
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A
TRADITIONAL SPINE SURGERY
Meike Jipp
1
1
Department of Psychology II, University of Mannheim, Schloss EO, Mannheim, Germany
Peter Pott
2
2
Laboratory for Biomechanics and Experimental Orthopeadics, Faculty of Clinical Medicine Mannheim,
Achim Wagner
3
, Essameddin Badreddin
3
Werner W. Wittmann
1
Keywords: Skill acquisition, System design, Man-machine interfaces
Abstract: Technological progress greatly revolutionizes medicine. Robots give the opportunity to reach greater
accuracy and thus improve the medical outcome. The results of a surgical intervention profoundly depend
on the robot system and on the training state of the operator. Since the learning of a surgical intervention
can be influenced by the complexity of the system, these interconnections are investigated with
psychological methods. Therefore, the skill acquisition process of a robot-based surgery is compared to a
traditional spine surgery. The usage of an appropriate robot shortens the learning curve of a spine surgery
due to a decreased complexity and reduces the impact of the surgeons’ psychomotor abilities on the
surgery’s outcome. For the design of a surgical system, different realizations must be tested in advance
regarding their cognitive workload to avoid training costs learning the operation of the system, afterwards.
The methods used are not restricted to surgical robotics.
1 INTRODUCTION
Medicine is one of the oldest sciences, as human
beings have always had a thirst for knowledge about
diseases and disorders. The development of
technology revolutionized medicine: in 1625 the
first microscope gave the opportunity to learn about
both bacteriology and chemistry
(http://techandmed.tripod.com/files/basicpages/histo
ry.htm), but only in the 21st century robotic systems
were approved for surgery
(http://electronics.howstuffworks.com/robotic-
surgery1.htm). Their capability to deal with large
amounts of data compensates for possible human
errors. Robots work more accurately and reduce the
convalescence time and possible traumata.
Nevertheless, with the use of robots, the surgical
process changes drastically and surgeons must
acquire additional skills. The design of the machine,
the man-machine interface, as well as the process of
surgery are limiting factors for the learning
complexity and are thus, responsible for clinical
results. However, the skill acquisition process with a
medical robot in particular is not well understood so
far. Considering the learning process in an early
stage of the system development may optimize the
outcome of the system and reduce the costs
drastically, which accumulate for the training of the
stuff. This interdisciplinary study between
engineering, medical, and psychological sciences is
one step to provide methods for the evaluation of the
interconnection between the learning process and the
56
Jipp M., Pott P., Wagner A., Badreddin E. and Wittmann W. (2004).
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A TRADITIONAL SPINE SURGERY.
In Proceedings of the First International Conference on Informatics in Control, Automation and Robotics, pages 56-63
DOI: 10.5220/0001136900560063
Copyright
c
SciTePress
system design. Hopefully, it will help the designers
developing their technical systems to fit human
skills.
As an example of a technical system, the hand-
held device Intelligent Tool Drive (ITD) for bone
treatment (Pott, 2003) is investigated. In its first
application, it will be used for stabilizing two or
more vertebrae (arthrodesis) requiring the surgeon to
drill holes into the pedicles of the vertebrae in
question. Fig. 1 roughly explains a vertebra’s
anatomy.
Figure 1: Anatomy of a vertebra.
(a) refers to the pedicles, (b) to the vertebral body.
To drill holes manually into the pedicles is a
difficult task as there is no room for mistakes: first,
the drill is only about 1 to 2 mm smaller than the
pedicles. Additionally, the surgeon cannot constantly
check his or her work with X-rays or similar
procedures due to the amount of radiation on both
the surgical team and the patient. Thus, the surgeon
needs experience to combine the feedback of the
drill’s resistance with the knowledge of anatomy to
figure out whether he or she is drilling at the right
place. Although this is a routine surgery about 30%
of the screws are not set ideally, about 5-6% of these
require repeated surgery (Siebert, 2000).
The concept of the ITD allows the improvement
of this type of surgery, especially regarding the
drilling process’s accuracy. The desired drilling
position is planned before the intervention basing on
3D computer tomography. During the intervention,
the robot system measures the actual position of tool
and patient and controls the accurate positioning of
the drilling tool. In this way disturbances and
displacements by the surgeon, which holds the robot
in his or her hands, can be compensated.
Implementing the ITD will require the surgeons
to perform the surgery a completely different way.
With the ITD the surgeon must plan the drilling
trajectories and he or she must find anatomic
positions for the matching of the robot coordinates
with the patient coordinates. Little research has been
done on the process to acquire the skill to perform
surgery, although it is completely different applying
new tools, so that it is obvious that the new method
must be learnt. Is the skill acquisition process shorter
or qualitatively different when using a device
compared to a traditional surgery? What if the new
tool requires all of the surgeon’s attention and no
resources are left for the patient? Which are the
underlying abilities determining the learning
process? Can the impact of these abilities be
changed through implementing the ITD in a
especially easy way, so that the need for skill
acquisition is reduced? An interdisciplinary
approach has been taken to start answering some of
these questions, and to give a first set of directions
so that the possibilities the robot offers can be full
taken advantage of. The following solution approach
gives necessary input to theoretically answer these
questions; the performed experiment gives the first
set of answers.
2 PROBLEM STATEMENT AND
SOLUTIONS APPROACH
2.1 Skill Acquisition Theory
(Ackerman, 1988)
Ackerman distinguishes between three phases within
the skill acquisition process, each of which is
determined by other abilities (Fig. 2). The first
phase, which is referred to as the cognitive phase, is
characterized through slow performance and few
errors. While practicing the learners need to build
productions, which are “if...then...clauses” that
connect a condition specifying when the actions
must be applied and the action itself (Anderson,
1980). If for example the traffic light turns red, then
the car driver must break. The process of building
productions requires both cognitive and attentional
resources (Ackerman, 1988).
Figure 2: Demonstrates the three phases of the skill
acquisition process. The first phase is given via the
straight line, the second one via the dashed and the third
one via the dotted line (adapted from Ackerman, 1988).
After having acquired a broad cognitive
representation of the task, the learner proceeds to the
associative phase. Practicing now results in finding
easier ways to reach the same result, in generalizing
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A TRADITIONAL SPINE SURGERY
57

the productions to other similar tasks, in eliminating
sub-goals and in strengthening the productions. The
ability, which determines this phase’s performance,
is the ability to compare the stored information with
the information about the new situation and to act
based on the outcome of this comparison. These are
defined as psychosensoric abilities (Ackerman,
1988).
In the last phase, which is called autonomous
processing, learners thoroughly understand the task
and have developed efficient productions that can be
performed automatically without or with only few
attentional/cognitive demands. Performing the task
is thus fast and accurate and the performance is only
limited by psychomotor abilities (Ackerman, 1988).
2.2 Factors influencing the
prototypical skill acquisition
process
This description of a skill acquisition process is only
prototypical. As already mentioned cognitive
abilities for example influence the way to learn, so
that interindividual differences result in qualitatively
different skill acquisition processes. However, not
only characteristics of the learner but also the ones
of the task influence the way to learn.
2.2.1 Characteristics of the task
A more complex task is – generally speaking – a
more difficult one, which results in a prolonged
cognitive and associative phase, so that the overall
skill acquisition process takes longer. Regarding the
robot-based spine surgery this has two major
consequences: first, the learning process is shortened
if its productions are less complex and second the
learning process can further be simplified if the
tool’s application is made less complex. A
comparison between the traditional way to perform
surgery and the robot-based one reveals that some
components are added to the traditional way, which
make it more difficult. The surgeon for example has
to “explain” the ITD on a 3D model of the patient,
where the hole should be ideally placed. However,
very difficult components are no longer needed.
When operating with the ITD the surgeon no longer
needs to consider the drill’s resistance in order to
figure out whether he or she is drilling at the right
spot or not. This is a great relief for the surgeon. An
exact and enclosing comparison of both methods is
out of the scope of this article, however it reveals
that the robot-based surgery is altogether less
complex, so that it can be inferred that the skill
acquisition process is shortened.
Task consistency refers to the number of
invariant rules for completing the task in question
successfully (Ackerman, 1987). If the task is
inconsistent, no general valid productions can be
generated, so that the task cannot be acquired. As the
ITD is used in a critical medical context, the rules
for deciding when a given production is to be used
must be highly consistent, so that learning takes
place.
2.2.2 Characteristics of the learner
Interindividual differences do determine
performance during the skill acquisition process:
cognitive abilities influencing the first,
psychosensoric the second and psychomotor abilities
the third phase of the skill acquisition process. The
first two refer to intelligence. The model of
intelligence on which the study is based on is the
Berlin Intelligence Structure Model developed by
Jäger (1982). This hierarchical model distinguishes
between two facets: operations and contents. The
contents refer to the type of material that must be
processed; the operations define what must be done
with the content. The figural content determines
performance during surgery. It for example requires
the surgeons to interpret the information on two-
dimensional X-rays three-dimensionally. An
operation is for example reasoning, which refers to
the ability to solve problems. Perceptual speed,
another operation, is related to the speed of the work
on simple, cognitive tasks. As this description
shows, the latter operation is closely related to the
cognitive requirements in the second phase,
reasoning to the requirements in the first phase.
How does the skill acquisition process change
when comparing two learners, one with high
reasoning, figural abilities, and perceptual speed,
and the other one with low abilities? Learners who
are more able show greater performance levels and
thus proceed to the next phase faster, because they
build productions that are more exact faster. As in
the next phase, this ability no longer predicts
performance and interindividual performance
differences are then balanced, if the learners have
the same level of the ability influencing performance
in the next phase. However, the advantage, the more
able learners have already gained, will not be caught
up by the others, so that learners with higher ability
levels have a general shorter and steeper learning
curve.
The individual differences in both the
performance level and the time needed to reach the
level where the next phase starts can be reduced if
the abilities underlying the first and second phase
can be made less important. As already described, an
ICINCO 2004 - ROBOTICS AND AUTOMATION
58

increased task complexity makes both the cognitive
abilities and the psychosensoric ones more
important, so that their influence can be reduced
through reducing task complexity. Therefore, the
robot-based and the traditional spine surgery have
already been compared with the result that the robot-
based one has been rated as less complex. Thus, the
first major accomplishment of implementing the
robot is a shortened skill acquisition process.
Another major factor heavily influencing the
skill acquisition are psychomotor abilities.
Psychomotor ability reflects the ability to react fast
on tasks that require little or no cognitive processing
at all (Ackerman, 1988). The abilities influencing
the success of the surgery in question are limited to
arm and finger movements: precision and co-
ordination. A participant with low abilities shows a
slower course of the acquisition process but also
fails to reach the same performance level. This
difference has huge consequences for the success of
a surgery: a surgeon with higher psychomotor
abilities will manage the challenges of the surgery a
lot better than one with less psychomotor abilities
even after having acquired the skill. This is
especially important, as here the drill’s resistance
must be analyzed and the operator must react with
very fine motor movements. Psychomotor abilities
thus decide on success or failure in a traditional
surgery. Here, the second accomplishment of
implementing the robot is apparent: the robot
reduces the impact of different ability levels and
thus enables not only surgeons with very high
psychomotor abilities to perform this type of
surgery.
2.3 Problem Statement
Summarizing, the ITD’s implementation
theoretically has two major accomplishments: it
reduces the impact of psychomotor abilities, so that
at the end of the learning process learners with less
abilities do not show a lower level of performance.
Second it reduces the impact of the cognitive
abilities because of its decreased complexity, so that
the learning process is shorter. However, the positive
effects can be reduced if the robot-based surgery is
made more complex than it needs to be and thus
increases the cognitive workload. Therefore, a
thorough analysis is necessary even before the
completion of the tool to make the robot benefit
from synergies between engineering and
psychology.
The registration of a vertebra, i.e. the matching
of the robot and the patient coordinate frames, is a
good example to demonstrate a possible reduction of
the ITD’ advantages. There are a couple of
algorithms which could work, however these vary
regarding the challenges for the surgeon. One
algorithm with which the matching could be
performed is the surface matching. Here, the surgeon
needs to scan the vertebrae using a pointer. The
scanned area should be as big as possible to ensure
successful matching. The computer tries to align
these scanned points on the patient’s bones with the
3D model to identify the vertebra that must be
performed surgery on. In contrast to the surface
matching, pair-point matching determines exactly
which points of the vertebrae must be scanned. The
surgeon then has to exactly identify the relevant
points on the screen, he or she has to find these
points on the patient and scan them. The probability
of successfully matching the 3D model and the
actual vertebra is here augmented, whereas the
scanning process is more complicated. Theoretically,
the surface matching should be chosen for the ITD’s
implementation. Otherwise the more complex
production needed to acquire the pair-point
matching which would make the robot-based
surgery more complex and thus reduce its positive
effect compared to the traditional surgery.
The experiment was designed in order to test the
impact of the matching procedure on the work load
of the surgeon, but it is also used to start research in
this field, showing that a learning curve is apparent
to validate Ackerman’s theory and implement it as a
basis for future research. These are the research
questions to be addressed:
-Does learning take place when operating the
spine?
-Is the learning curve concordant with
Ackerman’s skill acquisition theory? The theory is
tested empirically via the factors reasoning, figural
abilities, general intelligence, which should have
high predictive validity coefficients for the first
practice trials. The second and third phases was not
tested.
-Do the learning curves differ regarding the
cognitive workload? Altogether two learning curves
result out of this experiment: one without matching,
and one with the pair-point matching. This
hypothesis tests the impact of the performance of the
matching procedure on the skill acquisition process
regarding the cognitive phase. Through adding one
component of the robot-based surgery to the
traditional one, the answer of this hypothesis is an
important step to make the ITD cognitively as easy
as possible for the surgeon and thus to make major
advantage of the ITD’s implementation.
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A TRADITIONAL SPINE SURGERY
59

3 EXPERIMENT
3.1 Participants
The experiment’s participating group was one of
convenience: the participants were recruited in
lectures at the University of Mannheim, so that all
participants were students (50% male, 50% female).
Surgeons could not be recruited due to their strict
time schedule. Also, not enough students of
medicine could be convinced to participate, so that
17 participants study a major related to computer
science, 17 psychology, 5 medicine and 5 were from
other majors such as business. The group size of 44
was set so that possible medium effects can be
detected according to the standards set by Cohen
(1992). The reported average drilling experience was
little, whereas test theoretical problems might have
biased the results.
3.2 Apparatus and instruments used
Reasoning, general intelligence and figural abilities
were measured to predict performance regarding
drilling time and accuracy in the cognitive phase of
the skill acquisition process.
The diagnostic tool used to collect information
on intelligence was the Berlin Intelligence Structure
Test (BIS-4) (Jäger, Süß & Beauducel, 1997). The
short version of the test was used to assess general
intelligence and reasoning. For collecting data on
figural abilities, some further tasks were added to the
test. These resulting 25 tasks were separated into
two booklets, in between which a break of 10
minutes was included. Both the standardization of
the administration and of the analysis given in the
test’s manual were used to ensure objectivity. Other
major criteria of the test were repeatedly measured
for the BIS-4 and showed good results (for a
summary see (Jäger, Süß & Beauducel, 1997)). It
was decided to work with this test first because the
BIS-4 measures all relevant information needed to
investigate the cognitive phase, and second because
the test’s quality criteria are highly promising.
The time needed to drill was measured with a
standard, digital stopwatch during the drilling
processes. The stopwatch was started when the drill
first touched the vertebra and was stopped as soon as
the participant told the experimenter that he or she is
finished. The recorded time was reported to the
participants as feedback, which is necessary to
enhance the skill acquisition process. Regarding
accuracy, the participants were told to drill exactly
20 mm deep, directly in the vertebra’ center, at an
angle of 90
o
and were told to watch that the surface
area of the drilling to make sure it was not getting
too big. The depth, the surface area, and the
deviation from the center were all based on
measures of an electronic digital caliper
(repeatability accuracy: 0.01 mm). The angle was
assessed with a stick of wood that had the same
diameter as the drill (4mm), which was put into the
drilled hole and was adjusted to a vertical line. With
an angle made of steel the biggest deviation from the
ideal angle of 90
o
was recorded. If the participants
performed the matching, another variable was
included into the accuracy index: the success of the
matching trials. Feedback on each point was given
after each trial to the participant.
3.3 Experimental set-up
The experiment took place in two sessions. In the
first one, which was between 1.5 and 2 hours long,
participants performed the selected tasks of the BIS-
4. They were tested in groups with a maximum size
of 9 participants. The second session took place
between 1 and 2 weeks later with one participant
each and also took about 1.5 and 2 hours depending
on the condition into which the participants were
grouped randomly: the matching versus no matching
group. The second session started with a short
explanation of the experiment. While reading the
instructions to the participants, the procedure was
explained on a sketch of the “spine” used in this
experiment. These sketches roughly showed the
experimental setting: a piece of wood lying on the
table represented the spine, into which six round
sticks were inserted roundly shaped at the top. These
six pedicles were hidden under a towel during the
whole experiment, so that the participants had no
visual information about their shape, and were used
in order to perform the matching. The participants
had to find the highest point of a pedicle of their
choice and had to touch it with a pointer and then
press a switch lying on the floor. This pointer was
adapted in shape and size to the one used in the
medical setting. The pointer and the pedicles were
electrically connected to a display box. As soon as
the participant pressed the switch, two lights
indicated to the experimenter that first the switch
had been pressed, and second whether the highest
point had been touched or not. The participants
could choose the pedicle they wanted to match with
one constraint: it was not allowed to use the same
one twice in a row.
After having performed two of these matching
trials, one drilling procedure was performed. The
drilling process was the same in both groups: The
hole had to be drilled into similar vertebrae, that
were arranged on the other end of the “spine”: from
ICINCO 2004 - ROBOTICS AND AUTOMATION
60

16 vertebrae 10 had to be chosen. Each vertebra was
about 30 mm long and 12 mm wide and was inserted
into a bush made of aluminum that was inserted into
the “spine”. The drilling itself was made with a
portable drilling machine. Except the pointer and the
drilling machine, no other tools were used. The
pedicles into which the hole had to be drilled were
not hidden and were straight at the top. Last, a final
questionnaire was answered in order to collect
demographic data on the participants. The spine on
which both the drilling and the matching have been
performed is given in Fig. 3.
Figure 3: The “spine” used in this experiment. On the left
side the vertebrae used for the matching procedure are
displayed, the ones on the right side were used for the
drilling procedure.
3.4 Results
3.4.1 Pre-Analysis
Each variable indicating accuracy was tested with
the F-distribution to figure out whether a learning
effect took place. These are the results:
-For the deviation from the ideal depth the
learning factor is significant with a probability of
p = 0.000 (F(9,387) = 16.687). A learning effect
with an effect size of f
2
= 0.388 was found indicating
how many standard deviations the participants
improved their drilling.
-For the deviation from the ideal angle the
learning factor, is significant with an error
probability of p = 0.031 (F(9,387) = 2.069). The
effect size was calculated as f
2
= 0.049.
-For the deviation from the center, no learning
effect took place, which might be based on the
inaccurate feedback given to the participants. The
probability is p = 0.171 (F(9,387) = 1.436), which is
bigger than the accepted critical value of p = 0.05 to
mistakenly reject the hypothesis, that no effect is
there, although one exists. The size of the learning
effect was calculated as f
2
= 0.033, which shows that
an effect might be there, however, not big enough to
be detectable with the number of participants tested.
-For the surface area the learning factor is
significant with a probability of p = 0.016
(F(9,387) = 2.303). The effect size was calculated as
f
2
= 0.053.
-For the matching procedures the learning factor
is significant with a probability of p = 0.000
(F = 9,189) = 4.548. The effect size was calculated
as f
2
= 0.216.
As the learning curve is analyzed, the accuracy
index is only made up of those variables showing a
learning effect. These variables were transformed to
delete the information about the measurement unit
and about the ideal value, so that each single
variable gives information about the number of units
the ideal value has not been met. The mean was
calculated out of these transformations to indicate
the overall accuracy. The data set was also checked
for extreme values and two participants had to be
excluded.
The drilling time measures showed many
extreme values. As this might result in non-
significant results when testing the hypotheses, the
time measures were transformed logarithmically.
Despite this transformation, one participant had to
be excluded from the analysis.
3.4.2 Significance testing
Finally, the research questions can be answered:
-Does learning take place when operating the
spine regarding drilling time? The analysis shows a
significant learning factor (F(9,360) = 10.661,
p = 0.000) with an effect size of f
2
= 0.266.
Curvilinearity is tested as well with significant
results: the linear trend is significant with p = 0.000
(F(1,40 = 29.165, f
2
= 0.729), the quadratic one with
p = 0.000 (F(1,40) = 7.825, f
2
= 0.679) and the cubic
effect with p = 0.001 (F(1,40) = 12.343, f
2
= 0.308)
giving information about the learning curve’s shape.
-Does learning take place when operating the spine
regarding accuracy? The learning factor is
significant as well with p = 0.000 (F(9,351) = 0.725,
f
2
= 0.566). The linear trend is also significant with
p = 0.000 (F(1,39) = 67.372, f
2
= 1.713), the
quadratic one with p = 0.000 (F(1,39) = 17.042,
f
2
= 0.449) and the cubic one with p = 0.032
(F(1,39) = 4.917, f
2
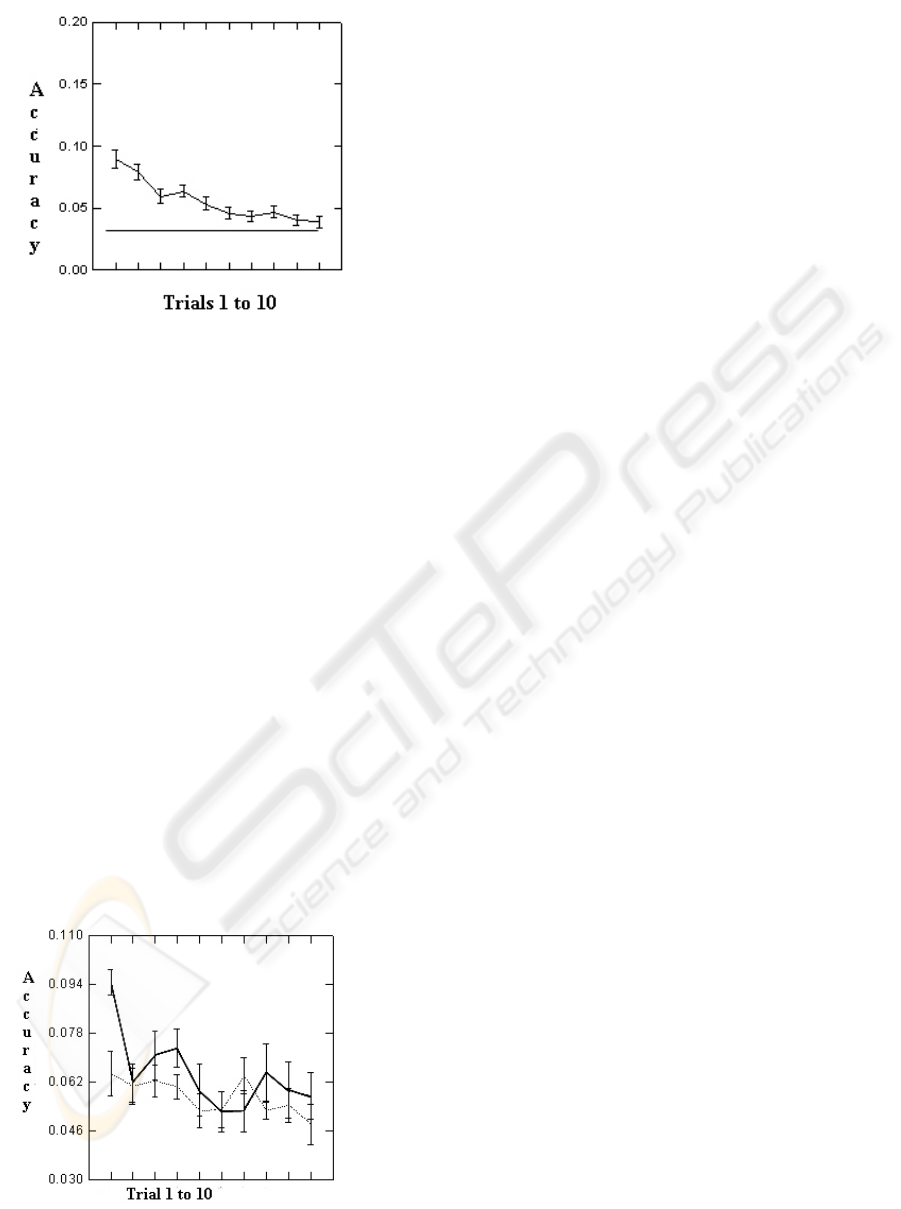
= 0.116). Fig. 4 shows the
learning curve of all participants over all trials.
-Is the learning curve concordant with
Ackerman’s skill acquisition theory regarding
drilling time? Testing this interaction effect between
learning and the cognitive factors reveals the
following results: The interaction effect between the
learning factor and reasoning is significant with
p = 0.010 (F(9,333) = 2.446, f
2
= 0.066), the
interaction effect between the learning factor and
general intelligence is not significant with p = 0.669
(F(9,333) = 0.744, f
2
= 0.020) and the interaction
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A TRADITIONAL SPINE SURGERY
61
effect between the learning factor and general
intelligence is not significant with p = 0.913
(F(9,333) = 0.440, f
2
= 0.012). Reasoning shows a
significant quadratic trend with p = 0.016
(F(1,37) = 6.389, f
2
= 0.172).
-Is the learning curve concordant with
Ackerman’s skill acquisition theory regarding
accuracy? The interaction effect between general
intelligence and the learning factor is significant
with p = 0.010 (F(9,324) = 2.463, f
2
= 0.069), the
interaction effect between the figural abilities and
the learning factor is significant with p = 0.002
(F(9,324) = 3.003, f
2
= 0.084) and the interaction
effect between reasoning and the learning factor is
not significant with p = 0.113 (F(9,324) = 1.539,
f
2
= 0.042). The curvilinear trends also reveals
significant results: the linear trend is significant for
the interaction between general intelligence and the
learning factor with p = 0.040 (F(1,36) = 4.539,
f
2
= 0.131) as well as the linear trend for the
interaction between figural abilities and the learning
factor with p = 0.007 (F(1,36) = 8.238, f
2
= 0.229).
The cubic trend is also significant but only regarding
the interaction between the learning factor and
general intelligence with p = 0.010 (F(1,36) = 7.361,
f
2
= 0.200). Fig. 5 visualizes the different learning
curves for the more and less intelligent participants.
-Do the accuracy’s learning curves differ
regarding the cognitive workload? A three-way
interaction effect between the cognitive factors, the
variable that groups the participants into their
experimental condition and the learning factor must
be tested: the result is not significant for general
intelligence with p = 0.921 (F(9,324) = 0.427,
f
2
= 0.010), for reasoning with p = 0.766
(F(9,324) = 0.636, f
2
= 0.017) and for figural
abilities with p = 0.988 (F(9,324) = 0.245,
f
2
= 0.007).
For all tests, the assumptions underlying the
statistical significance tests were checked, and none
of them was severely violated. Further, the stability
of the results was tested revealing very little
variation regarding the reported effect sizes, so that
the results can be interpreted.
3.5 Discussion, conclusion, and final
remarks
First of all, this study shows that it is both necessary
and possible to learn to perform surgery. Drilling
time shows a large learning effect: the participants
got faster with the number of trials performed until
about the 7th trial. It is surprising that learning
interacts with the participants’ reasoning abilities in
the following way: the more able participants need
more time to drill, show a longer learning process
and also improve their timing less than do the less
able participants. It is in this respect concordant to
the theory that reasoning actually predicts the
acquisition process, however, the effect’s direction
must be discussed. Probably the more able
participants focus on accuracy, so that the drilling
time is a less important factor for them. The
participants with greater figural abilities drill more
accurately, need less time to reach a comparable
accuracy index, and acquire the skill faster. The
same is true for general intelligence. As the latter is
based on various components of less general
intelligence factors such as reasoning or figural
abilities, this is not surprising. Especially general
intelligence shows relatively high correlations with
reasoning, however, without causing statistical
problems. This might be a reason for the results
regarding intelligence and drilling time. Altogether,
the results confirm Ackerman’s theory: skill
acquisition takes place for both time and accuracy
and the learning process depends in its first phase on
intelligence. The learning curve for accuracy is
altogether longer than the one for the drilling time.
Figure 4: Line plot of the accuracy levels over all
trials. Smaller numbers indicate better accuracy. The
asymptote shows that the participants do not reach a
perfect accuracy level.
Figure 5: Line plot of the two learning curves for the less
able participants (straight line) and the more able ones
(
dotted line
)
. Smaller numbers indicate better accurac
y
.
ICINCO 2004 - ROBOTICS AND AUTOMATION
62

Here about 9 to 10 trials are needed to reach the
phase in which the cognitive factors no longer play
an important role. Fig. 4 further demonstrated that
human beings do not reach a perfect accuracy level,
and gave a benchmark on the accuracy level of the
human beings that the robot must exceed. As this
“spine surgery” has only been a rough sketch of the
real surgery, one can be imagine how much bigger
the already detected medium-sized effects could be
if tested in the real word. Last, the impact of the
pair-point matching procedure on the skill
acquisition’s cognitive phase is not significant, so
that a possible effect has either been too small to be
detectable with the number of participants tested or
the effect might not be there. The results indicate
that the implementation of the pair-point matching
procedure, thus, does not impede the robot’s positive
impact.
Our simulation demonstrated that the input from
psychology paid off. This article provides methods
to analyze the demands on any technical system in
respect to the human skill acquisition process as an
important system design factor. Skill acquisition
theory worked in predicting and explaining
performance. Therefore, let us look at the demands
to be put on an excellent robot through the lens of
skill acquisition theory:
a) A robot should at least in the long run reduce the
cognitive load on the surgeon. The surgeon then can
invest his or her cognitive resources on other parts of
the surgery.
b) A robot should reduce the time it takes to acquire
a skill. In the long run, this should contribute to
reduce the inevitable costs of introducing it.
c) Reducing cognitive load the robot should enable a
larger percentage of medical doctors to learn and do
high-quality surgery.
d) A robot should reach a level of accuracy sooner
and outperform the benchmarks set by traditional
methods in terms of much higher accuracy.
Will our ITD fulfill these promises? Well, we are
working hard on it and future research will tell you
how much we succeeded.
REFERENCES
Ackerman, P.L., 1987. Individual differences in skill
learning: an integration of psychometric and
information processing perspectives. Psychological
Bulletin, 102(1), 3-27.
Ackerman, P.L., 1988. Determinants of individual
differences during skill acquisition: cognitive abilities
and information processing. Journal of Experimental
Psychology: General, 117(3), 288-318.
Anderson, J.R., 1980. Cognitive psychology and its
implications. New York: W.H. Freeman and
Company.
Cohen, J., 1992. A Power Primer. Psychological Bulletin,
112 (1), 155-159.
Jäger, A.O., 1982. Mehrmodale Klassifikation von
Intelligenzleistungen: Experimentell kontrollierte
Weiterentwicklung eines deskriptiven
Intelligenzstrukturmodells. Diagnostica, 28(3), 195-
225.
Jäger, A.O., Süß, H.-M. & Bedauducel, A., 1997. Berliner
Intelligenzstruktur-Test. Göttingen: Hogrefe.
Pott, P.P., Schwarz, M.L., Köpfle, A., Schill, M, Wagner,
A., Badreddin, E., Männer, R., Weiser, P., Scharf, H.-
P., 2003. ITD - a handheld manipulator for medical
applications: concept and design, 3rd annual meeting
of CAOS, Marbella, Spain.
Siebert, W., 2000. Navigation in der Wirbelsäulenchirur-
gie. Implant, 2, 9-10.
SKILL ACQUISITION PROCESS OF A ROBOT-BASED AND A TRADITIONAL SPINE SURGERY
63
