
USING WEB SERVICES TO DYNAMICALLY EMBED MEDICAL
CONTENT IN A CLINICAL INFORMATION SYSTEM
Martin Luethi
Picis, Inc., 9550 W. Higgins Rd, Rosemont, IL, 60018, USA
Keywords: Web services, medical calculators, drug dosage calculators, dynamic user interface.
Abstract: This paper describes a prototype software application that makes use of Web services to retrieve medical
content from an external Application Service Provider (ASP) service. The retrieved data is used by the sys-
tem to dynamically generate user interface components within a user-customizable department information
system and by clinicians to obtain results that will assist with medical decision-making. Medical forms are
frequently built and rearranged by medical system administrators. From the perspective of clinical end users
the content is seamlessly integrated and allows querying of dosages, interactions, and formulations using
collected parameters such as age, weight, and physiological data. Whereas the use of standalone personal
digital assistant (PDA) devices provides measurable benefits to clinicians, the feasibility of a seamless inte-
gration with user-customizable information systems has not been researched well. This paper describes one
approach that could be taken to integrate such medical calculators with a web-based clinical information
system. The solution described is not intended to represent functionality available in any actual or planned
product.
1 INTRODUCTION
Medical content and knowledge such as drug inter-
actions, medical calculators, drug dosing calculators,
drug formulations, and illustrations provide a high
benefit to clinicians and may decrease patient risk
significantly (Knollmann et al., 2005). Medical
knowledge has been made available in vast compen-
diums and in more recent days on the internet or as
standalone applications on mobile devices such as
PDAs. Whereas these applications provide a meas-
urable benefit, they lack integration and documenta-
tion capabilities with clinical information systems
that are concurrently used in the department. Conse-
quently retrieved results have to be duplicated using
the departmental procedures and systems in place.
Often departmental systems provide this medical
content as well. It is either provided by the software
vendor directly or external databases are purchased
from vendors and then tightly integrated with the
application. However, the conventional approach has
two major disadvantages: First, changing content
requires a new release or system maintenance cycle.
Second, the integration is often static and does not
allow the user to modify the clinical content.
The presented approach provides a solution to
these problems. Using an ASP model, the content is
directly queried from the content provider via Web
services. Updates of data and newly added function-
ality are immediately available at sites where the
system is in use. Further, the user interface (UI) is
instantiated in an ad hoc fashion and the content is
integrated within the dynamic structure. Updated
content is immediately available for use and required
UI elements are rendered. Patient data already avail-
able in the departmental system such as age, weight,
and height is automatically pulled into the calcula-
tors. Once all necessary parameters are collected an
additional Web service call is made to retrieve the
calculated result based on the parameters provided
by clinicians.
This paper also describes security challenges
specific to the use of external Web services with
medical data. Availability and reliability issues are
discussed as well as general patient safety risks and
testing strategies. Scenarios are discussed from the
perspective of the service requester.
291
Luethi M. (2008).
USING WEB SERVICES TO DYNAMICALLY EMBED MEDICAL CONTENT IN A CLINICAL INFORMATION SYSTEM.
In Proceedings of the First International Conference on Health Informatics, pages 291-297
Copyright
c
SciTePress

2 CLINICAL CONTENT
Medical knowledge is increasing rapidly. It is diffi-
cult for clinicians to keep up-to-date with new evi-
dence-based studies, medical literature, and FDA-
approved medications and their interactions, even
though they should be considered during medical
decision making. Prescription errors and adverse
drug events are a leading cause for malpractice liti-
gation (De Sousa, 1996). Improving access to this
knowledge could lead to better decision-making,
improve patient outcome, reduce costs, and increase
bed utilization (Pronovost et al., 2002).
Portable devices, namely PDAs, have been used
to make this knowledge accessible for clinicians
(Lapinsky et al., 2004). The largest criticism of these
systems besides data-related issues is their lack of
integration with departmental information systems,
their lacking ease of use, and the need to manually
update the devices’ databases. Content is preferably
accessed in one single application and used on desk-
top computers when away from the bedside. Subse-
quently, examples are provided for often accessed
content types.
2.1 Drug Dosage Calculators
Drug dosage calculators are used to calculate medi-
cation doses taking into account individual patient
data such as weight and age and other relevant in-
formation. The applied formulas may vary by treated
disease and type of medication.
The following table presents an example of a
simple calculation formula (1) for IV Dobutamine.
The parameters required for the calculation a-d are
listed.
a = drug amount (mg)
b = per fluid (ml)
c = weight (kg)
d = dose (mg/kg/min)
x = drip (ml/min)
x = a / b * c * d (1)
2.2 Medical Calculators
Medical calculators are used to generate a numeric
or textual result that is used for further medical deci-
sion making. Typical examples are the calculation of
probabilities of diseases and outcomes, index num-
bers, and scales. They can have one or multiple data
entry parameters, which can be numeric or chosen
from a selected textual option.
The following example is Basal E Expend for
females (2), which requires weight, height, and age
as input parameters and results the calorie use per
day.
a = weight (kg)
b = height (cm)
c = years
x = kcal/day
x = 9.6 * a + 655 + 1.8 * b – 4.7 * c (2)
2.3 Drug Interactions
The intake of more than one drug can result in se-
vere interactions. Before prescribing or applying
drugs, possible interactions have to be checked.
With the current prototype several dozens can be
checked simultaneously and the seriousness of inter-
actions is rated on a scale of 1-5. Each interaction is
accompanied with an explanation of the effects of
the interaction.
As an example the interaction between Aspirin
and Atenolol is provided. The result contains the
severity of the interaction and its description. To
obtain the desired result the drug identifiers have to
be provided.
a = Aspirin (drug 1)
n = Atenolol (drug n)
x = drug interaction (level, message)
x = a, …, n (3)
2.4 Other Content
A simple case of medical content is the provision of
textual and visual data regarding a contextual topic.
The difficulty is to provide an appropriate search
term to retrieve the data dynamically depending on
the context and to link it with the application.
2.4.1 Text Content
Medical text content requires one or more search
terms and a product code. Access of an encyclopae-
dic database is currently not supported. The service
returns a result of drugs and products in textual rep-
resentation.
2.4.2 Illustrations
Images are used for educational purposes. They pro-
vide explanations and textual values (Figure 1). Im-
ages are static and do not need any input parameter
except the expected graphic format and the illustra-
HEALTHINF 2008 - International Conference on Health Informatics
292
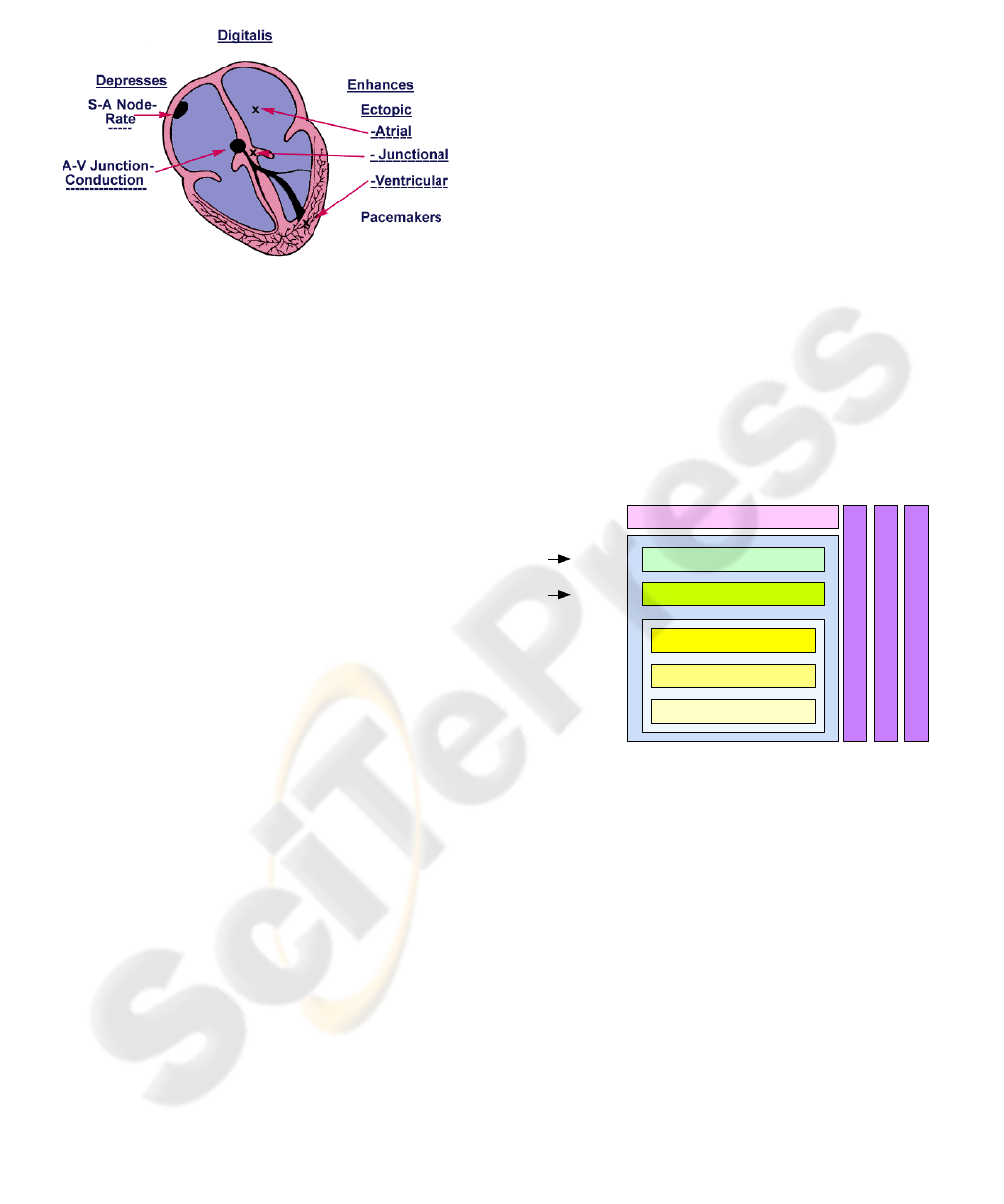
tion identifier. The binary output is embedded in the
XML body as base-64 encoded string.
Figure 1: Example of a medical illustration.
3 WEB SERVICES
A Web service is a software system that is designed
to support interoperable machine-to-machine inter-
action over a network. Its interface is described in a
machine-processable format so that other systems
can interact with the service exchanging messages
(W3C 2004). For a successful message exchange
mechanics and semantics of a message have to be
defined and mutually agreed upon.
The mechanics describe the message format, data
types, transport protocols, and transport serialization
protocols. Commonly these definitions can be found
in a Web services Description Language (WSDL)
document. The semantics give the message meaning
and its definitions are less standardized and not nec-
essarily written or negotiated.
The use of Web services in a Service-Oriented
Architecture (SOA) allows for the flexible and loose
coupling of applications in platform and language
independent manner. It accelerates application inte-
gration and facilitates rearranging the sequence of
required components as needed. However, commu-
nications of distributed systems are naturally less
reliable and slower than direct code invocation and
shared memory. Further, there are additional secu-
rity and privacy consideration in particular for ser-
vices transmitting confidential patient information
and cases in which the Web service data is directly
used for patient treatment.
Application of Web services in clinical areas and
related-fields as opposed to payer and business areas
are not very common. A few examples of their use
have been described (Cheng, Yang, Chen, Chen, &
Lai, 2004; Eaton, 2006; Jiang, 2004; Mykkänen,
Riekkinen, Sormunen, Karhunen, & Laitinen, 2007).
3.1 Standards
The Web services programming stack (Figure 2) is a
collection of standardized protocols that are used to
implement Web services (Gottschalk, Graham, Kre-
ger, & Snell, 2002). The foundation of distributed
Web services is the network layer. It is based on
HTTP allowing accessing the service from within a
hospital network through its firewalls. On top of the
network layer, an Extensible Markup Language
(XML)-based messaging protocol ensures the me-
chanics of the Web services. The Simple Object
Access Protocol (SOAP) is used to invoke method
calls for the content needed. Descriptions in WSDL
give details of the mechanics and the available ser-
vices of the interface. Available services and their
location (URI) are known to the service requesters
by informal means. However, publication and dis-
covery of Web services could be implemented using
the Universal Description Discover and Integration
(UDDI) standard. The service flow layer allows the
composition of services to an application. It has been
implemented proprietarily.
Figure 2: Web services programming stack.
Security, manageability, and quality of service apply
to all the discussed layers.
3.2 Security and Reliability
Web services are suspect to common threats of net-
worked data exchanges such as message alteration,
confidentiality, man-in-the-middle, spoofing, denial
of service, and replay attacks (W3C 2004). Such
attacks can be prevented by point-to-point security
technologies that secure the transmission from one
Web services to another or, if routed through multi-
ple services, by end-to-end security measures.
For the use of medical content as described,
message alteration and denial of service are possible
security risks. However, point-to-point technologies
are sufficient to secure the transmission since mes-
sages are not routed among service providers. To
USING WEB SERVICES TO DYNAMICALLY EMBED MEDICAL CONTENT IN A CLINICAL INFORMATION
SYSTEM
293

achieve this security, password authentication of the
requester and encryption of the communications link
using the Secure Socket Layer (SSL) protocol are
considered sufficient. Confidentiality attacks and
privacy concerns are not relevant for the discussed
system since there is not enough data transmitted to
identify a patient. Age and gender in conjunction
with physiological data alone is in most cases not
sufficient to deduce the identity of a patient.
Additionally, since the information system is
used in an information technology (IT) environment
that is not directly controlled by either party, it is
important to consider that Web service calls need to
be able to flow through organizations’ firewalls. It
can be tunnelled through existing ports and proto-
cols, which makes this less of an issue.
Requesting services over a public network in-
volving a requesting and providing agent, is intrinsi-
cally less reliable than local services. It can be dis-
tinguished between message reliability and service
reliability. If no answer can be retrieved an error
message is thrown. It would be possible to offer a
fail-over service provider that could be hosted within
a hospital network. Before values are submitted to
the service, the values are checked on the client.
They are checked for their validity and reviewed by
the clinician when documenting a visit. Failures are
not safety critical.
4 APPLICATION
The Web services consuming software application is
a web-based emergency department information
system (EDIS) that provides functionality required
by clinicians such as patient tracking, registration,
clinical workflow and task management, physician
and nursing documentation, orders, and post-
disposition management. The server-based applica-
tion is interfaced with several other information sys-
tems in the hospital such as the main registration
system, laboratory systems, pharmacy systems, bill-
ing and coding systems, etc.
The workflow in emergency departments de-
pends on forms and documentation requirements
vary significantly from site to site. Therefore, the
clinical documentation component allows medical
administrators to build and customize their own
forms. The form building process may be performed
via a drag-and-drop interface where UI elements are
selected from a library of elements. Further, meta-
data such as charge codes, clinical identifiers, risk
elements, and wording data can be attached. The
content elements could be stored in a library.
Once customizations have been finished the con-
tent is published and is used for documentation by
clinicians. Documentation is complaint-driven and
can consist of many different forms, whose sections
are selected dependent on patient attributes such as
age and gender.
4.1 Architecture
Clinical documentation forms are created in the con-
tent builder component. The elements that make up a
form are stored in a relational database containing
the metadata, but no presentation layer data. The
data is separated from the presentation layer, which
allows using the form definition data in a different
context such as for PDAs and paper forms for digital
pen devices.
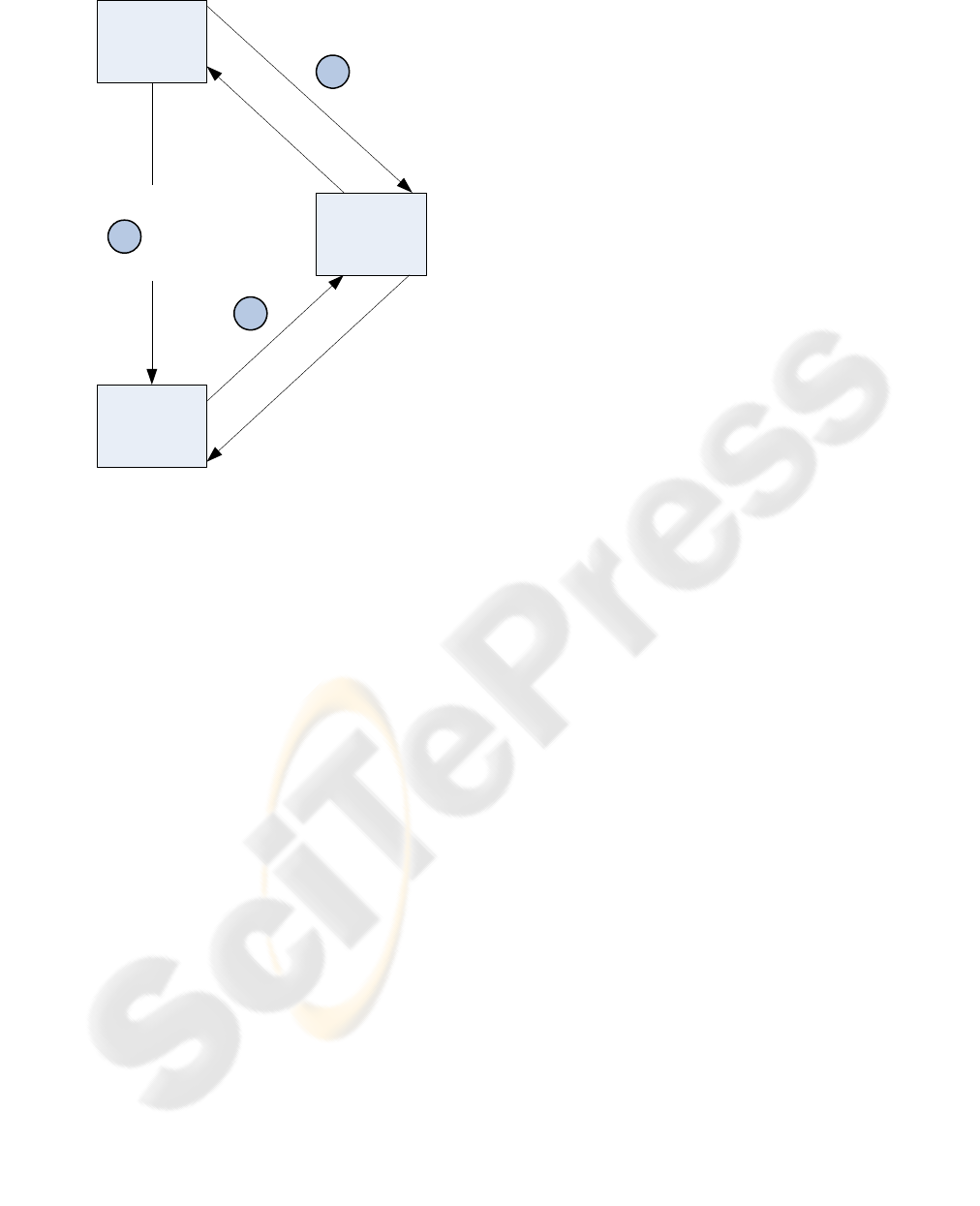
Figure 3 illustrates the process of using the Web
service. In the content builder component the clini-
cal form is assembled. At the location where a medi-
cal or dosage calculation is required, a generic calcu-
lator widget is positioned. A list of available calcula-
tors is presented to the user. This list could be re-
trieved through the Web service also, but is kept
locally for performance and manageability reasons.
The current prototype can contain hundreds of dif-
ferent calculators.
When the calculator is selected a Web service
call is made to the ASP service with the needed cal-
culator identifier (1). The Web service responds with
an XML document containing the field data for the
requested calculator. In the response, each required
data field is specified with label, variable name, and
data type. If the data type is an enumeration all pos-
sible options including their text and data representa-
tion are included. Further the formula used to calcu-
late the result is provided in Reverse Polish Notation
(RPN), where applicable.
The response is parsed and the UI elements are
dynamically generated (2). Since the presentation
layer is built using an object-oriented hierarchy of
classes the received data has to be mapped so that
the necessary objects can be instantiated. The entire
form containing also non-Web service retrieved
elements is then rendered to be used in the applica-
tion. During form creation, response time and per-
formance are not a primary concern since the form is
compiled into an intermediary format and cached
locally.
HEALTHINF 2008 - International Conference on Health Informatics
294
Web Service
Content
Builder
Application
X
M
L
R
e
q
u
e
s
t
G
e
t
M
e
d
C
a
l
c
B
y
I
D
(
)
X
M
L
R
e
s
p
o
n
s
e
a
r
r
a
y
O
f
R
e
s
u
l
t
s
UI Generation
X
M
L
R
e
q
u
e
s
t
G
e
t
M
e
d
C
a
l
c
R
e
s
u
l
t
(
)
X
M
L
R
e
s
p
o
n
s
e
a
r
r
a
y
O
f
R
e
s
u
l
t
s
1
2
3
Figure 3: Architecture.
The response is parsed and the UI elements are
dynamically generated (2). Since the presentation
layer is built using an object-oriented hierarchy of
classes the received data has to be mapped so that
the necessary objects can be instantiated. The entire
form containing also non-Web service retrieved
elements is then rendered to be used in the applica-
tion. During form creation, response time and per-
formance are not a primary concern since the form is
compiled into an intermediary format and cached
locally.
During system use by clinicians the required pa-
rameters are filled in and an Asynchronous
JavaScript and XML (Ajax) request is made to the
Web service to calculate the results (3). The
score/result field is populated with the result as soon
as available. The value can be a string or numeric
type depending on the calculator. Due to the asyn-
chronous nature of the call, the response does not
have to be instantaneous and some delays are toler-
able. If the service is unavailable or does not provide
the expected result an error message is thrown. Al-
ternatively, the request could be routed to a different
service, handled locally, or queued for later retrieval.
4.2 Visualization
The XML response of the Web service containing
the calculator data looks as presented below. Addi-
tionally there is a WSDL service description avail-
able that describes the expected response.
<MedCalcInfo …>
<Error />
<MedCalcID>bish</MedCalcID>
<Title>Bishop</Title>
<Inputs>
<Input>
<Name>Dilation</Name>
<Var>a</Var>
<InputType>Enum</InputType>
…
<Options>
<Option>
<Text>Cervix … <1 cm</Text>
<Value>0</Value>
<Selected>true</Selected>
</Option>
…
</Options>
</Input>
…
</Inputs>
</MedCalcInfo>
The response is parsed and the object hierarchy
is instantiated. The response also specifies the de-
fault values for enumerations as well as data types
that are required. The rendered interface enforces
data type checking using client-side validation. The
UI also consists of data types unknown to the Web
service. For example, in medicine the concept of
pertinent negatives is constantly encountered. This
means that such an element can assume three differ-
ent states: not answered, positive, or negative. In the
UI this concept is implemented as a checkbox that
can be negated by cycling through its different states
by clicking the mouse repeatedly. Positive values are
represented in a circled manner; negative values are
displayed slashed. This application specific UI com-
ponent could be considered a type of “SuperCheck-
box”.
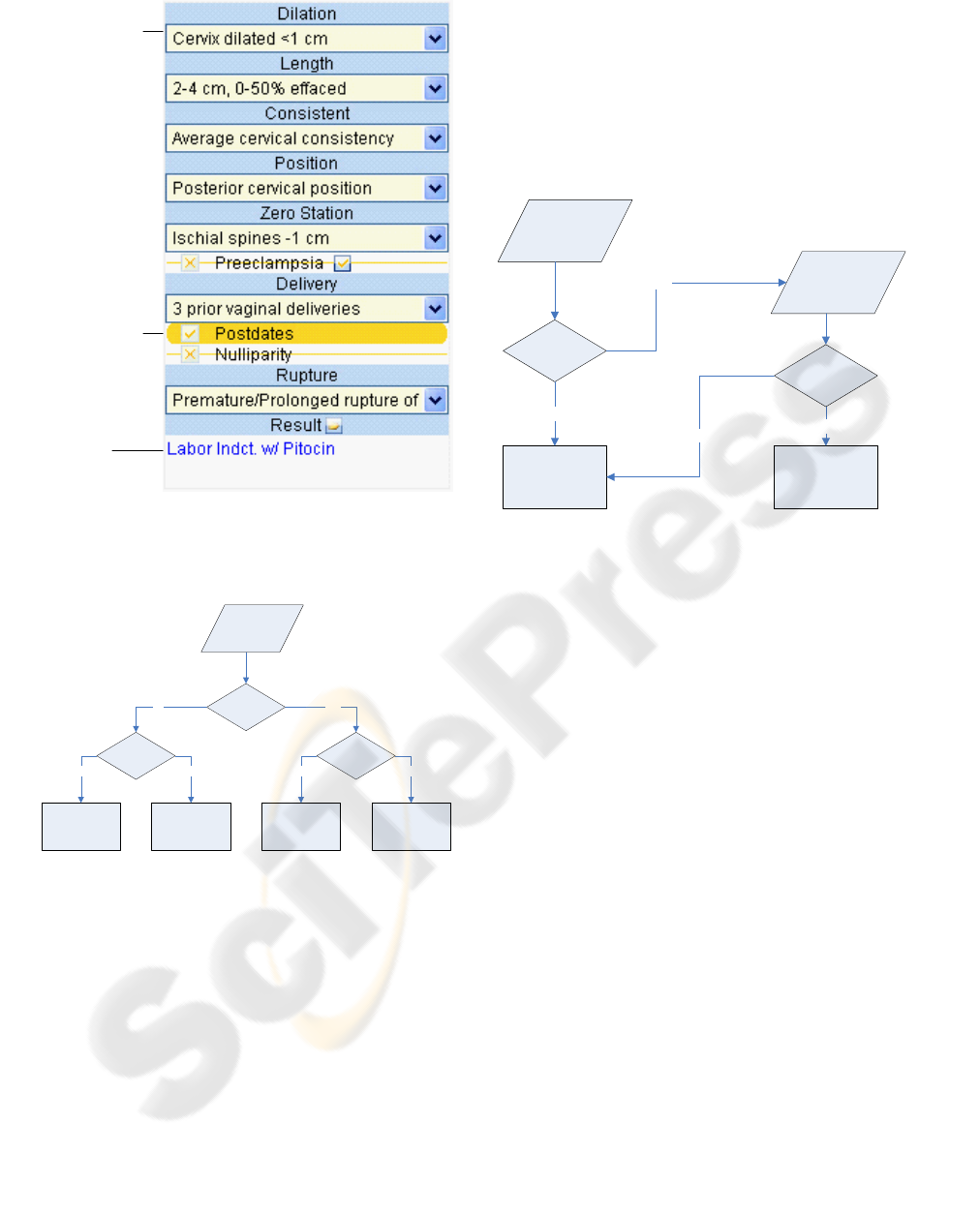
Figure 4 shows how the different data types are
displayed for the end users. This concept has to be
mapped from the Web service response. Enumera-
tions that are specified as yes/no option value are
visualized as SuperCheckbox instead of a dropdown.
USING WEB SERVICES TO DYNAMICALLY EMBED MEDICAL CONTENT IN A CLINICAL INFORMATION
SYSTEM
295
Enum Field
(1...n option)
Enum Field
(yes/no
option)
Result
Field
Figure 4: Dynamically generated user interface.
The UI element types are selected according to
the criteria presented in Figure 5.
Enumeration
Yes/no options
Yes
TextField
No
DropDown SuperCheckbox
YesNo
Check data
type
Datetime
No
Calendar
Yes
Figure 5: Data type mapping.
Additional to the field definitions received from
the Web service, a result field is rendered to present
the calculated scores or results. The results and val-
ues do not only have to be submitted to the Web
service for calculation but also documented in the
EDIS according to site-specific guidelines. The re-
quest and response are validated by the service
whether they lie in a sensible range.
4.3 Integration
Many values that are used in calculators are already
available in the system either through manual data
entry using different forms or through data interfaces
with external systems. Such values include vital
signs, weight, height, age, gender, etc. These values
can be automatically imported and pre-selected in
the appropriate UI elements. To provide real seman-
tic integration, a system would require the use of a
common nomenclature. String parsing, mapping,
and data type checking could be applied, which in
conjunction would provide the required reliability.
Check field
identifier
Match
Empty field
No
Retrieve
field value
Yes
Populate field
Correct data
type
Yes
No
Figure 6: Populate fields with existing data.
The quality of the described system can be assured by
automated unit tests that query the Web services for sev-
eral test cases. They also record the access time and la-
tency of the service response time. The UI is also tested
via a test automation framework.
4.4 Measurements
As indicated above, response times and reliability of
the discussed Web services are of some concern.
This is in particular the case for the calculation of
medical results. Whereas some delays are acceptable
due to asynchronous calls, response times should
generally not be beyond a 4 second threshold.
The measurements were taken querying the Web
services over the internet over a distance of 14 hops.
The average roundtrip time was 43 milliseconds.
The services were tested with 1 to 20 concurrent
clients. For each client 100 samples were taken. The
infrastructure is scalable but further prototype de-
velopment is required to identify practical limits.
Table 1 shows the results for retrieving the calcu-
lator data during form administration. During the
test, all requests could be completed successfully.
Generally not more than 5 concurrent users are ex-
pected to use the administration tool at any given
time. Rendering times of the data are negligible.
Table 1: Response times in seconds of calculator service.
HEALTHINF 2008 - International Conference on Health Informatics
296
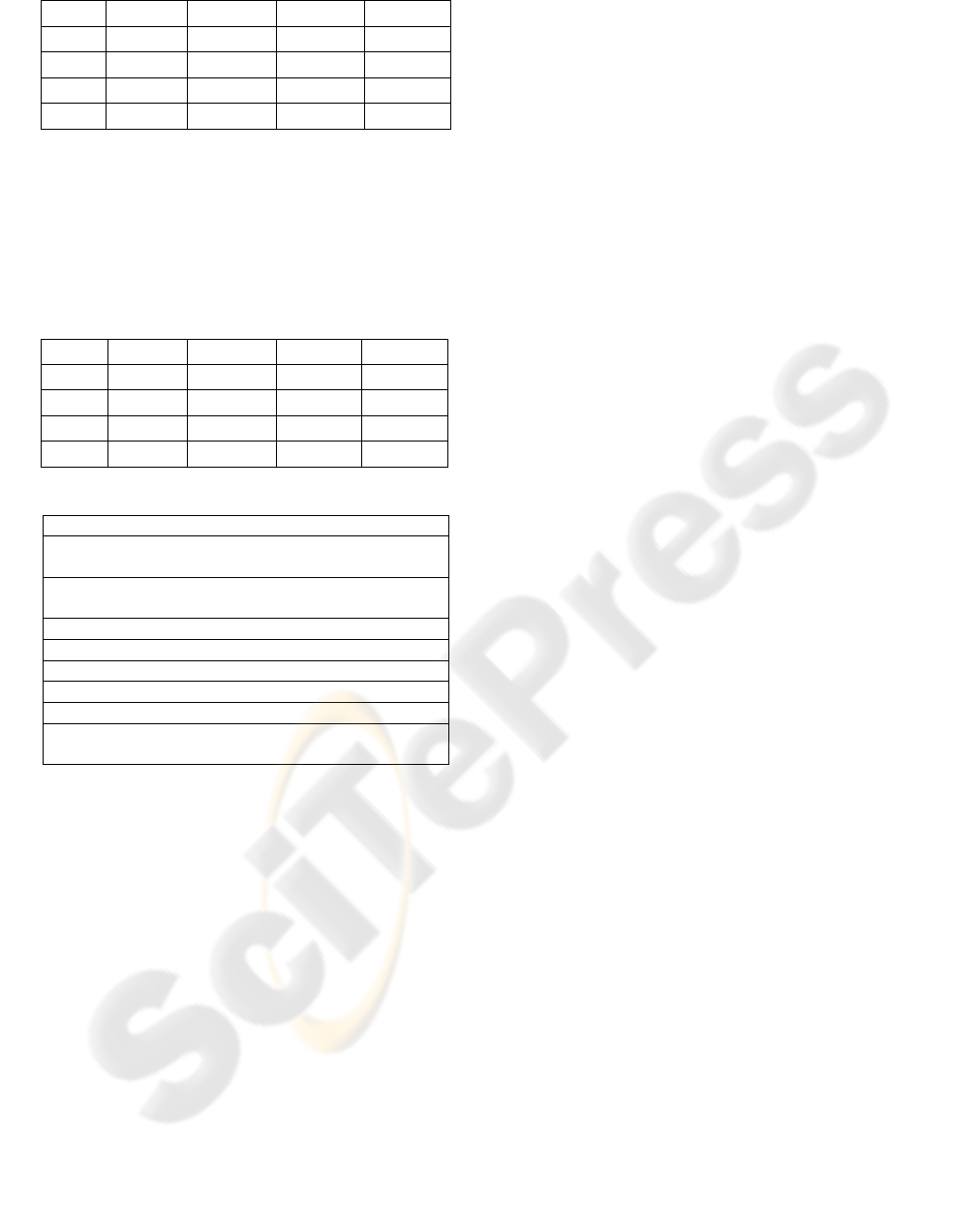
Clients Average Minimum Maximum Deviation
1 0.4930 0.3750 0.7500 0.0638
5 1.8393 0.4220 2.5310 1.1898
10 3.7522 0.4840 12.3140 1.8493
20 8.8832 0.3590 62.3220 5.7396
Table 2 lists the response times of the Web ser-
vice that calculates the results. It performs slightly
better using the same number of concurrent clients.
An acceptable wait time is arbitrarily set at 4 sec-
onds. To process more concurrent clients beneath
that threshold the infrastructure would need to be
load-balanced.
Table 2: Response times in seconds of result service.
Clients Average Minimum Maximum Deviation
1 0.6528 0.3120 3.0160 0.3870
5 3.1357 0.3440 14.1410 3.8315
10 3.4759 0.4530 12.9840 1.3377
20 7.8717 0.6250 27.4390 3.3215
Table 3: Conclusions.
Advantages
Immediate updates of frequently changing medication
information and no maintenance of additional servers.
Vast amount of available medical content for immedi-
ate use with minimal integration effort.
Seamless integration with clinical documentation.
Ability of user customization of clinical content.
Disadvantages
Dependence on external service.
Potential service outages and response time problems.
Regulatory and liability implications need to be deter-
mined.
5 CONCLUSIONS
This paper showed how medical content can be dy-
namically integrated into a clinical information sys-
tem. The primary challenge was the seamless inte-
gration of external content into a customizable UI.
The components are rendered on-demand but still
can be transparently arranged by medical system
administrators.
Whereas the retrieval of the form definition data
is only performed during system customization, the
retrieval of results occurs during the documentation
by clinicians and requires a higher level of availabil-
ity. Reliability was found to be high for the de-
scribed service and security requirements can be
fulfilled by point-to-point security technologies.
It was found that the advantages generally out-
weigh the disadvantages. The potential of having a
vast amount of external content available without a
significant integration effort was considered to be
the biggest advantage. Further, having this content
available using an ASP concept as opposed to in-
house hosting reduces maintenance to a minimum
for the service requester.
Future research is needed to address the accep-
tance of this content by clinicians. Also, the re-
sponse times and reliability over a high number of
customers needs to be considered. In a next step,
patient history from other systems could be inte-
grated using Web services across network bounda-
ries. Also, legal and regulatory concerns need to be
addressed.
REFERENCES
Cheng, P., Yang, C., Chen, H., Chen, S., & Lai, J. (2004).
Application of HL7 in a collaborative healthcare in-
formation system. Paper presented at the Engineering
in Medicine and Biology Society, 26th Annual Inter-
national Conference of the IEEE.
De Sousa, B. (1996). Prescription problems: clinical phar-
macology and lawsuits. Texas Medicine, 92(5), 57.
Eaton, A. D. (2006). HubMed: a web-based biomedical
literature search interface. Nucleic Acids Research, 34,
W745–W747.
Gottschalk, K., Graham, S., Kreger, H., & Snell, J. (2002).
Introduction to web services architecture. IBM Systems
Journal 41(2), 170-177.
Jiang, K. (2004). Integrating clinical trial data for deci-
sion making via web services. Paper presented at the
Engineering in Medicine and Biology Society, 26th
Annual International Conference of the IEEE.
Knollmann, B., Smyth, B., Garnett, C., Salesiotis, A.,
Gvozdjan, D., Berry, N., Lee, H., & Min, D. (2005).
Personal digital assistant-based drug reference soft-
ware as tools to improve rational prescribing: Bench-
mark criteria and performance. Clinical Pharmacology
& Therapeutics, 78(1), 7-18.
Lapinsky, S. E., Wax, R., Showalter, R., Martinez-Motta,
J. C., Hallett, D., Mehta, S., et al. (2004). Prospective
evaluation of an internet-linked handheld computer
critical care knowledge access system. Critical Care,
8(6), 414-421.
Mykkänen, J., Riekkinen, A., Sormunen, M., Karhunen,
H., & Laitinen, P. (2007). Designing web services in
health information systems: from process to applica-
tion level. International Journal of Medical Informat-
ics, 76(2-3), 89-95.
Pronovost, P. J., Angus, D. C., Dorman, T., Robinson, K.
A., Dremsizov, T. T., & Young, T. L. (2002). Physi-
cian staffing patterns and clinical outcomes in criti-
cally ill patients. The Journal of the American Medical
Association, 288(17), 2151-2162.
W3C (2004). Web services architecture. Retrieved 2007-
06-11, 2007, from http://www.w3.org/TR/ws-arch/wsa.pdf
USING WEB SERVICES TO DYNAMICALLY EMBED MEDICAL CONTENT IN A CLINICAL INFORMATION
SYSTEM
297
