
INTRODUCING A MOBILE SYSTEM FOR THE EARLY
DETECTION OF CARDIAC DISORDERS AS A PRECAUTION
FROM A CARDIOLOGISTS’ VIEW
Evaluation of a Survey
Onur von Burg, Marco Savini, Henrik Stormer and Andreas Meier
University of Friborg, Boulevard de Prolles 90, 1700 Fribourg, Switzerland
Keywords:
Cardiology m-health e-health mobile survey heart.
Abstract:
This paper illustrates the results of a survey of practicing cardiologists that were asked about various aspects
of a simplified telecardiology scenario using mobile devices. Such devices are becoming ubiquitous assets in
everybody’s life. Their application in a healthcare environment aims not only at supporting the patients over
traditional consultations but also maximizes the content of their health status information. The results of the
survey may help application developers to focus their efforts of applications in a similar setting.
1 EHEALTH AND MHEALTH
(Haas, 2006) defines eHealth as
...the application of Internet and other re-
lated technologies in the health care industry
to improve access, efficiency, effectiveness,
and quality of clinical and business processes
used by health care organizations, practition-
ers, patients, and consumers to improve the
health status of patients.
mHealth extends this notion by considering mo-
bile actors (patients, health professionals, ...) and
their environment. (Istepanian et al., 2006) simply de-
fine it as ”emerging mobile communication and net-
work technology for health care”. Certain areas of
eHealth like monitoring over distance can be greatly
improved when considering ubiquitous mobile de-
vices. (del Pozo et al., 2006) defines that potential
needs should meet certain criteria so that:
• eHealth services should be provided at any time
and any place, depicting the need for efficient,
ubiquitous and secure institutional care.
• Efficient coordination tools should be provided to
all health professionals dealing with each single
patient, in order to allow the implementation of
patient centered care.
The recent advances in mobile technology like
higher bandwidths or powerful smartphones with ad-
vanced features allow the creation of new medical ap-
plications that support both patients and doctors.
A number of researchers have worked on the idea
of assigning mobile devices to patients. It is possible
to distinguish between the following three domains:
1. Mobile devices are used to help the patient by pro-
viding information.
2. Mobile devices are used to transmit physiological
parameters.
3. Mobile devices are used to alert patients or med-
ical professionals when certain physiological pa-
rameters become critical.
The dialogue-based monitoring system in
(Komninos and Stamou, 2006) aims at supporting
elderly people in their preferred environment and can
therefore be assigned to the first domain.
The MOEBIUS project (Mobile extranet-based
integrated user services) that integrates doctors and
patients by submitting different physiological param-
eters (Fischer et al., 2006) can be considered as an ap-
plication of the second domain. Similarly, (Leimeis-
ter et al., 2005) describes the usage of mobile devices
in order to assist young cancer patients and concludes
that the usage of such a system has a number of ad-
vantages: higher compliance of appointments with
alerting functionality, higher data quality, less work
for the doctor to prepare the documentation as well as
less errors in the documentation. The use of context
44
von Burg O., Savini M., Stormer H. and Meier A. (2008).
INTRODUCING A MOBILE SYSTEM FOR THE EARLY DETECTION OF CARDIAC DISORDERS AS A PRECAUTION FROM A CARDIOLOGISTS’
VIEW - Evaluation of a Survey.
In Proceedings of the First International Conference on Health Informatics, pages 44-50
Copyright
c
SciTePress

in a mobile healthcare scenario using the information
groups Who, Where, When, Why and What has been
described in (Savini et al., 2007).
An example of the third domain collecting real-
time electrocardiogram signals including basic ar-
rhythmia detection with automatic alerting to a call
center is illustrated in (Liszka et al., 2004). Their
system architecture uses readily available commercial
off-the-shelf components.
1.1 Cardiology
1.1.1 Overview
Cardiovascular reasons represent the largest cause of
death in Switzerland with 37% of all deaths in 2004
(Junker, 2007). It is followed by cancer related deaths
with 26%. While the percentage of cardiovascular
related deaths of the 65 years and older increases
to 41.7%, it still contributes with 20% of all deaths
within the youngerage group of the 45 to 64 year olds.
Similar data exists in the EU with approximately 40%
of all deaths related to cardiovascular diseases (Euro-
stat, 2002, Chapter 8).
1.1.2 Cardiac Disorders
In (Guidant, 2007) the following general types of
heart diseases are identified:
Problems with the Heart’s Electrical System. If
the tissue that produces and sends electrical im-
pulses to the heart muscle is damaged, abnormal
heart beatings can occur in different variants:
Bradycardia (unusually slow or unsteady rhythm),
Tachycardia (more than 100 beats per minute),
Atrial fibrillation (the upper chambers of the heart
beat between 300 and 600 times per minute) and
Sudden Cardiac Death (heart stops to beat and
pump suddenly and unexpected).
Problems with the Heart’s Arteries. These prob-
lems represent the most common heart disease
in western countries. Fatty plaque builds up in
the arteries and less blood flows through the heart
muscle. This is illustrated in figure 1.
Problems with Arteries Outside the Heart. This
disease type also identifies the building up of
fatty plaque, but outside the heart, so less blood
flows through the body. If the blocked artery is
supplying the brain with blood, the patient may
experience a stroke in the worst case.
A thorough introduction into cardiology is given
in (Crawford et al., 2003).
Figure 1: Coronary heart disease (Know Heart Diseases,
2007).
1.1.3 ECG
An electrocardiogram can be defined as a non-
invasive test to reflect underlying heart conditions by
measuring the electrical activity of the heart and pro-
ducing an output in the form of a continuous strip
graph. Early analysis and exploration of the heart’s
electrical system and its measuring techniques were
examined by Willem Einthoven in the early 1900’s
(Biel et al., 2001).
The basic approach is to put electrodes on the
body. The following three types of ECGs can be iden-
tified:
Resting. Taken within a couple of seconds.
Activity. Taken under physical activity.
Long-term. Usually taken during a 24 hour period.
The number of leads indicates the quality of the
measurement. 12 leads ensure that all parts of the
heart are recorded. It is generally accepted that ECG
measurements with 3 leads ensure credibility (Burger
and Osswald, 2003).
Various research has already been conducted re-
garding the transmission of ECG data. (Nollo et al.,
2000) describes the national project ”Territorial Tele-
Cardiology” which focuses on providing experts with
EGC data from medical ambulatory locations and pa-
tients homes. The average time of response is 1.5
days. The project demonstrated the feasibility and
utility of a telecardiology network that offers im-
proved access and quality in rural areas.
The design of a wearable device for ECG moni-
toring has been presented in (Led et al., 2004). The
paper describes the usage of Bluetooth technology to
transfer the ECG data to a mobile base unit.
Compression of ECG data is a topic that is very
important in a homecare scenario, due to the limited
bandwidth available over mobile networks and the
high amount of data which is generated. An overview
of various methods and research for the compression
of biosignals is given in (Hadjileontiadis, 2006).
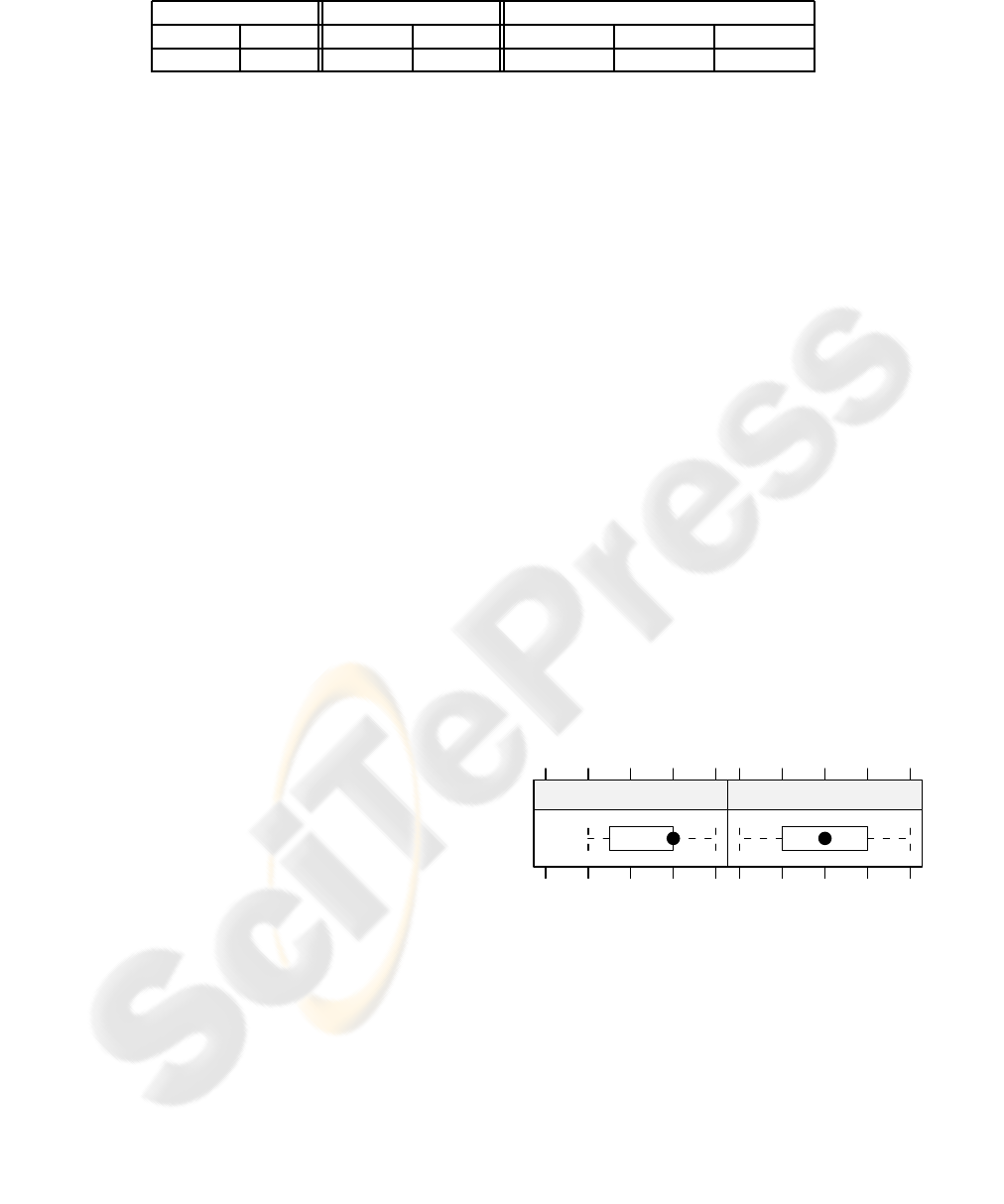
Table 1: Return rates.
Region Infrastructure Size of Location
German French Hospital Practice > 100’000 > 30’000 < 30’000
35.7% 35.6% 61.5% 33.1% 29.2% 26.3% 45.4%
2 SURVEY RESULTS
The main motivation for the survey was to understand
how cardiologists think about a telemonitoringsystem
as an instrument for the detection of heart-related dis-
orders. The main goal hereby was to research various
components of how such a system should be built and
what focus it should have in order to receive a high
acceptance with the people that will eventually have
to introduce such a system to the patients.
2.1 Approach
The printed questionnaires were sent on the 13th of
March 2007 to 277 (out of totally 533) practicing car-
diologists in Switzerland. French and German ques-
tionnaires were used to address the corresponding lin-
guistic regions in Switzerland. The Italian region was
not considered in this survey. 100 questionnaires were
returned without any special follow ups, resulting in
a total return rate of 36.1%. Table 1 illustrates the
various return rates relative to various variables.
2.2 Structure of the Questionnaire
In order to design the questionnaire, some aspects
from (Berekhoven et al., 2006) were applied:
• Interesting subject matter.
• Questionnaire as short as possible.
• Composition as interesting as possible.
• Questions as logical and easy as possible (optical
as well).
Prior to the creation of the questionnaire an inter-
view was held with a practicing cardiologist who has
some background in the field of telecardiology. The
result was a total of 12 questions that can be grouped
into two categories:
• Questions regarding ICT usage in cardiology in
general.
• Specific mobile telecardiology application related
questions.
A simplified process of a possible mobile telecar-
diology use case was illustrated on the first page of
the questionnaire in order to give the respondents an
idea about the intention of the survey.
The box-and-whisker diagrams used throughout
this paper in order to illustrate the responses use a
filled circle as median of the response and the po-
sition of the dot within the box gives an indication
about the skew of the data. The dotted lines define the
whiskers which can be seen as the smallest or biggest
non-outlier observations. Eventual outliers are drawn
as empty circles.
2.3 ICT in Cardiology
Two questions address the use of ICT within cardi-
ology. In one question, the cardiologists were asked
about their opinion on how they judge the desire of
their patients to have innovative applications for treat-
ment and diagnosis. 28.3% of the cardiolists think
that their patients have a fairly strong desire for in-
novative applications. The correlations of these re-
sults with the demographic variables shows that the
geographical region or the size of the location of the
cardiologists does not influence the results. However,
there is a correlation to the type of infrastructure the
cardiologists operate in, indicating that cardiologists
working in hospitals evaluate the desire of patients for
new medical applications slightly higher than cardiol-
ogists in practices (see figure 2).
(1: strongly disagree, 5: strongly agree)
1 3 5
Hospital
1 3 5
Practice
Figure 2: ICT usage for patients in cardiology.
The second question regarding ICT addresses the
perspective of the cardiologists and asked if ICT is
used sufficiently in cardiology. The mean is very sim-
ilar to the former question. Compared to the infras-
tructure the cardiologists operate in, there is no dif-
ference between practices and hospitals, unlike to the
former question. The results for both questions are
illustrated in figure 3.
In summary, the followingstatements can be made
in regard to ICT usage in cardiology:
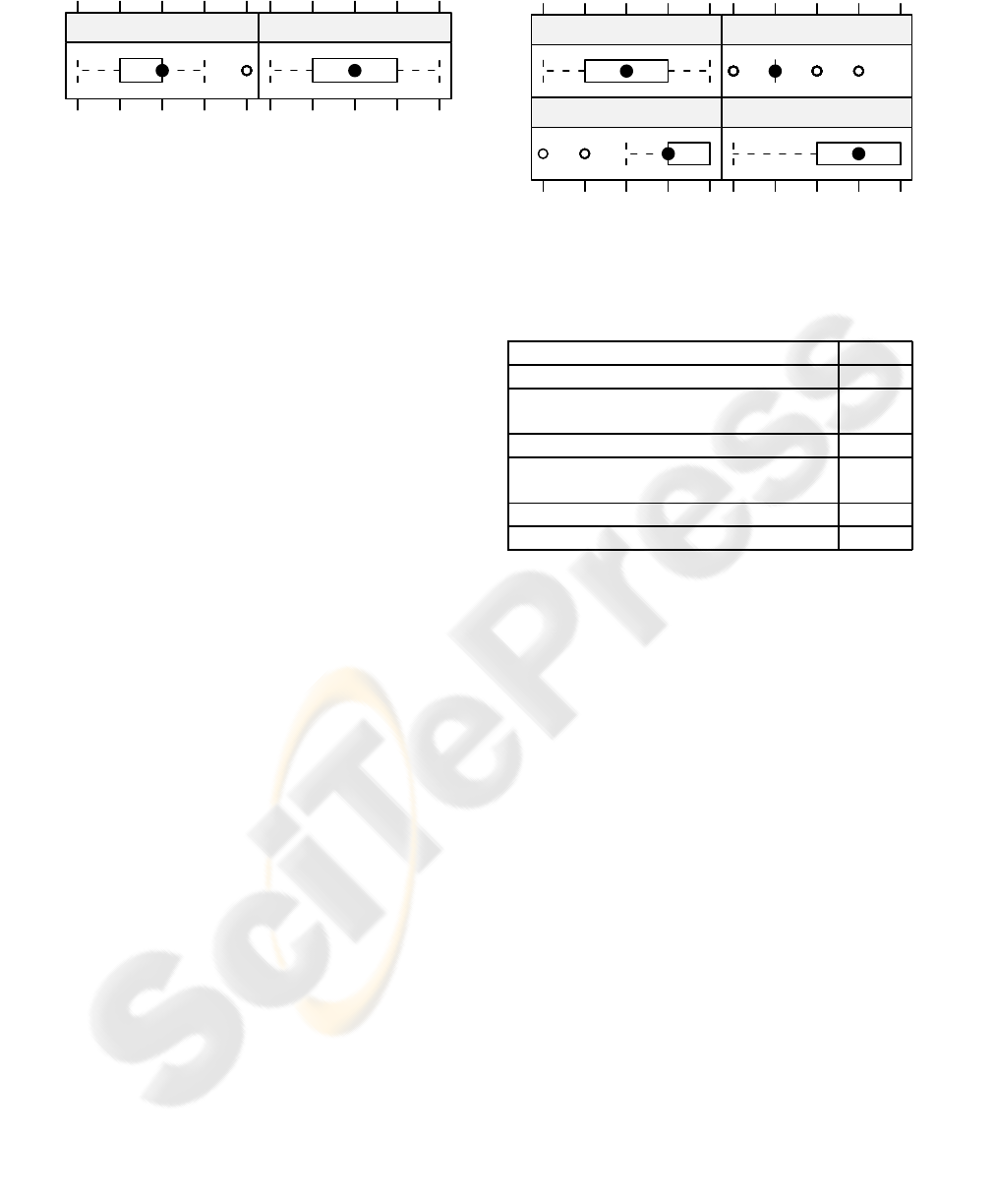
(1: strongly disagree, 5: strongly agree)
1 3 5
ICT for Cardiologists
1 3 5
ICT for Patients
Figure 3: ICT usage in cardiology.
• Patients have a certain desire for innovative appli-
cations in cardiology.
• Hospitalized patients have a higher desire for ad-
ditional ICT in cardiology than patients in prac-
tices.
• Cardiologists feel that today’s ICT usage in cardi-
ology is fairly sufficient.
2.4 Motivation and Components in
Telecardiology
Questions regarding the components in a telecardiol-
ogy setting can be broken down into three main cat-
egories: The Patient category analyzes the abilities
and the reasons of patients to use such a system. The
questions in the category Patient-end System Compo-
nents emphasize on various scenarios and number of
leads that are necessary to measure an ECG. Further-
more, it investigates if the viewing of the ECG on
a mobile base unit makes sense. The final category
Cardiologist-end System Components ad
2.4.1 Patient Ability
The cardiologists were asked to evaluate the ability
of their patients within certain age groups to record
and send their ECG data in a given scenario. The re-
sults shown in figure 4 are not surprising. Cardiolo-
gists judge that about half of their 60 to 70 years old
patients are able to record and send ECG data. The
confidence is considerably higher for their younger
patients.
2.4.2 Reasons for Patients
Possible reasons for using such a telecardiology sys-
tem were investigated in a separate question. The total
results, independent of the infrastructure or geograph-
ical region, are summarized in table 2.
Not surprisingly, the number one motivation is
giving better access to patients living in rural areas.
Cardiologists living in hospitals consider this even
(1: none, 3: about half, 5: almost all)
1 3 5
30−45 45−60
60−70
1 3 5
70−100
Figure 4: Patient ability per age group.
Table 2: Possible reasons for patients.
Reason Agree
Cardiac patients who live in rural areas 58.6%
High quantity of elderly patients with
limited mobility
42.4%
Higher service in quality and treatment 39.4%
Growth of mobile users with easiness
to send ECG data
36.4%
Time gain for patients 32.3%
Reduction of costs 18.2%
more important (75%) than their colleagues in prac-
tices (55%). The next four reasons are all rated with
about the same importance. Interestingly, altough car-
diologists assess elderly patients as less able to use
such a mobile application (see figure 4), their limited
mobility is ranked as number two reason. Further-
more, the possible time gain for patients using such
a solution is judged positively by 50% of all cardi-
ologists in hospitals as an important reason, whereas
only 29% of practices see it like that.
2.4.3 System Components for Patients
This section of the questionnaire addresses various
component settings and scenarios on the patient side
for a mobile telecardiology application.
The first question considers various usage scenar-
ios for patients and asked the cardiologists to evaluate
their view which is illustrated in figure 5.
Only one of the proposed scenarios, the perma-
nent transmission of ECG data for high risk patients,
received a relatively high response. Regarding the
periodic transmission of ECG data as a precaution,
the cardiologists in big cities valued it slightly higher
(mean 2.06) than their colleagues in towns (mean
1.79); this could be explained with the fact that car-
diologists in big cities tend to treat more patients for
routine check-ups.
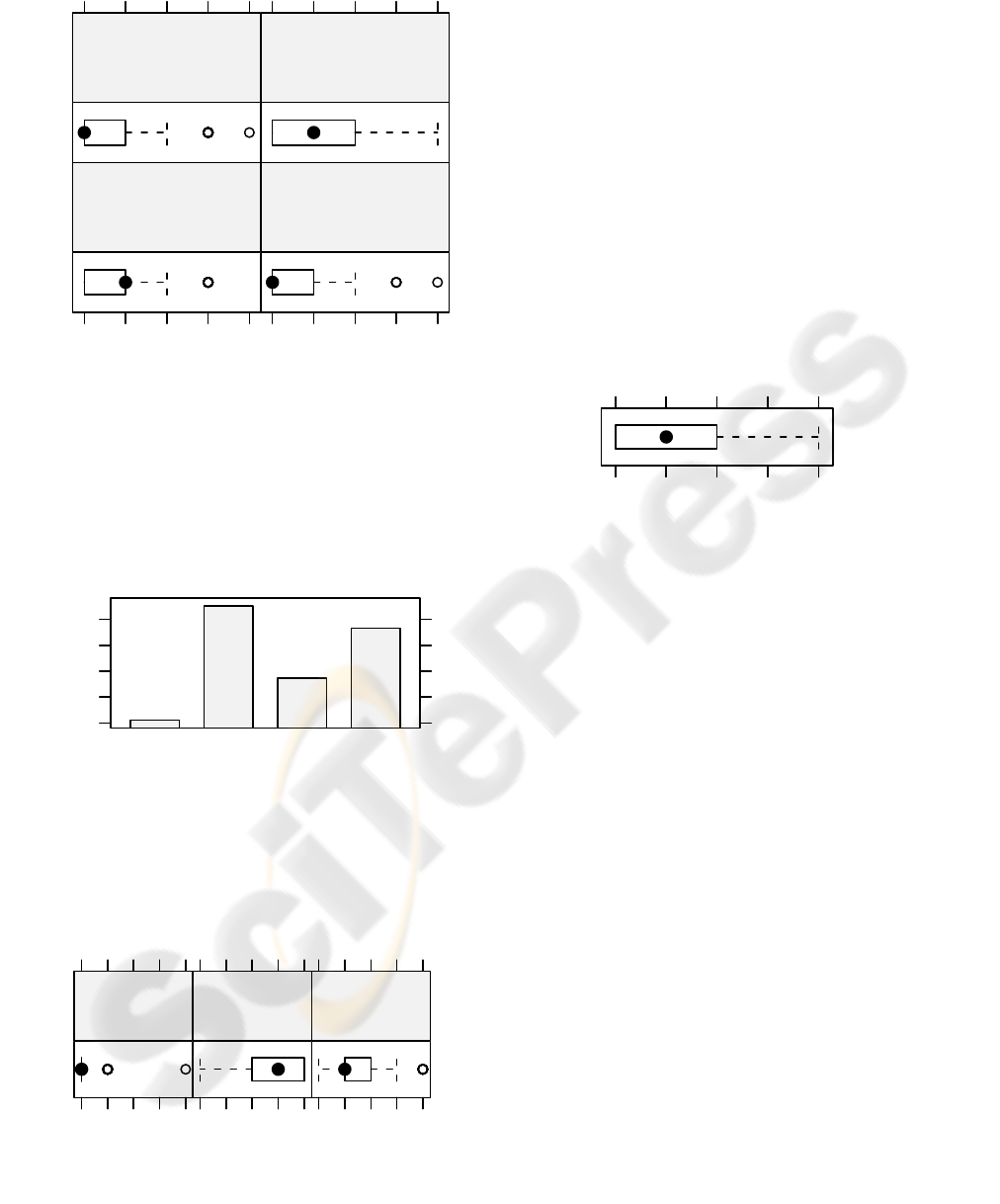
(1: absolutely unnecessary, 5: absolutely necessary)
1 3 5
Analysis of ECG data during
physical activity
for competitive athletes
Periodic transmission as
precaution for Sudden Child
Death Syndrome
Periodic transmission for
adults to cardiologists as
a precaution
1 3 5
Permanent wearing of sen−
sors with connection to an
emergency center for
high rish cardiac patients
Figure 5: Usage scenarios.
The second question addresses the number of
EGC leads necessary for a mobile application in order
to reliably record the ECG of a patient. The distribu-
tion in figure 6 clearly illustrates two preferences: 3
leads and 12 leads.
Percent
0
10
20
30
40
1 lead 3 leads 6 leads 12 leads
Figure 6: Number of leads preference.
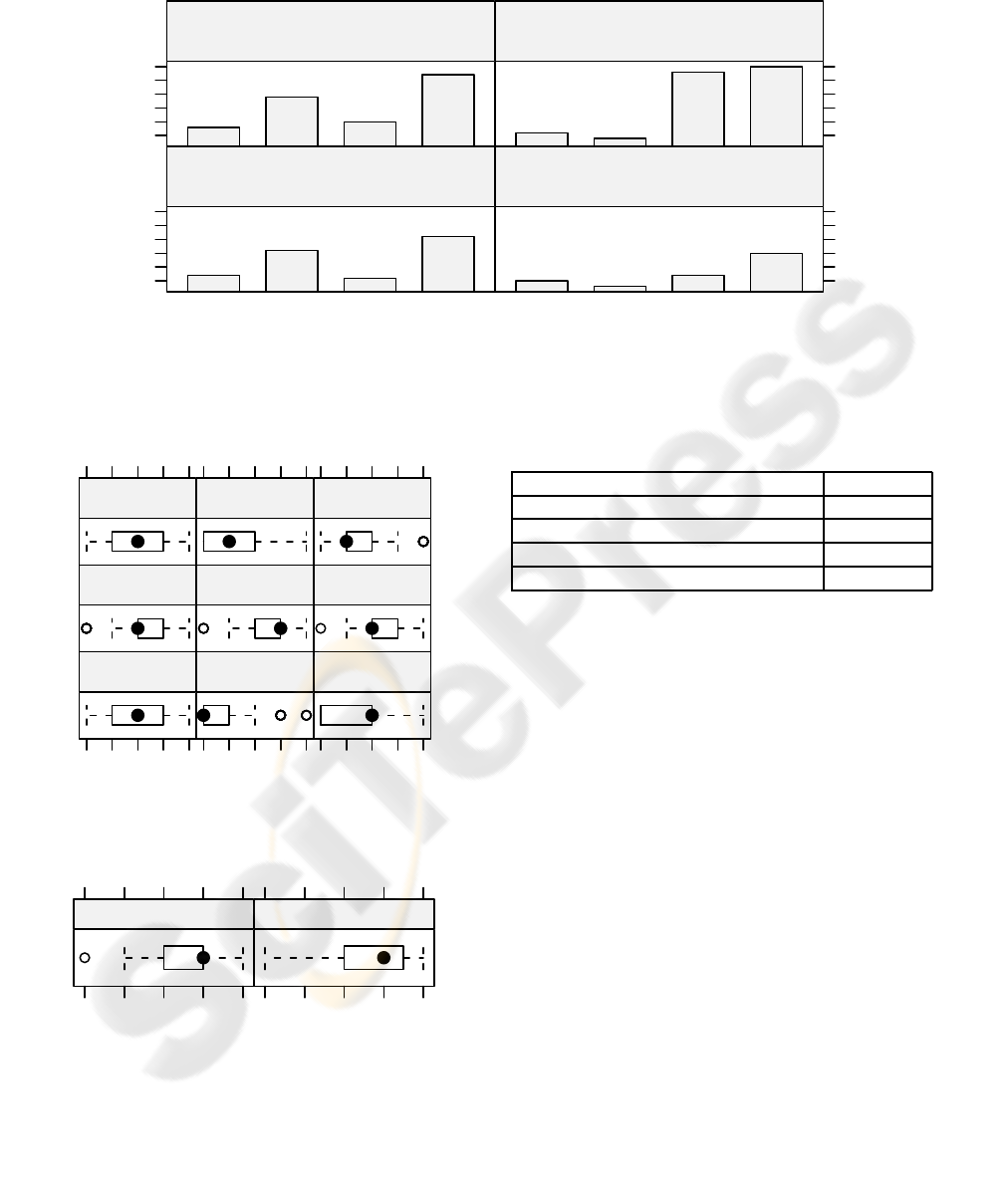
The evaluation of the effectiveness of diagnostics
using a mobile application for the three main types of
cardiac diseases is addressed in the third question and
its results illustrated in figure 7.
(1: not diagnosable, 5: very effective diagnosis)
1 2 3 4 5
Problems with
the arteries out−
side the heart
1 2 3 4 5
Problems with
the hearts’ elect−
rical system
1 2 3 4 5
Problems with
the hearts’
arteries
Figure 7: Evaluation of disease types.
Problems with the arteries outside the heart do not
represent situations that can be diagnosed using ECG
sensor leads. In relation to the number of leads, pa-
tients that haveproblems with the hearts’ arteries typi-
cally will use 12 leads and such applications will have
to consider the larger data sets required. For patients
that use such a mobile application as precaution for
the heart’s electrical system, a 3 lead ECG sensor ap-
pears to be more realistic.
The final question regarding the system compo-
nents on the client side investigates the need of the
patient to view his own ECG data on the mobile base
unit. The results in figure 8 show that cardiologists do
not consider such a functionality very desirable for
their patients. This might be due to the fact that ECG
diagrams can be quite complex to read and should
thus only be analyzed by experienced professionals.
(1: no necessity, 5: strong necessity)
1 2 3 4 5
Figure 8: Patient desire to view ECG on MBU.
2.4.4 Components in Telecardiology for
Cardiologists
The final part of this section considers the various
components of a mobile telecardiology solution for
the cardiologists themselves. It consists of two ques-
tions: The first question addresses the ICT knowledge
of the cardiologists based on possible components or
technologies that could be used for such a solution
and is illustrated in figure 9.
Internet applications, mobile communication, in-
formation system and PDAs rank highest in the list
and except for technical terms many possible compo-
nents and technologies seem to be known reasonably
well. Cardiologists in practices tend to have similar
or slightly higher knowledge in regard to Internet Ap-
plications, as figure 10 illustrates. The same is true
for mobile technologies and other fields.
This explains also the results of the next question:
The cardiologists were asked about their preferences
how they would like to receive the ECG data of the
patients for the various scenarios already interrogated
in figure 7. A summary of the preferences is ranked
in table 3.
However, the results in figure 11 make it obvi-
ous that the preferred end system heavily relies on the
kind of disease type that is handled with the solution.
Number of Responses
10
15
20
25
30
35
Application
E−Mail
Smartphone
Webbased
Analysis of ECG data during physical activity
for competitive athletes
Application
E−Mail
Smartphone
Webbased
Periodic transmission as precaution for
Sudden Child Death Syndrome
Periodic transmission for adults to cardio−
logists as a precaution
10
15
20
25
30
35
Permanent wearing of sensors connecting to an
emergency center for high risk patients
Figure 11: Preferred end systems per disease type.
(1: never heard of, 3: user knowledge, 5: extensive knowledge)
1 3 5
Bluetooth GPRS
1 3 5
GSM
Information
Systems
Internet
Applications
Mobile
Communications
PDA
1 3 5
Smart Phones UMTS
Figure 9: ICT knowledge of cardiologists.
(1: never heard of, 3: user knowledge, 5: extensive knowledge)
1 3 5
Hospital
1 3 5
Practice
Figure 10: Knowledge about internet applications.
Web-based solutions seem to be a good choice in
most cases. However, smart phones get a very high
rating when the application handles high risk patients
Table 3: Ranked summary of preferred end systems.
System Preference
Web-based solution 38.7%
Smart Phone 24.3%
E-Mail with attachment 21.2%
Dedicated application 15.8%
in an emergency. In such a situation, an e-mail that
may take from minutes up to hours to arrive to the
cardiologist, is not acceptable, even if the emergency
is handled by a dedicated center. However, e-mails
seems to be perfectly acceptable if the matter is about
observing a patient over a longer period of time as a
precaution.
3 CONCLUSIONS AND
OUTLOOK
The work in this paper focuses on the actual needs of
a mobile telecardiology application with the results
obtained from the survey. The conducted survey al-
lows several conclusions for the implementation of a
mobile application in cardiology:
• Except for the oldest age group (70-100), cardiol-
ogists agree that their patients are able to use such
a system.
• Cardiologists do not seem enthusiastic about the
proposed usage scenarios. However, a combina-
tion of factors, such as high risk patients in rural

areas, may strongly contribute to a higher accep-
tance.
• Addressing problems with the hearts’ electrical
system seems to be a widely accepted disease type
for such a mobile application.
• There does not seem to be a strong desire for the
patients to view their own EGC.
• The ICT knowledge of cardiologists and their
preferences imply that, except for emergency sit-
uations, an internet application would be a good
choice for their end system.
Security issues have explicitly been factored out
of the questionnaire in order not to overwhelm the
cardiologists with technical details. However, such
issues are a pivotal part of every health related ap-
plication and contribute highly to the acceptance and
credibility of a system.
3.1 Outlook
In this paper we illustrated the perspective of cardiol-
ogists regarding a mobile telecardiology application
scenario for patients. We would like to extend our
research in the following areas:
• A survey on the patients may give insights about
what elements to consider on the client side. It
would be interesting to analyze the technologi-
cal knowledge split by age group and the willing-
ness of patients to use such a system when offered
some well-defined benefits.
• The usage of standard equipment greatly con-
tributes to a seamless rollout to the public. We
would like to investigate how existing technolo-
gies can be integrated in order to provide a so-
lution that aids the patients and cardiologists and
that is also cost-effective.
• Qualitative interviews with cardiologists might
give us a better idea about possible usage scenar-
ios.
REFERENCES
Berekhoven, L., Eckert, W., and Ellenrieder, P. (2006).
Marktforschung – Methodische Grundlagen und prak-
tische Anwendung. Gabler Press.
Biel, L., Pettersson, O., Philipson, L., and Wide, P. (2001).
ECG Analysis – A new approach in Human Identi-
fication. IEEE Transactions on Instrumentation and
Measurement, 50:808–812.
Burger, P. and Osswald, S. (2003). Das EKG in der
Telemedizin. Swiss Medical Forum, 3:661–643.
Crawford, M. H., DiMarco, J. P., and Paulus, W. J., editors
(2003). Cardiology. Mosby, 2 edition.
del Pozo, F., de Toledo, P., Jimenez, S., Hernando, M. E.,
and Gomez, E. J. (2006). Chronic Patient’s Manage-
ment: The COPD example. In M-Health – Emerging
Mobile Health Systems, pages 575–585. Springer.
Eurostat (2002). Health statistics – Atlas on mortality in the
European Union. European Commission.
Fischer, H.-R., Reichlin, S., Gutzwiller, J.-P., Dyson, A.,
and Beglinger, C. (2006). Telemedicine as a new pos-
sibility to improve health care delivery. In M-Health
– Emerging Mobile Health Systems, pages 203–218.
Springer.
Guidant (2007). Heart Disease and Cardiovascular Disease
Therapies. http://www.guidant.com. accessed on 5th
June 2007.
Haas, P. (2006). eHealth ver¨andert das Gesundheitswesen
– Grundlagen, Anwendungen, Konsequenzen. HMD
Praxis der Wirtschaftsinformatik, 251:6–19.
Hadjileontiadis, L. J. (2006). Biosignals and Compression
Standards. In M-Health – Emerging Mobile Health
Systems, pages 277–292. Springer.
Istepanian, R. S., Laxminarayan, S., and Pattichis, C. S.
(2006). Ubiquitous m-health systems and the con-
vergence towards 4G mobile technologies. In M-
Health – Emerging Mobile Health Systems, pages 3–
14. Springer.
Junker, C. (2007). Todesursachenstatistik – Ursachen der
Sterblichkeit 2003 und 2004. Bundesamt f¨ur Statistik.
Know Heart Diseases (2007). Know Heart Diseases.
http://www.know-heart-diseases.com. accessed on 5th
June 2007.
Komninos, A. and Stamou, S. (2006). HealthPal: An Intel-
ligent Personal Medical Assistant for Supporting the
Self-Monitoring of Healthcare in the Ageing Society.
In Proceedings of UbiHealth 2006.
Led, S., Fernandez, J., and Serrano, L. (2004). Design of a
Wearable Device for ECG Continuous Monitoring Us-
ing Wireless Technology. In Proceedings of the IEEE
EMBS, pages 3318–3321.
Leimeister, J. M., Krcmar, H., Horsch, A., and Kuhn, K.
(2005). Mobile IT-Systeme im Gesundheitswesen,
mobile Systeme f¨ur Patienten. HMD – Praxis der
Wirtschaftsinformatik, 244:74–85.
Liszka, K. J., Mackin, M. A., Lichter, M. J., York, D., Pillai,
D., and Rosenbaum, D. S. (2004). Keeping a Beat on
the Heart. IEEE Pervasive Computing, 3(4):42–49.
Nollo, G., Nones, M., Malossi, C., Conforti, F., and Bato-
cletti, B. (2000). Standard communication protocol
for ECG exchange in tele-cardiology network for ru-
ral areas: three years project experience. Computers
in Cardiology, 27:663–666.
Savini, M., Stormer, H., and Meier, A. (2007). Integrat-
ing Context Information in a Mobile Environment us-
ing the eSana Framework. In Proceedings of the
ECEH’07, pages 131–142.
