
THE STRUCTURED STORAGE OF ONCOLOGICAL
CHEMOTERAPEUTIC REGIMENS
Contribution to Standardization of Therapeutic Procedures in Current Oncology
D. Klimes
1
, L. Dusek
1
, M. Kubasek
1
, J. Novotny
2
, J. Finek
3
and R. Vyzula
4
1
Institute of Biostatistics and Analyzes, Masaryk University, Kamenice 126/3, Brno, Czech Republik
2
Department of Oncology, General Teaching Hospital, Prague, Czech Republic
3
Charles University Prague, Medical Faculty Pilsen, Pilsen, Czech Republic
4
Masaryk Memorial Cancer Institute, Brno, Czech Republic
Keywords: Cancer Chemotherapy Protocols, Antineoplastic Combined Chemotherapy Regimens, XML, Clinical
Database.
Abstract: The aim of the chemotherapeutic regimens (CHR) digitalization project is the proposal of a universal
structure and creation of a publicly accessible database of contemporary CHR as a universal utility for the
communication and evaluation of contemporary and newly defined clinical schedules in anti-tumor
chemotherapy. After analysis of contemporary anti tumor CHR a standard XML structure was proposed,
which enables the recording of simple CHR from the field of chemotherapy in solid adult tumors, and also
has the potential of recording the complex treatment protocols in the field of paediatric oncology. The
resulting XML documents were saved on a web server. A publicly accessible CHR database was
constructed. There were a total of 130 XML documents with definitions of individual CHR in the first
phase. Linked to this data store, three examples of web applications were added to demonstrate the potential
uses of this newly created database.
1 INTRODUCTION
Chemotherapy, along with surgery and radiotherapy
is an irreplaceable part of the clinical treatment of
oncological illnesses across nearly all diagnoses. To
be more exact, we can define the term of
chemotherapy as encountered in this article. It is the
administration of individual preparations or
combinations of preparations from the anatomical-
therapeutic-chemical group (ATC) L01, which are
anti-tumor preparations. This ATC group currently
consists of nearly a hundred generic preparations,
which are divided into 5 basic groups: Alkylating
agents (L01A), Antimetabolites (L01B), Plant
alkaloids and other natural products (L01C),
Cytotoxic antibiotics and related substances (L01D)
and Other antineoplastic agents (L01X). Whether
these preparations are in practice applied either
separately in monotherapy or in combination, we
refer to them as a chemotherapeutic regimen (CHR).
The more complicated plans for the application of
cytostatics are classified in paediatric oncology as
treatment protocols. Standard CHR are based on
clinical studies and are published in the oncological
journals (Goldberg et al., 2004) (Henderson et al.,
2003) (Citron et al., 2003) and subsequently in
national or international guidelines (NCCN, 2006)
(CLS JEP, 2005).
However, CHR are not merely a list of applied
cytostatics in administered doses; the definition of a
CHR has its own basic rules, which are however not
strictly defined anywhere. The main features of
CHR include: doses of cytostatics are defined most
often according to the surface area of the patient's
body or their weight. CHR are applied in cycles, i.e.
defined time segments of the treatment are repeated
several times. There can be one or more repeated
segments. The days of application are identified
relative to the first day of each cycle (example Cycle
1- Day 1, Cycle 1- Day 8). These features are in
practice routinely used (see Figure 1).
148
Klimes D., Dusek L., Kubasek M., Novotny J., Finek J. and Vyzula R. (2008).
THE STRUCTURED STORAGE OF ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS - Contribution to Standardization of Therapeutic Procedures
in Current Oncology.
In Proceedings of the First International Conference on Health Informatics, pages 148-154
Copyright
c
SciTePress

FEC chemotherapy
Cyclophosphamide 75 mg/m PO days 1-14
Epirubicin 60 mg/m IV days 1 & 8
5-Fluorouracil 500 mg/m IV days 1 & 8
With cotrimoxazole support.
Cycled every 28 days for 6 cycles.
Figure 1: An example of CHR clinical definition (NCCN
Clinical Practice Guidelines in Oncology™ ©2006).
The aforementioned structure is frequently used,
however not standardized, as to prevent a wider use
of information technology. The vendors of a hospital
information system can create a special application
module for chemotherapy with a specific, internal
data structure or chemotherapy data is stored only as
a sequence of applications of cytostatics without
specific details. This situation hinders on the one
hand fast electronic transmission of new CHR and
the general intercommunication between computer
applications in this field, and on the other hand the
more advanced use of technology, for instance in the
field of the assessment and adherence to standard
CHR in clinical practice. A possible solution is the
creation of a structured data store of current CHR,
which will mirror current clinical guidelines and
which will be freely accessible to both clinics and
HIS providers. This article describes the proposed
structure of such a data store and the experience
gained during its construction. The practical usage
of such a database of CHR is demonstrated with the
example of a web portal, whose components are web
applications which use the CHR database as its
datasource.
2 METHODS
Preliminary analysis of problems showed that the
construction of a structured database of CHR calls
for certain steps:
1) The proposal of the structure of CHR
2) The unique identification of standard CHR
3) The digitalisation of current standard CHR
CHR can be considered as a type of structured
document, which is why the XML language was
chosen for its recording. Standard XML offers a
workable computational structure. In addition, it also
provides tools for the internal validation of
structures (XML schema) and tools for transforming
documents into different, more user-friendly
formats, for example HTML pages (XSLT). The
proposed XML structure of elements and attributes
was developed dynamically through the analysis of
clinical definitions of standard CHR for individual
oncological diagnoses. The source of the definitions
was the National and International oncological
guidelines (NCCN, 2006) (CLS JEP, 2005) and the
internal source of Masaryk memorial Cancer Institut,
a specialised hospital for the treatment of
oncological diseases in the Czech Republic. The
template for CHR was modelled using XML
schemes, which enabled the definition of individual
elements and attributes. The mandatory/optional
properties and frequency of repetition of elements
are defined by the maxOccurs and minOccurs
indicators.
2.1 Header of CHR
The created XML structure of CHR consists of two
parts. The first deals with the identification of CHR
and the possibility of its use in oncological diagnosis
(header). An example of this header is shown in
figure 2.
<name>AC(Fisher)</name>
<sysname>(1;60.0;mg/m2;iv)A+(1;600.0;mg/m2;i
v)C&21
</sysname>
<diagnosis>
<ICD10>C50</ICD10>
<line>1</line>
<purpose>adjuvant</purpose>
</diagnosis>
Figure 2: An example of CHR header definition.
The header contains the element name which
was used for the clinical identification of CHR. This
name was adopted either directly from clinical
guidelines or from clinical identification in the
information system of MMCI. These clinical names
do not guarantee uniqueness and do not adhere to
any strict rules. On the other hand the element
sysname was added to the individual definitions of
CHR on the basis of their internal structure. The
detailed principles of their creation are described
below.
The diagnosis element lists the individual
oncological diagnoses that each individual CHR can
treat. This is a complex element, which contains the
following nested elements. The code for diagnoses is
introduced according to the international
classification ICD-10 in same named nested
elements. The element line defines the CHR which
is suitable (or approved) for specific lines of
treatment.
THE STRUCTURED STORAGE OF ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS - Contribution to
Standardization of Therapeutic Procedures in Current Oncology
149

The element purpose specifies whether a CHR is
designed for adjuvant or palliative treatment. The
elements line and purpose can, within the one
element diagnosis, occur repeatedly in cases where
the CHR is intended for more lines or for both basic
purposes of treatment. In cases where the CHR is
used for more diagnoses, the whole complex
element Diagnosis is repeated.
2.2 Body of CHR
The second part of the structure describes the
administration of given CHR (body). A standard
CHR was divided into the following components
The name of administered cytostatics
Dosage of individual cytostatics
Units of doses
Method of administration
Day relative to cycle of administration
of cytostatic
Duration of one cycle in days
Total of completed cycles
Primarily proposed scheme for the body of the
CHR is presented in figure 3.
<group>
<id_group>1</id_group>
<interval>21</interval>
<noc>4</noc>
<drug>
.......
<drug>
<drug>
.......
<drug>
</group>
<group>
<id_group>2</id_group>
……….
</group>
Figure 3: The main frame of CHR body definition.
The element interval indicates the duration of
one cycle of chemotherapy in days. The length of
one cycle can be defined as the number of days
between day D1 on one cycle and D1 on the
following cycle. The actual length of the last cycle
can only be determined from the last defined day of
administration and cannot be compared with the
length of the preceding cycles.
The element noc (number of cycles) shows the
total of applied cycles. This parameter is limited by
clinical guidelines to a small number of CHR. These
guidelines often merely provide a recommendation
for the repetion of cycles. In practice the number of
applied cycles is decided by the actual state of health
of the patient. In cases where details were not
explicitly known, the value of this element was set
to 0.
The complex element drug describes the
application of individual cytostatics within the
framework of one cycle of chemotherapy. Since
many cytostatics are applied in CHR, the element
drug is referred to as a recurrent element. The
element drug encapsulates the nested elements for
labelling cytostatics, their dosage, day of
administration and method of administration. As
soon as we try to identify individually applied
cytostatics, the problem of their individual
classification arises. Existing practice is to cite the
full generic name of the cytostatic, which in certain
cases involves the brand name of the medication.
The ATC codes of identification of cytostatics are
not used in clinical practice, however they are ideal
for computer processing. We therefore decided to
include in the XML structure both an element for the
generic name of cytostatics (name) and an element
for the ATC code (ATC). The element name can be
inserted for each cytostatic repeatedly with the
attribute lang for various language versions of
classification. For the purpose of the systematic
naming of CHR (described below) the element abbr
was also defined for the abbreviated names of
cytostatics.
Doses of cytostatics, units of dosage of
cytostatics, method of administration and relative
day of administration were included within the
complex element administration, whose title was
shortened to adm for practical reasons. The element
dose was defined for the dosage of cytostatics as a
real number, for units of dosage the enumerative
element unit, for the method of administering the
enumerative element mode and for the day of
administering the whole number element unit,
respectively the two whole number elements
start_day and end_day.
In anti tumour chemotherapy, the dosage of
cytostatics is most commonly defined by the
calculation of the surface area of the patient or by
their weight. For this reason the element
unit was
defined with the values mg/m
2
and mg/kg.
Carboplatin has special dosage, where the dose is
defined in AUC. The resulting dose of this drug is
calculated depending on the laboratory value
parameters creatinine clearance (CrCl) according to
the formula:
HEALTHINF 2008 - International Conference on Health Informatics
150

dose(mg) = target AUC (mg/ml/min) * (CrCl +25)
(ml/min)
Two basic methods of administering cytostatics
(modes) are used, per oral and intravenous
administration. More detailed categorization can be
considered, for instance distinguishing between
intravenous administrations according to the length
of infusion. In the basic proposal there is the
difference between bolus administration and
infusion. For example in the case of the regimens
FOLFOX 4 and FOLFOX 6, which are used in the
treatment of colorectal carcinoma, it is necessary to
differentiate between the bolus dosage of
fluorouracil from its subsequent longterm infusion.
The element mode can thus include the values iv, iv-
bolus and po.
Day of administration is in clinical practice
presented as Dx, where x is the consecutive number
of days from the administration of the first
preparation in a cycle. Individual cytostatics can be
repeatedly administered within a cycle, either on
chosen days (e.g D1, D8) or daily in the course of an
appointed time period (e.g D1-D14). For the first
variant, the element day can be repeated within the
complex element adm, and in the second variant
there are, in place of the element day, two elements
start_day and end_day. An example of the complex
element drug is illustrated in figure 4.
<drug>
<name lang="cz">Cyklofosfamid
</name>
<name lang="eng">Cyclophosphamide
</name>
<atc>L01AA01</atc>
<abbr>C</abbr>
<adm>
<day>1</day>
<dose>600</dose>
<unit>mg/m2</unit>
<mode>iv</mode>
</adm>
</drug>
Figure 4: An example of the complex element drug.
For ‘multigroup’ regimens such AC+paclitaxel
(see figure 5) it was necessary to extend the
presented concept.
Doxorubicin 60 mg/m IV day 1
Cyclophosphamide 600 mg/m IV day 1
Cycled every 21 days for 4 cycles.
Followed by
Paclitaxel 175-225 mg/m by 3 h IV infusion
day 1
Cycled every 21 days for 4 cycles.
Figure 5: An example of multigroup CHR (NCCN Clinical
Practice Guidelines in Oncology™ ©2006).
For this type of CHR another encapsulating
structure was added to the XML scheme. This took
the form of the specific complex element group,
which contains all the defined elements of the body
of the CHR and can be repeated. For the
identification of groups, the element id_group was
added which contains the consecutive number of the
group. For multigroup CHR it is necessary that the
element noc must not be zero, at least for each group
except the last.
2.3 Systematic Naming of CHR
To prevent duplication in the database of CHR, a
concept was sought after, which would ensure the
individual identification of each of the stored CHR.
The identification of CHR used in clinical practice
seemed unsuitable, because as often happens, one
CHR has more than one name, or one name refers to
more than one CHR.
A unique standard naming of CHR was inspired
by Logical Observation Identifiers Names and
Codes (LOINC). LOINC is a structured
classification of laboratory methods (Huff et al.,
1998). There is a systematic name for each item (in
this example the laboratory method) consisting of
individual components which the method uniquely
refers to. In the case of LOINC, the names of
laboratory methods include the components,
property, timing, system precision and method.
Similarly, it is possible to create a unique
identification system of CHR. The following
requirements were necessary to be taken into
account within the proposals for the rules for the
systematic creation of naming of CHR:
The naming has to be unique
The naming must be automatically generated
from definitions of the CHR
All key components of the scheme must be
coded into the name
The name must remain "human readable"
The schematic name is created according to the
following syntactic rules:
THE STRUCTURED STORAGE OF ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS - Contribution to
Standardization of Therapeutic Procedures in Current Oncology
151
Administered drugs are classified with a unique
abbreviation
Drugs are alphabetically sequenced according to
abbreviations and are divided by the symbol
plus (+)
After the listing of the drug the duration of
cycle in days is added after the symbol(&)
For every drug, the following items are defined
in round brackets separated by a semicolon (;)
The first entry in the brackets is the day of
administration. It can be in the form of a number (1),
a list of numbers separated by commas (1, 8) or an
interval (1-14). The second entry is the dosage of the
medication. The third entry is the abbreviated name
for the method of administration. The fourth entry is
the unit of dosage.
Abbreviations used for cytostatic medications are
summarized in Table 1.
Abbreviations used are parts of the proposal for
the standardization of structures of CHR, because
currently the standard for the abbreviated
identification of cytostatics has not been found (on
the webpages of NCI (NCI Drug Dictionary
National Cancer Institute, 2005) only recommended
abbreviations can be found and all the well known
synonyms for given preparations). Clinically
established abbreviations are often diagnosis-
specific, for example cisplatin is listed under the
letter P in CHR such as BIP or BEP, in the regimen
M-VAC it is classified under the letter C, which is
however in the majority of cases used as the
abbreviation for cyclophosphamide. Due to the fact
that the number of well known cytostatics is very
similar to the number of existing chemical elements
for which two symbols are sufficient for the
abbreviated symbols, a similar concept was used for
the identification of cytostatics. The names of the
most frequently used cytostatics are written in the
table, each is recorded with a NCI abbreviation,
ATC code and proposed two letter identification,
which issues from the generic name of the cytostatic.
For multigroup CHR the concept was further
developed with square brackets enclosing individual
groups. The number of cycles is indicated before the
brackets separated by asterisks (*). Groups are
separated with the symbol +. An example of the
identification of the CHR AC+paclitaxel is
illustrated in figure 6.
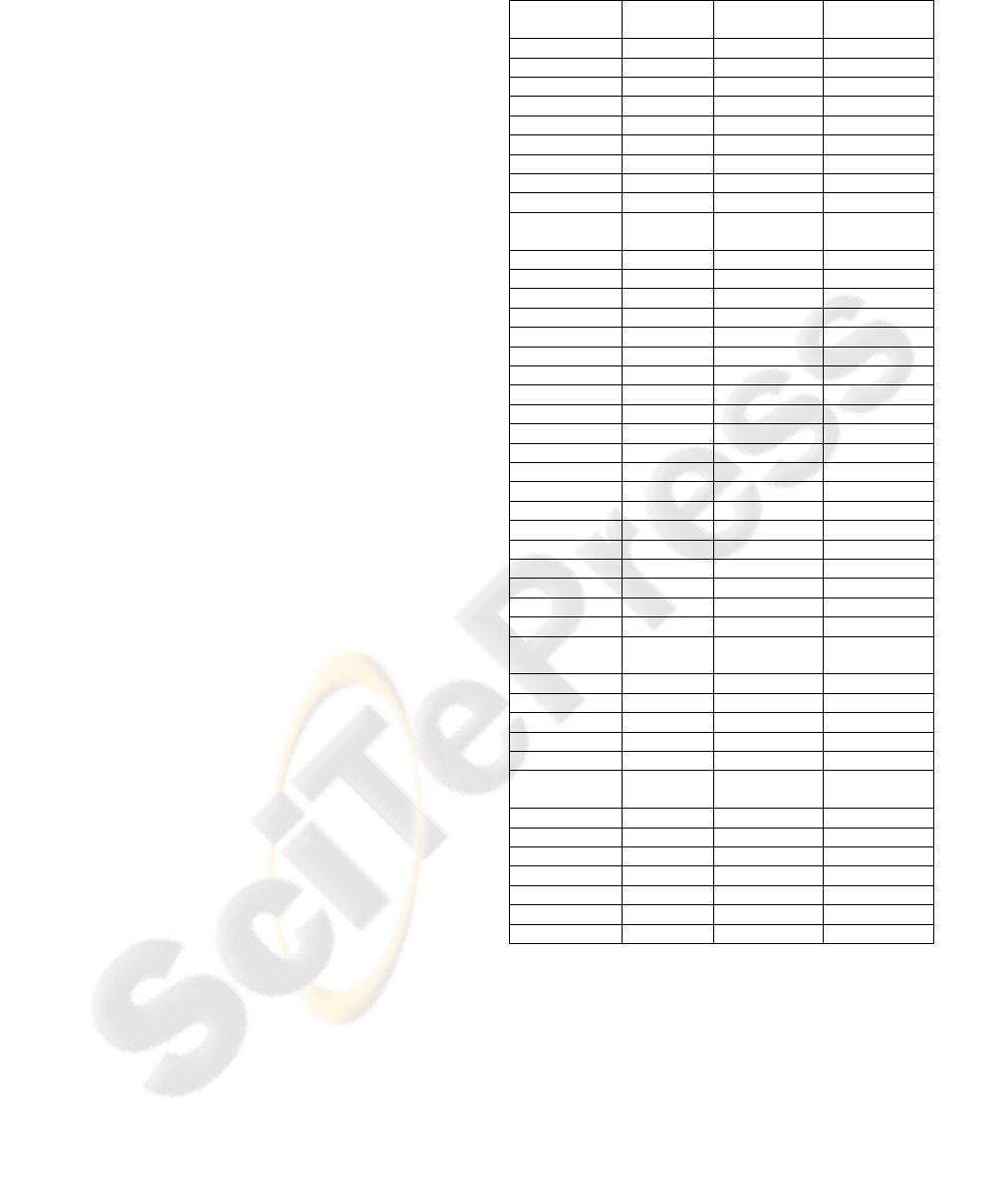
Table 1: Summary of most frequently used cytostatic
agents.
Cytostatic
agent
ATC - code NCI
abbreviation*
Used
abbreviation
bevacizumab L01XC07 ? Be
bleomycin L01DC01 BLEO B
busulfan L01AB01 BU, BUS Bu
capecitabine L01BC06 CAPE Ca
carboplatin L01XA02 CBDCA Cb
carmustine L01AD01 BCNU Bc
cetuximab L01XC06 MOAB C225 Ce
chlorambucil L01AA02 CHL, CLB Cl
cisplatin L01XA01 CDDP P
cyclophospham
ide
L01AA01 CTX C
cytarabine L01BC01 ARA-C Cy
dactinomycin L01DA01 DACT Ac
dacarbazine L01AX04 DTIC Dc
daunorubicin L01DB02 DNR Dn
docetaxel L01CD02 TXT Dt
doxorubicin L01DB01 DOX A
epirubicin L01DB03 EPI E
erlotinib L01XX34 OSI 774 Er
estramustine L01XX11 EM Em
etoposide L01CB01 VP-16 Et
fludarabine L01BB05 FAMP Fl
fluoruracil L01BC02 5-FU F
gefitinib L01XX31 ZD 1839 Ge
gemcitabin L01BC05 dFdC G
ifosfamide L01AA06 IFF, IFO If
irinotecan L01XX19 CPT-11 I
melphalan L01AA03 L-PAM Ml
methotrexate L01BA01 MTX M
mitomycin L01DC03 MITO Mi
mitoxantrone L01DB07 DHAD Mx
oxaliplatin L01XA03
1-OHP, L-
OHP
Oh
paclitaxel L01CD01 TAX Ta
pemetrexed L01BA04 LY231514 Pe
prednimustine L01AA08 ? Pr
procarbazine L01XB01 PCB Pc
raltitrexed L01BA03 ? Ra
rituximab L01XC02
MOAB IDEC-
C2B8 Ri
temozolomide L01AX03 TMZ Tm
thiotepa L01AC01 TSPA Ts
topotecan L01XX17 TOPO To
trastuzumab L01XC03 MOAB HER2 Tr
vinblastine L01CA01 VBL V
vincristine L01CA02 VCR Vc
vinorelbine L01CA04 VNB Vn
* NCI Drug Dictionary (NCI Drug Dictionary National
Cancer Institute, 2005)
4*[(1;60.0;mg/m2;iv)A+(1;600.0;mg/m2;iv)C&21]+
4*[(1;175.0;mg/m2;iv)Pt&;21]
Figure 6: An example of the identification of the CHR
AC+ paclitaxel
This identification of CHR is stored in a XML
file in the element sysname. The element sysname
acts as a unique identifier, a type of "fingerprint" of
HEALTHINF 2008 - International Conference on Health Informatics
152

the CHR and its primary function is to prevent
duplication in the data system.
3 RESULTS
A total of 160 CHR were entered into the database.
The definitions were formed according to the Czech
national guidelines for the cytostatic treatment of
solid tumors (CLS JEP, 2005). The validity of
entries according to International standards was
verified with reference to the International
guidelines NCCN (NCCN, 2006).
3.1 CHR Library Applications
As a demonstration of the use of structured records
of definitions of CHR a publicly accessible web
application was developed with three basic
functions: The Central Library of Chemotherapeutic
Regimens, Dose Intensity (DI) Calculator and
Therapy Organiser.
3.1.1 Search Engine
The Central Library is a simple search engine, that,
according to user entered criteria, searches and
displays the definition of the corresponding regimen.
Registered users have the possibility to add textual
commentaries to each CHR with supplementary
information, while for non registered users all
information is presented in a read only format.
3.1.2 Dose-Intensity Calculator
The DI Calculator enables users to calculate the
dose-intensity for selected CHR according to the
methods in (Hryniuk et al., 1984), and to compare
this with the actual intensities of cytostatics
administered to the patient in question.
3.1.3 Therapy Organizer
The Therapy Organizer enables users to devise time
plans for the administration of chosen CHR. It is
possible to display and print this plan in the form of
a calendar with suggested days and dosages for
individual cytostatics. The functions mentioned are
interconnected, for example, search results from the
Central Library of CHR can be directly used to
create a time plan in Therapy Organizer.
The applications are accessible at the internet
address
http://dios.registry.cz/?sec=software&lang=en
3.2 CHR Derivation
Thanks to a structured CHR library it is possible to
derive standard regimen only from a list of
applicated drugs and dates of administration. This is
useful when dose-intensity is evaluated and
available data doesn’t contain name of standard
regimen. During pilot tests there was success in
correctly deriving 98% of initial CHR from 180
patients who had been administered chemotherapy
for breast carcinoma.
4 CONCLUSIONS
CHR and their administration are routine practice in
contemporary oncology. The development of a
structured, electronic database of standard CHR can
help the faster propagation of information about new
CHR and at the same time enable assessment of their
adherence in clinical practice. The database is
created from XML documents, where every file
represents one CHR.
Unlike other printed or electronic sources about
CHR, this database contains only clear, structured
records of regimes. These records are inserted in
cooperation with expert oncologists. The result is a
new, always up-to-date information source that
forms the base for Dose Intensity Analysis and also
can be used in other computer applications in anti-
tumour therapy area.
ACKNOWLEDGEMENTS
Project DIOS, which addresses problems in anti
tumour chemotherapy, is supported by the grant
2608 from Ministry of Education of the Czech
Republic and by the Amgen Inc.
REFERENCES
Goldberg, R. M., D. J. Sargent, R. F. Morton, C. S. Fuchs,
R. K. Ramanathan, S. K. Williamson, B. P. Findlay,
H. C. Pitot, S. R. Alberts, 2004. A Randomized
controlled trial of fluorouracil plus leucovorin,
irinotecan, and oxaliplatin combinations in patients
with previously untreated metastatic colorectal cancer,
Journal of Clinical Oncology 22, no. 1: 23-30.
Henderson, I. C., D. A. Berry, G. D. Demetri, C. T.
Cirrincione, L. J. Goldstein, S. Martino, J. N. Ingle, M.
R. Cooper, D. F. Hayes, K. H. Tkaczuk, G. Fleming, J.
F. Holland, D. B. Duggan, J. T. Carpenter, E. Frei, R.
THE STRUCTURED STORAGE OF ONCOLOGICAL CHEMOTERAPEUTIC REGIMENS - Contribution to
Standardization of Therapeutic Procedures in Current Oncology
153

L. Schilsky, W. C. Wood, H. B. Muss, L. Norton,
2003. Improved outcomes from adding sequential
paclitaxel but not from escalating doxorubicin dose in
an adjuvant chemotherapy regimen for patients with
node-positive primary breast cancer, Journal of
Clinical Oncology 21, no. 6 (2003): 976-83.
Citron, M. L., D. A. Berry, C. Cirrincione, C. Hudis, E. P.
Winer, W. J. Gradishar, N. E. Davidson, S. Martino,
R. Livingston, J. N. Ingle, E. A. Perez, J. Carpenter, D.
Hurd, J. F. Holland, B. L. Smith, C. I. Sartor, E. H.
Leung, J. Abrams, R. L. Schilsky, H. B. Muss, L.
Norton, 2003. Randomized trial of dose-dense versus
conventionally scheduled and sequential versus
concurrent combination chemotherapy as
postoperative adjuvant treatment of node-positive
primary breast cancer: First report of intergroup trial
C9741/cancer and leukemia group B trial 9741,
Journal of Clinical Oncology 21, no. 8,p. 1431-39.
NCCN Clinical Practice Guidelines in Oncology™
NCCN, (accessed 1.10.2006). Available from
http://www.nccn.org/professionals/physician_gls/f_gui
delines.asp.
Zasady cytostaticke lecby malignich onkologickych
onemocneni: Ceska onkologicka spolecnost CLS JEP,
2005.
Huff, S. M., R. A. Rocha, C. J. McDonald, G. J. De Moor,
T. Fiers, W. D. Bidgood, Jr., A. W. Forrey, W. G.
Francis, W. R. Tracy, D. Leavelle, F. Stalling, B.
Griffin, P. Maloney, D. Leland, L. Charles, K.
Hutchins, J. Baenziger, 1998. Development of the
Logical Observation Identifier Names and Codes
(LOINC) vocabulary, Journal of the American
Medical Informatics Association 5, no. 3, p. 276-92.
NCI Drug Dictionary National Cancer Institute, 2005
(accessed 12.9. 2005). Available from
http://www.cancer.gov/drugdictionary/.
Hryniuk, W., H. Bush, 1984. The Importance of Dose
Intensity in Chemotherapy of Metastatic Breast-
Cancer, Journal of Clinical Oncology 2, no. 11, p.
1281-88.
HEALTHINF 2008 - International Conference on Health Informatics
154
