
AUTHENTICATION OF PROFESSIONALS IN THE RTS E-HEALTH
SYSTEM
Andr´e Z´uquete
IEETA / Univ. of Aveiro, Campus Univ. de Santiago, 3810-193 Aveiro, Portugal
Helder Gomes
IEETA / ESTGA / Univ. of Aveiro, Campus Univ. de Santiago, 3810-193 Aveiro, Portugal
Jo˜ao Paulo Silva Cunha
IEETA / Univ. of Aveiro, Campus Univ. de Santiago, 3810-193 Aveiro, Portugal
Keywords:
e-Health, authentication, public key certificates, PKI, smartcards, SSL/TLS, roles, RBAC.
Abstract:
This paper describes the design and implementation of a PKI-based e-Health authentication architecture. This
architecture was developed to authenticate e-Health Professionals accessing RTS (Rede Telem´atica da Sa´ude),
a regional platform for sharing clinical data among a set of affiliated health institutions. The architecture had
to accommodate specific RTS requirements, namely the security of Professionals’ credentials, the mobility of
Professionals, and the scalability to accommodate new health institutions. The adopted solution uses short
lived certificates and cross-certification agreements between RTS and e-Health institutions for authenticating
Professionals accessing the RTS. These certificates carry as well the Professional’s role at their home institu-
tion for role-based authorization. Trust agreements between health institutions and RTS are necessary in order
to make the certificates recognized by the RTS. As a proof of concept, a prototype was implemented with
Windows technology. The presented authentication architecture is intended to be applied to other medical
telematic systems.
1 INTRODUCTION
RTS (Rede Telem´atica da Sa´ude (?; ?)) is a regional
health information network (RHIN) providing an ag-
gregated view of clinical records provided by a set of
affiliated health institutions (HIs). Each HI uses its
own system to produce and manage clinical records,
which can be browsed and presented in different ways
by RTS. The goal of RTS is not to replace the systems
used by the affiliated HIs, but to provide a mediated,
global viewof patient’sclinical records independently
of the HIs holding their records.
RTS provides Portals for accessing clinical
records. Two Portals were foreseen: the Patients Por-
tal and the Professionals Portal. The first is to be used
by Patients to communicate with their family doctor
and other health system issues such as renovation of
prescription and schedule appointments. The second
is to be used by healthcare Professionals for accessing
clinical records required for their normal, daily work.
The RTS Professionals’ Portal is a web server ac-
cessible through RIS (Rede Inform´atica da Sa´ude
1
), a
nation-wide, private network, interconnecting all HIs,
including the ones affiliated with RTS. Profession-
als access data provided by RTS using a normal web
browser running on a computer connected to the RIS.
This paper describes an authentication architec-
ture providing strong authentication for Professionals
accessing the Professionals’ Portal. Strong authen-
tication is provided by using a two-factor approach:
possession of a security token and knowledge of a se-
cret. For the security token we chose a smartcard.
Smart cards are tamperproof devices with security-
related computing capabilities which are very conve-
nient for running computations using private keys of
asymmetric key pairs.
This paper is organised as follows. Section 2
overviews the authentication architecture and some
RTS requirements. Section 3 presents some design
goals. Section ?? presents the proposed authentica-
1
Health Computer Network
72
Z
´
uquete A., Gomes H. and Paulo Silva Cunha J. (2008).
AUTHENTICATION OF PROFESSIONALS IN THE RTS E-HEALTH SYSTEM.
In Proceedings of the First International Conference on Health Informatics, pages 72-80
Copyright
c
SciTePress

tion architecture. Section ?? presents some related
work. Section ?? presents our prototype implemen-
tation. Section ?? evaluates the architecture and the
implementation. Section ?? concludes the paper.
2 OVERVIEW
This paper describes an authentication architecture
providing strong authentication for Professionals ac-
cessing the Professionals’ Portal. Strong authenti-
cation is highly recommended in this case, as Pro-
fessionals can access sensitive data — the patients’
health records. The architecture allows Professionals
to roam between computers of their HI or other HIs.
Our authentication architecture had also to deal
with authorization issues. In fact, the RTS Portal uses
a role-based access control (RBAC) policy for deriv-
ing the Professionals’ authorizations to access clinical
data. Therefore, each time a Professional accesses the
RTS Portal, the later must learn a role that the former
may legitimately play for deriving authorisations.
The proposed architecture uses public key cryp-
tography as the basis for its operation. Each Profes-
sional is given a smartcard for storing and using per-
sonal credentials for accessing the RTS Portal. The
Professionals’ authentication process uses a facility
provided by web browsers, the SSL/TLS client au-
thentication with asymmetric keys and X.509 public
key certificates (PKCs), to prove the authenticity of
the Professional to the RTS Portal (?; ?).
Furthermore, the PKCs used by Professionals in
the SSL authentication process provide extra informa-
tion to the RTS Portal, besides the identity of the Pro-
fessionals, such as the HIs they are affiliated to and
the role they are playing. As a Professional may play
several roles simultaneously (e.g. Doctor and Chief
Doctor), the PKC must contain all the roles we can
play, being up to the RTS Portal to chose the role to
play, from the possible ones, in each session.
Since a Professional’s PKC carries roles the owner
can play, a mechanism must be provided to deal with
role changes. A possibility was to use certification
revocation for outdating given roles. However, revo-
cation validation requires online communication be-
tween the PKC validator and the PKC issuer, which
may not be possible or convenient. Furthermore,
some roles are very short in time, for example, va-
cation substitutions, and these dynamics can be more
easily managed by short lived certificates than by Cer-
tificate Revocation Lists (CRL).
Alternatively, we chose to used short-term validity
periods for Professionals’ PKCs, as in (?). This way,
Professionals’ PKC get automatically invalid after a
short period of time after their issuing and Profession-
als must apply for new ones. A simple and secure en-
rolment process was also conceived for getting new
PKCs.
The public key infrastructure (PKI) for managing
Professionals’ credentials for accessing RTS uses a
flexible, scalable grassroot approach. Each HI and the
RTS have their own PKI, including root and issuing
certification authorities (CA). The issuing CA of each
HI is responsible for issuing RTS credentials for local
Professionals. The issuing CA of RTS is responsible
for issuing credentials for the RTS Portal. The valida-
tion of certificates issued by separate PKIs is enabled
by cross-certification agreements. This means that the
RTS Portal will only be able to validate Professionals’
credentials issued by HI CAs cross-certified by RTS;
other people, including Professionals from other HIs,
cannot be authenticated by the RTS Portal, therefore
cannot access protected clinical data.
In this paper we mainly describe our architecture
for using smartcards for authenticating Professionals
and the RTS Portal when interacting with each other
and for providing Professionals’ roles to RTS. How-
ever, the architecture was designed taking into consid-
eration future enhancements and synergies, such as:
• Enable Professionals to use the same smartcard
for producing signed data as input for health in-
formation systems.
• Enable Professionals to give signed consents re-
garding accesses to the clinical data.
• Adoption of a similar authentication model for
authenticating Patients, possibly using the new,
smartcard-enabled Citizens Card.
• Usage of PKIs deployed for managing smartcards
to generate credentials for mutual authentication
within secure communications between hosts or
servers used in the RTS and in HIs (e.g. with
IPSec or SSL/TLS (?; ?)).
• Usage of PKI deployed in each HI for managing
the local authentication of Professionals access-
ing local services (e.g. secure wireless network
access).
3 DESIGN GOALS
A set of design goals were defined at start. Those
goals derived both from RTS requirements and from
previous experiences with informatics services in
healthcare environments.
The first goal was Professionals’ mobility. The
authentication architecture should not restrict the mo-

bility of Professionals; at the end it could be possi-
ble to use any computer, belonging to the RIS, to ac-
cess RTS services. Naturally, this goal depends on
software and hardware installed in client computers
accessing Professionals’ authentication tokens. Nev-
ertheless, we tried to facilitate the widespread use of
those tokens by using common hardware (e.g. USB
ports) and free software packages (e.g. software pack-
ages already provided by operating system vendors).
The second goal was to be pragmatic regarding
the implementation of a PKI for managing asymmet-
ric keys and PKCs. Nation-wide PKIs do not exist
for this purpose. And, though they could be advanta-
geous, they are also difficult to deploy and to manage.
Thus, we chose to start from a sort of minimalist, ad-
hoc scenario, with no global PKI on top of the RTS
and all the HIs, but instead with isolated, standalone
PKIs on each entity, RTS and HI.
The third goal was RTS independency regarding
the management of personnel in affiliated HIs. Each
HI is an independent organization, with its own Pro-
fessionals, human resources management department
and some kind of directory service to store the Pro-
fessionals’ information. Independent of RTS, they
will continue to manage their Professionals because
of their own, internal systems. It thus makes sense
to reuse HI Professionals information and let each HI
to manage the access of its own Professionals to the
RTS. This way, we avoid replication of information
and a centralized enrolment of Professionals in RTS.
The fourth goal was to minimize communica-
tion overheads related to the authentication of Profes-
sionals and fetching/validation of role membership.
Namely, we tried not to use on RTS any online ser-
vices from HIs to deal with details regarding the iden-
tification, authentication and role membership of Pro-
fessionals. Since Professionals’ information is man-
aged solely by their home HI (our previous goal), this
means that Professionals’ identification and authenti-
cation credentials should convey RTS as much infor-
mation as possible, to avoid contacting online services
at Professionals’ home HIs.
The fifth and final goal was browser compatibility.
To avoid the requirement of using a specific browser,
no client-side active code (ActiveX and Java Applets)
is used in RTS. Therefore, we could not use any spe-
cial code for managing the authentication of Profes-
sionals using a browser to access RTS. In other words,
the authentication mechanism using a two factor ap-
proach should be already available within the basic
functionality of all browsers. As we will see, although
the basic functionality exists in all popular browsers
(support of SSL client-side authentication), the exact
mechanisms and policies used to handle such support
are different and raise some problems.
4 AUTHENTICATION
ARCHITECTURE
The authentication architecture is resumed in Fig-
ure ??. The Professional uses a web browser to access
the web server that implements the RTS Portal, and
uses an SSL secure channel for protecting the com-
munication from eavesdropping. Furthermore, mu-
tual authentication is required in the establishment of
the SSL secure session, thus the browser authenticates
the RTS Portal and the RTS Portal authenticates the
Professional using the browser. Similarly, the Profes-
sional uses a web browser a mutually authenticated
SSL session to access the HI Issuing CA web server
for requesting fresh RTS credentials.
4.1 The Professionals’ Smartcard
A Professional’s smartcard carries two types of asym-
metric key pair and corresponding PKCs. One type
we call RTS credentials, which are to be used to
authenticate himself when accessing the RTS Portal.
The other type we call HI credentials, which are to
be used to authenticate himself when accessing his HI
issuing CA for getting new RTS credentials.
Smartcards are initialised and provided by HIs to
their own Professionals. At start they only carry the
HI credentials. When required, the owner uses them
for requiring RTS credentials. These credentials can
then be used to access the RTS Portal.
RTS credentials are short lived, lasting for one or
a few days. The RTS Portal doesn’t use remote HI
services for checking for their validity. Instead, it as-
sumes that a Professional’s role revocation will natu-
rally be enforced by not being able to get a new RTS
credential including the revocated role. On the con-
trary, HI credentials are long lived, because they are
used for long periods of time for getting new RTS cre-
dentials.
4.2 Professional Authentication
The Professional authentication is requested by the
SSL server-side of web servers and conducted by the
SSL client-side running on browsers. The SSL client-
side authentication uses the Professional’s smartcard
for his authentication. The browser is configured to
use smartcard services and when client-side authen-
tication is required it will prompt the Professional
for the right credentials, including the ones inside the
smartcard, he intends to use. The Professional chose
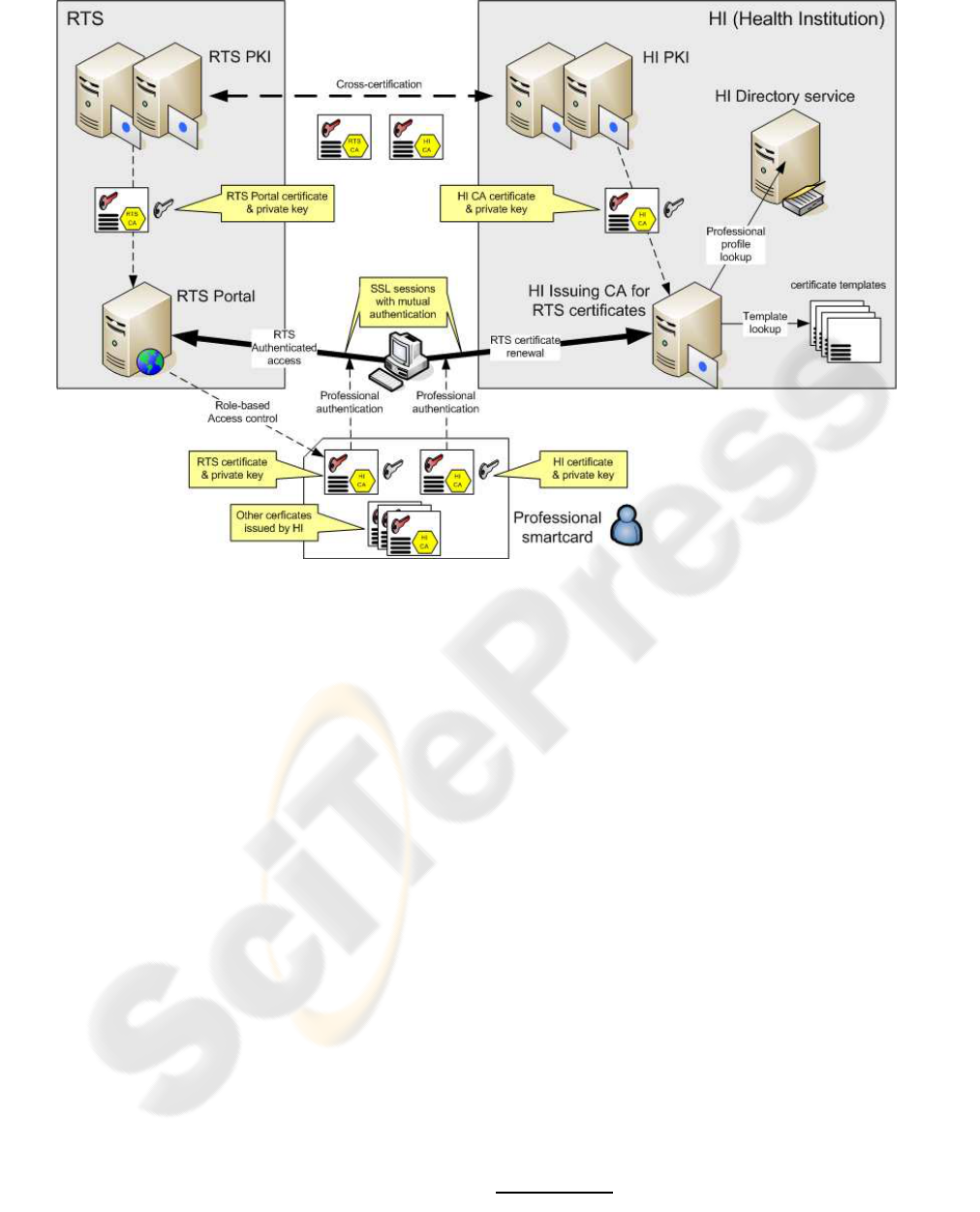
Figure 1: Overview of the authentication architecture for HI Professionals whiling to access the RTS Portal.
the right pair of asymmetric keys from the smartcard,
and the PKC of the public key, and the browser uses
them to provide client-side authentication.
This client-side approach is the same for access-
ing the RTS Portal or the HI Issuing CA. It is up to
the Professional to choose the right set of credentials,
from the smartcard, to get authenticated. And in all
cases it needs to introduce a PIN to unblock the smart
card for producing digital signatures required by the
SSL authentication protocol.
The web servers used by the RTS Portal and the
HI Issuing CA perform the following actions: (i) vali-
date the PKC chose and presented by the Professional,
(ii) use the certified public key to validate the SSL
secure channel establishment and (iii) enable the ser-
vice, RTS or CA, to access the Professional’s PKC.
The RTS learns from the PKC the Professional’s iden-
tity, his home HI and his roles; the CA learns only the
Professional’s identity.
4.3 Role Assignment and Selection
The roles of each Professional are embedded in the
PKC of his RTS credentials. These roles are stored
in extension fields, namely the Extended Key Usage
(EKU) field. Each role was given a numerical tag, an
ASN.1 Object IDentifier, reserved at IANA
2
for RTS.
Each time a Professional requests RTS creden-
tials, he gets, after proper authentication at the HI Is-
suing CA, a new PKC with the current roles he can
play. This PKC is communicated to the RTS web
server during SSL authentication and, if successful,
the PKC is made available for consulting by the RTS
Portal during the SSL session. This way, when a Pro-
fessional initiates an SSL-protected session with the
RTS Portal, it can easily learn the set of roles the Pro-
fessional can play and prompt the Professional for se-
lecting the right role for the current session.
4.4 Trust Relationships
Each entity, RTS and HI, uses an independent PKI for
managing RTS and HI authentication credentials used
by Professionals. The RTS is not meant to serve as a
CA for all HIs; it only deploys a PKI mainly for man-
aging its own certificates. HI certification hierarchies
may be isolated or integrated in wider hierarchies pro-
viding large-scale validation of certificates. For the
RTS that is irrelevant, all it requires is an Issuing CA
for issuing RTS credentials for local HI Professionals.
2
http://www.iana.org

Since RTS and HI certification hierarchies are iso-
lated from each other at the beginning, some mecha-
nism is required to enable the RTS Portal to validate
Professionals’ RTS credentials, issued by HIs. Sim-
ilarly, some mechanism is required to enable profes-
sionals to validate the credentials of the RTS Portal,
issued by RTS. This mechanism is cross-certification.
When an HI gets affiliated to the RTS, the RTS Issu-
ing CA issues a certificate for the public key of that
HI Issuing CA. With this certificate, the RTS is able
to validate all the PKCs of RTS credentials issued for
the Professionals of that HI. Similarly, the HI Issuing
CA issues a certificate for the RTS Issuing CA, en-
abling local Professionals to validate the credentials
of the RTS Portal.
4.5 Validation of Certificates
With this cross-certification in place, the validating
of certificates’ certification chains works as follows.
The RTS Portal trusts only on the (self-signed) certifi-
cate of the RTS Root CA. Similarly, the Professional
trusts only on the (self-signed) certificate of his HI
Root CA. Since certificate chain validations progress
recursively until finding an error or a trusted certifi-
cate, the validation chains are the following:
Validator
Professional RTS Portal
?
validation
sequence
RTS Portal
RTS Issuing CA
Professional
HI Issuing CA
ւ ւ
RTS Issuing CA
HI Issuing CA
HI Issuing CA
RTS Issuing CA
ւ ւ
HI Issuing CA
HI Root CA
RTS Issuing CA
RTS Root CA
ւ ւ
HI Root CA
HI Root CA
RTS Root CA
RTS Root CA
where
X
Y
represents the PKC of X issued by Y.
Besides cross-certification for certificate chain
validation, trust relationships between the RTS, HIs
and their Professionals must be complemented by
common certification procedures. Namely, all HIs af-
filiated to the RTS should follow similar procedures
for issuing RTS credentials. For instance, smartcards
with HI credentials should be initialised by HIs and
personally delivered to Professionals.
4.6 Validity of Authentication
Credentials
The authentication credentials stored inside a Profes-
sional’s smartcard are the HI credentials and the RTS
credentials. The first ones are used to establish an au-
thenticated session to get the second ones.
HI credentials are to be used frequently, for in-
stance, once per day or once for a couple of days, to
fetch new RTS credentials. Therefore, they should
have long validity periods and CRLs must be pub-
lished to prevent unwanted use of them after a given
instant. For instance, if a Professional moves from
one HI to another one, his smartcard from the former
HI must be returned and a CRL should be issued to
invalidate the public key of the HI credentials inside
the smartcard. Note, however, that CRL issuing and
validation are all executed within the same HI, and
not by external clients.
RTS credentials are valid only during short peri-
ods of time, one or two days. Therefore, no CRLs are
used to validate them, since the error window is too
narrow to allow a Professional to play a role he is no
longer allowed to. Consequently, by default the HI Is-
suing CA doesn’t publish CRLs for RTS certificates.
In special cases, such as disciplinary processes
and legal inquiries, it should be possible for the HIs to
provide to the RTS Portal, just in time, a list of RTS
certificates that should no longer be accepted while in
validity period. But since such cases should be rare, it
is preferable to deal them as the exception to the gen-
eral rule above stated: no CRLs exist and are checked
for RTS certificates.
All the certificates used in both HI and RTS cre-
dentials do not need to be published by Issuing CAs.
In fact, these certificates are used solely in the con-
text of SSL mutual authentication, and are communi-
cated to the interacting peers within the SSL protocol.
Therefore, they need not be published in some public
directory System, as other certificates do, because no
one needs them for other purposes.
5 RELATED WORK
The following e-Health Systems were analysed:
HYGEIAnet and MedCom/Sundhed.dk.
5.1 Hygeyanet
HYGEIAnet is the RHIN of Crete, Greece. It was de-
veloped by the Institute of Computer Science (ICS)
of Foundation for Research and Technology – Hel-

las (FORTH) to provide an integrated environmentfor
delivery of health care services in Crete Island (?; ?).
Similarly to RTS, HYGEIAnet is formed by sev-
eral HIs, namely Hospitals and Primary Care Units,
each with its own health data, information services
and human resources. HYGEIAnet operates above
these independent healthcare units, providing an in-
frastructure for sharing clinical information. Also, the
Integrated Electronic Health Record (I-EHR) is a key
element as it aggregates the patient health information
in all participating healthcare units.
The trust and security frameworks are imple-
mented in HYGEIAnet with VPNs, SSL, smartcards,
PKI, security certificates and digital signatures. A Re-
gional certification authority issues the certificates for
users and applications. These certificates can be used
to authentication and digital signing of documents and
in case of user certificates they can be stored in smart-
cards (?)
Authentication is a centralized process in
HYGEIAnet. All applications and services are
registered in the Health Resource Service (HRS)
and issued a unique ID. Each HYGEIAnet user also
must register in HRS to be able to use HYGEIAnet
services, and a unique user name and password is
provided. The username and password are com-
municated to an authentication server (AS) and a
certificate is issued from the regional CA.
In terms of authorization it follows a decentral-
ized approach, where each individual service main-
tains and manages roles (groups) and role based per-
missions. The user must be assigned to the proper role
in each service he is to have access.
When accessing a service, the user is authenti-
cated through the Authentication Service and gets his
individual access rights validated through the individ-
ual service.
The RTS and HYGEIAnet approaches for authen-
tication differ: HYGEIAnet has a centralised manage-
ment of resources (users and services), with certifi-
cates issued by a regional CA, and requires an online
AS for user authentication. On the contrary, RTS has
a decentralized management of resources, reusing the
management services belonging to the affiliated HIs,
with certificates issued by HI CAs for their own users
and services and not requiring any online user authen-
tication service to be used by RTS.
5.2 The Health Portal (Sundhed.dk)
and the Health Data Network of
Denmark (MedCom)
MedCom is the National Health Data Network of
Denmark. It is working since 1994, and it connects
more than 2000 Hospitals, Pharmacies, General Prac-
titioners (GPs) and Specialists. It started has a VAN
network exchanging EDIFACT messages (?). In 2004
it started the process of migration to the Internet and
EDIFACT messages were translated into XML mes-
sages. Today, both message formats are used (?).
Network security is implemented at three lev-
els (?; ?).
At the first level are VPN connections connecting
healthcare networks to a central hub in a star topology.
This solution allows the reuse of Internet connections
that all the health care units already have.
At a second level there is an agreement system
that controls the data flows from and to any of the lo-
cal healthcare networks. When a connection between
two healthcare networks is needed, a previous access
to the agreement system is required to establish the
connection between the two networks.
The third level of security is user authentication,
made locally through his username and password, or
his asymmetric key pair and PKC.
The Health Portal started in December 2003. It
works on top of the Health Data Network and reuses
its infrastructure and services. Unlike the Health Data
Network, that only provides services for Profession-
als, the Health Portal provides services for both Citi-
zens and Professionals (?).
User authentication, for both Citizens and Profes-
sionals, is made using OCES certificates
3
issued by
the national PKI that can be used in several national
public services. Professionals can use several OCES
certificates: (i) Administrativedigital signature for re-
gion, hospital or GP, (ii) health professional’s digital
signature based on personal identifier and (iii) autho-
rization for treating patients (?).
Comparing with RTS, the Danish system exten-
sively uses asymmetric keys and PKCs, benefiting
from a nation-wide PKI. However, many of the Dan-
ish system security requirements, such as Profession-
als’ digital signatures, are currently not required by
RTS, since it is not used for entering signed data into
the health information system. We believe, however,
that our architecture can evolve, but keeping its basic
structure, for provide security services similar to the
ones provided by Danish system. Furthermore, our
PKI may coexist with a national-wide PKI encom-
passing all HIs, though not necessarily using it.
3
OCES certificate: Public Certificate for Electronic Ser-
vice

6 PROTOTYPE
IMPLEMENTATION
As a proof of concept, a prototype of the authenti-
cation architecture was implemented. The prototype
extensively used available products for Windows op-
erating systems, because of its dominance in the com-
puter desktops of the HI currently affiliated to RTS.
The prototype included an RTS service, with a
two-level PKI and a web Server (Professionals’ Por-
tal), one HI instance, with a two level PKI, an Ac-
tive Directory Server and one registered Professional
(one smartcard). CAs were implemented with Win-
dows Certification Services available in Windows
2003 Server Enterprise Edition. When installed in
Enterprise mode, this CA interacts with AD to ob-
tain user information for certificate issuing, and uses
certificate templates, stored in AD and subject to AD
access control rules, for certificate issuance manage-
ment.
The key aspects to test in the prototype were (i)
the impact of different middleware software in smart-
card deployment, (ii) the deployment of an HI PKI for
the management of RTS credentials for local Profes-
sionals, and (iii) the use of short lived RTS credentials
to access RTS services.
6.1 Smartcard Deployment
Since smartcards are portable devices, in theory they
may be used to authenticate Professionals accessing
the RTS from different computers. However, this re-
quires some software installed in those computers: (i)
the card reader driver and (ii) middleware to fill the
gap between applications and smartcard services.
There are different trends in this specific middle-
ware area. Windows applications, such as the Internet
Explorer browser, use the CryptoAPI (CAPI), which
can use several Cryptographic Service Providers
(CSP) for interacting with different smartcards. An-
other approach is to use PKCS#11 (?), a standard
interface for cryptographic tokens. This interface is
used by Netscape and Firefox browsers.
Since middleware modules are usually specific for
smartcard manufacturers and some manufacturers im-
pose limits on the number of computers were they
can be installed or do not provide similar modules for
all operating systems, the following approaches were
foreseen: (i) the use of smartcards with native support
from the operating system, (ii) the use of open source
software or free binaries and (iii) the use of non-free
software providing support for multiple smartcards.
In our prototype we used only Windows XP sys-
tems for the Professional computers and two smart-
card tokens: Rainbow iKey 3000 and Schlumberger
4
Cyberflex e-gate 32k. None of them was natively sup-
ported by Windows. Also we were not able to get an
open source solution (openSC/CSP#11) working re-
liably. For the non-free solution we used SafeSign
Standard 2.0.3 software, and both smartcards worked
properly after their first initialization was made by
SafeSign. If this first initialization is not made by Safe
Sign, chances are that smartcards are not recognized,
has it happened with Cyberflex Card.
After low-level initialization (e.g. personaliza-
tion), smartcards were incepted with the Professional
HI credentials, allowing the owner to enrolment for
RTS certificates. The HI credentials cannot be re-
newed and the smartcard becomes useless when the
HI certificate validation period expires.
6.2 HI PKI Deployment
The HI PKI was implemented with an offlineRoot CA
and an online Issuer CA. The latter interfaces with an
AD and with an IIS 6.0 server with a web interface for
certificate enrolment, CRL Distribution Point (CDP)
and Authority Information Access (AIA) functionali-
ties.
Some groups were defined in AD, one for each
identified professional role, and Professionals as-
signed to them. They provide access control for cer-
tificate enrolment.
Certificates issued by the Issuing CA are tailored
using certificate templates. These templates allow the
definition of certificate characteristics and access con-
trol rules. Certificate templates were created, one for
each professional role that only differ in the specifica-
tion of certificate extensions and certificate security.
An application policy was defined for each Profes-
sional role, to be included in RTS certificates issued
for the role; application policies are simple ASN.1
OIDs used by RTS after reservation at IANA. The ap-
plication policy OID is stored in the certificate EKU
(Extended Key Usage) field. Also a certificate tem-
plate was defined for the HI certificate, with an appli-
cation policy for RTS certificate renewal.
Note that RTS certificates should contain all the
current roles of a Professional, and not only one.
However, that is simply not possible with certificate
templates and access control rules. Therefore, in the
prototype a Professional may have several RTS cre-
dentials, one for each role, and chose the proper one
when starting a session with the RTS Portal.
The customization of Windows certificate tem-
plates has also some limitations. Namely, certificate
templates do not allow for validity periods shorter
4
Now Gemalto, after being Axalto

than two days. This may be problematic if two days
is considered a large risk window for RTS credentials.
But in our opinion two days is perfectly reasonable.
The Issuer CAs also issues cross-certificates for
the public key of the RTS Issuing CA. Name con-
straints were used to define the name space for the ac-
cepted certificates. Certificate (issuance) constraints
and application constraints were not used because
they are not interpreted by browsers, since they re-
quire some application context (?).
A web interface, adapted from the Microsoft Cer-
tificate Services web interface, was deployed for en-
rolment for RTS certificates. After the Professional
authentication using its HI credentials, RTS certifi-
cates are immediately issued and installed in the Pro-
fessional’s smartcard. Both Internet Explorer and
Netscape can be used for RTS credential renewal.
6.3 Usage of RTS Credentials for
Accessing the RTS Portal
The validation of Professionals’ RTS credentials by
the RTS Portal, an IIS 6.0 web server, was performed
at two different levels. At the IIS level, validation
follows SSL rules and certification chains. At the ap-
plication level, validation includes checking RTS OID
values placed in EKU field of the received RTS cer-
tificate. The Portal only initiates a session with a Pro-
fessional if his certificate is considered valid at both
levels.
Finally, Professional can use both Internet Ex-
plorer and Mozilla Firefox to access the RTS Portal.
Tests were made in order to determine if the num-
ber PKCs from the HI PKI hierarchy in the smartcard
could be reduced, but due to different approaches be-
tween browsers for building and validation of certifi-
cate chain, we conclude that all certificates must be
present in order to allow both browsers to be used.
7 EVALUATION
In this section we evaluate the architecture and im-
plementation of our authentication system taking into
consideration the design goals presented in Section 3.
Concerning the first goal, a pragmatic PKI im-
plementation, it was achieved, since no specific,
large-scale PKI is required. On the contrary, the
PKI is build on top of independent PKIs and cross-
certification agreements. Trust relationships between
RTS and affiliated HIs are reflected in such cross-
certification and on common policies for issuing RTS
certificates for Professionals.
Concerning the second goal, Professionals’ mo-
bility, smartcards embedded in USB tokens are the
most promising solution nowadays but still raise some
problems. For instance, they (still) cannot be used
with PDAs and smartphones. Furthermore, and more
problematic, the usage of smartcards in USB-enabled
computers still raises the problem of software instal-
lation for dealing with them. As we saw in Section ??,
it is not simple to find a ubiquitous, free solution
for the middleware required by different applications
(browsers) to interact with many smartcards.
Concerning the third goal, leaving RTS out of the
management of Professionals working at the HIs, it
was totally attained. The RTS Portal only requires
Professionals to have a valid certificate issued by their
HI and containing a set of role on it. HIs have full
control on the management of local Professionals and
their role, enabling RTS access by issuing RTS certifi-
cates with the proper contents, namely Professional
identity, HI affiliation and possible roles.
The fourth goal, to minimize communication
overheads between RTS and HIs for authenticating
Professionals and getting their role, was also fully at-
tained. The RTS Portal, by itself, is capable of authen-
ticating Professionals just by validating their certifi-
cate, without checking CRLs remotely, and capable
of learning their role also from the certificate. No on-
line communication between RTS and HIs is required
in this process.
The fifth and final goal was browser compatibil-
ity. In this case we must say that it may be difficult
to provide the same set of functionalities with all the
browsers, because of the differences between the ex-
isting middleware solutions for bridging the gap be-
tween applications and smartcards (CAPI, PKCS#11,
etc.). Furthermore, some smartcard management ac-
tivities, such as garbage collection of useless creden-
tials inside the smartcard, may require the deploy-
ment of active code for running within Professionals’
browsers.
8 CONCLUSIONS
In this paper we described the design and imple-
mentation of an authentication architecture for Pro-
fessionals working within the RTS e-Health environ-
ment. Since Professionals access RTS services using
a browser and an RTS Portal, the authentication of
Professionals was mapped on top of SSL client-side
authentication. The credentials used in this authen-
tication are provided by their HIs and formed by a
private key and a short-lived X.509 PKC, both stored
inside a smartcard. The short lifetime of these certifi-

cates allows issuing CAs to simplify their PKI: they
are not published and they are not listed in CRLs.
The key characteristics of the authentication ar-
chitecture are (i) the use of smartcards for strong
authentication, to store Professional credentials and
to improve their mobility, (ii) the use of short-lived
RTS certificates carrying Professional identification
and roles for authentication on the RTS Portal and au-
thorization of operations required to the RTS, (iii) the
use of “normal”-lived HI certificates for Professional
enrolment for RTS certificates, (iv) a PKI where the
RTS and each HI run their own, private PKI with
(v) cross-certification for the establishment of trust
relations required to validate Professionals creden-
tials and RTS credentials within SSL sessions. This
authentication architecture is highly scalable and is
prepared to be applied to other medical telematic
projects such as the Brain Imaging Network Grid
(BING) (?) and the Grid-Enabled REpoSitories for
medicine (GERESmed), two medical networks now
under development an IEETA/University of Aveiro.
A prototype was implemented as proof of con-
cept and based exclusively in technology provided
by Windows systems or developed for Windows sys-
tems. Regarding the browsers used by Professionals,
we tested two of the most popular ones also on Win-
dows systems: Internet Explorer and Mozilla Firefox.
The major source of problems that we found for
implementing the prototype was the use and manage-
ment of smart cards by Professionals’ systems and
browsers. The variety of middleware existing for
managing smart cards and the different approaches
followed by different applications (browsers) regard-
ing the middleware make it very hard to provide a
clean, ubiquitous interface for Professionals. Further-
more, this is a critical issue in the deployment of this
authentication architecture along many different sys-
tems and computers.
ACKNOWLEDGEMENTS
This work was financed by the Aveiro Digital Pro-
gramme 2003-2006 of the Portugal Digital Initia-
tive, through the POSI programme of the Portuguese
Government, and by the FCT (Portuguese R&D
agency) through the programs INGrid 2007 (grant
GRID/GRI/81819/2006) and FEDER.
REFERENCES
Cunha, J. P. (2007). RTS Network: Improving Re-
gional Health Services through Clinical Telematic
Web-based Communication System. In eHealth Con-
ference 2007, Berlin, Germany.
Cunha, J. P. S., Cruz, I., Oliveira, I., Pereira, A. S., Costa,
C. T., Oliveira, A. M., and Pereira, A. (2006). The
RTS Project: Promoting secure and effective clinical
telematic communication within the Aveiro region. In
eHealth 2006 High Level Conference, Malaga, Spain.
Cunha, J. P. S., Oliveira, I., Fernandes, J. M., Campilho,
A., Castelo-Branco, M., Sousa, N., and Pereira, A. S.
(2007). BING: The Portuguese Brain Imaging Net-
work GRID. In IberGRID 2007, pages 268–276, San-
tiago de Compostela, Spain.
Dierks, T. and Rescorla, E. (2006). The TLS Protocol Ver-
sion 1.1. RFC 4346, IETF.
Housley, R., Ford, W., Polk, W., and Solo, D. (1999). In-
ternet X.509 Public Key Infrastructure Certificate and
CRL Profile. RFC 2459, IETF.
ISO 9735 (1988). Electronic data interchange for ad-
ministration, commerce and transport (EDIFACT).
http://www.iso.org
.
Katehakis, D. G., Sfakianakis, S. G., Anthoulakis, D., Kav-
lentakis, G., Tzelepis, T. Z., Orphanoudakis, S. C., and
Tsiknakis, M. (2005). A Holistic Approach for the
Delivery of the Integrated Electronic Health Record
within a Regional Health Information Network. Tech-
nical Report 350 (FORTH-ICS/ TR-350), Foundation
for Research and Technology - Hellas, Institute of
Computer Science, Heraklion, Crete, Greece.
Kent, S. and Atkinson, R. (1998). Security Architecture for
the Internet Protocol. RFC 2401, IETF.
Lloyd, S. (2001). CA-CA Interoperability. PKI Forum.
MedCom IV (2003). MedCom – the Danish Healthcare
Data Network. MedCom IV, Status Plans and Projects.
http://www.medcom.dk/dwn396
.
Pedersen, C. D. (2005). An baltic healthcare network and
interoperability challenges. Cisco eHealth think tank
meeting.
PKCS#11 (2004). PKCS #11 v2.20: Cryptographic Token
Interface Standard. RSALaboratories.
Ribeiro, C., Silva, F., and Z´uquete, A. (2004). A Roaming
Authentication Solution for WiFi using IPSec VPNs
with Client Certificates. In TERENA Networking Con-
ference 2004, Rhodes, Greece.
Rossing, N. (2005). The Health Portal (www.sundhed.dk)
And The Health Data Network Of Denmark. Execu-
tive Summary of Presentaion in eHealth Athens 2005.
http://www.ehealthathens2005.gr
.
Sundhed.dk (2006). The Danish eHealth experi-
ence: One Portal for Citizens and Professionals.
http://dialog.sundhed.dk
.
Tsiknakis, M., Katehakis, D. G., Sfakianakis, S., Kavlen-
takis, G., and Orphanoudakis, S. C. (2005). An Ar-
chitecture for Regional Health Information Networks
Addressing Issues of Modularity and Interoperability.
Journal of Telecommunications and Information Tech-
nology (JTIT), 4:26–39.
Voss, H., Heimly, V., and Sj¨ogren, L. H. (2005). The
Baltic ehealth Network – taking secure, Internet-based
healthcare networks to the next level. Norwegian Cen-
tre for Informatics in Health and Social Care.
