
AN AGENT BASED INFRASTRUCURE FOR FACILITATING
EVIDENCE BASED MEDICINE
Jennifer Sampson
Department of Computer and Information Science, Norwegian University of Science and Technology,Trondheim, Norway.
Ke
ywords: Multi-agent system, Evidence-based medicine
Abstract: Evidence-based medicine relies heavily on the timely dissemination of ‘best evidence’ to a wide audience of
health practitioners (Atkins and Louw, 2000). However, finding, assimilating and using this information
resource effectively can be difficult. In this paper we describe an infrastructure for facilitating evidence-
based health care using Agora - a multi-agent system. This paper discusses a new application for AGORA,
and also describes issues for disseminating such medical knowledge via an adaptive, intelligent, distributed,
mobile information service. We describe how an agent based approach can deliver clinical cases and
diagnosis information to clinicians at point of care tailored to her/his needs. This research in progress is
particularly important for the facilitating flow of information in health care.
1 INTRODUCTION
We are developing a multi-agent system to assist
with diagnosis decision making in health care using
mobile devices. This paper discusses an application
to AGORA, a multi-agent system, for disseminating
such medical knowledge via an adaptive, intelligent,
distributed, mobile information service. One of the
aims of the project is to provide a novel solution for
information service provision and selection for users
of mobile devices. The application of mobile
technology in this domain will involve the use of
software assistant agents to proactively
communicate availability of relevant clinical cases
to clinicians. The software agent will also
communicate with other software agents to make
informed decisions based on specific patient medical
results and documented medical research. This
research in progress is particularly important for the
facilitating flow of information in health care.
The overall research goal is to provide an
‘intelligent’ solution to medical services provision
through the use of agent assistants. The project is to
use agent technology to proactively communicate
availability of relevant clinical cases to clinicians
and provide personalised information tailored to
meet the clinician’s needs. We are particularly
interested in promoting a way to disseminate clinical
case reporting for diagnosis.
2 MOTIVATION
Previous research in the domain of evidence based
medicine and multi-agent systems (MAS) have
focused on information agents and appropriate
information retrieval methods (Abasola and Gómez
2000). We propose extending this work by using
agent technology to proactively communicate
availability of relevant clinical cases to clinicians
and provide personalised information tailored to
meet the clinician’s needs.
We are using an intelligent agents approach for
disseminating medical research knowledge via an
adaptive, intelligent, distributed, mobile information
service. By adaptive we mean the ability of the
service to adapt to the health professionals, service
providers and communication context. By intelligent
information services we understand ability of service
to employ planning, reasoning and knowledge
processing in order to satisfy the health professionals
requirements. An important intelligent feature of the
service is its pro-activity - ability to predict users’
needs and to take initiative. The pro-activity of the
service should be based on exploiting and (when it is
not available) building the health professionals
and/or service provider models by using machine
learning and inductive inference techniques. By
distributed information service we mean that
components of the service system can be distributed
493
Sampson J. (2004).
AN AGENT BASED INFRASTRUCURE FOR FACILITATING EVIDENCE BASED MEDICINE.
In Proceedings of the Sixth International Conference on Enterprise Information Systems, pages 493-496
DOI: 10.5220/0002657804930496
Copyright
c
SciTePress
across the network and that service can be composed
from these components. By mobile information
service we assume that both heath professionals and
service providers can employ mobile devices such as
mobile phones and PDAs for requesting/provision of
an information service. Currently we are developing
a prototype solution using Agora a multi-agent
system infrastructure. Future research will be
focused on the use of mobile devices to support the
dissemination of the service. A multi-agent system
infrastructure may include different levels and
components, however currently we are focused on
the cooperative work component in the
infrastructure which we consider to be at MAS
middleware level. An additional complicating factor
is the use of mobile devices for communicating
medical information to clinicians.
Due to the increasing number of mobile portable
devices in use opportunities for the development of a
wide range of mobile information services exists.
Matskin and Tveit (2003) comment that the
development of such technology as WAP (and other
mobile technology) makes it possible to provide
users of mobile phones with access to the Internet
and services which earlier were available only via
PCs connected to the Internet. The application of
mobile technology in the healthcare domain will
involve the use of software assistant agents to
proactively communicate availability of relevant
clinical cases, evidence-based research and patient
data to clinicians. The software agent will
communicate with other software agents to make
informed decisions based on specific patient medical
results and documented medical research. However
Matskin and Tveit (2003) note that mobile devices
have severe restrictions that may complicate
practical use of information services. These
restrictions are largely due to the limitations of
wireless data networks compare to wired networks
(less bandwidth, more latency, less connection
stability, less predictability and less standardized
protocols) and to the limitations of mobile handsets
compared to personal computers (small screen size,
complicated text input, limited memory, slow CPU
and more constrained energy supply).
We envisage necessary requirements for the
services are simplicity and expressiveness of the
services. It is possible that some of the limitations
will be relaxed in the future by development of
hardware or telecommunication networks
technology but at the moment we shall consider
these impediments when implementing mobile
services. Services should be personalized - they
should take into account changing healthcare
professional’s preferences. Thirdly, services should
be able to adopt both to changes in the healthcare
professionals preferences and in the context of
communication (Matskin and Tveit, 2003). In
addition we will assume that as much as possible
work for service customization and provision should
be done off-line without direct participation of the
user of the mobile device.
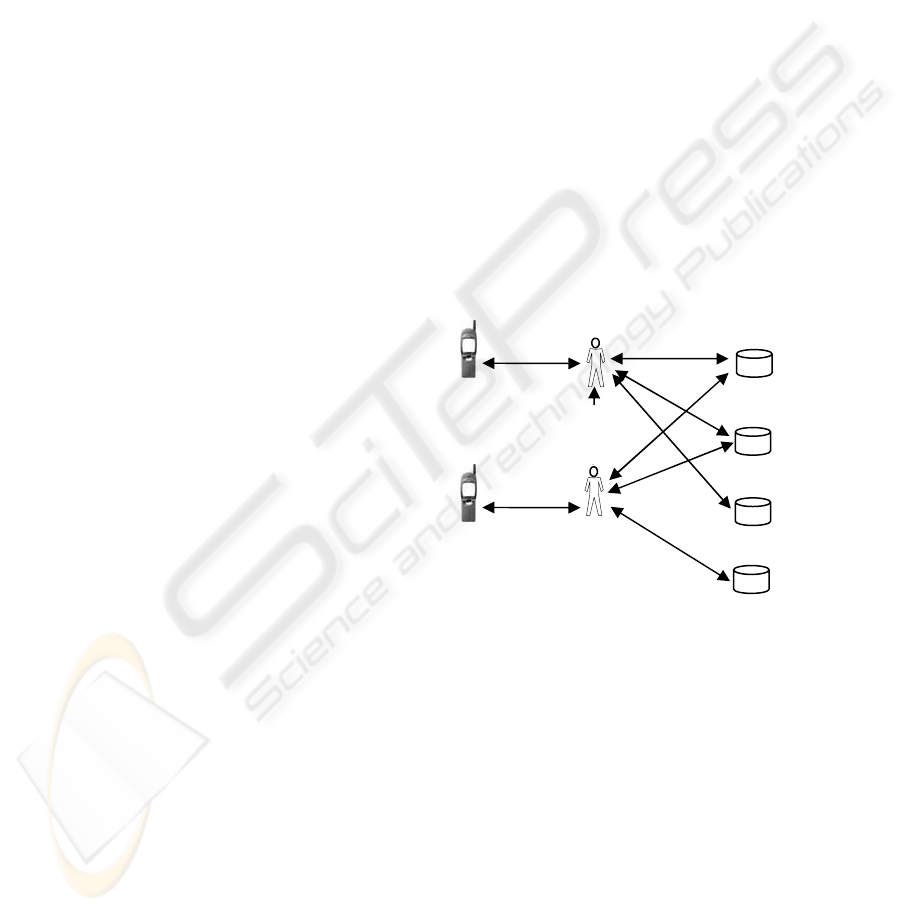
Each clinician should be able to present his or her
case profile by telling the EBM assistant specific
patient case information and define specific areas of
expertise. The confidentiality of the patient will be
adhered to through the means of agents who own the
sensitive patient data, this information will not be
released to other agents and is what we describe as
secret knowledge. The application is to facilitate
health care practice by providing relevant feedback
information regarding diagnosis and treatment
information based on similar cases via a mobile
service. This technology may be useful for doctors
treating patients where it is not suitable for patients
to attend a clinic, in this situation a remote check,
communication or diagnosis is essential. We foresee
that it should be possible to create certain default
profiles for specific types of health care professional
and case types.
Figure 1 depicts our high level
concept from an individual perspective.
3 THE AGORA CONCEPT
We are using AGORA as a prototype environment
for the development of an agent-based system for
facilitating evidence-based health care. Matskin et
al. (2001) have developed and successfully tested
the AGORA system in other domains such as e-
commerce. Our research is to modify the
architecture for use in the health care domain, in
particular for facilitating the dissemination of
clinical cases to clinicians. While AGORA has been
successfully used for virtual enterprises (Rao and
Petersen 2003) we recognise that it is necessary to
EBM internet
resources
EBM agent
assistant
Clinician
with WAP
phone/PDA
Clinician
with WAP
phone/PDA
Electronic
health
record
Medline
database
Cochrane
database
EBM
agent
assistant
Figure 1: Agent-based solution for evidence-based
healthcare
ICEIS 2004 - ARTIFICIAL INTELLIGENCE AND DECISION SUPPORT SYSTEMS
494

modify the architecture and underlying knowledge
base design to be appropriate for use in the
healthcare domain.
The term ‘Agora’ originating in Greece, is the
public forum and market place, where people
gathered to discuss politics, news, exchange views
etc. Similarly, agent Agoras are places where the
agents arrive to communicate, negotiate, coordinate,
collaborate and trade information and services
(Matskin et. al. 2001). We have used the Agora
metaphor in the development of a multi-agent
system which consists of a set of interconnected
Agoras and agents. Default agents are attached to an
Agora while the other agents are registered at an
Agora (Matskin et. al. 2001). The Agora system
allows where possible agents to register and present
activities. A matchmaker inside the agora compares
the activities, and if two or more activities match, a
negotiation agent will be started. This negotiation
agent will manage the negotiation between these
agents. The idea is that agents interested in some
topic can find an Agora that operates in the specific
domain, and then receive services and information
through the Agora. The registered agents suggest
that agents that want to "participate" in an Agora
have to be registered first. The agent will then
advertise themselves, and the Agora will help this
agent to find other agents and Agoras that may help
the agent to carry out tasks. Default agents are
agents that are bound to the Agora to perform some
services for the Agora. These agents may be
performing services like negotiation, coordination,
registration, or for example offering access to a
database. It is possible for agents to be registered at
several Agoras and that there could be interrelations
between Agoras (Matskin et. al. 2001).
Agora has been developed using Java, and
JATLite is used as a tool for communication
(Matskin et. al. 2001). Prior research has found that
it possible to run more than 70 agents concurrently
on the JATLite router. KQML is used as the basic
external communication language and protocol for
exchanging information and knowledge. A separate
communication format Message Wrapper has been
defined inside the agents and Agoras. Between the
internal format and the external KQML language
there is a translator. We are now using this translator
to use FIPA instead of KQML, by building a new
FIPA translator.
3.1 Using AGORA for facilitating
evidence-based heath care
The main advantage with the Agora approach is that
the agents have rather simple implementations
because of the gathering of specially designed
services and functionality inside the Agoras. In such
an application agents will represent the clinicians,
the case events and the evidence based medicine
service providers. In order to implement a virtual
health care Agora we first identify participants of the
cooperative work. We are interested in the roles
specific agents will undertake.
• Clinician agent - represents the medical
professional, at this point of time we only
consider practitioners of medicine who undertake
clinical work.
• Active case agent – represents a clinical case
currently under care
• Completed case agent – represents published
clinical case reports
• Case manager agent – a coordinator of cases and
clinicians in a health care environment.
• Diagnosis negotiation assistant agent –
matchmaking active case with other cases
• Cochrane library collaborator agent – manager of
the agents representing specific health domains.
Cooperative points for agents work in the health care
domain can be identified, as follows:
• Coordination of the health care activity
• Coordination of different clinician agents
• Coordination (information gathering) and
diagnosis support between a case manager agent
and the Cochrane library agents.
These cooperative points can be mapped into the
following set of agoras: a clinician agora, a case
agora, a diagnosis agora and a cochrane
collaboration agora.
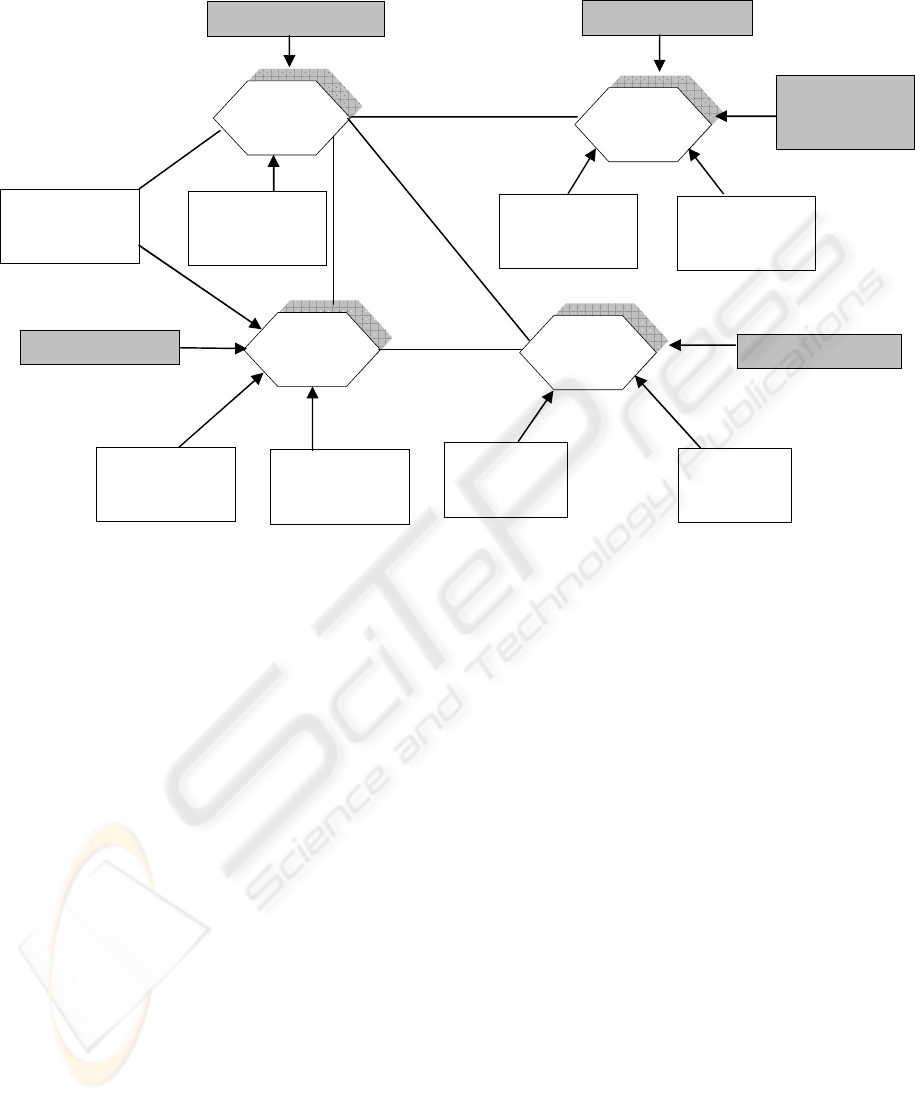
Agora represents both registered and default
agents (refer Figure 2). Registered agents are either:
coordination agents, negotiation agents or
participant agents. The first two types of agents
manage coordination and negotiation activities to be
performed at the corresponding Agora. The
participant agents represent participants of the
cooperative activity. The default agents in Agora are
the Agora manager, service and matchmaking
agents. Each participant agent (for example case
agent) presents offers and requests for information.
Offered activity (OA) may be any activity the agent
can perform by itself, for example in the heath care
domain an offered activity could diagnosis
information offered by the diagnosis assistant agent.
Interrelations and connections among agents and
Agoras are depicted at Figure 2. Lines between
Agoras mean that agents from connected Agoras can
be registered on both of them. Each Agora is
shadowed as there is more than one Agora of each
type. The coordination agents manage corresponding
protocols.
AN AGENT-BASED INFRASTRUCTURE FOR FACILITATING EVIDENCE BASED MEDICINE
495
Wanted activity (WA) could be any requested
information from clinician agents regarding clinical
cases. Agora allows direct matching of OA and WA;
however we are currently overriding this default
matchmaking using semantic matchmaking and
ontological analysis. This is an important issue in
clinical case matching, we are employing fuzzy
matching techniques, where the matching procedure
is not so precise or complete (80%/50%). Another
important consideration is the composition of cases,
we are determining the efficacy of service
composition in this domain. Each of the agents in
the Agora platform has the following modules: goal
analyser, knowledge base, planner (in XML),
scheduler, action creator and communication
threads. We are currently working on defining the
ontology for the knowledge base module of the case
and diagnosis agents. The knowledge base module
maintains storage, retrieval and querying knowledge.
CONCLUSION
The platform described in this paper was previously
developed using the Agora concept for facilitating
cooperative work. Our research is towards using
Agora for facilitating the dissemination of medical
knowledge and for assisting diagnosis in a clinical
setting.
REFERENCES
Abasola, J. and Gómez, M. (2000). “MELISA. An
ontology-based agent for information retrieval in
medicine”, Proceedings of the First International
Workshop on the Semantic Web (SemWeb2000).
Atkins, C. and Louw, G., 2000. Reclaiming Knowledge: A
case for evidence-based Information Systems. In Proc.
8th European Conference on Information Systems.
Matskin, M., Divitini, M., Petersen, S.A., 1998. AGORA:
a Multi-Agent Support for Distributed Information
Technology Applications', In, NIK'98.
Matskin, M. Kirkeluten, O. J. Krossnes, S.B. Sæle, Ø.,
2001. Agora: An Infrastructure for Cooperative Work
Support in Multi-Agent Systems. Wagner, T. and Rana
O.F.(Eds.): Infrastructure for Agents, Springer-Verlag
Matskin, M. and Tveit, A., 2003. Software Agents for
Mobile Commerce Services Support. K. Siau (ed.).
Readings in Database Management. Idea Group.
Rao, J. and Petersen, S., 2003. Implementing Virtual
Enterprises Using AGORA Multi-agent System. In
Proceedings of CAiSE 2003 Forum.
Diagnosis
Agent N
Clinician
Agora
Coordinati
on Agent
Figure 2: Virtual Health Care AGORA
Case
Agora
Case Agent
N
Clinician
Agent N
Clinician
Agent 1
Coordination Agent
Coordination Agent
Case Agent 1
Cochrane
Collaboration
Agora
Cochrane
Agent 1
Cochrane
Agent N
Coordination Agent
Case
Manager
Agent
Diagnosis
Agent 1
Diagnosis
Agora
ICEIS 2004 - ARTIFICIAL INTELLIGENCE AND DECISION SUPPORT SYSTEMS
496
