
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
Tri Huynh, Selin Erdem, Felix Eckert and Florian Matthes
School of Computation, Information and Technology, Technical University of Munich, Munich, Germany
Keywords:
Domain-Specific Language, Domain-Specific Modeling Language, Clinical Pathway Modeling, Adaptive
Case Management, Decision Support Tool.
Abstract:
e-Health systems leverage clinical pathways (CPs) models as standardized and optimized procedures to exe-
cute and manage medical treatments. To model CPs in decision support e-Health systems, our study devel-
ops Acadela, a low-tech-oriented, text-based Domain Specific Language (DSL) with visualization capability.
Acadela declares grammar to enforce textual syntax for modeling workflow, control flow, responsibility, med-
ical data visualization, and communications with external systems. Furthermore, Acadela provides a model
visualization to preview the CP and assist communication between medical and technical experts. To explore
the DSL’s expressiveness and usability, we conducted two separate descriptive user studies with six medical
professionals and eight technical adepts. First, we modeled five CPs used by medical professionals in their
daily routines. Through semi-structured interviews, we collected feedback regarding the language’s expres-
siveness. Next, we invited the technical adepts to model a hypertension CP and debug a faulty model written in
Acadela. Overall, the medical experts consider the modeled CPs accurately reflect their treatment procedure;
and the technical adepts consider the language easy to use and applicable to model CPs. The results imply
the DSL’s potential to model CPs with various degrees of complexity in different medical fields while being
user-friendly to modelers.
1 INTRODUCTION
E-Health applications are systems that apply a com-
bination of electronic communication and informa-
tion technology to transmit, store and retrieve digi-
tal data electronically for educational, clinical, or ad-
ministrative purposes in the healthcare sector, both lo-
cally and remotely (Mitchell, 1999). Operating treat-
ment processes for patients in e-Health applications
requires modeling clinical pathways (CPs). In sum-
mary, CPs are patient-care management plans that de-
fine care goals with the process and timing necessary
to achieve such goals with optimal efficiency (Panella
et al., 2003; Campbell et al., 1998; Every et al., 2000).
Applying CPs results in numerous benefits, from im-
proving patient conditions (Panella et al., 2008), re-
ducing complications (Preston et al., 2013), mortality
(Hai et al., 2019), length of stay, and costs (Yang and
Su, 2014). State-of-the-art solutions propose graphi-
cal or textual Domain Specific Languages (DSLs) to
model CPs and leverage their benefits in e-Health sys-
tems. However, each approach has distinct advan-
tages and limitations.
On the one hand, graphical DSLs enable model-
ers to build medical procedures by interacting with
visual elements. The advantages of this approach
are a user-friendly interface and learnable mechanism
(Hermans et al., 2009, p. 433), as the applications
display workflow elements following a logical and
hierarchical structure (Wienands and Golm, 2009, p.
458). Furthermore, visual artifacts foster communica-
tion among technical and domain experts (Heß et al.,
2015, p. 13), as they share a common understand-
ing of notations for CP elements. However, existing
workflow modeling languages, like BPMN, lack the
notation to express aspects besides workflow execu-
tion, thus demanding extra effort to develop custom
extensions for modeling and visualizing these aspects
(Heß et al., 2015, p. 4), (Braun et al., 2014, p. 10).
On the other hand, textual DSLs model CPs us-
ing a text-based interface and grammars (Cook et al.,
2007, pp. 15-17) or meta-models (Jouault et al.,
2006, p. 2). The textual model representation com-
bined with an IDE brings several benefits. First, ex-
tending the model is convenient by textually defin-
ing sub-DSLs of new domain concepts (Rieger et al.,
2018). Second, validating models is manageable as
textual DSLs only define constraints via grammar
(Baar, 2015). Third, an IDE offers convenient support
46
Huynh, T., Erdem, S., Eckert, F. and Matthes, F.
Acadela: A Domain-Specific Language for Modeling Clinical Pathways.
DOI: 10.5220/0012076500003538
In Proceedings of the 18th International Conference on Software Technologies (ICSOFT 2023), pages 46-58
ISBN: 978-989-758-665-1; ISSN: 2184-2833
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

with error warning, syntax highlighting, and auto-
completion of CP elements and their values (Cook
et al., 2007, pp. 13-14), (Merkle, 2010). How-
ever, textual DSLs typically offer no CP visualiza-
tion, which is essential to present a comprehensive
overview using graphical notations (Frank, 2013, p.
134) familiar to both domain and technical experts,
thus fostering communication and workflow analysis
to increase the quality of the treatment.
Furthermore, from literature research, existing
DSLs for CPs do not support the modeling of coor-
dination with external systems or customizing the vi-
sual representation of medical data. External com-
munication is vital to obtain decision-support data
(e.g., adverse drug-drug interaction effects (Thakrar
et al., 2007)), orchestrate and integrate with existing
(legacy) systems (White, 2009, p. 11) (Kurz et al.,
2015, p. 4) (Iroju et al., 2013, pp. 265-268), as they
require necessary data (e.g., user information, medi-
cal status) from these systems to execute healthcare
services for each patient case. Meanwhile, customiz-
ing data representation provides flexibility in display-
ing medical data (e.g., as a graph, image, or decorated
text (Michel, 2020, p. 36)) to express the patient’s
condition comprehensively and vividly. An under-
standable visualization is prominent in medical treat-
ment as they provide healthcare professionals with an
overarching and insightful overview of medical states
to ease decision-making, particularly in complicated
scenarios (Suganthi and Poongodi, 2021).
In addition to the technical functionality, a DSL
should be user-friendly to modelers. Therefore, we
also explore user-friendliness and learnability from
the modeler’s viewpoint in our study.
To address the missing essential CP concepts and
study the usability of our solution, we develop a
generic, textual DSL named Acadela for CP mod-
eling. Besides declaring essential CP elements,
Acadela can 1) define when and how to send HTTP
requests to external systems, 2) customize the graphi-
cal representation of medical data in the e-Health ap-
plication, and 3) visualize the modeled CP using ba-
sic shapes and color code. Our goal is to integrate
Acadela into e-Health applications without drastically
modifying the system while increasing the usability
and productivity of the CP modeling process.
The remainder of our paper consists of seven sec-
tions. First, we explained the research methodology
applied in our study. The next section presents the re-
lated work of existing DSLs that identify the required
concepts and features for modeling CPs discussed in
the fourth section. The fifth section showcases con-
crete syntax to model the identified CP concepts in
our DSL. The sixth and seventh sections report our
descriptive user studies regarding the expressiveness
and usability of the DSL, respectively. The final sec-
tion concludes our study and proposes future work.
2 METHODOLOGY
To envision the development and evaluation of our
DSL, we formulate three research questions focusing
on 1) the concrete syntax, 2) expressiveness, and 3)
usability as follows:
RQ1: How can a textual DSL model executable CPs
that supports external communication, customizable
graphical representation of medical data, and visual-
ization of CP models?
RQ2: Can the DSL model CPs from different medi-
cal fields with diverse complexity while being under-
standable to clinical experts?
RQ3: Do the modelers regard the DSL and the devel-
opment environment as user-friendly and learnable
for modeling CPs?
We answer RQ1 by identifying essential concepts
for modeling CP from literature research. Addi-
tionally, we selected the Smart Adaptive Case Man-
agement (SACM) (Michel, 2020), the engine of the
CONNECARE platform for integrated care that lever-
ages CP as a decision support tool for operating
treatments of chronic diseases (Vargiu et al., 2017).
SACM defines CPs using a custom XML structure,
thus we analyze the current XML syntax and SACM
capabilities to devise approaches for optimizing the
CP declaration with a DSL.
To model the CP concepts, we applied guidelines
and best practices of DSL design (Karsai et al., 2014,
pp. 3-5) to develop the Acadela syntax. First, our
DSL shall include only the necessary domain con-
cepts to model the identified CP requirements. Our
study develops a textual DSL because we aim to cre-
ate a lightweight, extensible DSL that is platform-
independent, i.e., the DSL can generate a CP model in
different formats (e.g., XML, UML) to be compatible
with various e-Health systems. To realize this goal,
we define the Acadela grammar using the textX meta-
language (Dejanovi
´
c et al., 2017). The textX gram-
mar parses the input CP model and generates the cor-
responding abstract syntax tree (AST). An Acadela
Interpreter processes the AST to construct a CP meta-
model object, and then translates the CP meta-model
into a SACM-compatible format, as shown in Fig-
ure 1. SACM creates CP models that execute patient
treatments at runtime from their meta-models.
Regarding usability, our DSL aims to provide low-
technical syntax, concise constructs, and flexible syn-
tactic rules extracted from popular programming lan-
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
47

Figure 1: The process to generate an SACM CP meta-model from a CP definition code written in Acadela.
guages (e.g., no semicolon to end a statement, indent-
and case-insensitive like in SQL). We select these fea-
tures with the expectation that modelers with basic
programming knowledge can quickly learn and apply
our DSL’s modeling concepts. Afterward, we follow
the guidelines of design science from Hevner et al.
(2004, p. 80) to begin the iterative design, develop-
ment, and refinement cycle of our DSL.
Considering Acadela’s expressiveness, RQ2
states the potential of modeling CPs with different
complexity applied in various medical departments.
Following this direction, we contacted six medical
experts and collected five CPs from their fields of ex-
pertise. We modeled the CPs in Acadela, which then
generates CPs in a format compatible with SACM.
We demonstrated the execution of CP models to
medical professionals in SACM to assess the DSL’s
accuracy and applicability from their perspective.
Finally, RQ3 explores the DSL’s usability from
the perspective of modelers. Thus, we conducted de-
scriptive user studies with technical staff in the health-
care sector or medical researchers with programming
or modeling experience. The participants developed
a hypertension CP using our Acadela IDE and gave
us quantitative and qualitative feedback on the DSL’s
user-friendliness, learnability, and applicability.
3 RELATED WORK
Graphical DSLs. Several DSLs are developed to
model CPs supporting evidence-based decisions in
clinical treatments. The motivation is that standard
business process modeling notations, like BPMN, do
not fully support modeling clinical procedures that
require discretionary execution paths to handle un-
predictable events. In this direction, Burwitz et al.
(2013) developed CP-Mod to support Evidence-based
Medicine (EBM) with the modeling of 1) decision
support, i.e., the recommended actions based on deci-
sion criteria, along with references to medical guide-
line documents; 2) Treatment alternatives and prob-
ability to indicate possible care approaches; 3) time
event representing time slots, waiting period or tem-
poral dependencies between activities.
Similarly, Braun et al. (2014) and Neumann et al.
(2016, 2017) extended BPMN to develop BPMN4CP
and BPMN
SIX
. Both DSLs first construct a domain
ontology through 1) requirement analysis and 2) do-
main analysis to examine whether a modeling lan-
guage is appropriate to model the concepts, proper-
ties, and constraints of the domain. Next, they per-
form an equivalence check to assess which model-
ing concepts are constructible with default BPMN
elements and to which extent. After that, the au-
thors classify whether a domain concept is mode-
lable by combining multiple BPMN elements (Equiv-
alence by Composition) or using BPMN elements and
domain-specific attributes (Equivalence by Specifica-
tion). The authors then apply a BPMN extension
procedure of Stroppi et al. (2011) to develop a do-
main class model (CDME) to extend concepts not
modelable by standard BPMN elements. The CDME
model is an abstract syntax that is derivable to con-
struct the concrete syntax (graphical notations) in a
BPMN extension model format (BPMN+X). As a re-
sult, BPMN4CP and BPMN
SIX
create an extended
BPMN model for CPs that includes quality indicators
and management of human, equipment, consumables,
and document resources concepts.
Textual DSL. Msosa (2018, 2019) developed
FCIG, a textual DSL to model Clinical Practice
Guidelines (CPGs) in Computer-Interpretable Guide-
lines (CIGs) forms. First, Msosa analyzed the domain
concepts of a CIG Guideline, which comprises a set
of Recommendations containing Actions and Condi-
tions to specify which medical interventions apply to
particular circumstances. Next, Msosa leveraged the
Xtext (Eclipse Foundation, nda) DSL build tool to de-
fine FCIG grammar. When processing a Guideline,
FCIG navigates through the AST to 1) retrieve all
Recommendations in the Guideline, 2) for each Rec-
ommendation, return the list of Actions that satisfy the
ICSOFT 2023 - 18th International Conference on Software Technologies
48
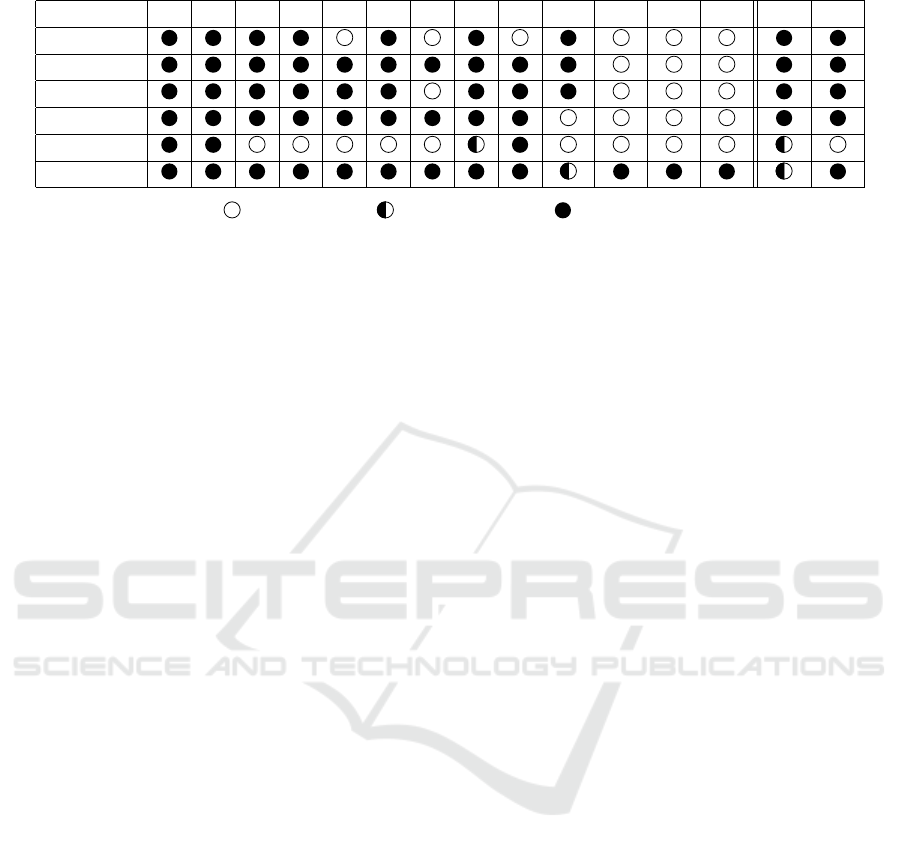
Table 1: Features Comparison of DSLs for CP modeling.
F1 F2 F3 F4 F5 F6 F7 F8 F9 F10 F11 F12 F13 SF1 SF2
CP-Mod
DSML4CPs
BPMN4CP
BPMN
SIX
FCIG
Acadela
No Support Partial Support Full Support
Condition, and 3) generate a function that evaluates
all Guideline’s Recommendations and returns appli-
cable Actions. The advantages of FCIG are 1) concise
syntax and 2) offering an IDE with syntax highlight-
ing and auto-completion to support modeling.
While existing DSLs model key aspects of CP op-
eration, they do not mention the support of external
systems communication, dynamic graphical render-
ing, and importing CP elements. Our study discusses
the necessity of the features, coded F11, F12, and F13
in Section 4, and our modeling solutions in Section 5.
4 CP MODELING FEATURES
From the literature study of existing DSLs, e-Health
systems, and CP definition and execution, we col-
lected the requirements for modeling executable CPs
in e-Health applications. Furthermore, we also collect
features for textual DSLs to support technical staff in
constructing CP models. Table 1 summarizes the im-
plementation of identified CP modeling (F#) and sup-
porting features (SF#) in DSLs from relevant litera-
ture and Acadela.
F1: The DSL shall model medical processes us-
ing concepts from the healthcare domains familiar to
healthcare professionals. Rationale: First, construct-
ing activities and phases of medical procedures is es-
sential to declare structured or alternative tasks in the
treatment. Second, concepts used in the DSL should
map to the terminology which prospective users are
familiar with (Frank, 2013, p. 136).
F2: The DSL shall model alternative treatment pro-
cesses, their triggering conditions, and potential val-
ues that trigger other alternatives. Rationale: Care
professionals frequently handle unpredictable scenar-
ios during the planned treatment process. Thus, a
DSL shall provide decision support to care profes-
sionals, patients, and their relatives (De Bleser et al.,
2006, p. 562).
F3: The DSL shall model evidence classes with data
assigned to them. Additionally, the DSL shall support
referencing the evidence. Rationale: CP processes
and decisions following EBM principles (Wang et al.
(2011, 2021)) shall be supplemented with informa-
tion on the evidence to decide the appropriate inter-
ventions.
F4: The DSL shall model iterative treatment pro-
cesses. Parallel repetition should also be supported.
Rationale: CPs shall support control flow by exe-
cuting both optimal, sequential procedures and repet-
itive, unpredictable processes. Parallel execution is
necessary to construct simultaneous tests (e.g. paral-
lel PCR tests (Berdal et al., 2008), (Perchetti et al.,
2020, p. 2)).
F5: The DSL shall model each medical process’s
treatment goal(s) based on medical practices and pref-
erences of individual patients. Rationale: Express-
ing care goals based on the applied remedies and the
patient’s preferences fosters treatment transparency
(Heß et al., 2015, p. 6). Furthermore, this feature en-
courages medical professional teams to establish uni-
fied remedies to achieve the care goal(s).
F6: The DSL shall support assigning responsibili-
ties to medical processes. The responsibilities distin-
guish between staff that executes medical tasks and
staff responsible for the treatment outcome. Ratio-
nale: Specifying the responsibilities of each health-
care professional optimizes the sequencing of medi-
cal procedures, indicates contact persons, and fosters
communication among staff (Heß et al., 2015, p. 6).
F7: The DSL should model checklists associated with
medical processes. Rationale: Checklists are widely
accepted and helpful instruments to present details
about the execution of medical processes (Healey
et al., 2011, p. 3) (Wolff et al., 2004, pp. 430-431).
F8: The DSL should model various aspects and infor-
mation needs of stakeholders in medical institutions.
Rationale: CPs aim to optimize medical care from
various perspectives. Therefore, a DSL should pro-
vide concepts to model treatment-related information,
such as (multidisciplinary) medical or organizational
aspects (Heß et al., 2015, p. 6). Besides, the DSL
should include medical guidelines to assist care pro-
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
49

fessionals to decide on appropriate interventions.
F9: The DSL should model the allocation of re-
sources to the medical process. Rationale: CPs also
aims to manage and optimize resource consumption
(Heß et al., 2015, p. 6). Resources comprise equip-
ment or documents used during the medical process
(Neumann et al., 2016, p. 4), medicine, and facilities
(Braun et al., 2016, p. 3252).
F10: The DSL should model time constraints and ex-
plicit time events. Rationale: the definition of CP in-
corporates the timing necessary to achieve care goals
(De Bleser et al., 2006), (Campbell et al., 1998), (Van-
haecht et al., 2006). Therefore, a DSL should provide
features to declare due dates or timed activities such
as periodic or time-lapsed tasks.
F11: The DSL should model external requests to or-
chestrate and integrate with existing or external sys-
tems (Michel, 2020, p. 37). Rationale: e-Health ser-
vices may need to interact with legacy systems that
store user data. Furthermore, delivering care services
may require sharing data with partner systems at dif-
ferent process lifecycles (e.g., activated, terminated).
For example, sending blood pressure data to a moni-
toring application when completing the measurement.
F12: The DSL should support customizing the graph-
ical representation of activity. Rationale: Customiz-
able UI display enhances extendability and supports
the modeling of specialized clinical use cases be-
cause modelers can define dynamic visual representa-
tions of data without relying on predefined templates
(Michel and Matthes, 2018). Besides, a comprehen-
sive overview of medical status influences the anal-
ysis of the patient’s condition and decision-making
process of medical experts (Suganthi and Poongodi,
2021), which affects the treatment quality. Thus, a
DSL shall assist modelers in designing comprehen-
sive graphical representations of data.
F13: The DSL should support importing CP elements
into the current CP definition. Rationale: Repeatedly
declaring common procedures (e.g., patient admis-
sion) in each CP results in duplication and cumber-
some modification for all affected CPs when the tasks
change. Therefore, defining these shared elements
once and importing them into CPs foster reusability
and flexibility of the modeling process.
SF1: The DSL should offer an IDE. For textual DSLs,
the IDE should have syntax highlighting and auto-
completion capabilities. Rationale: The combination
of auto-completion, syntax highlighting, and syntax
checking can enhance productivity when defining CP
elements, increase usability (Cook et al., 2007, p. 16-
17) (Merkle, 2010), and prevent typos.
SF2: The DSL should visualize the modeled CP
to demonstrate the reconstructed elements, such as
phases, activities and their inputs or outputs, responsi-
bilities, and control flows, using basic graphical nota-
tions. Rationale: A CP visualization provides visual
clues that can enhance the understandability and read-
ability of the models (Frank, 2010, p. 1). Another
benefit is reducing the learning effort as the clinical
experts do not have to understand modeling concepts
in-depth (e.g., (Hermans et al., 2009, p. 433)). Addi-
tionally, one noticeable feedback from our interviews
with technical staff is that Acadela needs a graphical
visualization to provide an overarching overview of
the CP model. These visual clues assist the debug-
ging and analysis of the model.
Observation: Existing DSLs satisfy the F1 feature
by providing essential constructs to model generic CP
process elements, e.g., Activities (Braun et al., 2016,
p. 3252), ProcessDefinition (Michel, 2020, p. 45).
In addition, the DSLs include concepts representing
decision criteria with conditional expression for acti-
vating alternative treatment paths (e.g., DecisionCri-
terion (Braun et al., 2014; Burwitz et al., 2013), Cri-
terion (Heß et al., 2015, p. 10), and SentryDefinition
(Michel, 2020, pp. 45, 47)), thus supporting F2.
Most DSLs support features F3, F4-F6, and F8.
We considered FCIG to fulfill F8 partly because the
DSL can use the Action concept to open a medical
document at a particular URL. However, FCIG does
not offer constructs to model organizational aspects
(e.g., medical departments or teams). Most DSLs sup-
port modeling evidence classes and repetitive activ-
ities (F3 and F4). Furthermore, existing DSLs can
model resource management aspects in CP operations
(F6 and F8). Most DSLs can express treatment goals
(F5), thus assisting care professionals in communicat-
ing and planning their therapies. Not all DSLs support
features F7 and F10 because of the original scope of
their CP application context.
Regarding the supporting features SF1 and SF2,
graphical DSLs offer an expressive IDE with ex-
tended concepts to help modelers construct CPs by
interacting with graphical elements. FCIG, as a tex-
tual DSL, also develops an IDE with syntax highlight-
ing, yet it does not auto-complete keywords or visu-
alizing CIG models. Acadela auto-completion covers
keywords but not element IDs in a CP meta-model.
The F11, F12, and F13 features are the novel
contributions of Acadela, which aim to support inter-
system communications and provide flexible model-
ing capabilities to modelers. Existing DSLs did not
discuss the three requirements, yet they are essential
in modeling CPs in integrated, adaptive e-Health plat-
forms as explained in the Rationale.
The following section presents our methods to
ICSOFT 2023 - 18th International Conference on Software Technologies
50

model CP that support the 15 identified features.
5 CP METAMODEL DEFINITION
In SACM, medical experts and modelers need to col-
laborate to define Stages and Tasks in the care pro-
cess, control flow, responsibilities, and communica-
tion to external systems in a CP. The first three ele-
ments are foundational building blocks for develop-
ing standardized and multidisciplinary CPs. This sec-
tion presents the Acadela grammar to enforce syntac-
tic rules of CP declaration, followed by the CP mod-
eling concepts and their concrete syntax in Acadela to
address the CP modeling requirements.
5.1 Grammar
Acadela arranges CP elements in a subsumption order
to provide a hierarchical structure of CP models. For
example, a Case object contains multiple Stages and
each Stage consists of Tasks. Each CP element has
user-defined attributes following the key=value pat-
tern. In addition, Acadela expresses attributes accept-
ing only SACM-defined values as directives, which
conforms to the #<attributeValue> pattern. The be-
low code expresses the semantics of Acadela gram-
mar in Extended Backus Naur Form (EBNF). To con-
dense the grammar, attributes, and directives of a
CP element are declared as <CpElement>Attrs or
<CpElement>Drts, respectively.
In EBNF, the # sign denotes the order of rules
within a group is interchangeable. The * sign means
a CP element has zero or more instances, while the +
sign allows one or more instances. The ? mark repre-
sents an optional element.
Sta rt = ( Im port *) ? ( Wo r k sp ac e | O b j )
Wo rk sp ac e = " Wor ks pa ce " ID
" d ef in e " C ase
Obj = Ca se | C a s eS et t i n g | Sta ge
| T ask | Form | A t tr i bu t e V al u e
| Ou t p u tF ie l d | I n p ut Fi el d | Ho oks
Hook = H tt pH oo k | Ca se Ho ok
| Du a lT as k Ho ok
Case = " Cas e " ID ( Cas eA t t r s C a s eS et t i n g
Re s p o n s i bi l it i es ( Ca se Ho ok +) ?
Su mm a r y Pa n e l S tag e +) #
Re s p o n s i bi l it i es = ( G rou p * U ser *) #
Ca se S e t ti ng = ( Ca se Ow ne r C as e P a ti en t
Ca s e S e t t in g At t rs ) #
Sta g e = " S ta g e " ID W or kf l ow Dr t s
St ag eA t t r s
( Ht tp Ho ok * Pr e co nd i ti on * Task +) #
Task = H um an Ta sk | Du al Ta sk
| Au t om a t e dT a sk
Hu ma nT as k = " Hum an Ta sk " ID W o rk f l o wD r t s
( Ta s k A tt rs Pr ec o nd it i o n *) #
( Ht tp Ho ok * F orm )#
Form = " For m " ID ( For mD rt s )? Fie ld +
Fie l d = I n p ut Fi el d * O u tp ut F i e ld *
In pu tF i e l d = " Inp ut Fi el d " ID
In p u t Fi e ld D r t s
In p u t Fi e ld A tt r s
Ou tp u t F ie ld = " Ou t pu tF i e l d " ID
Ou t p u tF i el d Dr t s
Ou t p u t F i el d At t rs
Ou t p u tF i el d Dr t s = ( Man da to ry R e a d o n l y )#
Ma nd at or y = "#" " ma nd at or y "
| " no t Ma n d a to r y "
Ou t p u t F i el d At t rs = ( De s cr ip t io n
Ex pr es s i o n ...) #
De sc r i p ti on = " l abe l " "=" ST RI NG
Regarding Tasks, since the syntax of HumanTask,
DualTask, and AutomatedTask are similar, the gram-
mar only expresses HumanTask. Similarly, Output-
FieldDrts and OutputFieldAttrs characterize the syn-
tax of directives and attributes of other CP elements.
5.2 Modeling CP Elements
Care Process (F1, F3, F4, F7, F12). In SACM, a
Workspace represents the medical institution provid-
ing healthcare services, and a Case is the CP for treat-
ing a particular disease. Acadela expresses treatment
phases and activities in a CP using Stages and Tasks
(F1). Since clinical processes are multi-stage proce-
dures, they can comprise distinct and possibly repet-
itive phases. SACM supports a parallelly repeated
Stage (Michel, 2020, pp. 80, 105), which Acadela
expresses as a #parallelRepeat directive (F4). Each
Stage comprises Tasks of type: human, automated,
or dual tasks, which are, respectively, conducted by
a person, third-party system, or both consecutively.
Listing 1 shows the Acadela syntax to declare a re-
peated Stage and a HumanTask to measure the Body
Mass Index (BMI) value. Figure 2 displays the result-
ing UI of Listing 1.
Sta g e E va lu at i o n #r ep e at Se r ia l
lab e l = ’ Eva lu at io n ’
Hu ma nT as k M ea su r e B mi
lab e l = ’ Me as ur e B MI ’
du eD at e R e f = ’ Se tt in g . Du eD at e ’
Form B mi Fo r m
In pu tF i e l d He igh t # nu mbe r (0 -3)
lab e l = ’ He ig h t ( m ): ’
In pu tF i e l d We igh t # nu mbe r (0 -300)
lab e l = ’ We ig h t ( kg ) : ’
Ou tp u t F ie ld Bm iS co re #n u mb er
lab e l = ’ BMI Sc ore : ’
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
51

ex pr es s i o n =
’ We ig ht / ( He ig ht * H e ig ht ) ’
uiR e f = ’ co lo r s (0 < ye ll o w < 18.5
< gr een < 25 < red < 10 0) ’
Listing 1: Sample definition of a BMI Measurement Task
in an Evaluation Stage.
Figure 2: The UI output from the Stage Declaration in List-
ing 1. The Figure shows the activated Evaluation Stage and
enabled MeasureBMI Task (left), and the UI of the Task
(right).
Each Task has a Form containing InputFields to
accept medical data to collect necessary medical con-
ditions for an evidence class, diagnosis, or documen-
tation (F1, F3). The medical information supports
care experts in determining the appropriate interven-
tions in EBM. Besides, Acadela represents a checklist
(F7) by defining multiple-choice InputFields that ac-
cept multiple answers. Additionally, the OutputFields
can visualize the input data in the SACM UI (F12).
Control Flow (F2): Medical experts execute alter-
native actions depending on the patient condition.
Therefore, CPs shall support conditional activation of
Stages or Tasks depending on specific medical data.
Listing 2 demonstrates the syntax of defining transi-
tion conditions using the Precondition construct in-
side a Stage. The previousStep attribute states the pre-
requisite Stage or Task, while the condition attribute
is a boolean expression for activating the Stage.
Sta g e E va lu at i o n #r ep e at Se r ia l
... // S t age At tr ib ut e s
Pr ec o n d it i o n
pr ev i o u sS t e p = ’ I d en t if i c a ti o n ’
co nd it io n = ’ Id e n ti f ic a t i on .
Fi l l C on s en t Fo r m . Con s en t = 1 ’
Listing 2: Defining a transition condition of a Stage. Here
the Evaluation Stage is activated if the Identification Stage
is completed and the patient consents with the treatment.
CP Summary Panel (F5): Listing 3 demonstrates
a SummaryPanel code displaying the treatment goal
from an InputField. This element displays the value
from an InputField or OutputField in the Case Sum-
mary page. InputFields can record the care goal while
Su mm a r y Pa n e l
Se c ti on Ta rg et Bm i # left
lab e l = " Ta rg e t BMI : "
In fo P a t h I d en t if i c a ti o n .
Se t T r e a t me n tG o al . Tar ge tB mi
Listing 3: SummaryPanel Definition to show the care goal.
Acadela traces the InputFields from the InfoPath attribute
by parsing the <StageId>.<TaskId>.<FieldId> pattern.
the OutputFields values indicate the progress or con-
straints to achieve the goal.
Responsibilities (F6). SACM supports referenc-
ing individual experts or professional groups in the
database and grants them access rights for operating
Stages or Tasks (F6), as shown in Listing 4. Model-
ers can optionally assign the unique ID of a Group or
User to the staticId attribute.
Re s p o n s i bi l it i es
Gro u p S tP a u l Nu r s e s name = ’ N u rs es ’
st at i c I d = ’ ef d c 39 5 2 e s7 5 ’
Se t ti ng
At tr ib ut e Nu rs es
#Link .#Us ers ( St P au l N u rs e s )
lab e l = ’ Nu rs e s ’
...
Sta g e E va lu at i o n
own e r = ’ Se tt in g . Nu rse s ’
Listing 4: SummaryPanel Definition to show the care goal.
Document (F8). In case medical documents (e.g.,
guidelines, forms) necessary to provide care services
(Heß et al., 2015; Braun et al., 2014) are accessible via
URLs, modelers can declare a link to each document,
as shown in Listing 5.
In pu tF i e l d M ed i ca l Gu i de l i n e
#d oc u m e nt L i n k (’ ht tps :// s tp a ul . de /
fi le p a t h ’)
lab e l =" L ink to Me di ca l Gu i d e l i ne :"
Listing 5: Defining a link to a document in Acadela.
Due Date Definition (F10). SACM supports defin-
ing a default due date from the current time in the
Case Setting. The due date is assignable to a Human-
Task or a DualTask, as shown in Line 6 of Listing 1.
External System Communication (F11). SACM
updates medical status in external systems by sending
HTTP requests (HttpHook) with Case, Stage, or Task
data when an event (e.g., activated, completed) oc-
curs in these elements (Michel, 2020, p. 113). Listing
6 defines a HttpHook inside the MeasureBMI Task.
Upon the Task completion, the HttpHook sends the
ICSOFT 2023 - 18th International Conference on Software Technologies
52
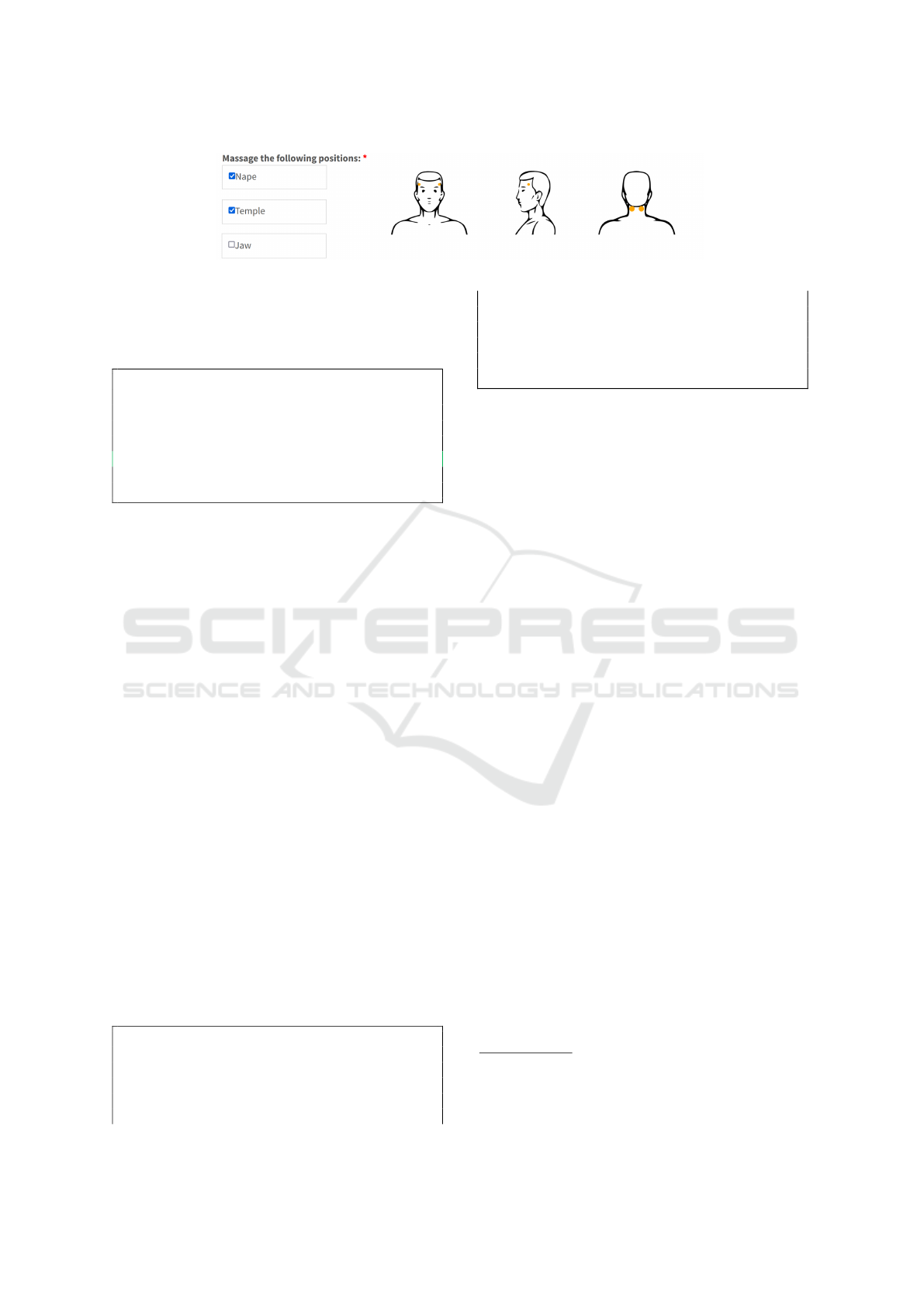
Figure 3: Illustration of selected massage positions in an InputField (left) affect the output image visualization (right).
Task data from its InputFields and OutputFields to
the external system URL using the POST method. If
the request fails, SACM shows the value of the fail-
ureMessage attribute to the user.
Hu ma nT as k M ea su r e B mi
lab e l = ’ Me as ur e B MI ’
... // O t her T a sk ’s el em en ts
Tr i gg er
On c om pl et e in v ok e ’ ht t ps ://
pa rt n er s y s te m . de / up da te ’
met ho d P OST wit h fa i lu re M es s ag e
" C an no t upd at e i nfo !"
Listing 6: Defining an external request triggered upon a
Task completion
Customizable Graphical Representation (F12).
The SACM UI of a Task is a grid layout of three
columns. Acadela specifies the column position of an
InputField or OutputField using a directive, e.g., #left,
#center, #right (F12). Besides, SACM supports ap-
plying color to a range of numeric values. Line 17 in
Listing 1 shows how Acadela defines the green color
of the BMI OutputField for a value from 18.5 to 24.9.
To render a customizable UI Template, an Out-
putField contains 1) a SVG image comprising graph-
ical elements to visualize medical data, 2) the CSS
style declaring the UI effect applied to the elements
(e.g., hide, show, fore- or background color), and 3)
a SACM command to dynamically modify the CSS
style based on InputField(s) value. Figure 3 shows an
example of displaying massage positions on a human
head based on the selected areas.
Import CP Element (F13). Acadela leverages the
textX scope provider to import CP elements defined
in a file into the current CP. textX supports FullyQual-
ifiedName (FQN) scope that expresses the location of
an imported object based on the file path and object
ID (Dejanovi
´
c, ndc). For instance, Listing 7 shows
how to import a Discharge Stage defined in the dis-
charge.aca file under the stage folder into a CP model.
// Fil e p a th : ./ st a ge / d is ch ar g e . ac a
def in e Sta g e D i s ch ar ge
... // S t age At tr ib ut e s
// - - - - - - -- - - - - -
imp or t sta ge s . di sc ha r g e
// im po rt s t ag es . d is ch ar g e as di
Wo rk sp ac e S tP a ul Cl i ni c
def in e C ase O T1 _ O b es it y
...
Sta g e E va lu at i o n ...
use S tag e Di s c h a r g e
// use St age di . Dis ch ar g e
Listing 7: Importing the Discharge Stage (lines 1-4) into
a CP. Lines 6 and 12 show how to import an element as
alias.
Web-Based IDE (SF1). To enhance the usability
and productivity of modelers, we developed a Web
IDE powered by Monaco
1
with 1) an auto-complete
feature to create CP elements from templates and 2)
syntax highlighting to help modelers identify CPs el-
ements.
CP Visualization (SF2). Acadela leverages GoJS
2
to develop a CP visualizer. GoJS provides functions
to graphically present CP elements. From the JSON
CP model generated by the backend, Acadela extracts
each CP element type and attribute to construct nodes
in the graph. Figure 4 shows the GoJS visualization
of a Hypertension CP used in our usability evaluation.
The Acadela Wiki
3
documents the DSL syntax for
defining CP elements.
6 EVALUATION
To explore the applicability of Acadela, we designed
two descriptive surveys to assess 1) expressiveness,
i.e., the ability to model CPs in different medical
fields, and 2) usability from the perspective of model-
ers. We recruited voluntary participants from staff
working in medical facilities or research institutions.
For each evaluation, we collected quantitative data by
a survey and applying a Likert scale from 1 (Strongly
Disagree) to 5 (Strongly Agree) for each statement.
We also interviewed participants to obtain feedback
regarding the DSL’s applicability and limitations.
1
https://microsoft.github.io/monaco-editor/
2
https://gojs.net/latest/
3
https://cobalt-plot-a08.notion.site/Acadela-Wiki-
ee58b3f2eb6a4627b55b470fe1717d9f
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
53
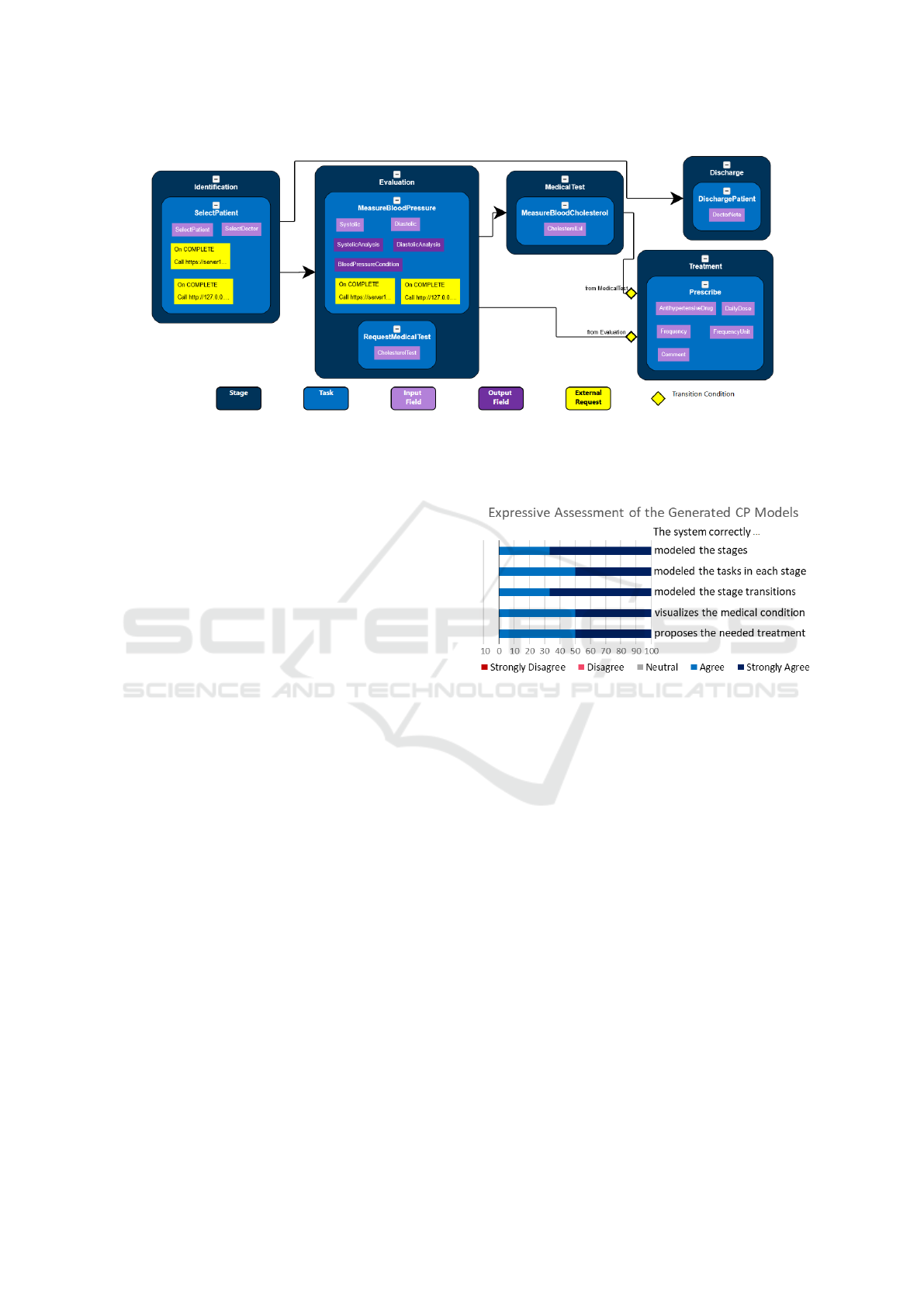
Figure 4: The visualization of the simplified Hypertension CP.
6.1 Expressiveness
Population Sampling: We contacted 16 medical
professionals in Germany and received six responses.
The response rate is moderate at 37.5 percent. The
age range of participants is from 20 to 60 years old.
Two medical professionals have more than 25 years
of experience, while others have up to five years.
Study Design: The six medical professionals
shared five CPs for treating Chronic Obstruction Pul-
monary Disease (COPD), Schizophrenia, Chronic
Headache, and two Diagnoses of Smoke Inhalation
Injury and Cervical Cancer. The CPs have various
complexity ranging from linear to dynamic, adaptive
treatment procedures. The complex CPs demonstrate
the language ability in modeling transition conditions
for unpredictable, personalized treatment processes.
The first three CPs are linear workflows, while the
other two support the decision-making with transi-
tion conditions applied to input medical data. The
last two CPs are complex due to their adaptive and
non-deterministic nature.
Experiment Environment: We host Acadela and
SACM in our computing devices and show them of-
fline or share the screen control via Zoom to avoid
being blocked by strict firewall policies in medical in-
stitutions. Due to the Corona pandemic, depending
on the participant’s preference, we presented the CP
model, collected the survey, and interviewed them on-
site or via Zoom.
Result: For each participant, we model their CP and
presented it in the SACM web application at their
workplace or via Zoom. After seeing the CP execu-
tion, we share the survey link with the participants and
ask for their opinions. Figure 5 shows the assessment
of medical experts on the accuracy of the modeled CP.
Figure 5: Medical professionals evaluation regarding the
accuracy of the modeled CPs.
The result suggests that the system constructs CPs
accurately with all participants agreed or strongly
agreed with each statement. In other words, Acadela
is potentially capable of reconstructing various medi-
cal procedures precisely, such that the SACM system
can correctly show and execute the treatment process
accordingly. Furthermore, in the subsequent inter-
view, the participants considered the modeled CPs as
correct. However, our Cervical Cancer Diagnosis CP
model does not correctly show the period before the
next test. Regarding the applicability, the participants
regarded the CP models as ”appropriate as a guide-
line”. Nevertheless, they should ”address treatment
variations” to be practically applicable. The evalua-
tion outcome implies a threat to internal validity, as
our study focuses on standard treatment processes but
did not substantially model potential alternative paths
in a CP. However, medical experts consider modeling
variations as a significant indicator of expressiveness.
When considering external validity, the limited
number of CPs and involved medical professionals in
our study suggests that Acadela may need additional
ICSOFT 2023 - 18th International Conference on Software Technologies
54
modeling concepts to express the medical terminol-
ogy and procedures in other treatments.
6.2 Usability
Population Sampling: We invited 21 technical
staff at medical or research institutions and recruited
eight participants from Germany, Spain, the Nether-
lands, and Italy. The response rate is moderate at 33.3
percent. Seven participants were 18 to 45 years old,
and one technical expert is over 46. Three partici-
pants have less than four years of experience, others
have more than eight years.
Study Design: All participants joined the experi-
ments online via Zoom. Each participant first at-
tended a training session, in which we introduced
how Acadela models CP elements and practiced
defining a CP together by completing an exercise.
Next, in a modeling session, the participants con-
structed elements of an incomplete hypertension CP
and fixed bugs of another CP model by examining
their error messages (EMs). We controlled the eval-
uation tasks and bugs such that all participants mod-
eled the same CP elements and debugged the same
syntax and semantic errors. Performing the same ac-
tivities builds a common baseline to gauge usability
and learnability.
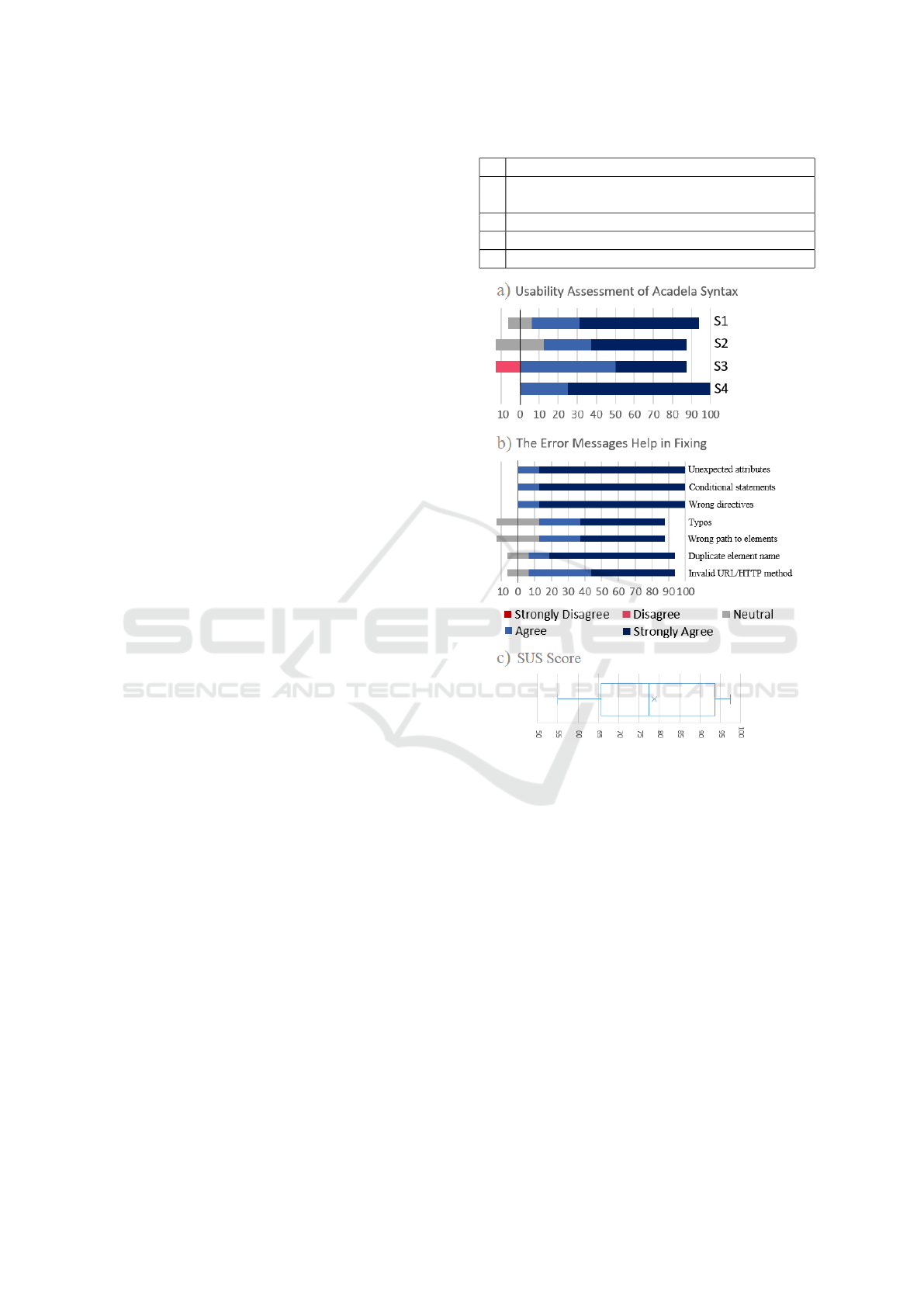
Result: After the debugging session, we asked the
experts to assess the usability of Acadela and its er-
ror validation. We presented a questionnaire with
statements regarding the a) User-friendliness of the
DSL, b) Helpfulness of EMs, and c) Overall usability
assessment using the System Usability Scale (SUS).
Figure 6 presents the evaluation outcome.
In the subsequent interview, overall, the partici-
pants comment on the syntax as ”simple”, ”elegant”,
and ”easy to learn” for users with competent program-
ming experience. In addition, EMs are considered
”useful” as they ”show the line number and the prob-
lem” to help users ”pinpoint the error”. Six out of
eight experts considered Acadela to have the poten-
tial to model CPs in e-Health applications.
Regarding limitations, the auto-complete feature
should ”show the names of elements in the code”,
which is convenient for the users and prevents typ-
ing a non-existing CP component. Furthermore, three
participants share an opinion that Acadela is ”fairly
easy to use”, but ”depend on the background and ed-
ucation” of modelers. Therefore, modelers need fun-
damental programming skills to model and debug the
Acadela code. One participant states that Acadela
ID Syntax Usability Statement
S1 The syntax for creating CP elements, i.e. Stage,
Task, Form, Field, is straightforward
S2 Editing CP elements is easy with the language
S3 Importing external modules is straightforward
S4 The language syntax was easy to learn and use
Figure 6: Usability quantitative evaluation result.
should model ”infographic”, ”videos”, and ”gamifi-
cation factors” to further support medical staff.
7 CONCLUSION
Our study develops Acadela, a textual DSL for mod-
eling CPs with visualization capability. Acadela sup-
ports the definition of workflow phases and activ-
ities, control flow, responsibilities, medical docu-
ment resources, timing constraints, communication to
external services, dynamic graphical representation
of data and the import of these elements to foster
reusability (RQ1). The language is overall consid-
ered user-friendly and learnable by professionals with
technical knowledge.
We leveraged the textX meta-language, guide-
lines of DSL design, and error messages to develop
the grammar, concrete syntax, and error validator of
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
55

Acadela. To evaluate our DSL expressiveness (RQ2),
we modeled five CPs and presented the executable
workflow in SACM, an e-Health platform for inte-
grated care, to six care professionals in five medical
fields. The result suggests that Acadela can accu-
rately model CP workflows in different medical de-
partments and complexity. However, both medical
professionals and technical staff wished to see more
modeling of visualization and variations in their CP.
To evaluate Acadela’s usability (RQ3), we invited
eight technical experts working in the healthcare in-
dustry or research to model a simplified CP for hyper-
tension treatment and fix bugs of another CP based on
their error messages (EMs). The result implies that
Acadela is potentially usable and learnable to tech-
nical staff. Most participants deem the syntax ”sim-
ple” and ”easy to learn”, while EMs help them lo-
cate, understand and fix errors. Therefore, they con-
sider the DSL applicable to model CPs in e-health ap-
plications. However, we reflected on the result that
Acadela is user-friendly for modelers with solid basic
programming knowledge or above. In addition, the
participants wished to see more capabilities, such as
the rendering of statistics. and auto-completion of CP
elements’ ID. Another concern is more participants
are needed to assess the DSL usability substantially.
Future Work. To further validate the applicability
of Acadela, one can expand the evaluation for mod-
eling CPs in more medical fields, such as Chinese
medicine or Orthopedics. Operating CPs in practi-
cal settings enable us to address the daily-life needs
and concerns of medical professionals while address-
ing the unique challenges of applying CPs in the med-
ical field. Furthermore, different medical treatments
require diverse forms of medical data visualization
and additional medical concepts, hence we can inves-
tigate the applicability and limitation of CP modeling
features provided by Acadela. This future practical
study is the first cornerstone for identifying potential
extensions or alternative solutions to assist medical
professionals in delivering quality care to patients.
ACKNOWLEDGEMENTS
We sincerely thank the medical professionals, re-
searchers, and technical staff for their time, support,
and patience in providing clinical pathways, conduct-
ing experiments, and valuable feedback to our study.
REFERENCES
Baar, T. (2015). Verification support for a state-transition-
dsl defined with Xtext. In International Andrei Er-
shov Memorial Conference on Perspectives of System
Informatics, pages 50–60. Springer.
Berdal, K. G., Bøydler, C., Tengs, T., and Holst-Jensen, A.
(2008). A statistical approach for evaluation of PCR
results to improve the practical limit of quantification
(LOQ) of GMO analyses (SIMQUANT). European
Food Research and Technology, 227(4):1149–1157.
Braun, R., Schlieter, H., Burwitz, M., and Esswein, W.
(2014). Bpmn4cp: Design and implementation of
a bpmn extension for clinical pathways. In 2014
IEEE international conference on bioinformatics and
biomedicine (BIBM), pages 9–16. IEEE.
Braun, R., Schlieter, H., Burwitz, M., and Esswein, W.
(2016). BPMN4CP Revised–Extending BPMN for
Multi-perspective Modeling of Clinical Pathways. In
2016 49th Hawaii International Conference on Sys-
tem Sciences (HICSS), pages 3249–3258. IEEE.
Burwitz, M., Schlieter, H., and Esswein, W. (2013). Mod-
eling clinical pathways-design and application of a
domain-specific modeling language.
Campbell, H., Hotchkiss, R., Bradshaw, N., and Porte-
ous, M. (1998). Integrated care pathways. Bmj,
316(7125):133–137.
Cook, S., Jones, G., Kent, S., and Wills, A. C. (2007).
Domain-specific development with visual studio dsl
tools. Pearson Education.
De Bleser, L., Depreitere, R., Waele, K. D., Vanhaecht, K.,
Vlayen, J., and Sermeus, W. (2006). Defining path-
ways. Journal of nursing management, 14(7):553–
563.
Dejanovi
´
c, I., Vaderna, R., Milosavljevi
´
c, G., and Vukovi
´
c,
ˇ
Z. (2017). TextX: a Python tool for domain-specific
languages implementation. Knowledge-based sys-
tems, 115:1–4.
Dejanovi
´
c, I. (n.d.c). Reference resolving expression lan-
guage (rrel). http://textx.github.io/textX/3.0/rrel/.
Eclipse Foundation (n.d.a). Language engineering for ev-
eryone! https://www.eclipse.org/Xtext/.
Every, N. R., Hochman, J., Becker, R., Kopecky, S., and
Cannon, C. P. (2000). Critical pathways: a review.
Circulation, 101(4):461–465.
Frank, U. (2010). Outline of a method for designing
domain-specific modelling languages. Technical re-
port, ICB-research report.
Frank, U. (2013). Domain-specific modeling languages: re-
quirements analysis and design guidelines. In Domain
engineering, pages 133–157. Springer.
Hai, J.-J., Wong, C.-K., Un, K.-C., Wong, K.-L., Zhang, Z.-
Y., Chan, P.-H., Lam, Y.-M., Chan, W.-S., Lam, C.-
C., Tam, C.-C., et al. (2019). Guideline-based critical
care pathway improves long-term clinical outcomes in
patients with acute coronary syndrome. Scientific Re-
ports, 9(1):1–9.
Healey, A. N., Nagpal, K., Moorthy, K., and Vincent, C. A.
(2011). Engineering the system of communication
ICSOFT 2023 - 18th International Conference on Software Technologies
56

for safer surgery. Cognition, Technology & Work,
13(1):1–10.
Hermans, F., Pinzger, M., and Deursen, A. v. (2009).
Domain-specific languages in practice: A user study
on the success factors. In International Conference on
Model Driven Engineering Languages and Systems,
pages 423–437. Springer.
Heß, M., Kaczmarek, M., Frank, U., Podleska, L., and
T
¨
ager, G. (2015). A domain-specific modelling lan-
guage for clinical pathways in the realm of multi-
perspective hospital modelling.
Hevner, A. R., March, S. T., Park, J., and Ram, S. (2004).
Design science in information systems research. MIS
quarterly, pages 75–105.
Iroju, O., Soriyan, A., Gambo, I., Olaleke, J., et al. (2013).
Interoperability in healthcare: benefits, challenges and
resolutions. International Journal of Innovation and
Applied Studies, 3(1):262–270.
Jouault, F., B
´
ezivin, J., and Kurtev, I. (2006). TCS: a DSL
for the specification of textual concrete syntaxes in
model engineering. In Proceedings of the 5th inter-
national conference on Generative programming and
component engineering, pages 249–254.
Karsai, G., Krahn, H., Pinkernell, C., Rumpe, B.,
Schindler, M., and V
¨
olkel, S. (2014). Design guide-
lines for domain specific languages. arXiv preprint
arXiv:1409.2378.
Kurz, M., Schmidt, W., Fleischmann, A., and Lederer, M.
(2015). Leveraging CMMN for ACM: examining the
applicability of a new OMG standard for adaptive case
management. In Proceedings of the 7th international
conference on subject-oriented business process man-
agement, pages 1–9.
Merkle, B. (2010). Textual modeling tools: Overview
and comparison of language workbenches. In
Proceedings of the ACM International Confer-
ence Companion on Object Oriented Program-
ming Systems Languages and Applications Com-
panion, OOPSLA ’10, page 139–148, New York,
NY, USA. Association for Computing Machinery.
https://doi.org/10.1145/1869542.1869564.
Michel, F. (2020). A Collaborative Purely Meta-Model-
Based Adaptive Case Management Approach for Inte-
grated Care. Dissertation, Technical University Mu-
nich, Munich.
Michel, F. and Matthes, F. (2018). A holistic model-based
adaptive case management approach for healthcare. In
2018 IEEE 22nd International Enterprise Distributed
Object Computing Workshop (EDOCW), pages 17–
26. IEEE.
Mitchell, J. (1999). From telehealth to e-health: the un-
stoppable rise of e-health. Department of Communi-
cations, Information Technology and the Arts.
Msosa, Y. J. (2018). Modelling evolving clinical practice
guidelines: a case of Malawi. PhD thesis, University
of Cape Town.
Msosa, Y. J. (2019). FCIG grammar evaluation: A usability
assessment of clinical guideline modelling constructs.
In 2019 IEEE Symposium on Computers and Commu-
nications (ISCC), pages 1141–1146. IEEE.
Neumann, J., Rockstroh, M., Franke, S., and Neumuth,
T. (2016). BPMNSIX–A BPMN 2.0 Surgical In-
tervention Extension. In 7th workshop on model-
ing and monitoring of computer assisted interventions
(M2CAI), 19th international conference on medical
image computing and computer assisted interventions
(MICCAI 2016), Athens, Greece.
Neumann, J., Wiemuth, M., Burgert, O., and Neumuth, T.
(2017). Application of activity semantics and BPMN
2.0 in the generation and modeling of generic surgical
process models. Journal of the International Foun-
dation for Computer Assisted Radiology and Surgery:
International Journal of Computer Assisted Radiology
and Surgery, 12:48–49.
Panella, M., Marchisio, S., Barbieri, A., and Di Stanislao,
F. (2008). A cluster randomized trial to assess the
impact of clinical pathways for patients with stroke:
rationale and design of the Clinical Pathways for Ef-
fective and Appropriate Care Study [NCT00673491].
BMC health services research, 8(1):1–8.
Panella, M., Marchisio, S., and Di Stanislao, F. (2003). Re-
ducing clinical variations with clinical pathways: do
pathways work? International Journal for Quality in
Health Care, 15(6):509–521.
Perchetti, G. A., Nalla, A. K., Huang, M.-L., Jerome,
K. R., and Greninger, A. L. (2020). Multiplexing
primer/probe sets for detection of SARS-CoV-2 by
qRT-PCR. Journal of Clinical Virology, 129:104499.
Preston, S., Markar, S., Baker, C., Soon, Y., Singh, S., and
Low, D. (2013). Impact of a multidisciplinary stan-
dardized clinical pathway on perioperative outcomes
in patients with oesophageal cancer. Journal of British
Surgery, 100(1):105–112.
Rieger, C., Westerkamp, M., and Kuchen, H. (2018). Chal-
lenges and Opportunities of Modularizing Textual
Domain-Specific Languages. MODELSWARD, pages
387–395.
Stroppi, L. J. R., Chiotti, O., and Villarreal, P. D. (2011).
Extending BPMN 2.0: method and tool support. In
International Workshop on Business Process Model-
ing Notation, pages 59–73. Springer.
Suganthi, S. and Poongodi, T. (2021). Interactive Visualiza-
tion for Understanding and Analyzing Medical Data.
In Exploratory Data Analytics for Healthcare, pages
101–123. CRC Press.
Thakrar, B. T., Grundschober, S. B., and Doessegger, L.
(2007). Detecting signals of drug–drug interactions
in a spontaneous reports database. British journal of
clinical pharmacology, 64(4):489–495.
Vanhaecht, K., WITTE, K. D., Depreitere, R., and Sermeus,
W. (2006). Clinical pathway audit tools: a systematic
review. Journal of nursing management, 14(7):529–
537.
Vargiu, E., Fern
`
andez, J., Miralles, F., Cano, I., Gimeno-
Santos, E., Hernandez, C., Torres, G., Colomina, J.,
de Batlle, J., Kaye, R., et al. (2017). Integrated care
for complex chronic patients. International Journal of
Integrated Care, 17(5).
Wang, S., Yu, H., Liu, J., and Liu, B. (2011). Explor-
ing the methodology and application of clinical path-
Acadela: A Domain-Specific Language for Modeling Clinical Pathways
57

way in evidence-based Chinese medicine. Frontiers of
medicine, 5(2):157–162.
Wang, X., Chen, J., Peng, F., and Lu, J. (2021). Construc-
tion of clinical pathway information management sys-
tem under the guidance of evidence-based medicine.
Journal of Healthcare Engineering, 2021.
White, M. (2009). Case management: Combining knowl-
edge with process. BPTrends, July.
Wienands, C. and Golm, M. (2009). Anatomy of a visual
domain-specific language project in an industrial con-
text. In International Conference on Model Driven
Engineering Languages and Systems, pages 453–467.
Springer.
Wolff, A. M., Taylor, S. A., and McCabe, J. F. (2004). Us-
ing checklists and reminders in clinical pathways to
improve hospital inpatient care. Medical Journal of
Australia, 181(8):428–431.
Yang, W. and Su, Q. (2014). Process mining for clinical
pathway: Literature review and future directions. In
2014 11th international conference on service systems
and service management (ICSSSM), pages 1–5. IEEE.
ICSOFT 2023 - 18th International Conference on Software Technologies
58
