
THE EFFECT OF ICT ENABLED SOCIAL NETWORKS ON
PERFORMANCE
Kon Shing Kenneth Chung and Liaquat Hossain
School of Information Technologies, University of Sydney, Camperdown, NSW 2006, Australia
Keywords: ICT use, social network structure, individual performance, process of care, general practitioners.
Abstract: Research in sociology of information and technology use highlight the importance of information and
communication technology (ICT) for supporting networks among professional peers. This paper explores
the effects of different types and patterns of ICT usage for supporting professional networks. In this study,
we ask—how can different types ICT help support professional networks? What are the implications of
patterns of ICT usage on supporting professional networks? Given an association between ICT types, usage,
network structure for supporting professional networks, what are its implications on performance? In our
study, we apply the theory of structural holes and its underlying assumptions (i.e., efficiency and
effectiveness) to develop a theoretical framework and propositions for exploring interlock between types
and patterns of ICT usage, network structure, and professional support networks for measuring the
performance of effective clinical care. Empirical evidence from Australian rural general practitioners’ data
show that both network structure and Internet-enabled ICT use play a crucial role when it comes to
performance in the medical consultation.
1 INTRODUCTION
The introduction of information and communication
technologies (ICT) into organisations and
occupational communities has produced unfathomed
changes in work patterns and communication
structure (1991). Literature in Information Systems
widely recognises that ICT allows for synergistic
goal achievement when used and aligned properly
with the task at hand (Goodhue et al., 1995). In
general practice, a number of studies highlights the
extent of computerisation in general practice,
although recent studies have surveyed actual use of
ICT by general practitioners (GPs). Australian
national surveys on ICT use by GPs was conducted
in 1998 (Nielsen, 1998), 2001 (Western et al., 2001),
and most recently in 2006 (Henderson et al., 2006;
McInnes et al., 2006). Although these studies
explore the use of ICT for clinical tasks in general
practice, none questions its use for communication
with peers, especially in rural practice. Building
upon theories of social network structure, we
introduce a conceptual model for exploring the
relationship between network structure, ICT use and
attitudes to processes of medical care. We associate
density, efficiency and effective size of a GP’s
professional network with attitudes to processes of
medical care. Based on literature on impacts of
technology use, we also explore task-level effects
and communication-structural effects on attitudes to
medical care. Preliminary results show that while
professional networks are important, internet-
enabled ICT use rather than ICT use for clinical
tasks accounts higher for performance in the medical
consultation. The following section discusses the
importance of professional networks and ICT use in
the context of rural general practice.
2 CONTEXT OF THE STUDY
The first study conducted nationally in Australia
claimed that computers were present in 31% of
Australian general practices (Nielsen, 1998). In
2001, this figure increased to 86% (with a likelihood
of 95% of Australian general practices to be
computerised by 2005), indicating that Australian
general practices were highly computerised
(Western et al., 2003). The study also showed that
GPs practising in capital cities were less likely to be
computerised than in the rural practices. The
primary reason was because rural GPs were
105
Shing Kenneth Chung K. and Hossain L. (2007).
THE EFFECT OF ICT ENABLED SOCIAL NETWORKS ON PERFORMANCE.
In Proceedings of the Ninth International Conference on Enterprise Information Systems - HCI, pages 105-110
DOI: 10.5220/0002355901050110
Copyright
c
SciTePress

geographically distant from other health care
centres, general practices, and hospitals. McInnes et
al’s (2006) recent study found that Australian
general practice has achieved near-universal clinical
computerisation, although Henderson et al’s (2006)
study show that GPs are still reluctant to fully
embrace the technology. Both studies confirm
Western et al’s (2001; 2003) speculation that
Australian general practices are more likely to use
computers for administrative rather than clinical
tasks.
2.1 Research Questions
It is interesting that ICT is hardly used as a
communication medium amongst GPs in Australia.
Given the significant problems that characterise the
rural GP workforce, empirical studies highlighting
GPs’ professional support network structure related
with ICT use are relatively few. The motivating
questions for this research are thus —what are the
implications of patterns of ICT usage on supporting
professional networks? Is there any correlation
between patterns of ICT usage and the social
network structures of the professional networks?
Can we make any distinction between the types,
usage patterns, and network structure for supporting
professional network? Given an association between
types, usage, network structure for supporting
professional networks, what are the implications on
performance? How do these factors relate to
improved performance of the knowledge intensive
work groups?
3 THEORETICAL MODEL
In the following section, we discuss the development
of the constructs of our conceptual model based on
literature review.
3.1 Performance: Attitudes to Care
General practice is the “provision of primary
continuing comprehensive whole patient medical
care” (RACGP, 2004). Therefore, we regard the
‘process of care’ dimension provided by GPs to
patients as relevant for the study. In particular, we
are interested in the effectiveness of the GP in
delivering clinical and interpersonal care. Previous
studies show that comprehensively measuring the
GP’s attitude towards these dimensions of care
comes closest to measuring their actual behaviour
(Cockburn et al., 1987; Howie et al., 1992).
Research in social psychology suggests that a
person’s attitude towards an object may be related to
the overall pattern of a person’s response to that
object (Ajzen et al., 1980). In other words, the
attitude towards behaviours is a direct determinant
of the behavioural intention to perform the
behaviour. It can therefore be argued that
perceptions that the GPs hold are likely to influence
their behaviour in the consultation.
3.2 Network Structure
A social network consists of a group of human
actors that have relationships or ties amongst
themselves (Scott, 2000). Since 1970s, social
networks have been regarded as a promising concept
for becoming a unifying framework in clinical
practice (Erickson, 1975) and hospital settings
(Anderson et al., 1985; West et al., 1999). In
general, social networks theory and practice is
regarded useful for clinical practice in location of
resources and serves as an interpreter of help-
seeking behaviour and utilisation of services.
Numerous studies have documented GPs’ need for
immediate access to information and the importance
of the social network of peers and colleagues. As
Dee and Blazek (1993, p. 263) maintains,
“…colleagues are familiar, reliable, immediately
available, and inexpensive; they give concise,
organised answers that synthesize available
information”. The value of a social contact is hence
much more profound in rural areas, where the
existence of social networks amongst GPs is highly
valued.
Structural properties of social networks have
been known to bear significant impacts on an
individual’s performance. Granovetter (1973) argues
that individuals are more likely to benefit from novel
information if they capitalise on weak ties in their
social network. This implies actors ought to
maintain a number of weak ties in order to capitalise
on information benefits. Coleman (1988) argues that
closure, or closed networks, enables individuals to
combine forces, and provide collective sanctions and
thus create trust by ensuring that obligations and
promises are kept and norms are followed. Thus,
denser networks attain higher closure. Previous
studies have shown that denser ties in an
individual’s social network is conducive to
intellectual performance (Coleman, 1988), job
performance (Sparrowe et al., 2001) and knowledge-
sharing (Cross et al., 2004). Burt (1992) however,
takes on a structural perspective by suggesting that
dense networks are far more inefficient than sparse
networks because (1) they are costly to maintain,
and (2) they provide redundant information.
Structural holes theory is based on the idea that
ICEIS 2007 - International Conference on Enterprise Information Systems
106
actors are in a better position to benefit from their
interactions and transactions with others if actors are
connected to others who are not connected
themselves or well organised. Thus, an optimised
network yields information benefits through non-
redundancy. Optimisation of a social network of an
individual is measured by effectiveness and
efficiency of one’s personal network. Efficiency is
about the channels of access offered by a primary
contact (broker) in a brokerage position to access all
others (ie. secondary contacts) in the network.
Effectiveness is about the total number of contacts
reached along with all the primary contacts.
Effectiveness is hence the yield of the entire
network. In the context of rural GPs, we propose the
following:
Proposition 1: Density of a rural GP’s
network is positively associated with attitudes
to process of care
Proposition 2: Effectiveness of a rural GP’s
social network is positively related with
attitudes to process of care
Proposition 3: Efficiency of a rural GP’s
social network is positively related with
attitudes to process of care
3.3 ICT Use: Clinical and Internet
based
ICTs are replacing traditional resources for
developing an actor’s social network (Nardi et al.,
2000) as they shape personal networks and re-draw
social boundaries. Therefore, a significant construct
in our model is ‘ICT use’. Computer supported
social networks (Wellman, 1996) that connect
people sustain ties that provide information and
social support in both specialized and broadly-based
relationships. Katz and Rice (2002) consider the
Internet as having great potential for connectivity
without much intention or social cost. This is
particularly useful for occupational groups such as
dispersed rural GPs who find maintenance of ties
with peers and communities difficult and expensive
(Pickering et al., 1995). ICT use hence fosters the
connection of ties and contributes to the growth of
social capital by supporting many-to-many
information exchanges among geographically
dispersed people.
At the task-level, research on ICT use by GPs
extend beyond informatics in hospitals and specialty
medicine to include computing in general practice
settings (Aydin et al., 1997). ICT use contributes to
process of care by providing benefits to GPs such as
better storage and retrieval of information, consistent
and accurate records, improved drug management,
and integration of clinical and administrative
functions (Nielsen, 1998). It appears that ICT is
utilised, and is a good fit with the general practice
tasks it supports (Goodhue et al., 1995). Given the
above arguments, we derive the following
propositions:
Proposition 4: Frequency of use of ICT by
rural GP for clinical-tasks is positively
associated with attitudes to process of care
Proposition 5: Frequency of use of ICT by
rural GP for internet-based tasks is positively
associated with attitudes to process of care
Proposition 6: ICT use significantly
moderates the interaction between network
structure and process of care
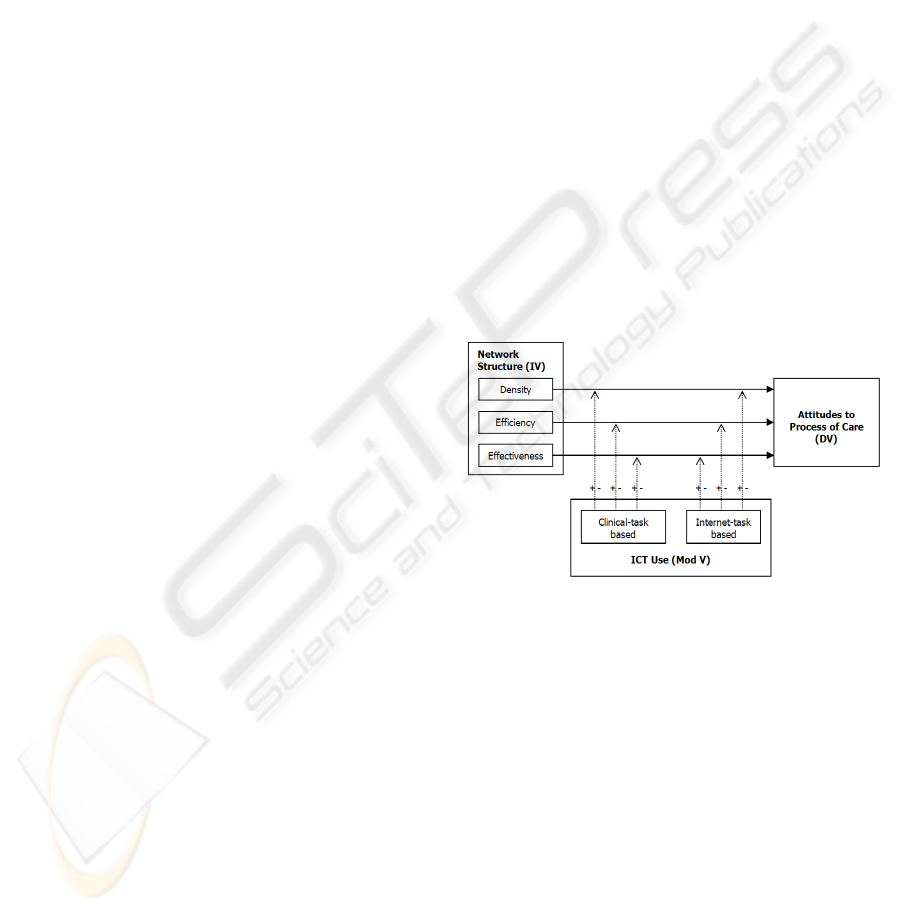
4 RESEARCH METHODOLOGY
The following section discusses the operational
model highlighting the significance of ICT use as a
variable that moderates the inherent relationship
between network structure and process of care
attitudes.
Figure 1: Operational Model for the Research.
4.1 Egocentric Network Approach
In the egocentric approach, the actor is the “ego”
and his affiliates, advisors, or friends, are known as
“alters” (Scott, 2000). Name generators are used to
elicit alters’ names. To elicit names from a GP’s
professional network, we asked:
“Looking back over the last six months, please
identify people (up to 15 maximum) who are
important in providing you with information or
advice for providing care to patients.”
Other name interpreter items solicited were
strength of each tie, measured by “time known the
person”, “frequency of interaction”, “type of
relationship”, and “degree of closeness” (Marsden et
al., 1984). Attribute data about frequency of
THE EFFECT OF ICT ENABLED SOCIAL NETWORKS ON PERFORMANCE
107
interaction via email, telephone (including mobile),
and video conferencing were also included in the
instrument to segregate face-to-face and ICT media
interactions. Finally, we asked GPs to determine
how the members of their professional network
relate to each other based on a five point degree of
closeness scale ranging from ‘especially close’ to
‘do not know each other’.
4.2 Survey Administration
The original survey was pre-piloted amongst a
group of 5 students (in the research laboratory) and
three rural GPs. Experts in the domain of general
practice, including former president of a rural
doctor’s association in Australia, professor and head
of discipline of general practice in a renowned
university, and rural GPs vetted the survey
instrument, which was then pre-tested for
comprehension and ease-of-use. Finally, the survey
was administered in two phases: first to sixty rural
GPs practising in a southern region of rural NSW
with nineteen responding (response rate: 31%);
second to 46 GPs in a rural doctors conference with
17 responding (response rate: 37%). Administration
was personal, which allowed for capturing of survey
duration, respondent reaction and errors in the
survey, which we eventually rectified.
4.3 Measures
Density is the ratio of existing number ties to the
maximum possible ties possible. Effectiveness is a
measure of the number of alters minus the average
degree of alters within the ego network, not counting
ties to the ego. Efficiency is measured by dividing
effectiveness by the number of alters in the ego’s
network.
For performance, we adapted Cockburn et al’s
(1987) validated instrument to measure four
dimensions of care: mutuality, communication,
responsibility for decisions and appropriateness of
consultations.
Clinical ICT task measures were based on the
reliable and valid item sets used by Western et al
(2001) and includes items such as frequency of
using ICT for “Generating health summaries”,
“Writing prescriptions”, and so on, measured on a
five point scale ranging from ‘Daily use’ to ‘Never’.
Internet task items were adapted from Andrews et
al’s (2004) and included “accessing medical
journals”, “accessing databases”, “consultation with
colleagues”, and so on.
5 RESULTS
There were 36 responses in total. However, 5
specialised in areas such as gynaecology and
orthopaedics, and were excluded from the analysis.
Of the remaining 29 GPs, the mean number of years
practised in a rural setting was 17.21 years (max=40
years; min=1 year).
To associate network structure, ICT use and the
dimensions of care, we ran a multiple regression
based on the four dimensions of care –
communication, mutuality, decision responsibility,
and appropriate consultation as the dependent
variable. We used density, efficiency and effective
size of the network as the network predictor
variables (model 1) and ICT use for clinical
functions and ICT use requiring internet functions as
the second block of predictor variables (model 2).
5.1 Communication Dimension
Table 1: Model summary for Communication Dimension.
Model R
R
Square
Adjusted
R Square
Std. Error
of the
Estimate
1
.405(a) .164 .059 5.67385
2
.408(b) .166 -.023 5.91807
(a) Predictors: (Constant), Network Density, Effective Size,
Efficiency; (b) Predictors: (Constant), Network Density,
Effective Size, Efficiency, Internet Functions, Clinical Functions
Our results indicate a multiple R of 0.405 (model
1) and 0.408 (model 2), which shows substantial
correlation between the predictor variables and the
variable ‘communication’, where approximately
16% of the variance in ‘communication’ is explained
by the two blocks of predictor variables. In model 1,
effective size bears greatest influence on
‘communication’ (β=0.002). In model 2, ICT use
(requiring Internet) bears greatest influence on
‘communication’ (β=0.066).
5.2 Mutuality Dimension
Table 2: Model Summary for Mutuality Dimension.
Model R
R
Square
Adjusted
R Square
Std. Error
of the
Estimate
1
.417(a) .174 .071 4.11406
2
.431(b) .186 .001 4.26593
(a) Predictors: (Constant), Network Density, Effective Size,
Efficiency; (b) Predictors: (Constant), Network Density,
Effective Size, Efficiency, Internet Functions, Clinical Functions
ICEIS 2007 - International Conference on Enterprise Information Systems
108
There is substantial correlation between the
predictor (independent) variables and the dependent
variable ‘communication’ (R = 0.417 and 0.431
respectively), where approximately 17-18% of the
variance in ‘mutuality’ is explained by the two
blocks of predictor variables. In model 1, effective
size bears greatest influence on ‘mutuality’
(β=0.209). In model 2, effective size bears greatest
influence on ‘mutuality’ (β=0.204), followed by ICT
use (requiring Internet) (β=0.134).
5.3 Decision Responsibility Dimension
Table 3: Model Summary for Decision Responsibility.
Model R R Square
Adjusted
R Square
Std. Error
of the
Estimate
1
.316(a) .100 -.013 3.20666
2
.363(b) .132 -.066 3.28896
(a) Predictors: (Constant), Network Density, Effective Size,
Efficiency; (b) Predictors: (Constant), Network Density, Effective
Size, Efficiency, Internet Functions, Clinical Functions
The results indicate considerable correlation
between the predictor (independent) variables and
the dependent variable ‘decision responsibility’ (R =
0.316 and 0.363 respectively), where approximately
10-13% of the variance in ‘decision responsibility’ is
explained by the two blocks of predictor variables.
In model 1, effective size bears greatest influence on
‘decision responsibility’ (β=0.127). In model 2,
effective size also bears greatest influence on
‘decision responsibility’ (β=0.240), followed by ICT
use (requiring Internet) (β=0.116).
5.4 Appropriate Consultation
Dimension
Table 4: Model Summary for Appropriate Consultation.
Model R R Square
Adjusted
R Square
Std. Error
of the
Estimate
1 .070(a) .005 -.120 6.35078
2 .260(b) .068 -.144 6.42042
(a) Predictors: (Constant), Network Density, Effective Size,
Efficiency; (b) Predictors: (Constant), Network Density, Effective
Size, Efficiency, Internet Functions, Clinical Functions
There is considerable correlation between the
predictor (independent) variables and the dependent
variable ‘appropriate consultation’ (R = 0.070 and
0.260 respectively), where approximately 6% of the
variance in ‘appropriate consultation’ is explained
by predictor variables in the second model. Model 2
also indicates that efficiency (β=0.796) and network
density (β=0.779) bears greatest influence on
‘appropriate consultation’, followed by ICT use
(requiring Internet) (β=0.343). This is probably true
because GPs are known to consult with their peers
and specialists for appropriate treatment. In such
cases, GPs consult those who can provide
information benefits to them in the shortest amount
of time (efficiency). Furthermore, it also indicates
that GPs who use internet functions (eg. for
communicating with peers and for accessing
educational materials) are more likely to provide
appropriate consultations.
6 CONCLUSION
Although our results are limited and not
generalisable to the population of GPs in Australia,
it shows that while individual professional network
properties are important in explaining process of
care attitudes, ICT use that required internet access
was equally important. GPs who used the internet
for communication (with professional networks of
peers, special interest groups) and accessing online
materials were better in communicating with
patients, making decision responsibilities, and
conducting appropriate consultations. Such GPs also
shared mutuality with their patients. ICT use for
clinical tasks did not contribute to either of the
dimensions of care. This is most likely the case
because GPs in the consultation process do not
usually have time to retrieve and digest information
from most forms of ICT (Bolton, 2006). At best,
ICT for clinical tasks are useful for quality assurance
such as checking drug interactions. Our results also
confirmed that effective size (or reach in the
network) was the most important predictor of
communication, decision responsibility and
mutuality dimensions of care. Efficiency (or access
to novel and useful information) and network
density (closure), on the other hand, were most
important predictors for appropriate consultation.
REFERENCES
Ajzen, I., & Fishbein, M., 1980. Understanding Attitudes
and Predicting Social Behavior. Engelwood Cliffs
New Jersey: Prentice Hall.
Anderson, J. G., & Jay, S. J., 1985. Computers and
Clinical Judgement: The Role of Physician Networks.
Social Science & Medicine, 20(10), 969-979.
THE EFFECT OF ICT ENABLED SOCIAL NETWORKS ON PERFORMANCE
109

Andrews, J. E., Pearce, K. A., Sydney, C., Ireson, C., &
Love, M., 2004. Current State of Information
Technology Use in a US Primary Care Practice-based
Research Network. Informatics in Primary Care,
12(1), 11-18.
Aydin, C. E., & Forsythe, D. E., 1997, 25th-29th October.
Implementing Computers in Ambulatory Care:
Implications of Physician Practice Patterns for System
Design. Paper presented at the Proceedings of the
American Medical Informatics Association 1997
Annual Fall Symposium, Nashville.
Bolton, P. G. M., 2006. Information Mastery and 21st
Century General Practice. The Medical Journal of
Australia, 185(2), 94.
Burt, R. S., 1992. Structural Holes: The Social Structure
of Competition. Massachusetts: Harvard University
Press.
Cockburn, J., Killer, D., Campbell, E., & Sanson-Fisher,
R. W., 1987. Measuring General Practitioners'
Attitudes Towards Medical Care. Fam. Pract., 4(3),
192-199.
Coleman, J. S., 1988. Social Capital in the Creation of
Human Capital. The American Journal of Sociology,
94, S95-S120.
Cross, R., & Cummings, J. N., 2004. Tie and Network
Correlates of Individual Performance in Knowledge-
Intensive Work. Academy of Management Journal,
47(6), 928-937.
Dee, C., & Blazek, R., 1993. Information Needs of the
Rural Physician: A Descriptive Study. Bulletin of the
Medical Library Association, 81(3), 259-264.
Erickson, G. D., 1975. The Concept of Personal Network
in Clinical Practice. Family Process, 14(4), 487-498.
Goodhue, D. L., & Thompson, R. L., 1995. Task-
Technology Fit and Individual Performance. MIS
Quarterly, 19(2), 213-236.
Granovetter, M. S., 1973. The Strength of Weak Ties. The
American Journal of Sociology, 78(6), 1360-1380.
Henderson, J., Britt, H., & Miller, G., 2006. Extent and
Utilisation of Computerisation in Australian General
Practice. The Medical Journal of Australia, 185(2),
84-87.
Howie, J. G. R., Hopton, J. L., Heaney, D. J., & Porter, A.
M. D., 1992. Attitudes to Medical-Care, the
Organization of Work, and Stress among General-
Practitioners. British Journal of General Practice,
42(358), 181-185.
Katz, J. E., & Rice, R. E., 2002. Social Consequences of
Internet Use: Access, Involvement, and Interaction
(1st Edition ed.). London: MIT Press.
Marsden, P., & Campbell, K. E., 1984. Measuring Tie
Strength. Social Forces, 63, 482-501.
McInnes, D. K., Saltman, e. C., & Kidd, M. R., 2006.
General Practitioners' Use of Computers for
Prescribing and Electronic Health Records: Results
from a National Survey. The Medical Journal of
Australia, 185(2), 88-91.
Nardi, B. A., Whittaker, S., & Schwarz, H. (2000). It's Not
What You Know: Work in the Information Age.
Retrieved 12th January, 2005, from
http://www.firstmonday.org/issues/issue5_5/nardi/inde
x.html
Nielsen, A., 1998.
A Study into Levels of, and Attitudes
Towards Information Technology in General Practice
(No. S2587/NG2132). Sydney: Commonwealth
Department of Health and Family Services.
Pickering, J. M., & King, J. L., 1995. Hardwiring Weak
Ties: Interorganizational Computer-mediated
Communication, Occupational Communities, and
Organizational Change. Organization Science, 6(4),
479-486.
RACGP. (2004). Rural General Practice - Definition.
Retrieved 14th November, 2004, from
http://www.racgp.org.au/document.asp?id=15301
Scott, J., 2000. Social Network Analysis: A Handbook.
London: SAGE Publications.
Sparrowe, R. T., Liden, R. C., Wayne, S. J., & Kraimer,
M. L., 2001. Social Networks and the Performance of
Individuals and Groups. Academy of Management
Journal, 44, 316-326.
Sproull, L., & Kiesler, S., 1991. Connections: New Ways
of Working in the Networked Organization.
Cambridge: MIT Press.
Wellman, B., 1996. For a Social Network Analysis of
Computer Networks: A Sociological Perspective on
Collaborative Work and Virtual Community. Paper
presented at the Proceedings of the 1996 ACM
SIGCPR/SIGMIS conference on Computer Personnel
Research Denver, Colorado, United States
West, E., Barron, D. N., Dowsett, J., & Newton, J., 1999.
Hierarchies and Cliques in the Social Networks of
Health Care Professionals: Implications for the Design
of Dissemination Strategies. Social Science and
Medicine, 48, 633-646.
Western, M., Dwan, K., Makkai, T., Mar, C. d., &
Western, J., 2001. Measuring IT use in Australian
General Practice. University of Queensland: General
Practice Computing Group.
Western, M. C., Dwan, K. M., Western, J. S., Makkai, T.,
& Mar, C. D., 2003. Computerisation in Australian
General Practice. Australian Family Physician, 32(3).
ICEIS 2007 - International Conference on Enterprise Information Systems
110
