
ON DESIGNING AN EHCR REPOSITORY
Petr Aubrecht, Kamil Matoušek and Lenka Lhotská
The Gerstner Lab, Czech Technical University in Prague, Technická 2, 166 27 Praha 6, Czech Republic
Keywords: EHCR, databases, multiagent systems.
Abstract: In an ongoing project, a pilot study and implementation of repository design for electronic home care
records (EHCR) is described. Electronic home care record is based on the idea of electronic health record,
however it also satisfies additional information and functionality requirements specific for home care. The
design is based on the home care data and service model (K4Care model). First we analyzed the problem
and decided about the platform, storage technology, cooperation with other parts of the system being
developed, and basic structure of the EHCR. Then we focused on the design of data storage and
transformation of the K4Care model into a database structure. Finally cooperation between the database and
multiagent system is proposed.
1 INTRODUCTION
An electronic health record (EHR) is a distributed
personal health record in digital format. The EHR
should provide secure, real-time, patient-centric
information to aid clinical decision-making by
providing access to a patient's health information at
the point of care. An EHR is typically accessed on
a computer or over a network. An EHR almost
always includes information relating to the current
and historical health, medical conditions and
medical tests of its subject, thus representing
a longitudinal collection of information for and
about patients. In addition, EHR should contain data
about medical referrals, medical treatments,
medications and their application, demographic
information and other non-clinical administrative
information.
Although there are few standards for modern day
electronic records systems as a whole, there are
many standards relating to specific aspects of EHRs.
These include:
ASTM Continuity of Care Record (CCR) is
a patient health summary standard based upon
Extensible Markup Language (XML); the CCR can
be created, read and interpreted by various EHR or
Electronic Medical Record (EMR) systems,
allowing easy interoperability between otherwise
disparate entities.
American National Standards Institute (ANSI)
X12 (EDI) is a set of transaction protocols used for
transmitting virtually any aspect of patient data. It
has become popular in the United States for
transmitting billing information, because several of
the transactions became required by the Health
Insurance Portability and Accountability Act
(HIPAA) for transmitting data to Medicare.
CEN, the European Committee for
Standardization, was founded in 1961 by the
national standards bodies in the European Economic
Community and EFTA countries. Now CEN is
contributing to the objectives of the European Union
and European Economic Area with voluntary
technical standards which promote free trade, the
safety of workers and consumers, interoperability of
networks, environmental protection, exploitation of
research and development programs, and public
procurement. CEN - CONTSYS (EN 13940) is
a system of concepts to support continuity of care.
CEN - EHRcom (EN 13606) is the European
standard for the communication of information from
EHR systems. CEN - HISA (EN 12967) is a services
standard for inter-system communication in
a clinical information environment.
DICOM is a heavily used standard for
representing and communicating radiology images
and reporting
Health Level Seven (HL7) is one of several
ANSI-accredited standards developing organizations
operating in the healthcare arena. HL7 messages are
used for interchange between hospital and physician
record systems and between EMR systems and
practice management systems; HL7 Clinical
280
Aubrecht P., Matou
ˇ
sek K. and Lhotsk
´
a L. (2008).
ON DESIGNING AN EHCR REPOSITORY.
In Proceedings of the First International Conference on Health Informatics, pages 280-285
Copyright
c
SciTePress

Document Architecture (CDA) documents are used
to communicate documents such as physician notes
and other material.
Integrating the Healthcare Enterprise (IHE),
while not a standard itself, is a consortial effort to
integrate existing standards into a comprehensive
best-practice solution
ISO TC 215 has defined the EHR, and also
produced a technical specification ISO 18308
describing the requirements for EHR Architectures.
OpenEHR represents a next generation public
specifications and implementations for EHR systems
and communication, based on a complete separation
of software and clinical models.
Various factors involving the timing, the right
players, market history, utility, governance play
a key role in the overall enrichment of the standard
and certification development. The standardization
and certification even though seem to bring
uniformity in the EMR development; they do not
guarantee their acceptability and sustainability in the
long run.
The core of any EHR system is a data repository
that is usually realized by a database system. Types
of databases include the following ones
(Bontempo & Saracco, 1995): hierarchical, network,
relational, and object oriented. The hierarchical and
network databases represent older forms that are not
used in newer applications. Relational database
departs significantly from those two types and is the
most common form of database today. Relational
databases are constructed using tables instead of tree
and network structures. The tables do not specify
how to retrieve the required data or navigate through
predefined path. Object oriented database is the most
recent approach to database management. The object
oriented database structure is derived from object
oriented programming and has no single inherent
database structure. The structure for any given class
or type of object can be anything a programmer
finds useful. Furthermore, an object may contain
different degrees of complexity, making use of
multiple types and multiple structures.
In the next sections we will describe individual
issues related to EHCR design in more details,
namely persistence and structure of EHCR.
2 SCHEMA OF PERSISTENCE
In programming, persistence refers specifically to
the ability to retain data structures between program
executions, such as, for example, an image editing
program saving complex selections or a word
processor saving undo history.
This is achieved in practice by storing the data in
non-volatile storage such as a file system or
a relational database or an object database. Design
patterns solving this problem are container based
persistence, component based persistence and the
Data Access Object model. When first introduced,
the idea was that persistence should be an intrinsic
property of the data, in contrast with the traditional
approach where data is read and written to disk
using imperative verbs in a programming language.
This emphasis has largely disappeared, resulting in
the use of persist as a transitive verb: On
completion, the program persists the data.
2.1 Storage Technology
For persistence, there were two ways in our case:
Relational database;
XML storage.
Relational databases have long history and today
are able to store data reliably and efficiently. There
exist a big number of available databases both
commercial and free.
XML databases are relatively new technology
with promising future, allowing natural storage of
data with complex structure (e.g. annotated texts).
On the other hand, there is no emphasis on
reliability. Also effectiveness of query execution
(using XPath) is usually low.
Because the content of the database is critically
important, we emphasize robustness of the storage.
Another important point is amount of data to be
stored, thus the ability of the technology to manage
huge dataset is crucial. Therefore the chosen
technology is relational database.
This requirement also affected the further
decision about which database to use. We analyzed
advantages and disadvantages of several potential
databases. The database we typically use for storage
of a big amount of data is PostgreSQL. It provides
a rich query language with strong emphasize of the
Structured Query Language (SQL) standard. It is
proven to be reliable and has a great support for
transactions. Its BSD licence is the most free and
open. From the administrative point of view,
PostgreSQL allows use of several languages for
stored procedures including Java, which can be used
for simplification of some tasks. For this database
there exists a convenient graphical interface. The
performance of PostgreSQL is more than sufficient.
ON DESIGNING AN EHCR REPOSITORY
281

Another database server is represented by Mysql.
It is known to be very fast for read-only databases.
Unfortunately, it has significant drawbacks – limited
SQL and transactions supported only in one backend
with a loss of performance. Practical experience
shows many issues e.g. saving invalid dates,
accepting syntax errors, or even unpredictable
errors. Its license is not so free, the resulting product
must either be of GNU General Public License
(GPL) or Mysql must be bought.
There are other databases, which could be used.
For example, Firebird, which is free, but with many
specifics. Microsoft SQL Server faced several
security issues in past and requires a specific
operating system.
Big players in the field – Oracle and DB/2 are
extremely expensive for our purpose. Although
Oracle provides a free version, it is limited in
database size.
Based on the analysis we decided to use
PostgreSQL. In case of remote database access, we
are going to establish a Secure Sockets Layer (SSL)
connection to the database to protect the transferred
data.
2.2 Overall Schema of Persistence
When we started the project, one of the key
questions was the format of messages in the system.
The formats discussed were the medical standards
HL/7 and ENV 13606 standards. We all decided to
implement these standards consistently with their
purpose – only for data interchange between this
system and external institutions. In detail, this
communication will be operated by specialised
translation software agents (Hyacinth, 1996). We
suggest that import will be manual in this project,
because of the small amount of medical data to
import and because the implementation is too
complex.
Figure 1: Schema of communication.
The format of messages within the multiagent
system – MAS (Wooldridge, 2002) will depend on
the concrete content of documents described in the
K4Care model (Campana, 2006). The overall
schema is in the Figure 1.
3 DATABASE STRUCTURE
3.1 Document Storage
For document storage there were two approaches
available:
Data oriented with all data precisely defined
and stored in multiple tables;
Document oriented with documents seen as an
atomic structure with no intervention with its
internal structure.
The decision is quite simple – the design of the
required documents is an incremental process,
documents are analyzed and their detailed structure
is prepared. Moreover, we expect in the future more
document types, which will lead to modification of
the structure. In the first case it requires changes in
the database structure and also in the API between
agents and data storage.
The decision is then to store particular
documents as XML documents without knowledge
(from the storage/database point of view) of its
internal structure. Together with documents their
schema will be stored – at the moment of document
storage, the schema must be known.
There is one key requirement on the document
schemas – to contain a text part for agents, which
will not understand the particular type, to be able to
display at least some information to the human
client.
3.2 Structure of EHCR
The schema evolved originally from the
fundamental report of the project (Campana, 2006),
describing the problem domain. We identified data,
which are required to be stored and then we
suggested a structure holding all the data. Later,
a part of the schema, e.g. rights of particular users to
some actions/documents, formed the ontology layer.
A part of the schema is shared with the ontology
layer. Figure 2 shows the schema of the storage.
The objects on the storage side are divided into
three groups:
The first group forms EHCR, e.g. description of
a patient and all his/her medical documentation. In
HEALTHINF 2008 - International Conference on Health Informatics
282
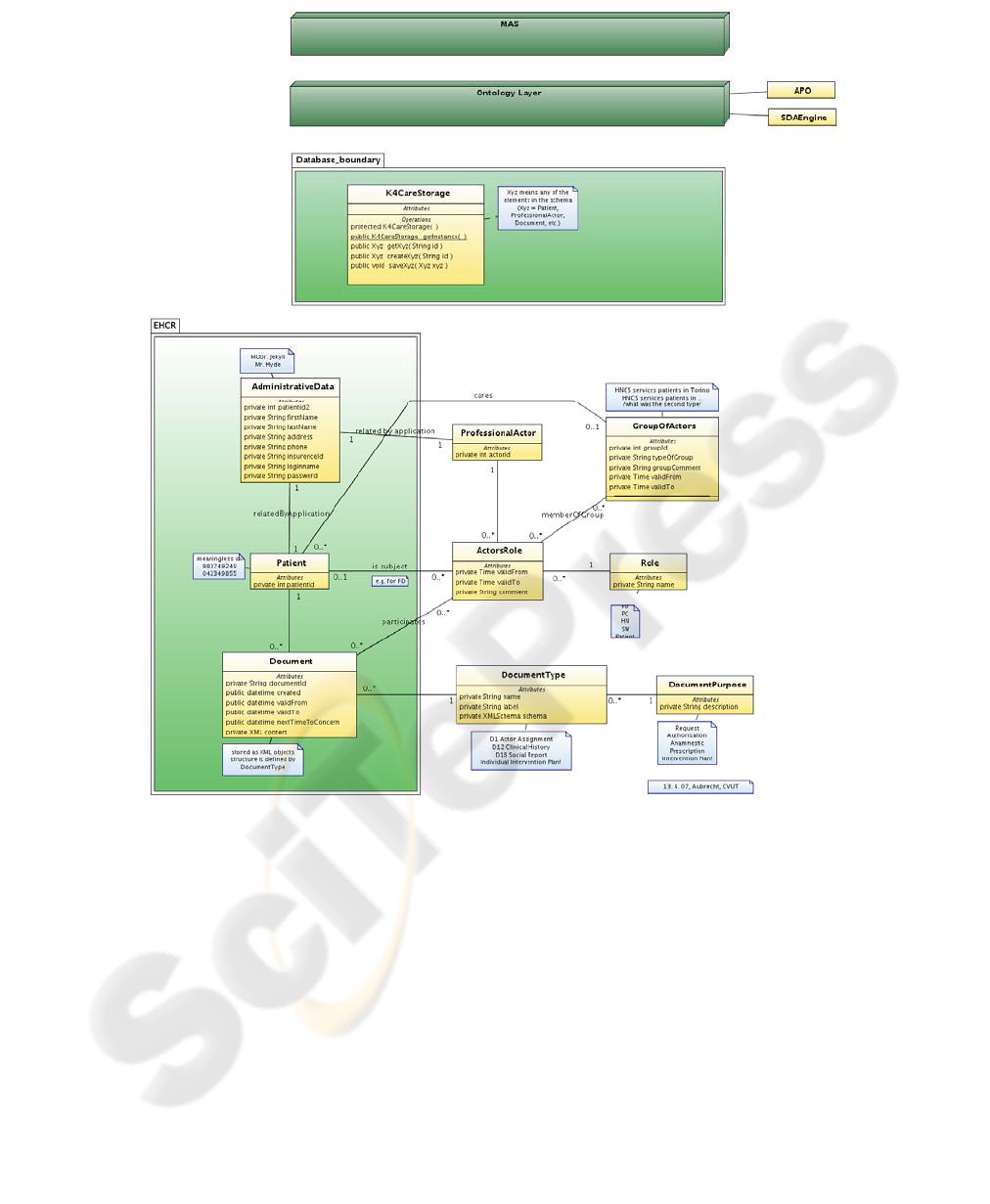
Figure 2: K4Care Model.
the schema this part is grouped into light green area.
It consists of administrative data and documents.
One of the requirements within the project was to
separate these two kinds of information, so the
relation between them is not presented in the
database, but implemented in Java program by
a kind of a cryptic function. These two parts can be
also physically separated (in two databases, possibly
on two computers) and joined by the program.
Documents are stored as XML-structured texts.
The second group of objects, ProfessionalActor,
ActorsRole, and GroupOfActors, describes the
structures used in the system. Information about
professionals is stored in a similar way to the
patients – separately from the administrative data.
An important part of these objects is dedicated to
groups of the professionals and which patients are
served by these groups.
The third group of objects, DocumentType,
DocumentPurpose, and Role, is a part of schema
shared with ontology layer. Information about
document types and purposes and about roles of
professionals must be stored in both storage (e.g.
because it is required to find professionals or
documents with a professional in some particular
role) and ontology (these information is a part of
descriptions of rules performed by the ontology
layer).
ON DESIGNING AN EHCR REPOSITORY
283

Documents represent an important part of the
whole schema. They are stored in XML format due
to the structured content, which can be changed in
the future. The corresponding XML schema is stored
in the DocumentType, so during each save operation,
the structure of the XML document can be verified.
As a result, the data store does not “understand” the
content of the XML documents. Their processing is
done by the higher levels of the system. Only a few
common attributes are stored explicitly as specific
attributes. These attributes are used in document
search.
Each document is assigned an attribute
NextTimeToConcern, which allows launching some
actions in the future, like appointments after some
period, regular vaccination, etc.
Besides the document data, the EHCR have to
store the following, so called intervention plans:
Formal Intervention Plan (FIP). It is not going
to change for a long time and belongs to
a group of diseases, syndromes or symptoms
(from ontology layer). FIPs will not be stored
in the repository, as they are not connected to
any patient. The stored FIPs may be
associated to diseases, syndromes and even
symptoms, described by codes proposed by
medical partners using the International
Classification of Diseases version 10. These
codes should be used in the formal/individual
intervention plan descriptions.
Individual Intervention Plan (IIP) belongs to
a single particular treatment of a patient. This
kind of intervention plan is valid only for the
time of the treatment. It is created on demand
and based on a FIP. It will be attached to the
EHCR of the patient.
The IIPs will be stored as documents, similarly
to any other medical information. The plans
including FIPs and IIPs will be expressed using
SDA* model (Riaño, 2007). An interpreter and
a graphical interface for creating and modifying the
plans are under development.
Steps written using the SDA* model will be
performed by software agents in the MAS part of the
system.
3.3 Multiagent System and Database
Cooperation
Cooperation between multiagent system and storage
is schematically shown in figure 2. First, between
these two parts is an ontology layer, responsible for
checking rights and providing semantic services to
the MAS.
In the upper part, there is the interface of the
storage to the outside components (client side). It
can be either ontology layer, as designed in the
K4Care project, or directly the multiagent system.
The opposite side uses K4CareStorage object as
an entry point to the storage and as a controller for
creation and modification of all of the available
objects. For each object it provides all of the four
operations: creation, retrieve, update, and remove.
Objects returned are connected together using
pointers to the related object, so the connection
using primary and foreign keys (used in the
database) is hidden to the client side and thus
convenient.
Both the developers of the agents and the
developers of the database may need to modify such
interfaces. These modified interfaces will be handled
carefully.
4 DOCUMENT SCHEMAS
Currently, XML schemas are being created to make
clearer the structure of the EHCR documents
planned to be used in K4Care. All the documents
defined in (Campana, 2006) can be incorporated in
EHCR as long as they belong to the patient.
The structure of the most relevant documents is
being discussed with the medical partners. Real
documents are examined and described in the form
of XML Schema. Together with documents are
stored intervention plans as a specific type of
document (in most cases with NextTimeToConcern
attribute set, when a next step of the plan should be
performed).
In the tables 1 and 2, there are shown for
illustration the most relevant service specific and
common documents to be implemented in the first
stage:
HEALTHINF 2008 - International Conference on Health Informatics
284
Table 1: Examples of the service specific documents for
the first stage.
Document name Abbreviation and type
MDE scales
D11 – anamnestic
multi-dimensional
evaluation
Set of forms filled in by the evaluation unit (EU) during
the first problem assessment and/or in occasion of the
periodical or end-treatment re-evaluation.
Clinical history
D12 – anamnestic
clinical assessment
All the available pertinent clinical information of the
patient (HCP) – previous test results, discharge sheets,
consultations, previous treatment. It is written by the
family doctor (FD) and the physician in charge of the
home care (PC); it is read by EU and the other
professionals in charge of the patient (according to their
competencies in the process of care of the individual
patient), by the patient him/herself.
Physical examination
report
D13 – anamnestic
physical examination
The report contains signs and symptoms of diseases
and/or conditions written by FD, PC, specialist
physician (SP); can be updated in any occasion of
evaluation. It is read by FD, PC, head nurse (HN); SP
and nurse (Nu) in charge of the patient.
Medical follow-up form
D19 – anamnestic
follow-up
It is written by FD or PC during the follow-up activities.
Nursing follow-up form
D20 – anamnestic
follow-up
It is written by Nu or HN during the follow-up
activities.
Table 2: Examples of the common documents for the first
stage.
Document name Abbreviation and type
Actor assignment
D01 – request
Is the information that links an individual action to
individual HCP for an action (or series of actions) to be
performed.
Actor confirmation
D02 – authorization
Is the information that declares that the actor knows the
assignment and accepts it.
5 CONCLUSIONS
The initial stage of the design and development of
EHCR data repository in the frame of the K4CARE
project has been described. Data storage was chosen
with respect to the nature of the data – absolute
requirement of secure and safe way of handling. For
this purpose there were used industrial standards for
storage: robust relational database engine with
transactions and SQL query language. In case the
application will access storage remotely, it can
provide SSL connection to the server.
The schema of data stored in the database
reflects the needs of medical specialists. Documents
themselves are stored in XML format in order to
allow further evolution of their structures. Other data
is stored in relational form to allow fast search and
concurrent access.
The overall schema is general enough to allow
cooperation with external partners using different
formats and efficient inner communication within
parts of the system.
ACKNOWLEDGEMENTS
The research has been supported by the EU FP6
project No. 026968 K4CARE “Knowledge-Based
HomeCare eServices for an Ageing Europe” and
partially by the GA CR project No. 201/05/0325
“New Methods and Tools for Knowledge Discovery
in Databases”.
REFERENCES
Bontempo, C. J., & Saracco, C. H. (1995). Database
Management Principles and Products, Upper Saddle
River, N.J.: Prentice-Hall PTR
Campana, F., et al. (2006). D01 – The K4CARE Model,
interim report.
Hyacinth, S. N. (1996). Software Agents: An Overview, In
Knowledge Engineering Review, 11(3):1–40,
September 1996, Cambridge University Press.
Riaño, D. (2007). The SDA* Model: A Set Theory
Approach. Machine Learning and Management of
Health-Care Procedural Knowledge. In CBMS 2007,
20th IEEE International Symposium on Computer-
Based Medical Systems. IEEE Computer Science
Press.
Wooldridge, M. (2002). An Introduction to MultiAgent
Systems, John Wiley & Sons Ltd.
ON DESIGNING AN EHCR REPOSITORY
285
