
WIRELESS TELEMEDICINE AND SERVICE LEVEL
MANAGEMENT ARCHITECTURE SPECIFICATION
Cristina Miyata, Tereza Cristina Carvalho
Department of Electrical Engineering, University of Sao Paulo, Sao Paulo, Brazil
Stewart Russell, Akira Kawaguchi
New York Center for Biomedical Engineering, City College of New York, New York, USA
Keywords: Wireless Telemedicine, Service Level Management, RM-ODP
Abstract: Wireless telemedicine is a new and evolving area in medical and health care systems, exploiting new
developments in mobile telecommunication and multimedia technologies and their integration into new
mobile health care delivery systems. A growing body of researchers and manufacturers are working to
develop a new generation of wireless technology applications for the medical field. In industry and clinical
practice, it is common to outsource services from non-core departments, such as Information Technology
(IT) and financial support. Overall business performance depends on these outsourced services, therefore a
contractual guarantee of outsourced service performance must be developed, which is then monitored by a
Service Level Management (SLM) process. A rigorous approach is needed to specify SLM system
architectures that are scalable, flexible, reliable and secure. This paper will discuss the establishment of
architecture suitable for the evaluation and measurement of quality of services (QoS) for wireless
telemedicine applications. We consider a case-study of a wireless diabetes information management system.
The overall methodology and a stepwise specification approach based on the reference model for Open
Distributed Processing (RM-ODP) is presented.
1 INTRODUCTION
Mobile computing, now a mature and established
field, is becoming the dominant computing paradigm
(Myers B.A. et al., 2003). The application of this
fast developing information technology in heath-care
industry will also bring promising economic and
technology contribution. As the healthcare
industry’s transition from paper to electronic
medical records continues, another technological
revolution is taking place in hospital, clinics, and
practitioner’s offices. Healthcare delivery itself is
being increasingly mobilized through the use of
wireless technologies.
Telemedicine is the use of telecommunications to
provide medical information and services.
Applications can be tailored to meet a need for
interactive communication, real-time biometric data
transfer, database management, information
processing, or some combination thereof (Lin, J.C.,
1999) (Tacharka, S. et al., 2001). Providing
caregivers real-time access to accurate patient data
(clinical histories, treatments, medications, tests, lab
results, insurance information) has the potential to
reduce medical errors, increase data accuracy,
increase efficiency of healthcare personnel, and
improve both clinical care, and patient self-care (de
Sonnaville, J.J. et al., 1997)(Fund M.M., 1999).
Wireless telemedicine is a new and evolving area
in medicine and healthcare systems. It involves the
use of a wide array of mobile telecommunication
and multimedia technologies and their integration
for new mobile healthcare delivery systems
(Pattichis C.S. et al., 2002). In fact, wireless
solutions could be useful at most patient care points,
from clinical monitoring, lab result reporting and
medication management, to robotic delivery carts,
real-time eligibility verification and claim
submission. Examples of wireless applications found
in healthcare facilities today are: administration and
resource management; wireless pre-hospital care;
mobile workstations; medication management;
hand-held data assistants; patient monitoring;
70
Miyata C., Cristina Carvalho T., Russell S. and Kawaguchi A. (2004).
WIRELESS TELEMEDICINE AND SERVICE LEVEL MANAGEMENT ARCHITECTURE SPECIFICATION.
In Proceedings of the First International Conference on E-Business and Telecommunication Networks, pages 70-78
DOI: 10.5220/0001399000700078
Copyright
c
SciTePress

ambulatory and home patient monitoring (Watchter
G., 2004).
As current mobile computing limitations are
properly studied and addressed, the possibilities for
mobile telemedicine applications increase (Chalmers
D., 2004). These limitations include: highly variable
communication quality due to environmental
variations and handoff, management of data location
for efficient access, restrictions of battery life and
screen size, connection cost, and increased security
risks.
The next generation of mobile communication
environment should be able to effectively support
high-speed wireless applications with proper
security mechanisms and Mobile Quality of Service
(QoS), which is the set of performance elements
associated with the wireless link, such as channel
error rate, and with mobile units, such as Handoff-
call Dropping Probability (HDP) and New-call
Blocking Probability (NBP) (Hu F. et al., 2004). A
summary of important QoS characteristics for wired
and wireless telemedicine applications is presented
in section 4.
In most industries, including healthcare,
outsourcing non-core business services and
departments, such as IT (Information Technology)
and financial departments, is common practice.
Since overall business performance depends on
services provided by outsourced departments, the
company and the outsource service providers
establish a contractual guarantee, or Service Level
Agreement (SLA), of outsourced services
performance.
In order to guarantee the agreed upon service
level, charge customers correctly, and improve the
service provider’s products, the service provider
needs a Service Level Management process (SLM)
to articulate the SLA. They also can create products,
monitor services, measure their service level, and
produce Service Level Reports (SLRs) through the
SLM. An SLM system, by measuring the quality of
monitored services, allows the service provider, to
act before an SLA is violated, and will generate an
appropriate SLR. A business enterprise may also
employ SLM systems to check the actual delivered
service level against SLRs generated by service
providers (Lewis L., 1999).
Recent work at University of Sao Paulo (USP)
introduced an Open Distributed Processing
Reference Model (RM-ODP) based method of SLM
system architecture specification for
telecommunication service providers (Miyata, C.M.
et al., 2003). An overview of this method is
presented in section 3.
This paper discusses the establishment of an
architecture suitable for the evaluation and
measurement of the service quality of wireless
telemedicine applications. The goal of this research
is to develop a systematic approach to specify SLM
system architectures that are scalable, flexible,
reliable and secure. A case model considered for the
study is a wireless diabetes information management
system described in section 2. Recently, several
wireless systems for the management of data and
reports for self-test blood-glucose meters have been
developed (Kawaguchi A. et al., 2003) (Vigersky
R.A. et al., 2003). Each of these systems has the
potential to reduce the administrative burden to the
patient significantly. As promising as these systems
are, without appropriate design consideration,
interoperability with each other and with existing
computer systems will be severely limited. Section 5
presents an ODP reference model based method of
SLM system architecture specification for wireless
telemedicine systems, as exemplified with the
Wireless Blood-glucose Management system.
2 WIRELESS BLOOD GLUCOSE
MONITORING: A CASE STUDY
The New York Center for Biomedical Engineering
and Department of Computer Science at City
College of New York (CCNY), in conjunction with
the Bayer Corporation, have been developing a
system, called the Wireless Blood-glucose
Monitoring System (WBgM), that will automatically
transfer blood-glucose readings from a hand-held
glucose meter to a wireless personal digital assistant,
and then to an Internet database (Kawaguchi A. et
al., 2003) (Vigersky R.A. et al., 2003). The data will
then be represented to the diabetes management
team and to the patient in a consistent manner with
their needs. Iterative design procedures will result in
a product that can lead to more effective
management, record keeping, and team
development.
A major impediment to the progress towards
evidence-based medical practice, shared patient care
and resource management in healthcare is the
inability to effectively share information across
systems and between caregivers. Electronic and
paper healthcare records are held in islands of
information in independent information systems,
each with its own technical culture and view of the
healthcare domain. For the need of the public use,
system development practice must be based on an
enterprise model that encompasses the capabilities
required to process medical information by hospital,
government, insurance parties, etc.
The objectives of the WBgM system
development are (1) to specify a generic and open
means for combining healthcare records or dossiers
WIRELESS TELEMEDICINE AND SERVICE LEVEL MANAGEMENT ARCHITECTURE SPECIFICATION
71

consistently, simply, comprehensibly and securely,
to enable the sharing of data between different
information systems in different places, and (2) to
produce tools and guidelines that can be used in the
migration from legacy healthcare systems, as an
evolution strategy for a region or Member State, or
as an exploitation plan for a healthcare site or
commercial company.
The WBgM is essentially a data management
system, designed to improve communication
between patient and doctor, and encourage
participation in self-care. As such, the value added
components of the WBgM are not as easy to define
as one that is purely technology based. Even with
flawless technical performance, the successful
implementation of a health care aid must have
evaluation criteria based on measurable outcomes to
the health or convenience of the user.
3 ODP BASED SPECIFICATION
METHOD FOR SLM
ARCHITECTURE
The RM-ODP based method for SLM system
architecture specification introduced by the
Polytechnic School of University of Sao Paulo uses
TMN network management concepts; TMF
definitions of services, service levels and SLM
process; ISO/ITU-T concepts related to quality of
service; and RM-ODP open and distributed system
specification principles.
The method is basically composed by eight
phases (Miyata C.M., et al., 2003): (1) Business
modelling; (2) Service modelling, (3) Service
relevant QoS characteristics identification, (4) QoS
and SLA modelling, (5) Proactive monitoring
definition; (6) SLRs generation process definition,
(7) Accounting management system integration
definition, and (8) SLM system architecture
definition.
The use of RM-ODP viewpoints (enterprise,
information, computational, engineering and
technology) organizes the process of specifying
SLM system architecture requirements and reduces
its complexity. Although the work referred to deals
specifically with the specification of SLM systems
architectures for telecommunication services
providers, the method can be extended and adapted
to other service provisioning areas, such as
healthcare services.
4 QOS IN WIRELESS
TELEMEDICINE
The overall satisfaction of users depends on myriad
performance elements, all of which must be
correctly monitored and evaluated. The collective
effect of these performance criteria is termed Quality
of Service (QoS). Depending on the service, there
are a number of different relevant QoS
characteristics, parameters and mechanisms. This
section lists important QoS characteristics for wired
and wireless telemedicine applications.
In order to guarantee end-to-end QoS in
telemedicine solutions, it is necessary to guarantee
QoS in all services that comprise the solution:
including applications, network infrastructure (wired
and wireless) and customer care. QoS related to
network performance in IP networks is qualified in
terms of latency, jitter, throughput, packet loss,
packet error and availability (QoS parameters).
Several Internet Engineering Task Force (IETF)
groups have been working on standardized
approaches (QoS mechanisms) for IP-based QoS
technologies.
Next generation wireless and mobile devices will
support applications ranging from traditional cellular
voice to web browsing and interactive multimedia
applications. Efforts have been made to identify new
QoS parameters that are exclusive to wireless
communications and create Mobile QoS algorithms
and mechanisms (Sadeghi, B. et al., 2004).
Accordingly, infrastructure and application QoS
parameters related to operational performance are:
Mean Time To Failure (MTTF), Mean Time To
Repair (MTTR) and Mean Time Between Failure
(MTBF).
In addition, packet error, packet loss and
availability affect the reliability and overall
application performance of the telemedicine
solution. Multimedia telemedicine applications are
sensitive to delay, jitter and throughput.
Furthermore, security of patient’s health information
and profile must be guaranteed in telemedicine
solutions in terms of confidentiality, authentication,
data integrity, non-repudiation and access control.
Though it is common sense that there is no bullet-
proof security solution, security and its risks can be
managed. Appropriate security policies and
mechanisms—e.g. to choose an appropriate
cryptographic scheme and algorithm—must be
employed in telemedicine solutions according to the
level of security needed (Kawaguchi A. et al., 2003).
Performance of many services can’t be measured
using objective QoS characteristics. Subjective QoS
characteristics usually need end user feedback to be
measured. A widely accepted formulation to
ICETE 2004 - GLOBAL COMMUNICATION INFORMATION SYSTEMS AND SERVICES
72
measure customer satisfaction is the ServQual
equation (Parasuraman, A. et al., 1988):
Quality = Perceptions - Expectations
Users judge quality to be satisfactory when their
expectations are met. The more their expectations
are exceeded, the higher is the perceived service
quality. Standards to measure some subjective QoS
characteristics such as voice clarity (ex: MOS,
PSQM and PAMS) were elaborated. Despite the fact
that there is no standard for customer care and
helpdesk services performance measurement, several
guides provide techniques to obtain customer
feedback and analyze collected data (Hill N., 1996)
(Vavra T.G. 1997).
5 SLM ARCHITECTURE FOR
WIRELESS TELEMEDICINE
APPLICATIONS
In this section, we present the comprehensive result
of the adaptation and application of the SLM system
architecture specification, as method mentioned in
section 3, to obtain the specification of the
architecture of the SLM system that will monitor the
quality of the Wireless Blood-glucose Monitoring
(WBgM) system.
In order to specify SLM system architectures for
wireless telemedicine applications, it is important
that professionals with knowledge of business,
operations and technology are involved. In this case
study, three separate human resource elements must
work together in this development, the Diabetes
Management Team (DMT), the Health Care
Administration Team (HCAT), and the Computer
Support Team (CST). Although each organization
will differ in the composition of these teams,
members of the DMT typically can include the
patient, the primary care physician, an
endocrinologist, nutritionist, physical therapist,
ophthalmologist, cardiologist, and support staff. The
HCAT can include office managers, database
administrators, accounting personnel, insurance
liaisons, and medical ethicists. The CST can include
WBgM design, development, technical support
teams and data center operations.
5.1 Business Modelling
First, it is necessary to obtain a common
understanding of the business, services and what
goals to achieve with the SLM solution.
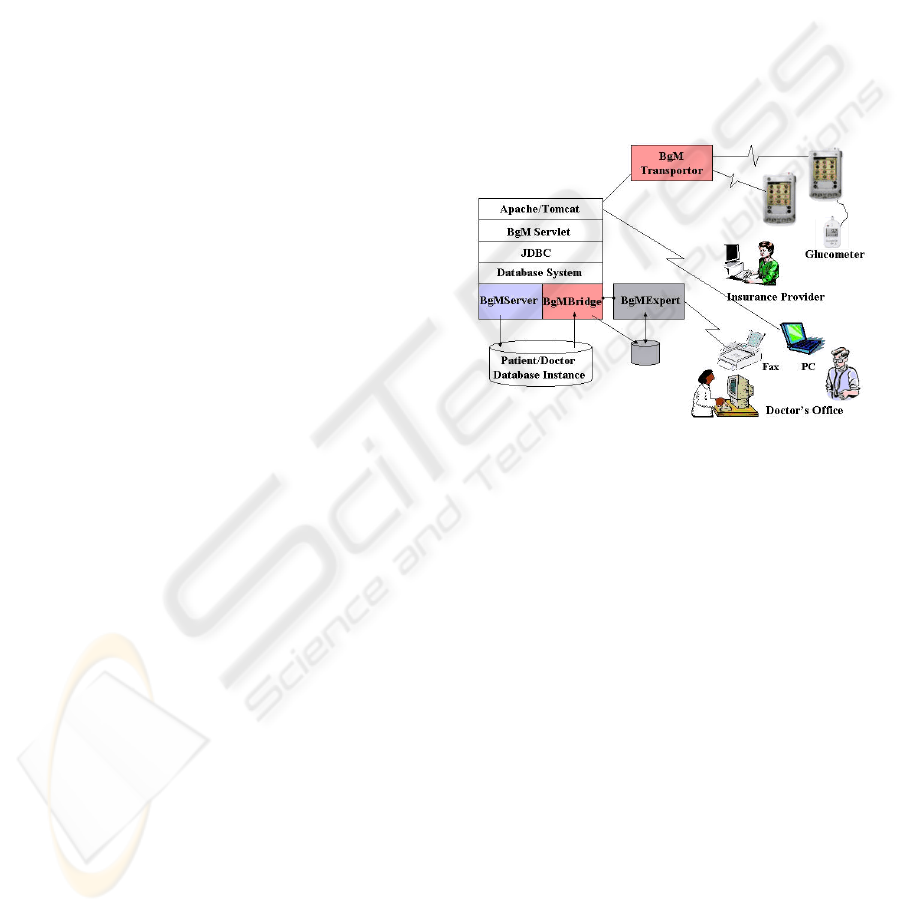
The user may input data from his/her meter
manually or automatically to a wireless device for
upload to a secure cross-platform Internet database.
The user may also (1) input service request
parameters to view current and historic data on the
local device, (2) activate the master Expert System
program that runs on the laboratory computer to
analyze data, (3) email a report from the Expert
system to a recipient doctor's office. The WBgM
electronic transactions consist of a simple set of
formatted data that represents (a) patient profile such
as patient identities, names and contact addresses,
(b) biometric data represented with time-stamped
blood-glucose reading and coded nutrition
characteristics uniformly accepted in the medical
practice, and (c) doctor profile similar to patient
profile. All the data entries and access to them are
coded based on the ANSI SQL standard relational
database format.
Figure 1: DMT business model
The overall objectives of the DMT are to
facilitate the regulation of patient BGL at or near
normal levels. Research has shown that the
following procedures can help reach this goal:
a) Exchange accurate BGL data between patient
and DMT.
b) Increase timeliness and frequency of BGL data
exchange.
c) Provide patient interim self-care diagnostic
information between office visits.
d) Improve the dynamics of data distribution
among members of the DMT.
e) Reduce complexity of equipment connectivity
apparatus.
f) Reduce complexity of data analysis software.
The overall objective of the HCAT is to ensure
that the WBgM adheres to accepted health care
protocol and administrative practices.
WBgM’s database architecture allows the
registered patient to grant access to her/his profile
and blood-glucose readings to a particular set of
members of the DMT. The DMT registration is
verified by the system administrator. Furthermore,
clinical researchers at authorized institutions can
access the patient data once given permission from
WIRELESS TELEMEDICINE AND SERVICE LEVEL MANAGEMENT ARCHITECTURE SPECIFICATION
73

the DMT and patient. This allows the researchers to
conduct studies on diabetes across the patients, not
bound by a particular doctor or hospital. The
certificate method of authentication will build a
chain of trust electronically for the clinical studies,
and the patient is guaranteed the right to revoke the
granted access to the doctors (which in turn revokes
associated researcher’s access) at any time. The
objectives of the HCAT are to:
a) Ensure the security of patient confidential data.
b) Facilitate the addition or removal of members of
the DMT.
c) Facilitate the addition or removal of data-access
privileges of members of the DMT.
d) Reduce costs associated with diabetes
management.
e) Reduce the incidence of fraud and abuse related
to patient records.
f) Facilitate inter-institutional data sharing for
research purposes.
g) Facilitate compliance with local, state, and
federal laws.
The overall objective of the CST is to ensure that
industry best practice methods are used. The CST
should address the same business objectives listed
for the DMT and HCAT above. The specific
objectives of the CST are to:
a) Measure services resources utilization and
performance
b) Measure service usage time
c) Measure service outage time
d) Deliver usage reports to HCAT
e) Implement new designs and/or configurations
based on requests from the DMT and the HCAT
These specific objectives listed above refer to two
sets of performance parameters: those of the WBgM
system, and those of the CST technical support and
development teams. These parameters in turn
directly impact the WBgM service level.
In the following sections, an SLM system
architecture will be specified that will measure
WBgM service level.
5.2 Service Modelling
From the business model, it is possible to elaborate a
service model. As stated in the previous section, the
WBgM service level can be measured by monitoring
WBgM system’s performance and CST technical
support and development teams’ performance.
Table 1: WBgM related services resources
Service Service Resource
WBgM system WBgM Server application
WBgM Expert application
WBgM Database system
WBgM Apache/Tomcat
WBgM Server machine
WBgM Expert machine
CST helpdesk Helpdesk system
ISP connection Router
In order to elaborate an appropriate WBgM
services model, it is necessary that CST identify
what services that compose the WBgM service
needs to be monitored. Table 1 shows a list of
services and services resources needed to deliver the
CCNY implementation of WBgM.
Figure 2: Service model
Figure 2 shows a generic service model. Each
service listed in Table 1 is a service element that
composes another service element called “WBgM”.
Each service uses one or more service resources. ISP
connection services and outsourced helpdesk
services are usually sold with SLAs. It is interesting
to the CST that the SLM system also monitors these
services to ensure that service providers are
respecting the agreed service levels.
5.3 QoS characteristics identification
For each service to be monitored, it is possible to
identify relevant QoS characteristics to achieve each
business objective. DMT and HCAT business
objectives identified in the previous section were
divided into three areas: communication, clinical
utility, and security. This classification is useful for
the CST to address these objectives in the WBgM
system design. Tables 2 to 4 describe how each of
these objectives will be achieved with the CCNY
WBgM solution.
Subjective feedback from the DMT, HCAT and
the system end users can be used to measure how
expectations were fulfilled. DMT, HCAT and CST
must decide whether WBgM SLM system will
manage end customers feedback or not.
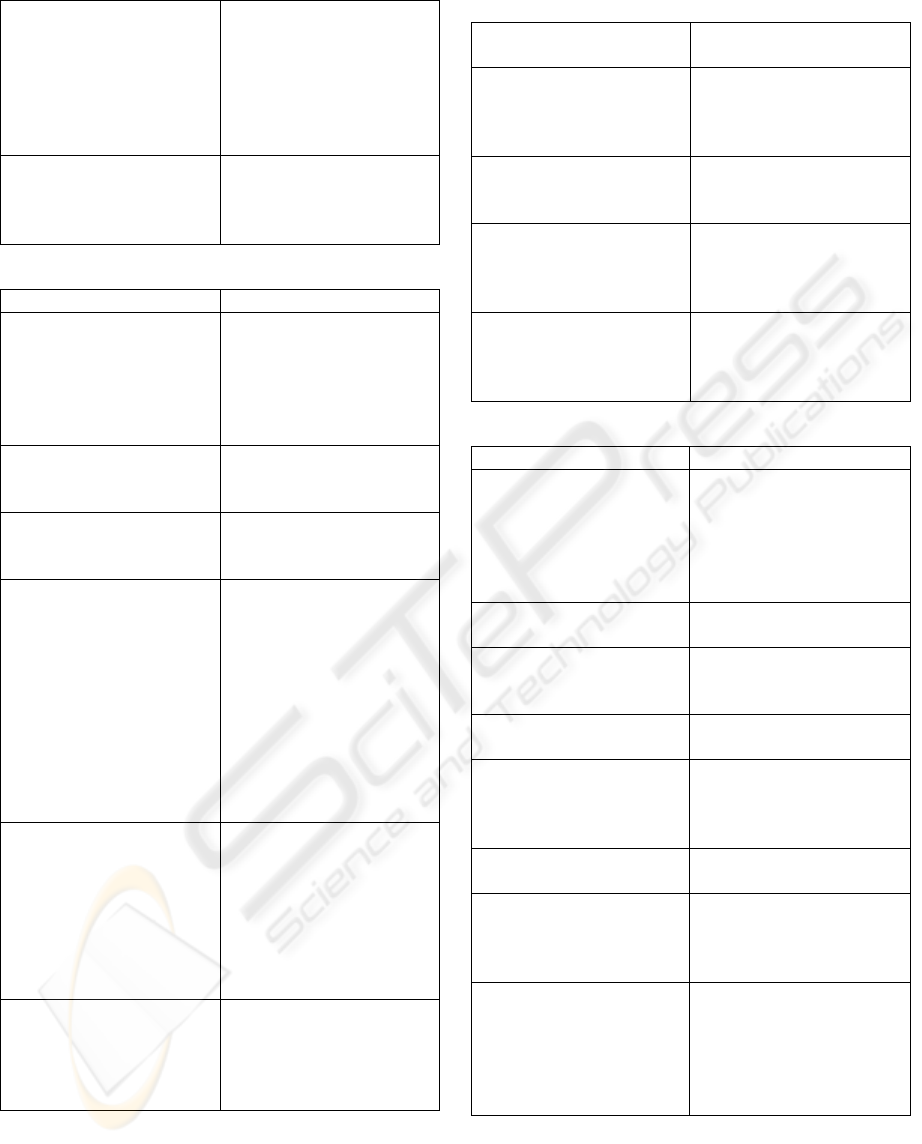
Table 2: Communication objectives
Objective How will be achieved
Exchange accurate BGL data
between patient and DMT
CCNY WBgM solution obtains
exact measure of patient. It is
also necessary to guarantee the
data integrity.
Improve the dynamics of data
distribution among members of
the DMT
WBgM solution with easy
GUIs, high availability,
efficient technical support and
ICETE 2004 - GLOBAL COMMUNICATION INFORMATION SYSTEMS AND SERVICES
74
24x7 communication between
patients and physicians (ex:
leave messages to patients or
physicians on the WBgM
system or send messages to
their email or mobile in case of
urgency).
Reduce complexity of
equipment connectivity
apparatus
WBgM solution with easy
GUIs (few and simple steps)
and apparatus and software
configuration.
Table 3: Clinical utility objectives
Objective How will be achieved
Increase timeliness and
frequency of BGL data
exchange
To encourage patients to send
their BGL more frequently, the
process of sending and
measuring BGL must be simple
and executable in an acceptable
amount of time and cost.
Provide interim selfcare
diagnostic information to the
patient between office visits
BgMExpert module provides
patients selfcare diagnostic
information and guidelines.
Reduce complexity of data
analysis software
WBgM solution itself cannot
reduce complexity of data
analysis software.
Reduce costs associated with
diabetes management
Patients’ quality of live is
improved and costs associated
with diabetes management will
be reduced, because patients
are able to have selfcare
diagnostic information, contact
physicians when needed, the
number of patients with
hypoglycaemia or other
diabetes related complications
decreases.
Facilitate inter-institutional data
sharing for research purposes
Since patient’s profile and
health information are solely
owned by the patient, patients
must grant researchers access to
his/her information in the
WBgM system. Data sharing is
also facilitated if WBgM
system has open interfaces.
Facilitate compliance with
local, state, and federal laws
WBgM solution must be
designed to comply with
existent laws. Solution must be
flexible enough to be able to
implement new requirements.
Table 4: Security objectives
Objective Security services to be
implemented
Ensure the security of
patient confidential data
Confidentiality, access
control, non repudiation,
data integrity and
authentication
Facilitate the addition or
removal of members of the
DMT
Access control, non
repudiation and
authentication
Facilitate the addition or
removal of data-access
privileges of members of
the DMT
Access control, non
repudiation and
authentication
Reduce the incidence of
fraud and abuse related to
patient records
Confidentiality, access
control, non repudiation,
data integrity and
authentication
Table 5: QoS characteristics for CCNY WBgM
Service Resource QoS characteristics
WBgM Server application - Availability
- Service response time
- Number of connected
users
- User connection time
- Number of user operation
WBgM Expert application - Availability
- Service response time
WBgM Database system - Availability
- Hard disk utilization
- Transactions rate
WBgM Apache/Tomcat - Availability
- Service response time
WBgM Server machine - Availability
- CPU utilization
- Hard disk utilization
- Memory utilization
WBgM Expert machine - Availability
- Service response time
Helpdesk system - Availability
- Num of tickets opened
- Average time to close a
ticket
Router - Availability
- CPU utilization
- Bandwidth utilization
- Memory utilization
- Interface errors
- Interface discards
WIRELESS TELEMEDICINE AND SERVICE LEVEL MANAGEMENT ARCHITECTURE SPECIFICATION
75

Relevant QoS characteristics to be monitored by
the SLM system were listed to achieve CST business
objectives (Table 5).
5.4 QoS and SLA modelling
Figure 3: Generic QoS model
Figure 4: Generic SLA model
The QoS characteristics in terms of specific
business goals identified in the previous section will
allow two specific models to be generated by the
professionals involved. First, the QoS model is
shown in Figure 3. It refers to the linkages between
services and tuneable quality aspects of the system.
In this way, feedback with regard to one or a number
of specific service elements may be directly related
to a QoS characteristic that may be adjusted to
improve user satisfaction. The second, the SLA
model shown in Figure 4, represents a configuration
that relates services with users. The SLA model is
necessary so that the effect on end users of any
changes in services resulting from modification of
QoS characteristics may be traced.
5.5 Monitoring definition
Proceeding from the SLA model, professionals with
operational and technology knowledge (HCAT and
CST) will then identify appropriate monitoring
thresholds for the monitored characteristics. These
professionals will then design and develop
appropriate monitoring systems that will record and
report the status of the key characteristics.
5.6 Report generation definition
It is necessary to define what reports and how they
will be generated and delivered to users. DMT,
HCAT and CST must then define what kind of
reports will be generated by WBgM SLM system.
5.7 Accounting definition
In order to charge customers according to
established SLAs, it is necessary to define the
integration of the SLM system with the billing
system. WBgM service is not a commercial product
yet and some of WBgM service provider’s services
could be outsourced. WBgM solution users could be
charged for its use according to SLAs and WBgM
service provider’s outsourced services need to be
monitored to verify if delivered services adhere to
established SLAs. It will be a significant advantage
to future development that the WBgM system have
open interfaces to facilitate integration with
accounting management systems.
5.8 SLM architecture specification
Figure 5: WBgM SLM system architecture
The cumulative result of these 7 steps is the SLM
architecture specification. Beginning with the goal
ICETE 2004 - GLOBAL COMMUNICATION INFORMATION SYSTEMS AND SERVICES
76

of adhering to RM-ODP principles, through
identification of QoS characteristics, and
establishment of the SLA model, a clear
specification for an SLM system architecture is
realized. Figure 5 shows an example of an SLM
system architecture for the CCNY WBgM solution.
6 CONCLUSION
This paper described the detailed study and the use
of USP RM-ODP based method of SLM system
architecture specification to monitor telemedicine
solutions. In particular, the SLM specification for
the CCNY WBgM system.
Advances in wireless communications and
devices continue to revolutionize our way of living.
Wireless telemedicine extends telemedicine
application possibilities and promises to benefit a
large number of people. In some areas of the globe,
wireless telecommunication has been introduced in
advance of wired technology. Wireless healthcare
applications can have a tremendous positive
influence in these developing areas. The
development of these wireless telemedicine
applications can make use of both wireless and
wired infrastructure and services. However, the
success of telemedicine applications will have a
critical dependence on the overall performance of
member services that comprise the solution.
Flexibility, distribution, interworking and
interoperability are important features that derive
from the ODP-based method of SLM specification
and architecture design for telemedicine
applications. The fate of a given wireless application
will dep end strongly on the designers’ ability to
adhere to a rigorous and robust ODP design that can
be successfully monitored for QoS by the
specification of an appropriate SLM system.
REFERENCES
Myers, B.A., Michael, B., Handheld Computing. IEEE
Computer, 2003. 36(9).
Lin, J.C., Applying Telecommunication Technology to
Healthcare Delivery. IEEE EMB Magazine, 1999.
18(4): p. 28-31.
Tacharka, S., Istepanian, R., Bansitas, K. Mobile E-
Health: The Unwired Evolution of Telemedicine. in
Proceedings of HealthComB. 2001. Italy.
de Sonnaville, J.J., M. Bouma, L.P. Colly, W. Deville, D.
Wijkel, and R.J. Heine, Sustained good glycaemic
control in NIDDM patients by implementation of
structured care in general practice: 2-year follow-up
study. Diabetologia, 1997. 40(11): p. 1334-40.
Fund, M.M., Patients as effective collaborators in
managing chronic conditions, in Center for the
Advancement of Health. 1999, Milbank Memorial
Fund: New York.
Pattichis, C.S., E. Kyriacou, S. Voskarides, M.S. Pattichis,
R. Istepanian, and C.N. Schizas, Wireless telemedicine
systems: An overview. IEEE Antennas and
Propagation Magazine, 2002. 44(2): p. 143-153.
Watchter, G., Hospital Unplugged: The Wireless
Revolution Reaches Healthcare, retrieved from
Telemedicine Information Exchange (TIE)
Telemedicine 101 – Telemedicine Technology
Topics:, on February 9, 2004,
http://tie.telemed.org/telemed101/topics/wireless.pdf
Chalmers D., S., M., A Survey of Quality of Service in
Mobile Computing Environments, retrieved from IEEE
Communications Surveys, on February 9, 2004, IEEE,
http://www.consoc.org/livepubs/surveys/public/2q99is
sue/sloman.html.
Hu, F., Sharma, N.K., A Priority-determined Multi-Class
Handoff Scheme with Guaranteed Mobile-QoS in
Wireless Multimedia Networks, retrieved from IEEE
Transactions on Vehicle Technology, on February 9,
2004, IEEE,
http://www.ce.rit.edu/%7Efxheec/ieee_veh.pdf
Lewis, L., Service level management for enterprise
networks. 1999, Norwood: Artech House.
Miyata, C.M., Becerra, J.L. An ODP Vision of QoS
Management: An application in the SLM Architecture.
in 1st International Conference on Software
Engineering Research and Practice. 2003.
Kawaguchi, A., Russell, S., Qian, G. Developing a
Wireless Blood-Glucose Monitoring System: Concept
and Practice. in 7th World Multiconference on
Systemics, Cybernetics and Informatics (SCI2003).
2003. Orlando, Florida: IEEE.
Vigersky, R.A., E. Hanson, E. McDonough, T. Rapp, J.
Pajak, and R.S. Galen, A wireless diabetes
management and communication system. Diabetes
Technol Ther, 2003. 5(4): p. 695-702.
Sadeghi, B., Knightly, E.W., Architecture and Algorithms
for Scalable Mobile QoS, Wireless Networks 9,
retrieved from Rice University, on February 27, 2004,
http://www-
ece.rice.edu/networks/papers/SaKnWinet03.pdf
Kawaguchi, A., S. Russell, and G. Qian. Security Issues in
the Development of a Wireless Blood-Glucose
Monitoring System. in the 16th IEEE Symposium on
Computer-Based Medical Systems. 2003. New York,
NY.
Parasuraman, A., L.L. Berry, and V.A. Zeithaml,
SERVQUAL: A multiple-item scale for measuring
customer perceptions of service quality. Journal of
Retailing, 1988. 64(1): p. 12-40.
WIRELESS TELEMEDICINE AND SERVICE LEVEL MANAGEMENT ARCHITECTURE SPECIFICATION
77

Hill, N., Handbook for Customer Satisfaction
Measurement. 1996.
Vavra, T.G., Improving Your Measurement of Customer
Satisfaction: A Guide to Creating, Conducting,
Analyzing, and Reporting Customer Satisfaction
Measurement Programs. 1997.
ICETE 2004 - GLOBAL COMMUNICATION INFORMATION SYSTEMS AND SERVICES
78
