
SOFTWARE AGENTS REPRESENTING MEDICAL GUIDELINES
John McGrory, Frank Clarke
Dublin Institute of Technology, Dublin 8, Ireland
Jane Grimson
School of Computing, Trinity College Dublin, Dublin 2, Ireland
Peter Gaffney
Adelaide & Meath Hospital, Incorporating the National Children's Hospital (AMNCH), Tallaght, Dublin 24, Ireland
Keywords: Clinical laboratory validation, patient-centred, patient-focused, agents, computer-interpretable-guideline
(CIG), guidelines and protocols. Software Agents representing medical guidelines.
Abstract: Guidelines are self-contained documents which healthcare professionals reference to obtain specific disease
or medical condition knowledge for a particular population cohort. They view these documents and apply
known facts about their patients to access useful supportive information to aid in developing a diagnosis or
manage a condition. Traditional CIG models decompose these guidelines into workflow plans, which are
then called using certain motivational trigger conditions controlled by a centralised management engine.
Therefore, CIG guidelines are not self-contained documents, which specialise in a particular condition or
disease, but are effectively a list of workflow plans, which are called and used when the patient information
is available. The software BDI agent offers an alternative approach which more closely matches the modus
operandi of narrative based medical guidelines. An agent’s beliefs capture information attributes, plans
capture the deliberative and action attributes, and desire captures the motivational attributes of the guideline
in a self-contained autonomous software module. This synergy between the narrative guideline and the BDI
agent offers an improved solution for computerising medical guidelines when compared to the CIG
approach.
1 INTRODUCTION
Clinical guidelines are condition focused documents
through which domain specific aims, goals,
procedures, plans and normal reference ranges are
disseminated to healthcare professionals (Browne,
2005) (Oosterhuis, 2004). To maximise influence on
a market audience these documents are written in
domain specific languages and ontologies (e.g.
cardiology, neurology and paediatrics). The purpose
of these documents are to guide the reader, and
streamline activities around a particular medical
condition, organ or disease using evidence based
supportive information. When a clinical or
laboratory guideline is developed by an expert group
they focus on best practice for the specific disease,
condition or organ. They include all relevant
knowledge, logic and motivational aspects they
deem necessary to adequately describe the domain.
Therefore, guidelines are autonomous self-contained
documents, which can be used in whole or in part, to
provide supporting information for healthcare
decision-making, once their meaning is not taken out
of context.
Clinicians and laboratory technologists care for
patients so it is their responsibility to filter through
these guidelines acting on a patient’s behalf. They
must make use of the maximum decision-making
support offered by these resources based on the
known facts about the individual. This is termed
patient-centred validation. However, the enormous
quantity and presentation style of these documents
makes it difficult for professionals to quickly
identify relevant guidelines, and extract information
and intended logic contained within them, and apply
142
McGrory J., Clarke F., Grimson J. and Gaffney P. (2008).
SOFTWARE AGENTS REPRESENTING MEDICAL GUIDELINES.
In Proceedings of the First International Conference on Health Informatics, pages 142-147
Copyright
c
SciTePress

them usefully in a patient-centred fashion (Peleg et
al., 2003).
One approach to overcome these issues is to use
Computer-Interpretable-Guidelines (CIG). The
underlying operation of CIG models is to decompose
the narrative guideline into separate workflow
activities and management rules. The management
rules from each guideline are linked together
centrally using an inference engine. This inference
engine is constructed by the CIG developers using
rules that link the various workflow activities
together. These management rules provide the
motivation for a centralised inference engine to
choose particular workflow activities depending on
the patients known characteristics (e.g. weight,
gender, height). As more guidelines are decomposed
and added, the number of workflow activities and
the size and complexity of the centralised inference
engine increases. Using this technique the original
self-contained knowledge developed by the
guideline author’s is fragmented and the true context
is lost.
Agent-oriented software operates on the notion
that human intelligence and decisions can be
synthesised by managing tangible elements, such as
beliefs, goals, sub-goals, plans and intentions. Each
agent is an autonomous software module that is self-
contained, has its own inference engine and a set of
beliefs, goals and plans. The goals, beliefs and plans
are encoded into the agent and the inference engine
interprets them. When a goal is chosen the inference
engine searches plans that match currently known
beliefs and prioritises them. The most appropriate
plan is selected and executed to perform some
activity or choose another goal. In addition to its
inference engine the agent approach also permits
separate agents to socialise, work in groups and
collaborate to solve common goals.
There are characteristic similarities between
guidelines and a particular type of agent, namely the
Belief-Desire-Intention (BDI) agent as shown in
Table 1.
Table 1: BDI to Guideline mapping.
By encoding the agent with the knowledge, logic
and motivational components of a guideline, it
creates an opportunity for an individual agent to
represent a single guideline. As additional guidelines
are added, new agents are created to represent them.
This technique means that the original self-contained
knowledge developed by author’s remains as an
integrated software module and the context is
retained.
The thrust of this paper is to demonstrate that a
single software agent possesses the ability to
reproduce the function and content of a clinical
guideline as a 1:1 ratio. This is because a synergy
exists between guideline and agent characteristics.
2 COMPARISON OF
GUIDELINES, CIG’S AND
AGENTS
Guidelines play a crucial supporting role in the
detection, diagnosis, treatment, and supervision of
diseases in patients, in a modern healthcare setting.
In some cases these documents aid in the planning of
treatments, quantifying of medication amounts,
monitoring of patient responses, which could all
have serious patient safety issues if inaccurate
information was used. Therefore, it is vital the
knowledge, logic and motivation contained within
the guideline are clearly understood with reference
to a specific patient. But how do CIG’s and agents
reproduce the knowledge, logic, action and more
specifically motivation of guidelines? In the
following subsections the function, use and
methodology behind guidelines, CIGs and agents are
discussed.
2.1 Guideline Infrastructure
Guidelines are autonomous literature sources which
seldom rely on any other knowledge, except some
base-level understanding. They provide information,
logic and motivation in order to describe aspects of a
particular domain. The guideline document itself is
made up of a series of aims, goals, procedures and
plans. It was never expected guidelines would be
used exclusively in a form of cookbook medicine,
but more in a complementary and supportive role by
providing domain specific information. Therefore,
these documents are rarely used in whole, but more
in part, to aid in healthcare delivery. This means that
the guideline should be viewed holistically, and not
just as a collection of separate workflow elements
taken out of context.
In summary, a clinical guideline is a self-
contained document which specialises in a specific
BDI
Structure
Characteristics Guideline Structure
Belief
↔
Informational
attributes
↔
Facts
Desire
↔
Motivational
attributes
↔
Goals and aims
Intension
↔
Deliberative
attributes
↔
Selection of
Actions
SOFTWARE AGENTS REPRESENTING MEDICAL GUIDELINES
143
condition, organ or disease. Medical professionals
interface with this document in light of the known
patient information to support their patient-centred
healthcare delivery.
2.2 Computer-Interpretable-Guidelines
The underlying principle behind the CIG approach is
to disassemble the guideline into separate workflow
activities, and then orchestrate rules to link these
activities together centrally based on the presented
patient data. The majority of CIG’s decompose the
medical guideline into an Arden Syntax Medical
Logic Module (MLM) or similar by dividing the
narrative guideline into ‘evoke’, ‘data’, ‘logic’ and
‘action’ slots. These slots are used to develop a
software workflow activity plan, complete with a
triggering condition, but contain no motivation or
goal. As more guidelines are added, rules controlling
the selection, merging and division of workflow
activities increases. The centralised CIG control
engine which manages these activities provides the
motivation or goal for the software to operate. As all
guidelines are coupled together via the centralised
set of management rules it is not possible to
distribute this activity among a number of computer
systems. This is fundamentally different to the true
operation of a medical guideline where many copies
of the same guideline exist.
In summary, a CIG is a list of workflow plans
which are called and used when the relevant patient
information is available. It is centralised and the
original knowledge is fragmented and cannot be
truly interfaced with.
2.3 Software Agents
An agent is an autonomous self-contained software
module which is programmed using belief, goal and
plan attributes. Each agent has its own inference
engine which interprets these attributes in order to
perform some activity. The principle of a BDI
agent’s operation is based on a belief capturing the
informational attributes, the desire capturing
motivational attributes and the intention capturing
the deliberative attributes of an agent (Rao et al.,
1995). An agent shell is a generalised version of an
agent which can be adapted for a wide variety of
different applications. There are a number of BDI
agent shells available such as Jason, 3APL and
Jadex. Jadex 0.932 was the agent shell used in this
research. Although there are characteristic
similarities between agents and guidelines the raw
Jadex shell is not capable of capturing guideline
functionality without some modification. To this end
the Jadex agent shell was adapted and this modified
version of the Jadex agent was titled Autonomous
Socialising Knowledge agent (ASK-agent).
Using the ASK-agent model a guideline can be
decomposed into workflow activities, but instead of
having a centralised inference engine to manage all
the guidelines, each guideline has its own inference
engine. The guidelines have the ability to
communicate with other resources using message
passing. The ASK-agent encodes the separate
workflow paths and motivational management rules
of the guideline within a single autonomous software
module. There is no centralised engine managing the
separate ASK-agents, therefore the approach is
distributed. Each agent registers itself, complete
with the services it provides, language and ontology
it uses with a Directory Facilitator (DF). The DF
acts as a goldenpages for agents, allowing them to
be looked-up, accessed and used as independent
resources.
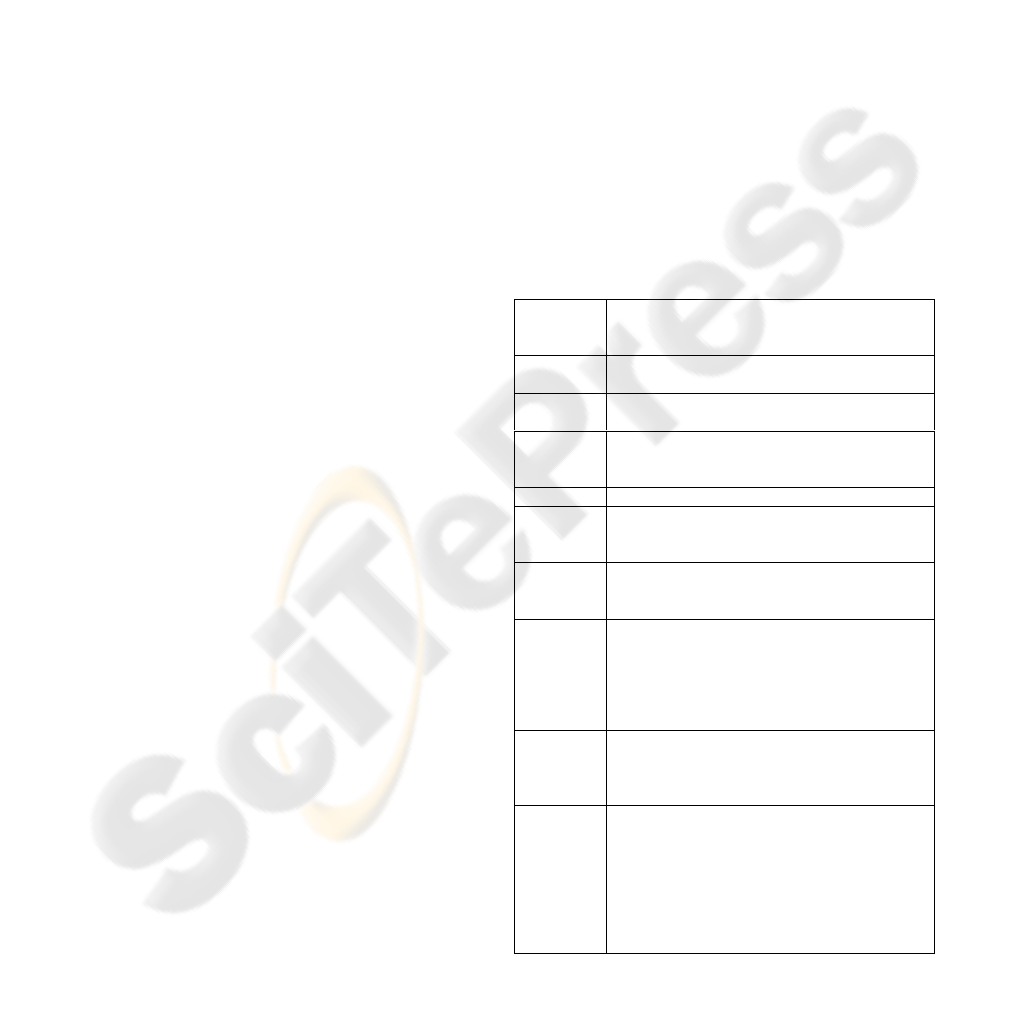
Table 2: Adapted MLM to Agent map.
The agent’s beliefs capture and encode the
information attributes of the guideline, the agent’s
Adapted
MLM
Slot
ASK-Agent Component
Evoke The ASK-agent’s action trigger to perform
some task, or perform goal.
Data Belief, the facts the agent uses to trigger logic.
A belief can be any Java object.
Logic Condition, precondition or trigger based on
beliefs used for the selection of an appropriate
workflow activity plan or goal.
Action Execution of the workflow activity.
*NEW*
Achieve
Goal
Motivates the ASK-agent to achieve a specific
goal to reach some desired state, such as
determine patient gender, age, PatientID.
*NEW*
Maintain
Goal
Motivates the ASK-agent to maintain a specific
condition (e.g. maintain the plausibility value
above 60%)
*NEW*
Query
Goals
Motivates the ASK-agent to seek alternative
avenues on an IF basis without committing to
the workflow activity (e.g. test alternative paths
before committing to the path, such as would
knowing the gender of the patient alter the
outcome?).
*NEW*
Meta-level
reasoning
If more than one workflow activity is triggered
simultaneously, but only one should be chosen
the ASK-agent must choose the most
appropriate course of action to take.
*NEW*
Modal
reasoning
If data stored in the beliefs or received in a
message has a level of truth, but cannot be
established as 100% true or false, then the
ASK-agent can weight its selection of an
appropriate action (e.g. the patient could have
kidney failure, probability of 60%, but the
patient could also have liver failure, probability
of 55%)
HEALTHINF 2008 - International Conference on Health Informatics
144

plans capture and encode the deliberative and action
attributes of the guideline, and the desire captures
and encodes the motivational attributes of the
guideline. This can be accurately and efficiently
completed by using an adapted MLM to agent map
as shown in Table 2, which was used in a proof of
concept agent application developed by the authors.
The extended MLM structure provides a means
to extract the guideline motivational components in
the form of achieve, maintain and query goals.
These motivational components provide the driving
force behind the agent’s activity. Using this
approach an agent can act faithfully and
autonomously on behalf of the guideline in a self-
contained capacity. Thus when patient specific
information is presented to the individual agents, via
message passing, they have the ability to apply their
encoded knowledge and logic, and provide a
supportive response based solely on that
information. Using this operation dynamic an agent
module can also make use of the maximum
supportive response from the other separate agent’s
(which represent guidelines) based on the known
facts about the individual patient. By providing a
framework which allows separate agents broadcast
supportive communications to each other, the agent
approach offers the opportunity for the data to be
validated in a patient-centred fashion.
In summary, an ASK-agent is a self-contained
software module which specialises in a specific
condition, organ or disease affecting a particular
population cohort. Other agents (software or human)
interface with this software knowledge in light of the
known patient information, and receive supportive
information from the agent to aid in their patient
specific healthcare delivery.
3 PROCEDURE TO CONVERT A
GUIDELINE TO ASK-AGENT
To provide a consistent technique for developing
ASK-agent modules, which can act faithfully and
accurately on behalf of a guideline, it is important to
document, and explain the conversion process. The
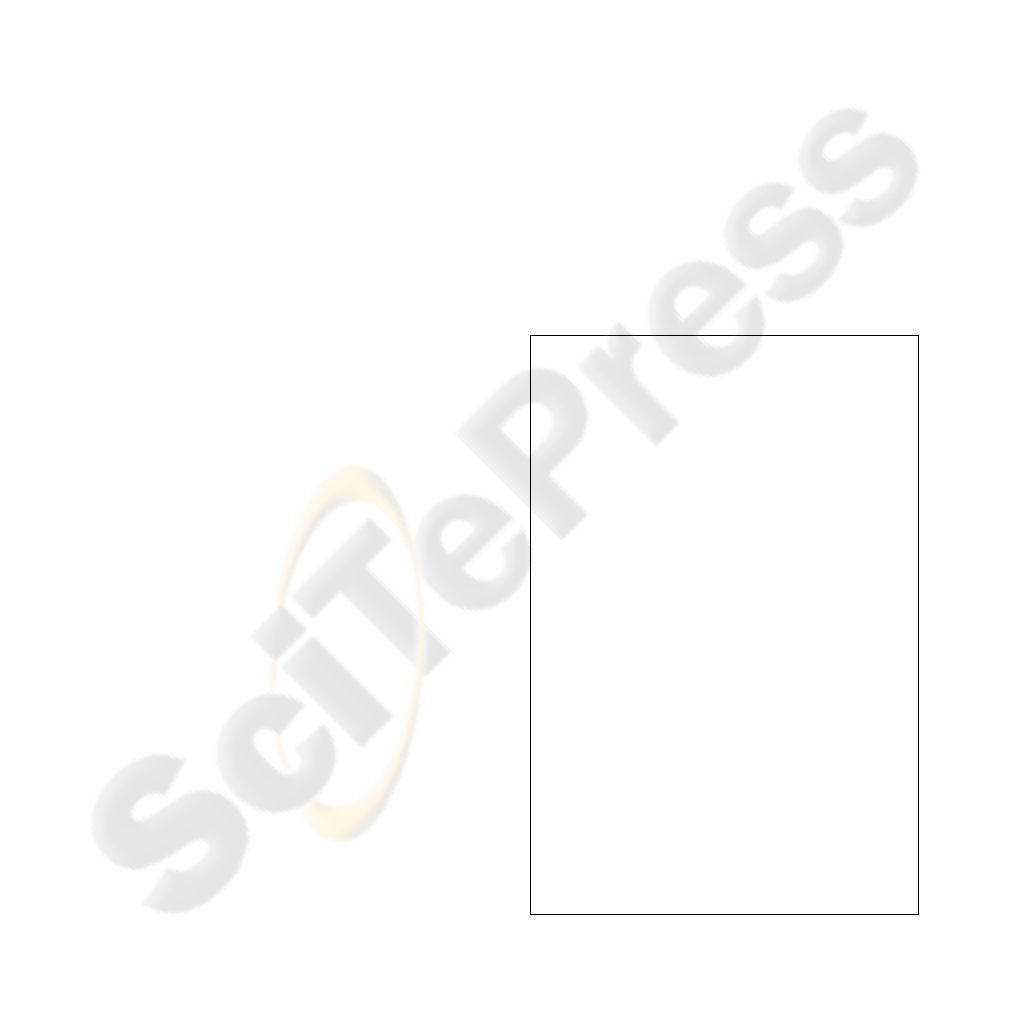
development of an ASK-agent module from a
specific narrative guideline is based on the cycle
shown in Figure 1. This procedure uses the
expanded MLM mapping to the Agent Definition
File (ADF) Extended Mark-up Language (XML) file
and Java plans. The procedure is divided into six
steps each of which is described in the following
subsections.
Select
Guideline
Convert guideline
to Extended MLM
Convert Extended
MLM to
Agent ADF
File & Plans
?
Does implementation
represent guideline motovation,
logic and knowledge?
Review guideline
Yes
No
Upload/Execute
1
2
6
5
4
3
Select
Guideline
Convert guideline
to Extended MLM
Convert Extended
MLM to
Agent ADF
File & Plans
?
Does implementation
represent guideline motovation,
logic and knowledge?
Review guideline
Yes
No
Upload/Execute
1
2
6
5
4
3
Figure 1: Encoding of expert agent procedure.
3.1 Select Guideline
The medical institution chooses a guideline that
matches and complements their core activities. The
types of guidelines being discussed are text based
documents with conclusions being derived using
rule-based or statistic-based decisions or numerical
analysis. Neither the proposed ASK-agent nor
existing CIG approaches can manage guidelines
which have been developed using graphical imagery
and charts.
3.2 Convert Guideline to Extended
MLM
The guideline document is an amalgamation of a
number of workflow activities which are triggered
using motivational goals. Consider for illustration
purposes the example of a generalised guideline
extract shown in Table 3.
Table 3: Generalised guideline extract.
Evoke:
Arrival of laboratory results for analyte results X, Y and Z.
Data:
PatientAge
PatientGender
Logic:
IF (25Years < PatientAge >50Years) AND (40U/L < X >
130U/L) THEN perform ActivityA.
IF (PatientGender = Male AND (8U/L < Y > 40U/L) THEN
perform ActivityB.
IF (PatientGender = Female AND (6U/L < Y > 35U/L) THEN
perform ActivityB.
IF (PatientGender = Female AND (50U/L > Z) THEN perform
ActivityC.
Action:
ActivityA
ActivityB
ActivityC
SOFTWARE AGENTS REPRESENTING MEDICAL GUIDELINES
145
The evoke slot relates to the triggering condition
which is used to start this specific workflow path.
The data information is retrieved from the
Laboratory Information System (LIS) by completing
an SQL query, or by executing an archetype query.
An archetype is a recently employed term used in
medical informatics. It is described in the CEN pre-
standard prEN13606:2004(E) as a reusable, template
model which presents a specific viewpoint of a
domain reference model. The logic relates to a rule
for selecting an activity. Finally the action is the
activity to be performed, such as “print message to
screen” or perform another activity.
3.3 Convert MLM into Agent ADF File
and Java Plans
The agent is encoded by directly mapping the
extended MLM components to the ASK-agent. Code
1 illustrates how the Jadex ADF is encoded using
XML. This file contains MLM slot components such
as data, evoke, action, logic, query goal, achieve
goal, maintain goal and meta-level priority. Meta-
level reasoning is where two or more plans or goals
can be triggered at the same time and a choice is
needed on which one takes priority. For example
consider the generalised guideline extract shown in
Table 2. The first logical statement may be triggered
calling on activityA to be executed. But any of the
other three logic statements could also be triggered
simultaneously calling on activityB or activityC. Do
all need to be performed together, or should one
activity be completed first? These decisions are
traditionally realised centrally within the CIG
engine, and are not part of the distributed MLM
modules themselves. This motivation must be
extracted from the original narrative guideline
document and added to the BDI, providing the
motivating force behind the agent’s activity. Using
Jadex this ordering of activities can be completed
using priority attributes. Other components utilised
by the expert agent model but not explicitly declared
in either the narrative guideline or MLM are
language, ontology and service descriptions. If the
guideline was developed using a specific language
or ontology, it is important that the sender of
messages to it are aware of this, so a richer form of
communication can be established. To this end the
Jadex agent permits the declaration of an agent’s
language and ontology. The service description is
used to register services the guideline can perform.
In practice a guideline can perform many services,
for example validate analyte Y and Z results if the
PatientAge is known, or validate analyte X and Z
results if PatientGender is known. These are
services the ASK-agent is able to provide and are
described using the Service Description component.
For each service described using the ASK-agent
eight parameters are used to describe it. These
parameters are name, type, ownership,
GuidelineReference, InformationNeeded
ValidationType, ontology and protocol. These
services are registered with the DF goldenpages
agent. Type is used to identify the field of expertise
to which the ASK-agent belongs (e.g. liver, kidney,
and haematology). Ownership is used to identify the
guideline implementation owner (e.g. department).
GuidelineReference is used to identify the guideline
that the ASK-agent represents (e.g. ISBN).
InformationNeeded is a list of the data the ASK-
agent requires in order to process the validation
request (e.g. SerumALK_P, SerumALT,
SerumGGT). The InformationNeeded titles can be
developed to match the medical domain titles. Both
ontology and protocol where described earlier. There
presence in the service description is so other ASK-
agents can identify the ontology and protocol used
by this particular agent.
<!-- First Heading -->
<!-- <H3> Second Heading</H3>
<H4> Third Heading</H4> -->
<agent xmlns:xsi="http…>
<imports>…</imports>
<capabilities>…</capabilities>
<beliefs>Data_MLM_Slot </beliefs>
<goals>Evoke_MLM_Slot, Query
Goals, Achieve Goals, Maintain
Goals and Meta-level priority
</goals>
precondition, conditions and
triggers activating the goal are
represented by the Logic MLM
Slot
<plans>Action_MLM_Slot, Meta-
level priority </plans>
precondition, conditions and
triggers activating the plans are
represented by the Logic MLM
Slot
<events>…</events>
<languages>…</languages>
<ontologies>…</ontologies>
<expression>…</expression>
<servicedescription>…
</servicedescription>
</agent>
Code 1: Jadex agent ADF XML constructor.
HEALTHINF 2008 - International Conference on Health Informatics
146
3.4 Expert Agent Testing
Once the Agent ADF XML file and associated plans
are developed the implementation needs to be
thoroughly tested to ensure it represents the original
guideline’s motivations, logic and knowledge.
Guidelines are autonomous self-contained entities;
therefore the agent must act in a similar fashion. If
the implementation of the guideline achieves this
then it is uploaded into the main agent platform and
can be used as part of the ASK-agent group.
3.5 Upload and Execute Agent Module
The developed ADF XML file and Java plans which
represent the guideline are loaded into the JADE
Remote Agent Management. Using the JADE
Remote Agent Management GUI each agent is
selected in turn using the “Start New Agent” button
and loaded into the manager. Once installed the
agent is able to act as part of the social group. The
uploaded agents can be switched on, off or
suspended by using the JADE Remote Agent
Management GUI.
3.6 Review Guideline Conversion to
ASK-Agent
If the agent module autonomous action does not
represent the intended operation and understanding
of the original narrative guideline, its encoding
should be reviewed. This review continues until the
agent represents the true operation of the guideline.
4 CONCLUSIONS
The purpose of this research is not to dismiss the
CIG approach, but re-examine it from a processing
point of view. This research demonstrates the
agency approach offers a solution to the
management of medical guidelines electronically, in
a manner similar to that provided by the original
narrative guidelines themselves. This is because of
the synergy between the knowledge base, plans,
decisions, action, goals and the self-contained
components between guidelines and agents. It
illustrates that this method permits the guideline
content to be stored within one standalone agent
module, and the entire knowledge, logic and data
can be interfaced with by other agents when
necessary. The ASK-agent approach permits a single
guideline to be expressed within a standalone agent,
but for true patient-centred validation to occur these
separate agents must be able to communicate with
other modules and collaborate. These last two
aspects are covered in more detail in separate papers
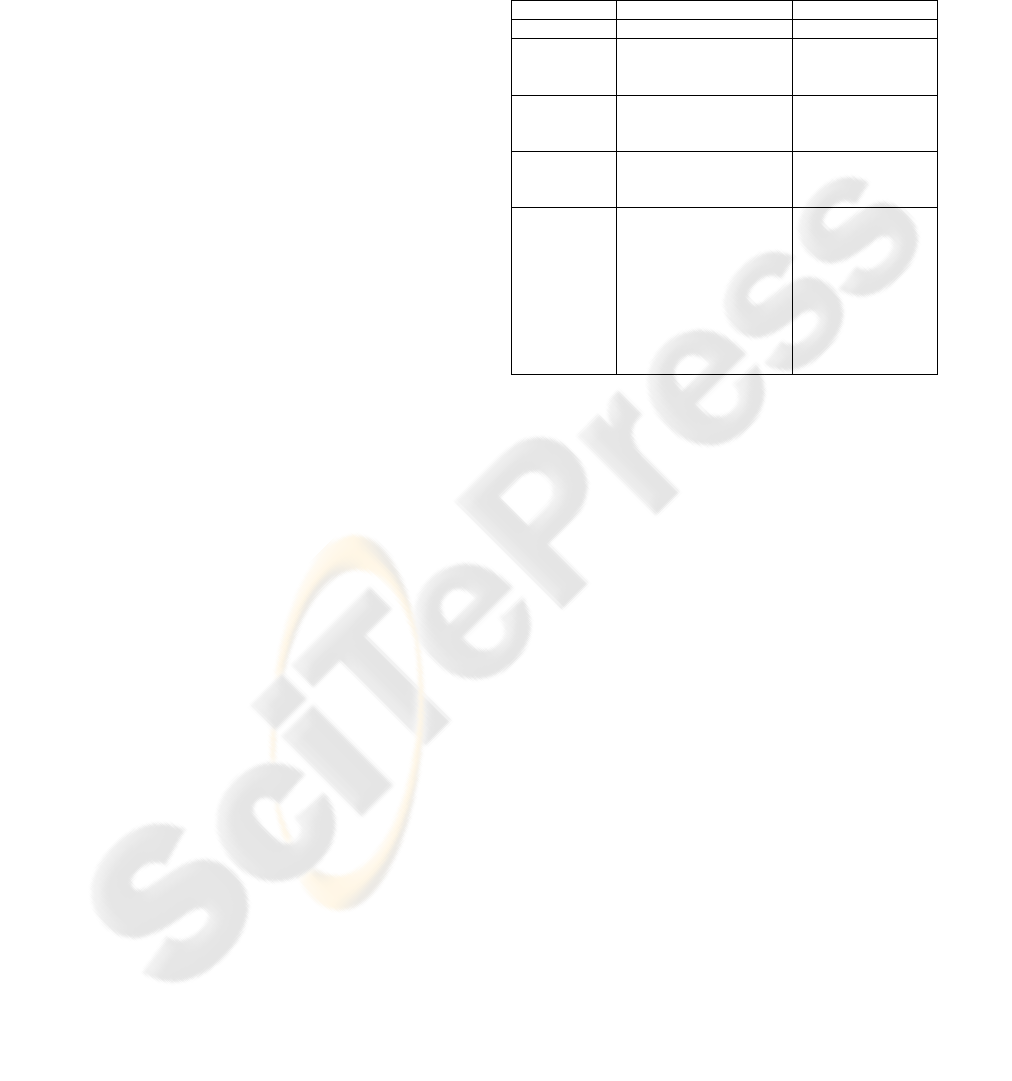
presented at this conference. So in summary the key
differences between the CIG and ASK-agent
approaches are detailed in Table 4.
Table 4: Generalised guideline extract.
Aspect CIG ASK-Agent
Processing Centralised Distributed
Guideline
content
Fragmented within CIG
engine.
Integrated as a
standalone
module.
Method of
accessing
information
Data entry and the
execution of CIG rules.
Message passing.
Encoding of
guideline
content
Menu or/and graphical. XML and Java.
Size of
file(s)
created
For a single guideline
the CIG engine is
small. However, as
more MLM’s are added
the CIG engine
application file
becomes very large.
Processing cannot be
distributed.
For a single
guideline the
ASK-agent is
larger than the
CIG. However, as
model is
distributed the
system file size is
not a limitation
ACKNOWLEDGEMENTS
The authors wish to acknowledge and thank the
work undertaken by developers of the Jadex agent
platform at Distributed Systems and Information
Systems Group, Computer Science Department,
University of Hamburg. http://vsis-
www.informatik.uni-hamburg.de/projects/jadex/
REFERENCES
Browne E.D., 2005. Workflow Modelling of Coordinated
Inter-Health-Provider Care Plans, School of
Computer and Information Science, University of
South Australia, Adelaide, PhD Thesis January 2005.
Oosterhuis W.P., Bruns D.E., Watine J., Sandberg S.,
Horvath A. 2004. Evidence-Based Guidelines in
Laboratory Medicine: Principles and Methods,
published in Clin Chem, year 2004, Vol50 pgs 806-818.
Peleg M., Tu S., Bury J., Ciccarese P., Fox J., Greenes R.,
Hall R., Johnson P., Jones N., Kumar A., Miksch S.,
Quaglini, S., Shortliffe E, Stefanelli M. 2003.
Comparing Computer-interpretable Guideline
Models: A Case-study Approach, accessed via Journal
of the American Medical Informatics Ass. Volume 10
Number 1 Jan / Feb 2003.
Rao A., Georgeff M., 1995. BDI Agents: From Theory to
Practice, proceedings of the first international
conference on multi agent systems (ICMMAS-95) San
Francisco USA 1995.
SOFTWARE AGENTS REPRESENTING MEDICAL GUIDELINES
147
