more test subjects abandon the ride. In addition, a
clear three-way division of the test subjects can be
made in our sample: while a third of the subjects
already quit by lap five, another third manages to ride
until lap 10 before quitting. The last third seems to
have no difficulty in spending the entire time in VR.
A more detailed analysis shows that the sensitive
group consists mainly of female participants who
have little experience with computer games.
This finding is consistent with the state of the
research (see Curry 2019), but not only Saredakis et
al. (2020) summarize that more research is needed to
0
0,5
1
1,5
2
Early
dropout
(N=26)
Middle
dropout
(N=28)
Latedropout
(N=26)
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
18

better identify and understand the prevalence of cyber
sickness due to gender differences or other individual
factors regarding immersive technology (Harth et al.
2018). Currently, the discrepancies identified appear
to be best explained by a complex combination of
various individual factors and uncontrolled
experimental variables (Grassini/Laumann 2020).
The main question of this study was whether the
activation of the layer makes a difference in the
occurrence of cyber sickness. However, this technical
evaluation turned out to be more difficult than
expected. The results of our study seem to be
determined by at least two limitations in their
informative value:
The transferability of our results to a
generalization is limited by the underlying sample.
Firstly, it consists of a rather young sample, and
secondly, it is very different in terms of previous
experience with digital games and virtual reality
experiences. Here, an experimental design would be
advisable for a follow-up study that is oriented
towards both the separation of genders and the
separation of computer game experience.
The methodologically determined limitation
concerns the generous offer of a possible exit at any
time during the experiment. With this, we generated
ethically valuable, but less meaningful data. This is
because it can be assumed that the test persons
terminated the experiment before the actual
occurrence of severe cyber sickness. In the case of the
sensitive subjects, this probably happened even
earlier. In a further series of experiments, we would
therefore not offer a self-chosen exit (proactively) at
any time, but rather wait for the individual wish to
quit. Therefore, a more rigid procedure, which was
not considered mainly for ethical reasons, would
probably have led to significantly higher numbers of
laps, higher scores in the FMS and more significant
differences in the post-CSQ.
Nevertheless, a clear tendency for the effect of the
layer can be seen with the data we collected. Thus,
our results are in line with the literature regarding
technical solutions against cyber sickness (cf.
Pico/Wright 2016). A direct comparison of the exit
times between the two experimental groups
with/without the layer shows that the layer can delay
the exit of the test persons by about 2 laps (see Figure
8). Although the layer does not provide immunity, it
does delay the onset of cyber sickness.
In light of our findings, it is possible that the layer
could also be utilized in other virtual reality
environments, extending its applicability beyond the
roller coaster test scenarios. Further research would
Figure 9: Comparison of the cumulative exit points during
15 rounds of rollercoaster (with layer = blue; without layer
= red; N=80).
be required to investigate the efficacy of the layer in
different settings and to determine whether its
positive effects on reducing cyber sickness symptoms
remain consistent across a wider range of
applications.
Another aspect to consider is user acceptance of
the layer. Although our study did not specifically
focus on evaluating user satisfaction, it is crucial to
explore whether users perceive the layer as a helpful
and acceptable solution in their virtual reality
experiences. Investigating the optimal transparency
levels for the layer and examining how it could be
adjusted to accommodate individual preferences and
needs would provide valuable insights for enhancing
user experience.
The layer may prove particularly useful during the
initial training phases of virtual reality applications,
akin to how astronauts undergo training to mitigate
the effects of motion sickness. By using the layer to
cushion the impact of cyber sickness during early
exposure to virtual environments, users may be able
to gradually acclimate to the VR experience,
eventually reducing their reliance on the layer. This
approach would position the layer as a temporary
solution for easing the transition into VR usage, rather
than a permanent fixture.
In conclusion, our study presents a promising first
step in exploring the potential of the layer as a means
of reducing cyber sickness symptoms. While it does
not provide complete immunity to cyber sickness, it
delays the onset of symptoms and may offer valuable
benefits for users, particularly during the initial stages
of virtual reality exposure. Further research is needed
to refine the layer's application, assess user
acceptance, and evaluate its efficacy in a broader
range of virtual environments.
0%
20%
40%
60%
80%
100%
123456789101112131415
withLayer w/oLayer
Look at the Horizon: Evaluation of a Software Solution Against Cyber Sickness in Virtual Reality Applications
19

ACKNOWLEDGEMENTS
We would like to thank the Internal Research Grant
of the Faculty of Health at Witten/Herdecke
University for funding this study.
REFERENCES
Bendall, R. C. A., Galpin, A., Marrow, L. P., & Cassidy, S.
(2016). Cognitive style: Time to experiment. Frontiers
in Psychology, 7. doi:10.3389/fpsyg.2016.01786
Bimberg, P.; Weissker, T.; Kulik, A. (2020): On the Usage
of the Simulator Sickness Questionnaire for Virtual
Reality Research. In 2020 IEEE Conference on Virtual
Reality and 3D User Interfaces, Abstracts and
Workshops (VRW), pp. 464-467. DOI: 10.1109/
VRW50115.2020.00098
Bock, O. L., & Oman, C. M. (1982): Dynamics of
subjective discomfort in motion sickness as measured
with a magnitude estimation method. Aviation, Space,
and Environmental Medicine, 53(8), 773–777.
Chang, E.; Kim, H.T. & Yoo, B. (2020): Virtual Reality
Sickness: A Review of Causes and Measurements.
International Journal of Human–Computer Interaction,
36:17, 1658-1682, DOI: 10.1080/10447318.
2020.1778351
Citroën (2020): Citrëon launches the first Glasses that
restore the taste for Travel: Seetroën! Online: unter:
https://www.citroen.com/en/Highlight/55/citroen-
launches-the-first-glasses-that-restore-the-taste-for-
travel-seetroen.
Curry, C. (2019): Cybersickness in Virtual Reality:
Examining the Influence of the Virtual Environments
on Sex Susceptibility. In SIGGRAPH Asia 2019
Doctoral Consortium (SA '19). ACM, New York, 7, 1–
4. https://doi.org/10.1145/3366344.3366628
David, S.; Nesbitt, K.; Naivaiko, E. (2014): A Systematic
Review of Cybersickness. IE2014: Proceedings of the
2014 Conference on Interactive Entertainment, 1–9,
https://doi.org/10.1145/2677758.2677780
Dennison, M.S.; Krum, D.M. (2019): Unifying Research to
Address Motion Sickness. In 2019 IEEE Conference on
Virtual Reality and 3D User Interfaces (VR), pp. 1858–
1859.
Duzmanska, N.P.; Strojny, P.; Strojny, A. (2018): Can
Simulator Sickness Be Avoided? A Review on
Temporal Aspects of Simulator Sickness. Frontiers in
psychology, 9, 2132. doi:10.3389/fpsyg.2018.02132
Gavgani, A.M.; Walker, F.R.; Hodgson, D.M.; Nalivaiko,
E. (2018): A comparative study of cybersickness during
exposure to virtual reality and "classic" motion
sickness: are they different? In: Journal of Applied
Physiology, DOI: 10.1152/japplphysiol.00338.2018
Grassini, S. & Laumann, K. (2020): Are Modern Head-
Mounted Displays Sexist? A Systematic Review
on Gender Differences in HMD-Mediated
Virtual Reality. Front Psychol. 7;11:1604. doi:
10.3389/fpsyg.2020.01604. PMID: 32903791;
PMCID: PMC7438857
Harth, J.; Hofmann, A.; Karst, M.; Kempf, D.; Ostertag, A.;
Schäfermeyer, B.; Przemus, I. (2018): Different Types
of Users, Different Types of Immersion. A User Study
on Interaction Design and Immersion in Consumer
Virtual Reality. In: IEEE Consumer Electronics
Magazine, vol. 7, no. 4, pp. 36-43, July 2018. doi:
10.1109/MCE.2018.2816218
Islam R., Lee, Y.; Jaloli, M.; Muhammad, I.; Zhu, D.; Rad,
P.; Huang, Y. & Quarles, J. (2020): Automatic
Detection and Prediction of Cybersickness Severity
using Deep Neural Networks from user’s Physiological
Signals. In: IEEE International Symposium on Mixed
and Augmented Reality (ISMAR), pp. 400-411, Porto
de Galinhas, Brazil, doi: 10.1109/ISMAR50242.
2020.00066.
Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal,
M.G. (1993): Simulator Sickness Questionnaire: An
Enhanced Method for Quantifying Simulator Sickness,
The International Journal of Aviation Psychology, 3:3,
203-220, DOI: 10.1207/s15327108ijap0303_3
Keshavarz, B., Speck, M., Haycock, B., Berti, S. (2016).
Effect of Different Display Types on Vection and Its
Interaction with Motion Direction and Field
Dependence. i-Perception, 2017, 1–18, DOI:
10.1177/2041669517707768
Keshavarz, B., & Hecht, H. (2011): Validating an efficient
method to quantify motion sickness. Human Factors,
53(4), 415–426. https://doi.org/10.1177/0018720811
403736
Kim, H.K., Park, J., Choi, Y., Choe, M. (2018): Virtual
reality sickness questionnaire (VRSQ): Motion
sickness measurement index in a virtual reality
environment. Appl Ergon. 2018;69:66-73.
doi:10.1016/j.apergo.2017.12.016
Kreuzpointner, L., Lukesch, H., Horn, W. (2013).
Leistungsprüfsystem 2. LPS-2. Hogrefe, Göttingen
2013.
LaViola, J.J. (2000): A discussion of cybersickness in
virtual environments. In: SIGCHI Bull. 32 (1), S. 47–
56. DOI: 10.1145/333329.333344.
Lienert, G.A., Raatz, U. (1994): Testaufbau und
Testanalyse. Weinheim: Beltz.
Litleskare, S. (2021). The relationship between postural
stability and cybersickness: It's complicated - An
experimental trial assessing practical implications of
cybersickness etiology. Physiol Behav. 2021 Jul
1;236:113422. doi: 10.1016/j.physbeh.2021.113422.
Madary, M.; Metzinger, T.K. (2016). Real virtuality: a code
of ethical conduct. Recommendations for good
scientific practice and the consumers of VR-
technology. Frontiers in Robotics and AI, 3, 3.
Mayor, J.; Raya, L. & Sanchez, A. (2021): A Comparative
Study of Virtual Reality Methods of Interaction and
Locomotion Based on Presence, Cybersickness, and
Usability. IEEE Transactions on Emerging Topics in
Computing, vol. 9, no. 03, pp. 1542-1553.
doi: 10.1109/TETC.2019.2915287
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
20

McHugh, N.; Jung, S.; Hoermann, S. & Lindeman, R.W.
(2019): Investigating a Physical Dial as a Measurement
Tool for Cybersickness in Virtual Reality. Proceedings
of the 25th ACM Symposium on Virtual Reality
Software and Technology (VRST '19). ACM, New
York, NY, USA, Article 32, 1–5. https://doi.org/
10.1145/3359996.3364259
Picot, E.; Wright, C.I. (2016): Motion Sickness - Newly
Engineering Glasses may Offer a Solution. J Appl
Mech Eng 5: 197. doi:10.4172/2168-9873.1000197
Rebenitsch, L., Owen, C. (2016): Review on cybersickness
in applications and visual displays. Virtual Reality 20,
101–125. https://doi.org/10.1007/s10055-016-0285-9
Saredakis, D., Szpak, A., Birckhead, B., Keage, H.A.D.,
Rizzo, A.; Loetscher, T. (2020). Factors Associated
with Virtual Reality Sickness in Head-Mounted
Displays: A Systematic Review and Meta-Analysis.
Front. Hum. Neurosci. 14:96. doi: 10.3389/
fnhum.2020.00096
Sevinc, V.; Berkman, M.I. (2020): Psychometric evaluation
of Simulator Sickness Questionnaire and its variants as
a measure of cybersickness in consumer virtual
environments [online]. Applied ergonomics, 82,
102958. Applied ergonomics. doi:10.1016/j.apergo.
2019.102958
Stanney, K.M.; Kennedy, R.S.; Drexler, J.M. (1997):
Cybersickness is Not Simulator Sickness. Proceedings
of the Human Factors and Ergonomics Society Annual
Meeting, 41(2):1138–1142. doi: 10.1177/10711813
9704100292
Witkin, A. H., Lewis, H. B., Hertzman, M., Machover, K.,
Bretnall, P., & Wapner, S. (1954). Personality through
perception: an experimental and clinical study (Vol.
XXVI). Oxford, England: Harper.
Yildirim, C. (2020): Don’t make me sick: investigating the
incidence of cybersickness in commercial virtual reality
headsets. Virtual Reality 24, 231–239. https://
doi.org/10.1007/s10055-019-00401-0
Zupanic, M. (1993): Aspekte der Prädiktion und
Prophylaxe der Simulatorkrankheit. Diplomarbeit an
den Fachbereichen Psychologie und Sicherheitstechnik
der Universität Wuppertal, 5/93.
Look at the Horizon: Evaluation of a Software Solution Against Cyber Sickness in Virtual Reality Applications
21
