
MEDIS – A WEB BASED HEALTH INFORMATION SYSTEM
Implementing Integrated Secure Electronic Health Record
Snezana Sucurovic
Institut Mihailo Pupin, Volgina 15, Belgrade,Serbia and Montenegro
Keywords: Electronic Health Record (EHCR), Security, Privacy.
Abstract: In many countries there are initiatives for building an integrated patient-centric electronic health record.
There are also initiatives for transnational integrations. These growing demands for integration result from
the fact that it can provide improving healthcare treatments and reducing the cost of healthcare services.
While in European highly developed countries computerisation in healthcare sector begun in the 70’s and
reached a high level, some developing countries, and Serbia and Montenegro among them, have started
computerisation recently. This is why MEDIS (MEDical Information System) is aimed at integration itself
from the very beginning instead of integration of heterogeneous information systems on a middle layer or
using HL7 protocol. MEDIS has been implemented as a federated system where the central server hosts
basic EHCR information about a patient, and clinical servers contain their own part of patients’ EHCR.
Clinical servers are connected to a central server through the Internet and the system can be accessed
through a browser from a place that has an Internet connection. A user also has to have a public key
certificate to be able to login. As health data are highly sensible, MEDIS implements solutions from recent
years, such as Public Key Infrastructure and Privilege Management Infrastructure, SSL and Web Service
security as well as pluggable, XML based access control policies.
1 INTRODUCTION
MEDIS is based on European Committee for
Standardisation standards ENV 13606 (CEN, 2002)
and ENV 13729 (CEN, 2002), where the former
defines architecture of EHCR, and the latter secure
authentication. Applying these standards provides
interoperatibility and their component-oriented
architecture is suitable for distributed systems such
as MEDIS. CEN ENV 13606 standard named
“EHCR Communication” is a high level template
which provides a set of design decisions which can
be used by system vendors to develop specific
implementations for their customers. The main item
in CEN architecture standard is an Architectural
Component. The Architectural Components are
organised in a hierarchical structure. For a patient,
there is a Root Architectural Component which
represents a folder of patient record in the system
and contains the basic information about a patient.
On the other hand, there is a Record Component
established by original component complexes
(OCCs), selected component complexes (SCC), data
items (DI) and link items (LI). An OCC comprises
(according to data homogeneity) four basic
components: folders, compositions, headed sections
and clusters. A SCC contains a collection of data
representing an aggregation of other record
components that is not determined by the time or
situation in which they were originally added to the
EHCR. It may contain a reference to a set of search
criteria, a procedure or some other query device
whereby its members are generated dynamically
(actually a distributed query, for example “current
medication”). A Link Item is a component that
provides a means of associating two other instances
of architectural component and specifying the
relationship between them (“caused by”, for
example). A Data Item is a Record Component that
represents the smallest structural unit into which the
content of the EHCR can be broken down without
losing its meaning. A component is in a lower
position in hierarchy if it contains more homogenous
data. An example: Emergency Admission (Folder 1)
> Assessment (Composition 1) >Accident Details
(Section 1)> Causes of accident (Section 2) >
Accident cause, as text (Data Item 1).
Each Architectural Component has reference to
access control policy for that component defined as
a Distribution Rule (Fig. 4). The Distribution Rule
160
Sucurovic S. (2006).
MEDIS – A WEB BASED HEALTH INFORMATION SYSTEM - Implementing Integrated Secure Electronic Health Record.
In Proceedings of the Eighth International Conference on Enterprise Information Systems - ISAS, pages 160-164
DOI: 10.5220/0002444001600164
Copyright
c
SciTePress

comprises classes Who, Where, When, Why and
How which define who, where, when, why and how
is allowed to access the component (Table 1).
Table 1: Distribution Rule objects.
Classes Attributes Type
Who Profession
Specialization
Engaged in care
Healthcare agent
String
String
Boolean
Class
Where Country
Legal requirement
String
Boolean
When Episode of care
Episode reference
Boolean
String
Why Healthcare process code
Healthcare process text
Sensitivity class
Purpose of use
Healthcare party role
String
String
String
Class
Class
How Access method (read,
modify)
Consent required
Signed
Encrypted
Operating system
security rating
Physical security rating
Software security rating
String
Class
Boolean
Boolean
String
String
String
2 THE MEDIS ARCHITECTURE
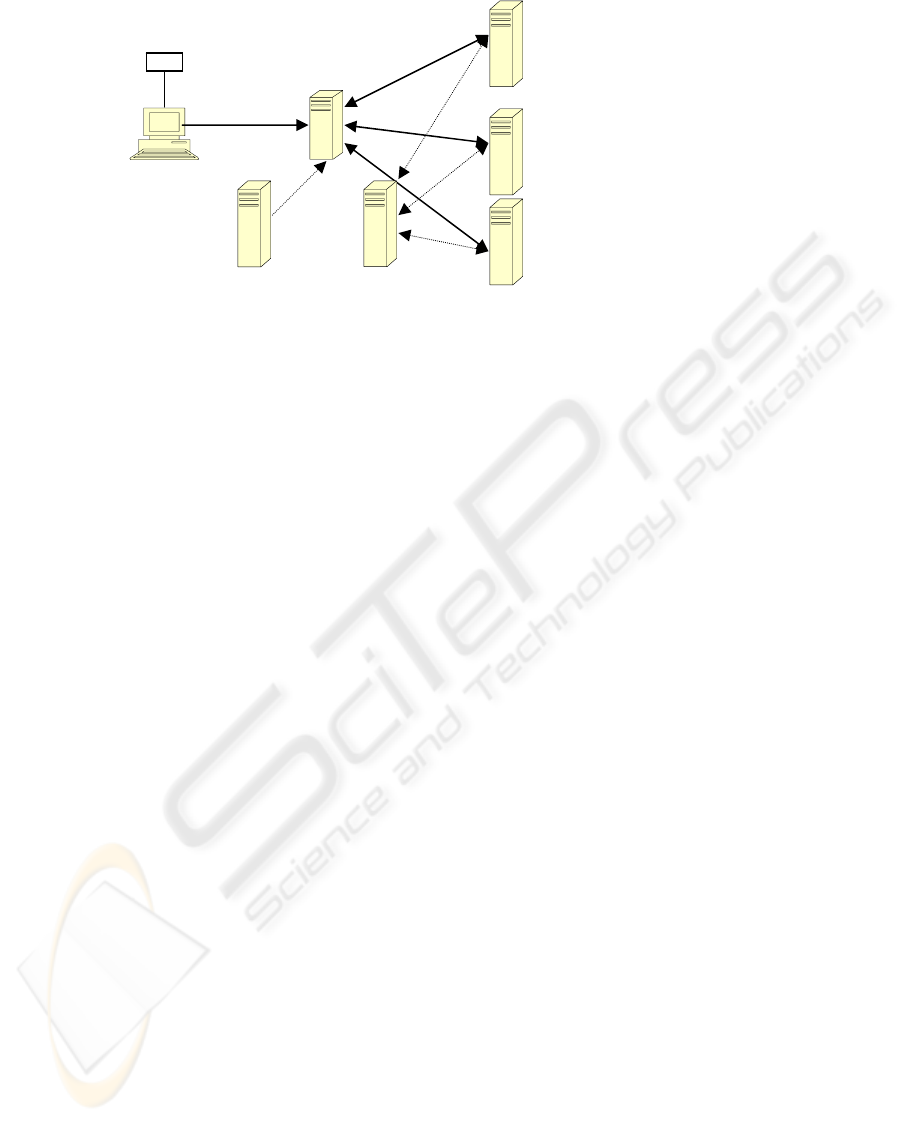
MEDIS has been implemented as a federated
system. Architectural Components are created in
compliance with CEN ENV 13606 and stored there
where they are created – at hospitals and clinics and
are accessed via a central server which contains a
Root component and the addresses of the clinical
and hospital servers. Architectural components that
are hosted on the clinical and hospital servers have
pointers to supercomponents and linked components
(Fig. 1.). HTML pages are created on the central
server and contain five frames: the required
Architectural Component (AC) in the right frame,
links to subcomponents and linked components in
the left upper frame, links to Selected Component
Complex (actually distributed queries) in the left
lower frame, the AC position in the hierarchical
structure of EHCR in the upper frame and
information about a user in the lower frame. (Fig. 2).
A physician can define the position in EHCR (and
therefore HTML page) which will appear when he
requests EHCR for a patient.
In the MEDIS prototype there is an
authentication applet (Sucurovic, 2005) which is
processed in a browser and, after successful
authentication, a HTML page has been generated
using JSPs on the central server. The Clinical
Servers tier has been implemented in Java Web
Services technology using Apache Axis Web
Service server and Tomcat Web Server. Business
logic has been implemented in reusable components
– Java Beans.
3 IMPLEMENTING SECURITY
IN MEDIS
As health data are highly sensitive, security has been
the main item in MEDIS. We’ve implemented
authentication, access control and encryption and, in
that way, we’ve met requirements for privacy and
confidentiality. MEDIS implements solutions from
recent years, such as Public Key Infrastructure and
Privilege Management Infrastructure, SSL and Web
Service security as well as pluggable, XML based
access control policies.
3.1 Authentication
Using a password as a means of verification of
claimed identity has many disadvantages in
distributed systems. Therefore, MEDIS implements
CEN ENV 13 729 (CEN ENV, 2002) which defines
authentication as a challenge-response procedure
using X.509 public key certificates (Sucurovic,
2005). However, MEDIS implements not only
public key certificates management, but also
attribute certificates management (Blobel, 2003),
(Sucurovic, 2006). Originally, X.509 certificates
were meant to provide nonforgeable evidence of a
person’s identity. Consequently, X.509 certificates
contain information about certificate owners, such as
their name and public key, signed by a Certificate
Authority (CA). However, it quickly became evident
that in many situations, information about a person’s
privileges or attributes can be much more important
than that of their identity. Therefore, in the fourth
edition of the X.509 Standard (2000), the definition
of an attribute certificate was introduced to
distinguish it from public-key certificates from
previous versions of the X.509 Standard.
In the MEDIS project X.509 PKCs are supposed
to be generated by public Certificate Authority,
while ACs are supposed to be generated by MEDIS
Attribute Authority. The public key certificates are
transferred to users and stored in a browser. The
attribute certificates are stored on LDAP server,
because they are supposed to be under control of
MEDIS access control administrator. In the MEDIS
approach attribute certificates contain user’s
MEDIS – A WEB BASED HEALTH INFORMATION SYSTEM - Implementing Integrated Secure Electronic Health
Record
161
attributes as XML text. There are two types of
public key and attribute certificates: the Clinicians’
and Patients’ as distribution rules contain a flag
which denotes if the Architectural Component is
allowed to be read from a patient.
3.2 Access Control
In a complex distributed system, such as MEDIS,
access control is consequently very complex and has
to satisfy both fine grained access control and
administrative simplicity. This can be realised using
plugable, component based authorisation policies
(Beznosov, 2004). An authorisation policy is the
complex of legal, ethical, social, organisational,
psychological, functional and technical implications
for trustworthiness of health information system .
One common way to express policy definition is
XML schemadata. These schemes should be
standardised for inter-operatibility purposes (Blobel,
2004). The MEDIS project aims at developing the
authorisation policy definitions, using XML scheme,
which are based on CEN ENV 13 606 Distribution
Rules (CEN 2002).
The MEDIS project has adopted XML as the
language for developing constrained hierarchical
Role Based Access Control and, at the same time,
has focus on decomposing policy engines into
components (Beznosov, 2004), (Zhou, 2004),
(Blobel, 2004), (Chadwick, 2003), (Joshi, 2004).
The MEDIS project authorisation policy has several
components (MEDIS Technical Report, 2005).
First, there is an XML schema of user attributes that
corresponds to the attribute certificate attributes.
User attributes are transfered in SOAP Headers.
Secondly, there are Distribution Rules attached to
each Architectural Component (Fig. 3). Third, there
is an Authorisation Policy on the clinical server. It
defines hierarchies of How, When, Where, Why and
Who attributes (hierarchy of Roles, Professions,
Regions etc). In that way, a hierarchical RBAC can
be implemented, with constraints defined by security
attributes (software security, physical security rating
etc.) and non-security attributes (profession,
specialisation etc.). There are, also, two master
Authorisation Policies. The Master Authorisation
Policy for Hierarchy defines which combination of,
for example, role hierarchy and profession hierarchy
is valid. There is another master Authorisation
Policy – the Master Authorisation Policy for DRs: it
defines which combinations of attributes in a
Distribution Rule are allowed in general and for an
archetype. There is an enable/disable flag, which
defines if the given combination of hierarchies is
enabled or disabled (for the first master
Authorisation Policy) and if the given combination
of attributes in a Distribution Rule has been allowed
or forbidden (for the second master Authorisation
Policy). There are in fact, two administrators: one on
the clinical server and another on the central LDAP
server. In that way, this approach provides flexibility
and administrative simplicity.
As in (Joshi, 2004) grouping information content
into concept clusters reduces complexity of the
specification process and security administration. In
the MEDIS project there is a content based access
control specification on three levels: conceptual,
archetype and instance, i.e. master authorisation
policies can be defined on the conceptual and
archetype level while there are Distribution Rules
related to the Architectural Component, as access
control specification on instance level.
Smart Card
Clinical Server I
Clinical Server II
Clinical Server N
Central
Server
LDAP
Attribute
Certificate
LDAP
Master Authorisation Policy
Figure 1: MEDIS architecture.
ICEIS 2006 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
162

Figure 2: CEN ENV 13606 Composition Component example.
3.3 Encryption
The MEDIS project implements Web Service
security between the clinical and central server and
SSL between the central server and a client
(Microsoft, IBM, 2004). We use Apache's
implementation of the OASIS Web Services
Security (WS-Security) specification – Web Service
Security for Java (WSS4J) (W3C Recommendation,
2002). WSS4J can secure Web services deployed in
most Java Web services environments; however, it
has specific support for the Axis Web services
framework. WSS4J provides the encryption and
digital signing of SOAP messages as well as the
transfer of SAML attributes in SOAP Header. In our
application Attribute Certificate’s attributes are
transferred in SOAP Header. The RSA algorithm
has been chosen for signing and the TripleDES for
encryption. Communication between the browser
and Web Server has been encrypted using SSL.
Currently, Netscape 6 browser and Tomcat 5.0 Web
Server are used and the agreed chiper suite between
them is SSL_RSA_WITH_RC4_128_MD5.
4 CONCLUSION
The aim of MEDIS project is the development of a
prototype of secure national healthcare information
system in which communication is based on the
Internet. Compared to other existing Web based
EHCR the originallity of the MEDIS is CEN ENV
13606 based architecture where Root Component is
hosted on a central server and other components in
hierachy are placed on clinical servers. As health
data are highly sensitive MEDIS implements
solutions from recent years, such as Public Key
Infrastructure and Privilege Management
Infrastructure, SSL and Web Service security as well
as pluggable, XML based access control policies.
The MEDIS project aims at giving contribution to
standardisation of access control policies based on
CEN ENV 13606 Distribution Rules definition. The
MEDIS project aims at contributing to initiatives for
building integrated national and global healthcare
information systems.
MEDIS – A WEB BASED HEALTH INFORMATION SYSTEM - Implementing Integrated Secure Electronic Health
Record
163

REFERENCES
Beznosov K., 2004, On the Benefits of Decomposing
Policy Engines into Components, In. 3
rd
Workshop on
adaptive and Reflect Middleware, Toronto
Blobel B. et. al., 2003, Using a privilege management
infrastructure for secure Web-based e-health
applications, Computer Communications, Elsevier
Blobel B., 2004, Authorisation and access control for
electronic health record system, Intern. Journal of
Medical Informatics, Elsevier, No.73, pp. 251-257,
Chadwick D. et. al., Role based access control with X.509
Attribute Certificates, IEEE Internet Computing,
March/April 2003, pp. 62 – 69
Commite Europen de Normalisation ENV 13606
Standard, 2002, Extended Architecture
Commite Europen de Normalisation ENV 13729
Standard, 2002, Secure user identification
Joshi J. et. al., Access Control Language for Multidomain
Environments, IEEE Internet Computing,
November/December 2004, pp. 40-50.
MEDIS Technical Report, Retrieved September 28,2005
from
http://www.imp.bg.ac.yu/dokumenti/MEDISTechnical
Report.doc
Microsoft and IBM White Paper, Security in Web service
world: A Proposed Architecture and Roadmap,
Retrieved September 28,2005 from http://www-
128.ibm.com/developerworks/webservices/library/ws-
secmap
Sucurovic S., Jovanovic Z., February 2005, Java
Cryptography & X.509 Authentication, Dr. Dobb’s
Journal, San Francisco
Sucurovic S., Jovanovic Z., 2006, Java Cryptography &
Attribute Certificate Management, Dr. Dobb’s Journal,
San Francisco
XML Encryption Syntax and Processing, W3C
Recommendation, 2002
XML Signature Syntax and Processing, W3C
Recommendation, 2002
Wei Z. et. al., 2004, Implement role based access control
with attribute certificates, ICACT 2004, International
Conference on Advanced Communication Technology,
Korea
Architectural Component
Distribution Rule
Who When Why How Where
0..1
0..*
0..* 0..*
Fi
g
ure 4: Distribution Rule
(
CEN ENV 13606 Part 3
)
.
0..*
DRs
Attribute Certificate’s
attributes
Clinical Server
Authorisation Policy
ACs
Master Hierarchy
Authorisation Policy
Master DR
Authorisation Policy
LDAP Serve
r
SOAP Message Header
Access Decision Function
Figure 3: MEDIS access control components.
1..*
ICEIS 2006 - INFORMATION SYSTEMS ANALYSIS AND SPECIFICATION
164
