
Optimization of Surgery Scheduling Problems Based on Prescriptive
Analytics
Jo
˜
ao Lopes
1 a
, Gonc¸alo Vieira
1 b
, Rita Veloso
2
, Susana Ferreira
2
, Maria Salazar
2
and Manuel Filipe Santos
1 c
1
Department of Information Systems, University of Minho, Guimar
˜
aes, Portugal
2
Centro Hospitalar Universit
´
ario de Santo Ant
´
onio (CHUdSA), Portugal
Keywords:
Prescriptive Analytics, Surgery Scheduling Problems.
Abstract:
Surgery scheduling plays a crucial role in modern healthcare systems, ensuring efficient use of resources, min-
imising patient waiting times and improving organisations’ operational performance. Additionally, healthcare
faces enormous challenges, with a general modernisation of all clinical and administrative processes expected,
requiring organisations to keep up with the latest advances in Information Technology. The scheduling of surg-
eries is a crucial sector for the good functioning of hospitals, and the management of waiting lists is directly
related to this process, which has seen the COVID-19 pandemic cause a significant increase in waiting times
in some specialities. Surgery scheduling is considered a highly complex problem, influenced by numerous
factors such as resource availability, operating shifts, patient priorities and scheduling restrictions, putting sig-
nificant challenges to healthcare providers. In this research, in collaboration with one of the leading hospitals
in Portugal, the Centro Hospitalar Universit
´
ario de Santo Ant
´
onio (CHUdSA), we propose an approach based
on Prescriptive Analytics, using optimisation algorithms to evaluate their performance in the management
of the operating room. The results allow identifying the feasibility of this approach, taking into account the
number of surgeries to be scheduled and surgical spaces in a time perspective, prevailing the priority of each
surgery in the waiting list.
1 INTRODUCTION
Over the last few years, we have witnessed a grow-
ing concern for the quality of Healthcare provided
to citizens. Organisations are increasingly seeking
more efficiency, with stronger investments in Artifi-
cial Intelligence (van Hartskamp et al., 2019), seek-
ing to assist health professionals in making increas-
ingly complex and demanding decisions (G
¨
org
¨
ul
¨
u and
Pickl, 2013). A system capable of improving, assess-
ing and preventing future scenarios becomes a focal
topic in hospital development due to organisational
objectives that each entity needs to meet and the in-
creasingly precise treatment that must be provided to
patients (Briganti and Le Moine, 2020). Alongside
this, there is a belief that the immense volume of data
in a Hospital should be better utilised. The existence
of organisational and clinical data allocated in Hos-
pital Databases makes Healthcare an area with enor-
a
https://orcid.org/0000-0001-7854-8293
b
https://orcid.org/0009-0004-2635-105X
c
https://orcid.org/0000-0002-5441-3316
mous potential for the application of Intelligent Sys-
tems, capable of improving the clinical follow-up pro-
vided to patients and managing the different organi-
sational processes inherent to any clinical speciality
(Jayaratne et al., 2019).
The Surgical Scheduling Problem (SSP) is one
of the most debated issues in hospital management.
The COVID-19 pandemic aggravated this process, as
many specialities interrupted their normal functioning
to respond more efficiently to other critical patients,
increasing the number of patients waiting for a va-
cancy to perform the surgeries they need. This needs
to be rethought, as the old scheduling processes have
already resulted in long waiting lists, making it crucial
to develop strategies that can mitigate waiting times
and financial losses for these organisations.
In cooperation with the Centro Hospitalar Univer-
sit
´
ario de Santo Ant
´
onio (CHUdSA), a study was car-
ried out to understand the feasibility of a more au-
tonomous solution, according to the intervention of
each hospital manager. The aim is to codify the ex-
isting restrictions in this process and implement opti-
474
Lopes, J., Vieira, G., Veloso, R., Ferreira, S., Salazar, M. and Santos, M.
Optimization of Surgery Scheduling Problems Based on Prescriptive Analytics.
DOI: 10.5220/0012131700003541
In Proceedings of the 12th International Conference on Data Science, Technology and Applications (DATA 2023), pages 474-479
ISBN: 978-989-758-664-4; ISSN: 2184-285X
Copyright
c
2023 by SCITEPRESS – Science and Technology Publications, Lda. Under CC license (CC BY-NC-ND 4.0)

misation algorithms that solve the increase in waiting
lists and associated costs. This study covers the en-
tire research process, from identifying and codifying
constraints to selecting and developing optimisation
algorithms, allowing a general understanding of the
viability of this approach.
2 PROBLEM DEFINITION
2.1 Surgical Scheduling Problem
Room planning is a task that needs to be addressed in
many fields. A notable field in healthcare is planning
operation rooms for surgeries. Cost containment and
reduction have become one of the primary goals in
healthcare management, with hospital managers and
professionals trying to understand each factor that in-
cludes the total cost of providing better services. Op-
erating Rooms (OR) are one of the areas that have
been gathering considerable attention since it is the
most critical cost centre and consumes a large propor-
tion of the Hospital’s total expenses. As a result, they
offer the potential for significant cost-saving, and the
Surgery Scheduling Problem (SSP) has been studied
over the years and generated a variety of approaches
and heuristics (Visintin et al., 2017).
Based on these concepts, the SSP consists of as-
signing operations to a time interval so that surgery is
only scheduled once, at a given time, and never over-
laps with another (Agnetis et al., 2014). Despite the
different development approaches, with very diverse
implementations in the type of algorithms, there are
different perspectives obtained from the time scale
and the surrounding constraints, evidencing the in-
existence of standard approaches to the problem of
SSP that effectively prove its effectiveness compared
to hospital management carried out nowadays. As a
reflection, this problem still presents a scarcity of ac-
curate proposals that may allow the establishment of
standard rules and guidelines to manage this hospital
process. In order to define the bases for the devel-
opment of a decision support system, a research was
designed to prove the effectiveness of different opti-
mization algorithms in the conception of an approach
with common restrictions to different specialties, aim-
ing at a more global solution to the different health
organizations.
2.2 Optimization Algorithms
Currently, there is a growing trend in the adoption
of computational tools based on optimization meth-
ods. According to Cortez (Cortez, 2014), opti-
mization methods are divided into three main cate-
gories: Blind Search (BS), Local Search (LS) and
Population-Based Search (PBS). BS assumes the ex-
haustion of all alternatives, ensuring that all solutions
are tested. It has an easy implementation, but its feasi-
bility differs significantly if the search space is contin-
uous or too large (Luke, 2012). LS is the most mod-
ern category of optimization and is based on new solu-
tions that are generated from existing solutions. Sev-
eral methods focus on a local neighbourhood through
a given initial solution and use previous searches to
guide the next one. PBS presents a new approach to
optimization algorithms, using a set of candidate so-
lutions instead of a single (Delen, 2019).
3 RESEARCH METHODOLOGY
Two methodologies were followed: Design Science
Research (DSR) as a research methodology, pro-
viding the necessary guidelines, and Cross-Industry
Standard Process for Data Mining (CRISP-DM). DSR
consists of 6 phases: 1. Identifying the problem and
motivation; 2. Defining objectives of the solution;
3. Design and development; 4. Demonstration; 5.
Evaluation; 6. Communication (Peffers et al., 2007).
For Data Mining (DM) projects was chosen CRISP-
DM, providing a global perspective on the life cycle
of a data mining project. Includes 6 phases: 1. Busi-
ness Understanding; 2. Data Understanding; 3. Data
Preparation; 4. Modelling; 5. Evaluation; 6. Deploy-
ment (Azevedo and Santos, 2009). Figure 1 repre-
sents the crossover between these two methodologies.
4 DATA UNDERSTANDING
For the development of this study, surgeries scheduled
in a time interval were considered, as well as the exist-
ing shifts. Two new attributes were developed directly
related to shifts: the total time associated to an oper-
ating room and an occupation time with the related
time history as a control parameter. Only the medi-
cal speciality Obesity was considered. Each surgery
involves the execution of all necessary procedures.
Additionally, an estimated time is used, associated to
each type of surgery, using the interquartile mean, ob-
tained through the history of the times related to the
performance of that surgery by ICD10 code in the last
three years. The period under consideration is based
on the non-consideration of atypical restrictions, such
as the period between 2020 and 2021, associated to
the COVID-19 pandemic. The CHUdSA provided all
data.
Optimization of Surgery Scheduling Problems Based on Prescriptive Analytics
475
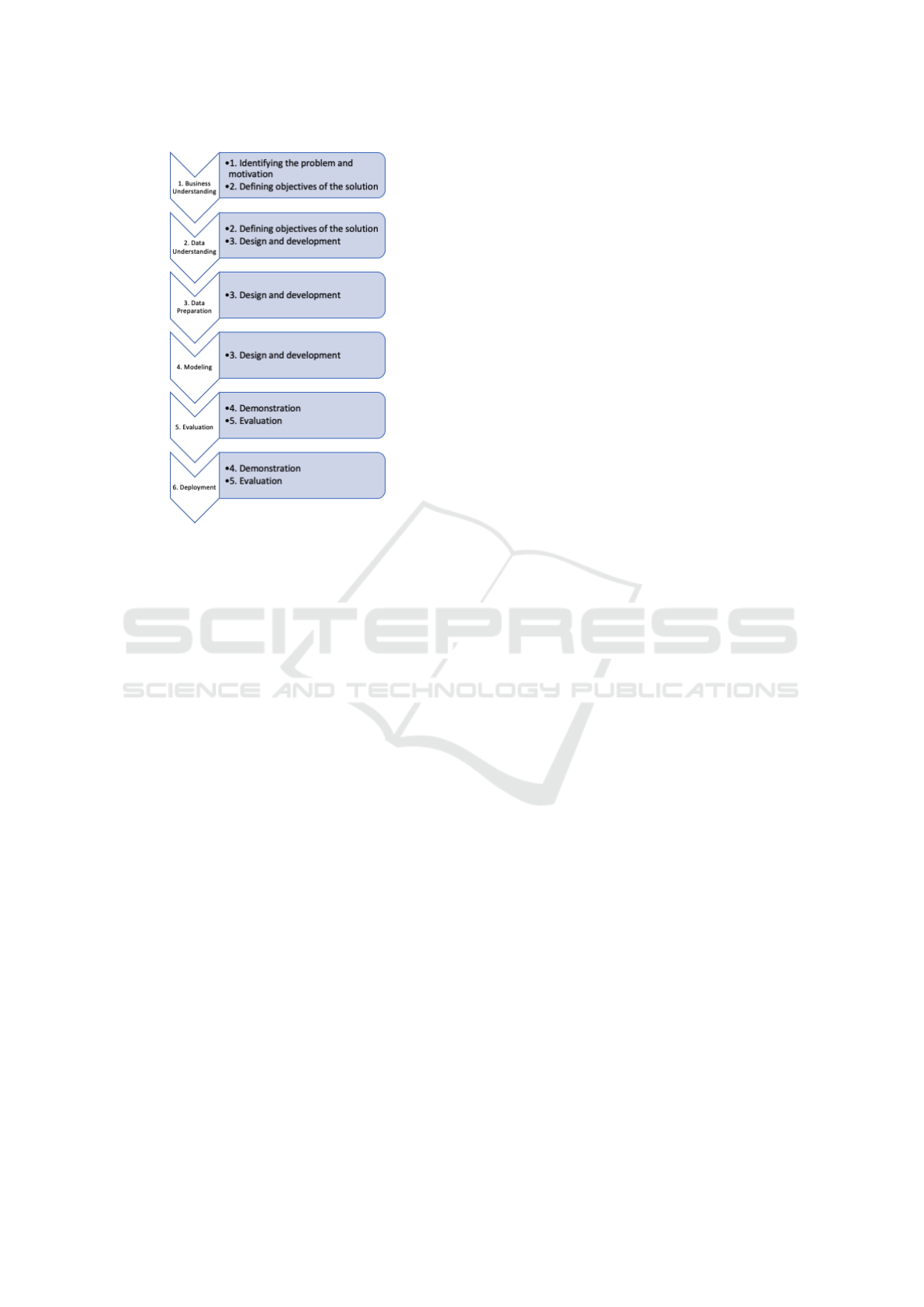
Figure 1: Crossover of Methodologies.
5 MODELING
The approach developed by the team takes into ac-
count the operational needs of CHUdSA, seeking to
strike a balance between patient typology and prior-
ity with providing the best patient care. In this sense,
hospital administrators must consider several factors
when performing surgical planning, such as the shifts
available to allocate a patient, the number of shifts
and professionals available, and the ability to perform
new admissions, always seeking to reduce the wait-
ing list for surgery. Based on a set of basic rules used
in any speciality and to model a solution for the PSS,
we consider, for this study, a surgical area of a hos-
pital, composed of S operating rooms, a finite hori-
zon of periods H, in days, and a set N of selected
patients waiting to have their surgeries scheduled.
Each patient in {1, ..., N} has a type of surgery per
ICD10 code and thus has an estimated time associ-
ated with that surgery. This time includes the duration
of the surgery and an additional time for cleaning and
pre-surgical preparation. Regarding operating rooms,
each one specifies the day and the operating room.
Additionally, it was considered that all surgeons could
be assigned to surgery. Thus, minimizing the number
of surgeries exceeding the Guaranteed Maximum Re-
sponse Time (GMRT) is the primary goal of the op-
timization. This definition translates into wanting to
obtain a solution capable of providing surgeries in a
shorter timeframe to patients while reducing the mon-
etary costs to the hospital inherent to paying signifi-
cant fines for performing surgeries after the deadline.
The design considerations for this approach are:
1. There is a prioritized patient list for surgeries. Pa-
tient priority is defined based on medical and wait-
ing time factors.
2. The hospital contains a specific set of ORs. Each
one is unique and specially adapted for certain
types of interventions.
3. A surgery that is programmed after its deadline
earns a penalty depending on your priority.
4. After a scheduling proposal performed by the
algorithms has been defined, the surgeries not
scheduled remain on the waiting list for the next
scheduling. The increase in waiting days for
surgery makes these surgeries seen as priorities to
be planned in future proposals;
5. Each surgery also has information regarding the
time required to perform necessary procedures,
such as cleaning room and preparing it.
The typical structure of these solutions is based on
three main code sectors: Initial Solution (IS), Evalu-
ation Function (EF) and Objective Function (OF), in
this order.
1. IS is a first representation of the problem in a
coding process. Ensures an initial guess, often
called a ”starting point” for the algorithm (Gan-
domi et al., 2013);
2. The definition of EF translates to evaluating a pos-
sible solution in the context of the problem to be
maximised or minimised. The function allows
different solutions to be compared, providing a
ranking or a quality measure score (Michalewicz
et al., 2006);
3. The OF is composed by the optimisation algo-
rithms. The implementation depends on the type
of algorithms to be deployed (blind search, local
search, population-based search, multi-objective
search) (Cortez, 2014).
The Initial Solution (IS) was obtained in random
or sequential slots through the list of specialised surg-
eries by assigning one slot to each input surgery. It
is implemented by the first fit method (Brent, 1989)
and obtained by assigning surgeries in available slots,
respecting the time constraints associated with each
surgery and the existing turnovers with the addition
of multiple surgeries to a given slot.
The performance is evaluated by a function devel-
oped for this purpose. Each solution considers the as-
signed surgeries by specifying a penalty (p) obtained
in a surgery (represented mathematically as follows):
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
476
pt =
i
∑
i=1
p
i
(1)
The OF was developed considering two local op-
timisation algorithms:
1. Hill Climbing (HC) is a local optimization method
that climbs a hill until a local optimum is found,
adopting consecutive searches for new solutions
within the neighbourhood of the current solution,
adopting a new solution if it is better than the
previous one (Balan, 2022). Hill Climbing (HC)
implementation was retrieved and adapted from
(Cortez, 2014) and can be perceived by the fol-
lowing function:
hclimbing(par, f n, change, control, type) (2)
The input variables are presented as follows:
• The initial solution (par);
• The evaluation function (fn) that evaluates the
total penalty of the allocated surgeries;
• A change function (change), responsible for
generating the next candidate, creating minor
disturbances in the initial solution by swapping
surgeries between different slots, and evaluat-
ing if this was profitable;
• The variable control is a list that indicates the
number of interactions to execute and the infor-
mation to collect throughout the solution;
• A last variable (type) indicates the main goal:
minimisation.
2. Simulated Annealing (SA) implementation was
also adapted from (Cortez, 2014). In contrast to
HC, which adopts a fixed value for this control
parameter, SA uses a variable temperature during
the search. The method starts with a high tem-
perature, gradually decreasing the control param-
eter until it reaches the minimum value or until the
set number of iterations is reached. The following
function represents the SA implementation:
simulated annealing( f unc, s0, niter, step) (3)
The input variables are presented as:
• The evaluation function (func) that evaluates
the total penalty, similar to HC;
• The initial solution (s0), also similar to HC;
• Maximum number of iterations (niter);
• Parameter to control the cooling speed of the
model (step).
6 EVALUATION AND
DEPLOYMENT
OR management by the CHUdSA can be classified by
the number of surgeries performed in each speciality
and the number of surgeries performed after the dead-
line. Such variables determine the total penalisation
of the hospital, translating into costs that it will have
to assume. Based on this, Table 1 represents a general
analysis of the existing data considering the special-
ity chosen (Obesity) for this study to understand the
relationship between the number of surgeries to be al-
located and the number of available vacancies. The
choice of this speciality takes into account the most
frequent scenario in which the number of surgeries
to be allocated is greater than the number of exist-
ing shifts. In this scenario, the optimisation of the
ORs must be extremely efficient to achieve the great-
est number of surgeries with the existing resources.
Table 1: Analysis between number of surgeries and avail-
able ORs in Obesity.
Number of surgeries Number of Time Slots
198 122
The implementation of HC and SA algorithms
leads to a set of results presented in Tables 2 and 3.
Table 2: Final Results of Hill Climbing Algorithm.
Hill Climbing Algorithm Results
Penalty 0
Surgeries without Penalty 190
Surgeries with Penalty 0
Unscheduled surgeries 8
Table 3: Final Results of SA Algorithm.
SA Algorithm Results
Penalty 0
Surgeries without Penalty 164
Surgeries with Penalty 1
Unscheduled surgeries 33
It was also possible to understand the impact of
the algorithms on the scheduling of each surgery: the
HC schedules 98% of surgeries for a more recent
date, compared to the scheduling date performed by
CHUdSA. In SA, it was possible to obtain a more re-
cent date in 85% of surgeries.
To perform the deployment of this solution, an ap-
plication was developed, which allows testing the dif-
ferent algorithms according to a set of variables that
interfere directly with the type of scheduling propos-
als generated. In it, all the necessary information is
available for a professional to validate the scheduling
Optimization of Surgery Scheduling Problems Based on Prescriptive Analytics
477

proposals and confirm a possible appointment. Figure
2 present the constitution of the final prototype.
Figure 2: Prototype for visualisation of a scheduling pro-
posal.
The main objective of this prototype is to inte-
grate the ability to generate possible scheduling so-
lutions for the physicians responsible for performing
this process in each speciality. These should be able to
test potential alternatives, edit the final solution, and
change the variables that directly influence the ability
to generate solutions (execution times, scheduling in-
tervals and desired efficiency), having them the final
responsibility of submitting the final proposal. Once
a solution is approved, data is sent to the clinical sys-
tem, as well as to the Database of the CHUdSA Busi-
ness Intelligence system (AIDA-BI), allowing hos-
pital professionals to consult the information at any
time, such as responsible physicians, schedules, pro-
cedures, users and operating rooms.
7 DISCUSSION
Through the implementation of these algorithms, a set
of results can be proven:
1. The penalty of automatic scheduling, according to
the described optimisation algorithms, proves the
feasibility of this approach as a response to the
SSP.
2. All implemented algorithms can offer improve-
ments in ORs management and organisation. Still,
HC is the algorithm that achieves better schedul-
ing capability;
3. The SA algorithm presents a higher than expected
number of unscheduled surgeries. This can be jus-
tified by the fact that SA does not include as a de-
termining factor the heuristic ability to establish
new solutions from the defined number of itera-
tions but through a probabilistic value (tempera-
ture) determining the ability to find new solutions.
Common to both algorithms is that certain surg-
eries have a minimum execution time greater than
the maximum time of an existing shift and, there-
fore, would never be scheduled in this optimisa-
tion process. By recommendation of CHUdSA
professionals, these surgeries are always treated
as exceptional cases and should be managed ac-
cording to specific internal procedures;
4. Modeling the first solution with a surgery allo-
cation algorithm, taking into account the priority
and longevity of a surgery on a waiting list, repre-
sents an important improvement in the scheduling
process. The total penalty proves the possibility
of improving the management of surgeries in the
possible time-space;
5. Additionally, this implementation focused on AI-
based heuristics translates into a substantial im-
provement in the number of surgeries that are al-
located after the surgical limit. Thus, we can no-
tice a great capacity for improvement of OR man-
agement with a solution capable of optimising the
scheduling process in this speciality.
8 CONCLUSION AND FUTURE
WORK
The study of allocation and scheduling problems is
always considered to be of great complexity. Taking
this reality to healthcare, the responsibility to create
an effective solution is even more significant since the
priority must always be the care provided to patients,
trying to pay attention to the existing resources and
the practices of good organisational management in-
creasingly important in the hospital context.
The developed approach offers a first sketch of
what can be contemplated in an intelligent system to
support all the decisions made in SSP. Considering
a general constraints model for any hospital, imple-
menting optimization algorithms, and considering the
same constraints for generating the initial solution, it
was possible to prove the ability to find better solu-
tions for surgical scheduling. The HC and SA algo-
rithms demonstrate the capacity to have a better oc-
cupation of the available ORs, with clear highlights
to HC, which allocates a significant percentage of
surgeries (96%), always trying to considering as main
reference the scheduling limit without accumulating
penalties. The use of many iterations in the imple-
mented algorithms means a high computational load
and a waiting time for solutions, which is still impor-
tant in order to make it possible to find the best alter-
natives within each scheduling scenario.
DATA 2023 - 12th International Conference on Data Science, Technology and Applications
478

Taking into account all the limitations found in
scheduling problems and the high level of organisa-
tional complexity that a hospital currently has, we
consider this approach a possible solution to SSP
problems, of which the organisation of surgeries on
time and the necessary cost control, crucial to opti-
mise all management processes, always prevail. SA
presents extremely satisfactory results, nullifying the
number of surgeries with a penalty, i.e., surgeries with
a scheduled date higher than the deadline. Further-
more, this algorithm provides a nearly optimal solu-
tion, reaching a stabilisation point after 100 iterations,
something that does not happen in the HC and that
may justify the fact that it does not allocate a greater
number of surgeries.
In the first phase of this research, new perspec-
tives were obtained on how an approach based on AI
heuristics can translate into a solution capable of au-
tomating and improving this process. However, some
scenarios could be further explored as future work:
1. Testing this study in other healthcare specialities
will be the first step to understanding if the suc-
cess of implementing this logic is well achieved
in different environments.
2. A deeper study on the nullification of the schedul-
ing penalty may be equated. While the hospital
would like to pay the least amount of costs related
to surgeries scheduled after the deadline, it may
be pertinent to identify whether a proposal with
a higher penalty will better serve the hospital’s
scheduling interests.
3. A new constraint can be added, always consider-
ing that there are urgent cases to be executed. De-
spite in this study only surgeries from the waiting
list were considered, it is possible to complement
the scheduling constraints with an additional rule,
always leaving space in an OR for urgent cases;
4. Improving the efficiency of the optimization
method by exploring new models and their con-
figurations (only local search algorithms were ad-
dressed, but there is some scope for development
for population-based, blind search or even multi-
objective search algorithms).
REFERENCES
Agnetis, A., Coppi, A., Corsini, M., Dellino, G., Meloni,
C., and Pranzo, M. (2014). A decomposition approach
for the combined master surgical schedule and surgi-
cal case assignment problems. Health Care Manage-
ment Science, 17(1):49–59.
Azevedo, A. and Santos, M. (2009). Business Intelligence
- State of the Art, Trends, and Open Issues. Funchal -
Madeira, Portugal.
Balan, S. (2022). Metaheuristics in optimization: Algorith-
mic perspective. Informs.
Brent, R. P. (1989). Efficient implementation of the first-
fit strategy for dynamic storage allocation. ACM
Transactions on Programming Languages and Sys-
tems, 11(3):388–403.
Briganti, G. and Le Moine, O. (2020). Artificial Intelli-
gence in Medicine: Today and Tomorrow. Frontiers
in Medicine, 7. Publisher: Frontiers.
Cortez, P. (2014). Modern Optimization with R. Use R!
Springer International Publishing : Imprint: Springer,
Cham, 1st ed. 2014 edition.
Delen, D. (2019). Prescriptive Analytics: The Final Fron-
tier for Evidence-Based Management and Optimal
Decision Making. Pearson FT Press, Hoboken, 1st
edition edition.
Gandomi, A. H., Yang, X.-S., Talatahari, S., and Alavi,
A. H. (2013). Metaheuristic Algorithms in Modeling
and Optimization. In Metaheuristic Applications in
Structures and Infrastructures, pages 1–24. Elsevier.
G
¨
org
¨
ul
¨
u, Z.-K. and Pickl, S. (2013). Adaptive Business In-
telligence: The Integration of Data Mining and Sys-
tems Engineering into an Advanced Decision Sup-
port as an Integral Part of the Business Strategy. In
Rausch, P., Sheta, A. F., and Ayesh, A., editors, Busi-
ness Intelligence and Performance Management: The-
ory, Systems and Industrial Applications, Advanced
Information and Knowledge Processing, pages 43–58.
Springer, London.
Jayaratne, M., Nallaperuma, D., De Silva, D., Alahakoon,
D., Devitt, B., Webster, K. E., and Chilamkurti,
N. (2019). A data integration platform for patient-
centered e-healthcare and clinical decision support.
Future Generation Computer Systems, 92:996–1008.
Luke, S. (2012). Essentials of Metaheuristics. Lulu, 2nd
ed. 2012 edition.
Michalewicz, Z., Schmidt, M., Michalewicz, M., and
Chiriac, C. (2006). Adaptive Business Intelligence.
Springer-Verlag, Berlin Heidelberg.
Peffers, K., Tuunanen, T., Rothenberger, M. A., and Chat-
terjee, S. (2007). A Design Science Research Method-
ology for Information Systems Research. Journal of
Management Information Systems, 24(3):45–77.
van Hartskamp, M., Consoli, S., Verhaegh, W., Petkovic,
M., and van de Stolpe, A. (2019). Artificial Intel-
ligence in Clinical Health Care Applications: View-
point. Interactive Journal of Medical Research,
8(2):e12100.
Visintin, F., Cappanera, P., Banditori, C., and Danese, P.
(2017). Development and implementation of an oper-
ating room scheduling tool: an action research study.
Production Planning & Control, 28(9):758–775.
Optimization of Surgery Scheduling Problems Based on Prescriptive Analytics
479
