
Work partial granted by FCT (POCTI/0753/2004) through CINTESIS n
º
753/2004 FCT, by KCrypt (POSC/EIA/60819/2004) and LIACC through
the Programa de Financiamento Plurianual, FCT and Programa POS
I
.
A FIRST APPROACH FOR A REGIONAL WIDE VEPR
Pedro Vieira-Marques
Informatics Department, Faculty of Medicine,University of Porto
CINTESIS, Faculty of Medicine, University of Porto, Portugal
Arthur Cunha, Luís Antunes
LIACC, Faculty of Science, University of Porto, Portugal
Ricardo Cruz-Correia, Altamiro Costa-Pereira
Department of Biostatistics and Medical Informatics, Faculty of Medicine University of Porto
CINTESIS, Faculty of Medicine, University of Porto, Portugal
Keywords: Electronic Health Records; Agents and Cooperative Systems; Integration and Interoperability.
Abstract: Patients visit multiple health institutions and leave a trail of information scattered around hospitals,
healthcare centres and laboratories. Information availability is of major importance in healthcare delivery.
Most of the Electronic Patient Record systems are unarticulated and usually address only the specificities of
a single medical specialty. Virtual Electronic Patient Records such as MAID (Multi Agent system for the
Integration of Data) system provide for the necessary means for intra-institutions departmental information
integration. In this paper is presented a mobile agent based extension to the agent based MAID system in
order to enable inter-institution patient data integration. This system was designed as a MAID extension
with additional patient data integration features. In order to accomplish this, modules for external data
discovery and collection where developed using mobile agents. Data collection activities are trigged by
scheduled clinical events. The system is intended to enhance an existing institutional system taking it
beyond the institutional barrier providing health professionals with a more complete patient clinical history.
-
1 INTRODUCTION
Through the years Electronic Patient Record (EPR)
systems have been developed in order to provide
physicians with structured and helpful information.
However most of these systems are unarticulated
and usually address only the specificities of a single
medical specialty. Integration of healthcare
Information Systems (IS) is essential to support
shared care in hospitals, to provide proper care to
mobile individuals and to make regional healthcare
systems more efficient.
Healthcare is recognised as one of the most
important areas for applications and services
integration.
However, to integrate clinical IS in a way that
will improve communication and data use for
healthcare delivery, research and management, many
different issues must be addressed (Berg 2001;
Littlejohns, Wyatt et al. 2003). Consistently
combining data from heterogeneous sources takes a
great deal of effort because the individual feeder
systems usually differ in several aspects, such as
functionality, presentation, terminology, data
representation and semantics (Lenz and Kuhn 2002).
Successful integration seeks ubiquity – data
stored at one place should be available elsewhere;
consistency and integrity – different data items
stored within the system should not be contradictory
and integrity constraints should be maintained;
synchronization – in particular, concurrent data
access should not result in inconsistent data; single
system image – the user should be able to interact
with the system via a singe standard user interface;
and finally transparency – the user should not be
aware of heterogeneous system components.
215
Vieira-Marques P., Cunha A., Antunes L., Cruz-Correia R. and Costa-Pereira A. (2008).
A FIRST APPROACH FOR A REGIONAL WIDE VEPR.
In Proceedings of the First International Conference on Health Informatics, pages 215-218
Copyright
c
SciTePress

Multiagent systems can successfully solve
problems where the required knowledge is
physically distributed in several places (for example,
they can gather patient data from different medical
institutions or discover distributed e-health services)
(Moreno 2006). Previously, we have developed
MAID (Multiagent System for Integration of Data)
(Cruz-Correia, Vieira-Marques et al. 2005), an
agent-based system that provides access to patient
data that’s scattered between different units of major
Portuguese hospital. It has been running for two
years, having integrated (searched, verified,
collected and stored) over 2 millions clinical
records.
In (Vieira-Marques, Robles et al. 2006) we
proposed a model for a medical-information-
gathering system that addresses issues such as inter-
institutional patient health data integration, the
retrieval of momentarily unavailable online remote
data, and secure data access and transport. In this
model, clinical events scheduling trigger agents to
gather information for a particular patient clinical
history, making that history as complete as possible
when those events occur. Integration efforts are
directed at clinical documents and not at the data
themselves.
Figure 1: MAID Mobile model description.
In this paper, we describe a pilot implementation of
the model which is focused in gathering information
from multiple institutions, aiming at creating a first
approach to a national wide Virtual Electronic
Patient Record (VEPR).
2 METHODS
The system design was divided in three phases. To
each phase corresponds one functional moment of
the system (Fig. 1).
2.1 Events Management Phase
This is the first phase and corresponds to the
management and scheduling of new events like
consultations or surgeries. These events trigger
actions for information search and retrieval. The
Scheduler Agent (SA) manages the events and a set
of information search and retrieval Mobile Agents
(MA). To each patient a set of remote places where it
is known to exist clinical information is stored. This
list will grow has new places with information are
discovered.
2.2 Information Search Phase
The second phase consists on a search performed by
MA that will move between remote systems looking
for information (exams, lab reports, etc) of a
designated patient. If any documents are discovered
references are collected and stored.
Besides clinical information, MA will ask for
additional platforms where it is known for the
patient data to exist. If other platforms are provided
then they are added to the agent itinerary.
2.3 Document Retrieval Phase
At this stage, the process of searching for
information references has ended and the collected
references have been stored locally for retrieval.
This retrieval will make use of basic remote transfer
services using ftp or http urls or trough interfacing
web services. After collection actions all the
information is made available to the end user.
3 RESULTS
A set of agents was implemented using JADE
platform and are described in the following sections
along with their interactions while pursuing the
designated objectives for each stage.
3.1 Scheduler Agent
This agent (SA) is in charge of scheduled events and
MA management.
When some event is scheduled the SA constructs
two itineraries, one with the remote systems that are
known to have patient information and other with
the complementary MAID systems retrieved from a
directory services agent. These itineraries are
delivered to two independent MA. Upon MA’s return
this agent is notified that the process is finished and
HEALTHINF 2008 - International Conference on Health Informatics
216
the MA have returned with the collected information.
This agent will also receive a message from the
Local Broker Agent (LBA) informing about
referenced documents retrieval success in order to
eliminate the event from its list.
3.2 Mobile Agent
The MA actions are crucial to the purpose of this
system as they are the ones in charge of discovering
and carrying new information about a given patient.
These agents’ actions are implemented using a
Finite State Machine (FSM) which describes its roles
and roles transitions during the different stages of
moving, remote systems interaction, etc.
As soon as the agent receives the message from
the SA, it saves the necessary data (itinerary and
patient id) and moves to the first place. While in the
remote platform, messages are exchanged with the
remote broker agent (RBA). This message exchange
has the purpose of obtaining the new local interface
role, allowing the MA to retrieve the document
references. During the initial exchange of messages
a simple authentication is performed.
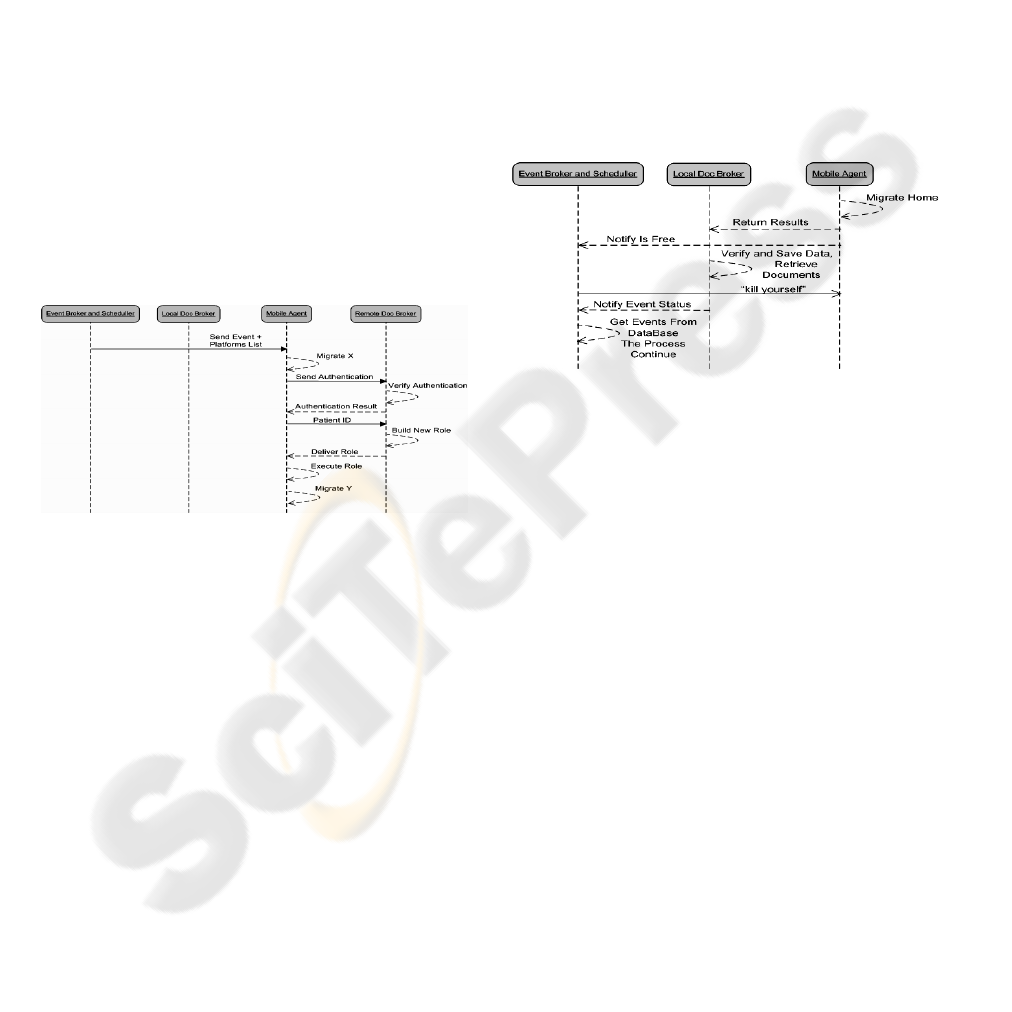
Figure 2: Agent interactions taking place during
Information Search Phase.
As soon as the MA receives the role, it adds it to
its FSM defining the necessary additional state
transitions. From this moment on the agent is ready
to get existing data through the execution of the new
role. The retrieved data include a document
reference list and a list of platforms that the visited
system knows to have documents related to the
patient the MA represents. By doing so, it will
discover new sources of information. When the MA
finishes its itinerary it will go back to the original
platform. Upon arrival he notifies the SA of its return
and delivers the gathered information to the LBA.
3.3 Remote Broker Agent
This agent stays in the local system and acts as an
interface agent to incoming agents. It has to be
implemented in accordance to each platform
specificity, as all remote system at this point are
MAID systems they are implemented the same way
in all nodes. It is in charge of authenticating and
providing the interface behavior to the incoming
agent.
3.4 Local Broker Agent
This agent is in charge of receiving the result of the
references retrieval process. After receiving new
references from the MA, it stores them into the
database and starts the document retrieval process
trough the external services provided by each
platform. After the documents being retrieved they
are made available to the end user (Doctor, Nurse,
etc) through existing user interfaces. The documents
are saved in the file system digitally signed,
guaranteeing the documents integrity.
Figure 3: Agent interactions taking place during
Document Retrieval Phase.
3.5 Agent Interactions
The UML activity diagrams describe the interactions
between the different agents during information
references search (Fig. 2) and document retrieval
(Fig. 3).
4 DISCUSSION
This prototype extends the MAID systems by
implementing a set of interfacing agents enabling the
retrieval of remote documents. It addresses a
scenario where multiple MAID systems coexist. We
feel that multi-agent technologies can help
implement integration between heterogeneous
healthcare Information Systems in a satisfactory
manner.
4.1 Integration Achieved
Regarding ubiquity, our implementation enables the
exchange of information between each integrated
system in a similar way. All information is
A FIRST APPROACH FOR A REGIONAL WIDE VEPR
217

equidistant to each system. To face the problem of
latency of communications, or even momentary lack
of connectivity between different institutions when
the healthcare professional needs the patient
information, the system tries to collect useful patient
data a prior, i.e., before the user request. Scheduled
appointments trigger data discovery and report
collection. Agents facilitate ubiquity as they allow
MAID to operate in an asynchronous faction, which
is more powerful than other technology solutions
like web services that rely on synchronous
communication.
Regarding synchronization, our proposal takes
two different approaches. When integrating patient
data in an institution, MAID collects all updated
reports from the departmental IS so that its local
repository stays updated. In this scenario on the
other hand, when integration occurs between
different MAID systems our method is more like
lazy synchronization, i.e., the information is
updated only when a healthcare professional access
to the system is scheduled. Although, this approach
may raise problems in unscheduled accesses, we feel
that full synchronization stresses network resources
too much.
Although single system image is usually
regarded as being a user interface issue, MAID
delivers the same functionality of single image not
to human users but to requesting systems that may
have user interfaces themselves.
Consistency and integrity were not a major
concern in this implementation. Nevertheless it
should be noticed that MAID has already some data
quality checking in place, namely to detect wrong
patient identifications (Cruz-Correia, Vieira-
Marques et al. 2006). For full consistency checking,
it is essential to have documents introspection which
stresses the use of informatics standards like XML
to describe documents, or even healthcare related
standards like HL7-CDA or OpenEHR.
Unfortunately, the Portuguese reality is still far from
having healthcare IS that give access to their data
through this standards.
Transparency is very difficult to obtain when
dealing with documents generated in heterogeneous
IS, because they lack normalization regarding
presentation. To achieve a high level of transparency
it is essential to use structured documents (e.g.
XML).
4.2 Implementation Issues
By providing interfacing behaviours to incoming
mobile agent there is no need for complex
interactions reducing interface agent congestion
which would arise from multiple agents requesting
database queries.
REFERENCES
Berg, M. (2001). "Implementing information systems in
health care organizations: myths and challenges." Int J
Med Inf 64(2-3): 143-156.
Cruz-Correia, R., P. Vieira-Marques, et al. (2005).
"Integration of hospital data using agent technologies -
a case study." AI Communications 18: 191-200.
Cruz-Correia, R., P. Vieira-Marques, et al. (2006).
"Monitoring the integration of hospital information
systems: how it may ensure and improve the quality of
data." Stud Health Technol Inform 121: 176-82.
Lenz, R. and K. A. Kuhn (2002). "Integration of
Heterogeneous and Autonomous Systems in
Hospitals." Business Briefing: Data management &
Storage Technology.
Littlejohns, P., J. C. Wyatt, et al. (2003). "Evaluating
computerised health information systems: hard lessons
still to be learnt." BMJ 326: 860-3.
Moreno, A. (2006). "On the evolution of applying agent
technology to healthcare." IEEE Intelligent Systems
21(6): 8-10.
Vieira-Marques, P., S. Robles, et al. (2006). "Secure
Integration of Distributed Medical Data using Mobile
Agents." IEEE Intelligent Systems Journal 21(6): 47-
54.
HEALTHINF 2008 - International Conference on Health Informatics
218
