
INSTR
UMENTATION AND LABVIEW BASED CONTINUOUS
PROCESSING FOR CHEST PHYSIOTHERAPY
Luc Marechal, Christine Barthod, G
´
erard Gautier, Jacques Lottin
Laboratory SYstems and Materials for MEchatronics (SYMME),University of Savoie, BP80439, Annecy-le-Vieux, France
Jean Claude Jeulin
R
´
eseau Bronchiolite de Haute Savoie (RB74), 8 avenue de champ fleuri 74600, Seynod, France
Keywords:
Force Sensing Resistor Sensors, Motion Sensors, LabVIEW, Continuous Processing, Infant Chest Physiother-
apy.
Abstract:
Infant chest physiotherapy (CPT) has never been the purpose of any assessed scientific study although it is
widely used for newborn babies suffering from bronchiolitis. It is thus compulsory to quantify the limits of
the gesture to obtain the expected effect. In this paper, we present original instrumented gloves designed to
perform measurements during the CPT act on babies to characterize the gesture. Associated electronics and
software were specially developed with LabVIEW for data acquisition, continuous processing and analysis of
the characteristic parameters. The measuring system and its readout electronics were calibrated. A drive to
do measurement with babies in real situation validates the principle of the system. The analysis of the results
highlights relevant parameters for typical phases of the CPT act.
1 INTRODUCTION
As the demand for clinical or medical instrumen-
tation design increases rapidly, the techniques and
methods used to convert medical and physiological
information to electrical signals grow too. Quan-
titative responses must be relevant to allow a bet-
ter understanding of the medical or clinical analysis
through computer interfaces. In surgery or physio-
therapy for example, the characterization of the ges-
ture for a medical or a clinical act is more and more re-
quired (Davidson, 2002). The need of standard quan-
titative definition of chest physiotherapy gesture ex-
pressed by physiotherapists is at the beginning of our
study. Hardly any study concerning the character-
ization of infant chest physiotherapy technique has
been achieved. This paper presents the method and
the system for the characterization of the physiothera-
pist gesture when performing chest physiotherapy act
on newborn babies. First a chest physiotherapy tech-
nique is rapidly described in order to explain the need
of practitioners regarding the definition and character-
ization of their gesture. We present the implementa-
tion of force and displacement sensors on innovative
instrumented gloves that we designed to record the
characteristic parameters of the gesture. In a second
part, the study of the different components of a com-
puter based measuring system is detailed. In partic-
ular, the acquisition system, the readout electronics,
the acquisition program and important details of the
coding are presented. Finally, measurement results
are proposed, showing the reliable capability of the
system to give a scientific definition of the gesture.
2 MEASURING SYSTEM
2.1 Medical Context
Bronchiolitis is an acute disease of the respiratory
tract that affects young babies. In French-speaking
European countries, the two consensus conferences,
held in 1994 and 2000, concerning the management
of bronchiolitis in infants have widely recommended
the use of chest physiotherapy in order to provide care
(ANAES, 2000). These techniques aim at generat-
ing forced respirations in order to improve bronchial
pulmonary exchanges. More particularly in France,
the forced expiration maneuver used is the Increase
41
Marechal L., Barthod C., Gautier G., Lottin J. and Claude Jeulin J. (2008).
INSTRUMENTATION AND LABVIEW BASED CONTINUOUS PROCESSING FOR CHEST PHYSIOTHERAPY.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 41-46
DOI: 10.5220/0001049800410046
Copyright
c
SciTePress

of Expiratory Flow technique (IEF). IEF technique
is a thoracic-abdominal movement generated by the
hands of the physiotherapist on the infant’s chest. The
infant being lain on a table, the physiotherapist places
one hand on the thorax close to the neck and the other
hand on the abdomen. The ”thoracic hand” presses
uniformly with its cubital part whereas the ”abdomi-
nal hand” has a global support. The applied pressure
sequences must be synchronized with the infant free
respiratory cycle.
2.2 Assesment of Needs
These last years, due to management with the IEF
technique, results have shown an improvement of the
clinical evolution of babies’ health preventing many
of them from reaching the critical state of the hospi-
talisation (Postiaux et al., 2006). Consequently, the
CPT act is more and more used and the efficiency of
this physiotherapy technique is now currently admit-
ted in France. Although the IEF technique requires
a good know-how, the physiotherapist has an empiric
approach and relies his practicing on his own percep-
tion. He adapts and controls the magnitude and the
frequency of the gesture versus the sound of the in-
fant respiratory system and his own sense of touch.
A qualitative protocol for the IEF technique has been
defined (Fausser et al., 2002) but no quantitative def-
inition has been made. The demand is then twofold:
on one hand, to prove the efficiency of the gesture for
validating the technique; on the other hand, to char-
acterize the gesture to enhance learning and create di-
dactical situations.
2.3 Implementation of Force and
Displacement Sensors
As it was decided to quantitatively define the basic
gesture of the IEF technique, technical discussions
between instrumentalists and expert physiotherapists,
about the practical knowledge for doing the efficient
gesture, allowed to choose its physical parameters to
record. So, specific instrumented gloves were de-
signed to measure during the CPT act (Mar
´
echal et al.,
2007): the space displacement of the physiotherapist
hands, and the distribution of the force applied by the
hands on the infant’s chest. A third relevant parameter
consisting of the sound of the infant respiratory sys-
tem has to be taken into account too. Thus, the mea-
surement system should neither modify the physio-
therapist’s gesture nor being cumbersome or disturb-
ing for the infant.
Since the force measurement system must be thin,
flexible and painless for the baby, and because the
force applied by the practitioner is as well quasi-static
as dynamic, Force Sensing Resistor sensors (FSR)
from Interlink Electronics were chosen. FSR are
polymer thick film (PTF) devices which exhibit a de-
crease in resistance with an increase in the force ap-
plied to the active surface (Interlink, 2004). After an
exhaustive comparative study of different sensors, we
have chosen the most appropriate one as far as their
size and cost are the lowest, for equivalent technical
properties. Such sensors have already been used for
biomedical devices (Morris et al., 2006).
The FSR sensors are glued on a cotton glove by
an adhesive band (supplied by 3M). What is innova-
tive with such gloves is the location of the sensors.
Investigation of the contact between the physiother-
apist hands and the infant body has been led so that
we can characterize it. The contact shapes have been
determined after several tests according to the refer-
ent physiotherapist, so that the most interesting pres-
sures applied during the IEF act can be seen and mea-
sured. Regarding hygiene and medical environment, a
thin medical latex glove is worn over the instrumented
glove so that the sensors are not directly in contact
with the skin of the toddler.
Besides, the measurement of the position of the
hands of the physiotherapist is performed thanks to
a six-degree of freedom electromagnetic tracking de-
vice, the Flock of Birds (FoB, from Ascension Tech-
nology). It is composed of one transmitter and two re-
ceivers. Each receiver is placed on a cotton glove on
the upper side of the back of each hand. Manufacturer
claims that the system accuracy is 1.8 mm and 0.5
◦
RMS for position and orientation respectively within
a working range of ± 1.2 m in any direction. No con-
ductive material must be present near the system be-
cause interferences produce significant error measure-
ment (LaScalza et al., 2003). This system is suited
to our application because the transmitter is placed 30
cm far from the head of the baby and the displacement
of the hands doesn’t exceed 5 cm in each direction.
2.4 Signal Conditionning
Preliminary trials were made with the referent physio-
therapist in order to determine the range for our appli-
cation. Then, we designed the FSR signal condition-
ing according to the manufacturer’s advices among
suggested electrical interfaces.
For a force-to-voltage conversion, the FSR device
is the input of a current-to-voltage converter. In the
shown configuration (Figure 1), the output voltage is
inversely proportional to the FSR resistance. An out-
put swing of 0 V to 10 V is desired to enhance the
sensitivity of the measurement system. Vref is set to -
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
42
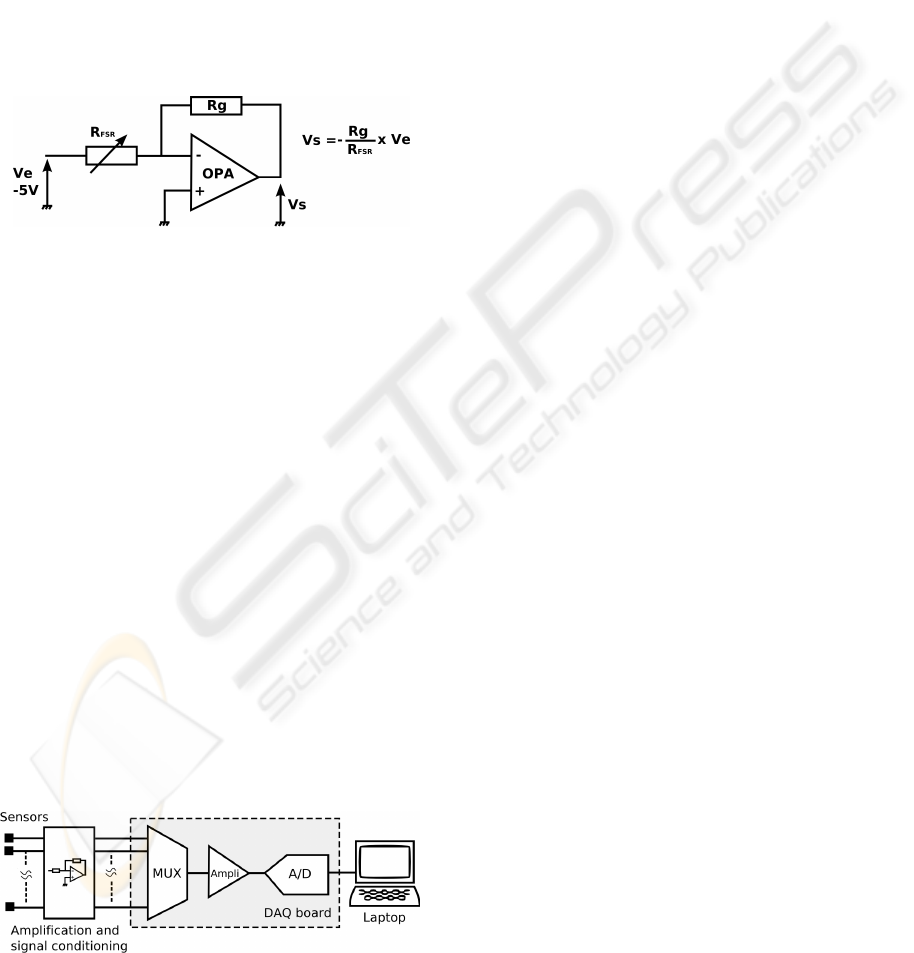
5 V. It is to be noticed that a variation of the reference
voltage would lead to a variation of the output volt-
age. The supply voltage should be constant. Hence,
a precision voltage reference, the AD584, was cho-
sen for that purpose. The current through the FSR
should be limited to less than 1 mA/cm
2
of applied
force, to prevent from damaging the sensor. Rg value
of 15 kΩ was chosen to limit the current and maxi-
mize the output voltage range. Moreover, the risk of
electronic noise is avoided with these sensors because
the value of resistance in the feedback loop is high
enough. This circuit is simple, easy to implement, re-
liable and costless.
Figure 1: FSR associated electronics.
3 DATA ACQUISITION AND
PROGRAMMING
FSR sensors voltage responses are acquired using
a NI-9205 DAQ card and NI cDAQ-9172 compact
chassis for USB interface communication. It fea-
tures a 32 single-ended analog inputs with a sampling
rate up to 250 ksamples per second. Figure 2 is a
block diagram of the system. The program is written
in Graphical programming using National Instrument
LabVIEW version 7.1 since dataflow language is well
adapted for application with parallel tasks. Sampling
rate was chosen at 200 Hz for each sensor. This has
been defined after tests and recordings of the CPT act:
observation of the gesture pointed out important vari-
ations lasting about 100 ms. In order to have enough
samples to acquire and plot the signals, we chose
a resolution of 5 ms which is well adapted to have
enough accuracy.
Figure 2: Acquisition block diagram.
3.1 Continous Processing (Figure 3)
In the aim to display the measurements when the
gesture is being performed, we decided to process
the signals on-the-fly during their acquisition. The
length of the trial, up to several minutes, and the num-
ber of signals (fifteen) increase rapidly the amount
of the collected data. Regarding these parameters,
the recording of the data must be done throughout
the measurement. The DAQ board performing the
acquisition stocks the samples in its circular mem-
ory. The Ni DAQmx driver ensures the continuous
transfer of the digitized data to the computer memory.
The reading of the samples is done block by block
with the LabVIEW program by the Analog Input (AI)
Read routine returning data from the buffer. This high
level priority routine is expensive in terms of perfor-
mance. As a matter of fact, for slow frequency rate
acquisition when AI Read is called, data might not be
all present in the buffer. So, AI Read will wait for
data to be available. This waiting time from a pri-
ority task involves heavy performance cost. To rem-
edy this, Ch
ˆ
alons recommends an optimisation of the
computer resources when a continuous processing is
desired (Ch
ˆ
alons, 2001). In order to acquire and pro-
cess a continuous amount of data, we used a new pro-
gramming technique in our code which stands for a
call of the AI Read routine only when needed. To do
so, a variable is used to indicate the number of analog
input data remaining in the buffer. The new version
of the DAQ driver NI-DAQmx 8.3 makes easier the
programming by using a simple Read property node
that returns the state of the buffer. This frees enough
resources to activate other asynchronous tasks that are
less time critical such as display and file storage, and
allows continuous display.
This solution is low cost to perform ”real time”
acquisition and display, in comparison to Real Time
hardware modules. The program runs on a conven-
tional Laptop PC, Pentium M CPU at 1.6 GHz with
512 MB RAM under Windows 2000. Any reasonably
current PC should be compatible with our measure-
ment system. The program has been tested and shown
to operate reliably.
3.2 Monitoring and Visualization
Before each trial, a user friendly interface enables the
user to supply information about the management of
the patient. Sex, age, size, weight and pathology are
also asked. A text box is dedicated to comments and
evolution of the clinical state. All information are
saved in a result file detailed further. While gesture is
performed by the physiotherapist, waveform plot dis-
INSTRUMENTATION AND LABVIEW BASED CONTINUOUS PROCESSING FOR CHEST PHYSIOTHERAPY
43
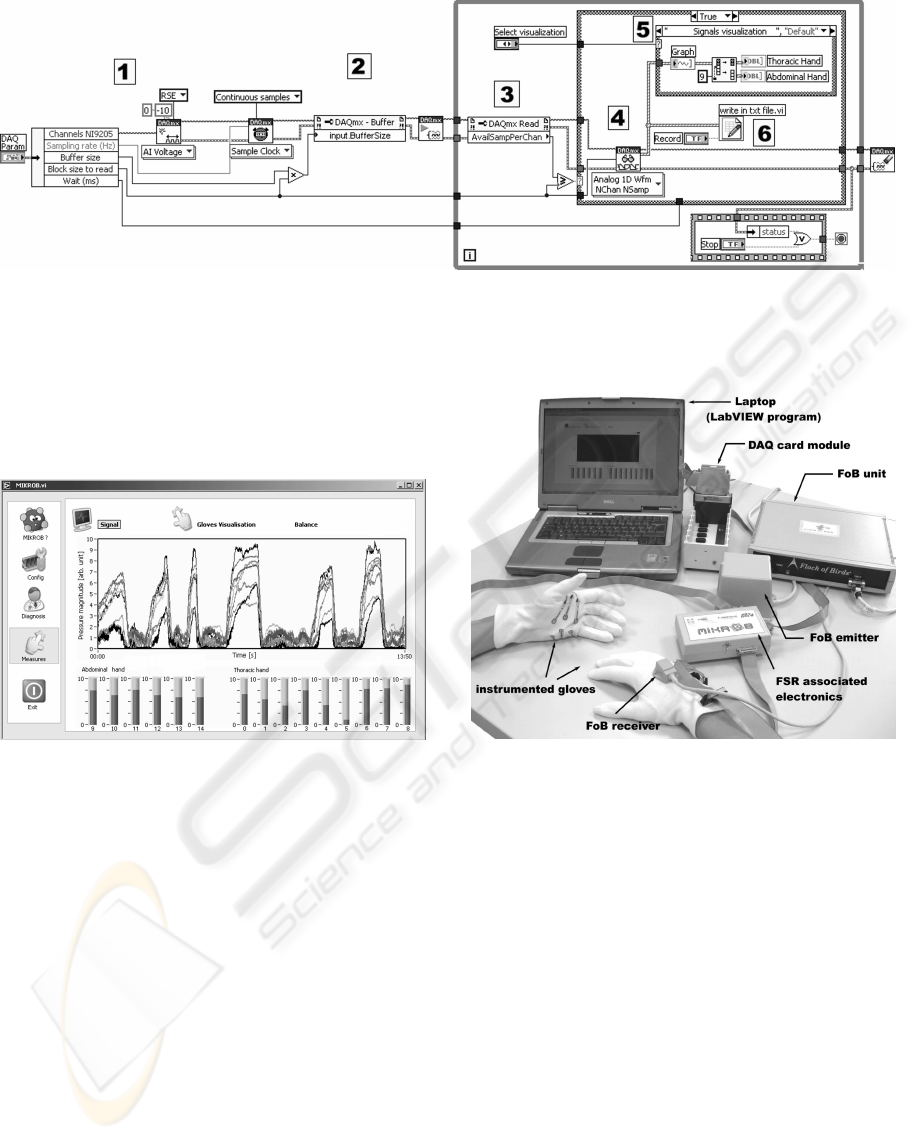
Figure 3: Structure of the LabVIEW acquisition program: (1) acquisition configuration; (2) definition of buffer size; While
loop: (3) reading buffer state; (4) reading of samples by AI read routine if the buffer is fulfilled; (5) graphical display update
and (6) file storage when AI read routine is not solicited.
plays signals issued from each sensor in ”real time”.
The monitoring screen is presented Figure 4.
Figure 4: Monitoring screen.
Simultaneously to force measurements, the trajec-
tories of the hands are recorded with the FoB sensors
located on the gloves. The whole system is presented
Figure 5.
3.3 File Output
For each trial the program saves the data in a *.txt file.
Spreadsheet file format compliant for common soft-
ware such as Microsoft Excel or OpenOffice Calc was
not chosen because they have a limitation of 65536
rows. The file contains the values of the output data
of the fifteen sensors versus the time, for each mea-
surement. It also contains the acquisition parameters:
measurement rate, trial start and end times. The aver-
age size of the result files is of 10 MB which is accept-
able in comparison with actual disk space capabilities.
Figure 5: Whole measuring system.
4 FIRST RESULTS
4.1 Calibration System Validation
Calibration of FSR devices before use is of inevitable
occurrence. Calibration curves supplied by the man-
ufacturer are carried out with the sensor placed be-
tween two rigid materials. However, it is worthwhile
noting that the response of this kind of sensor depends
on the nature and shape of the contact. Consequently,
FSR sensors should be calibrated in the same situa-
tion as the use. Former studies focused on measur-
ing forces developed by the human hand when grip-
ping objects (Nikonovas et al., 2004). In this work,
Nikonovas used FSR sensors between human hand
tissues and stiff surface, nevertheless calibration was
not made in the conditions of their use. Besides, Cas-
tro (Castro and CliquetJr, 1997) placed small rigid
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
44
plates over and under the active area of the sensor
to improve its behaviour during use, but for calibra-
tion the force was applied thanks to a small sphere.
Regarding our application, the contact is between hu-
man hand tissues and human body tissues. Pertaining
to the work of Castro, in order to enhance FSR re-
sponse, we thought to insert plates on both sides of
the sensors, but we can’t mount them on rigid sub-
strates since they could injure the infant during the
CPT act. For use and calibration, we also tried to in-
sert the sensors between different flexible substrates
such as thin layers of polymer materials or silicones
but it had no relevant effect on sensor response.
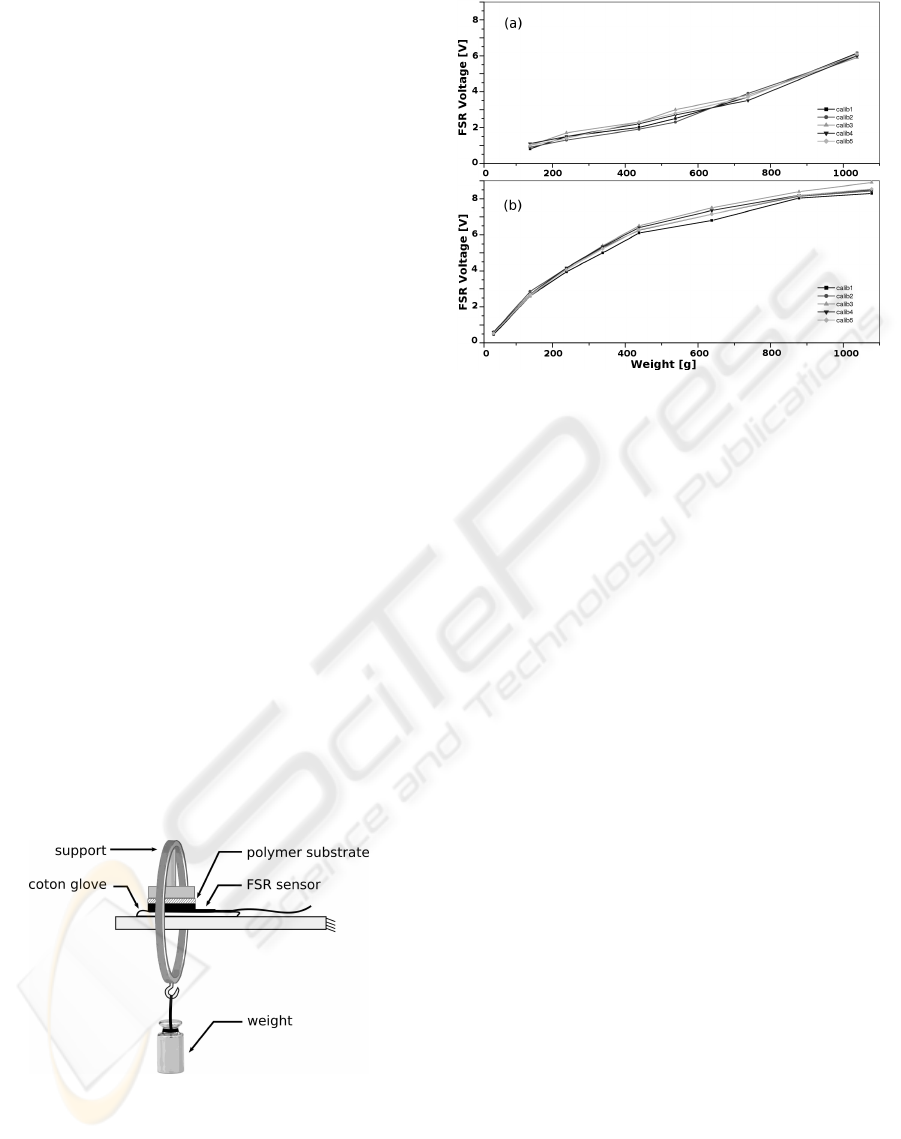
A specific workbench is implemented to calibrate
the sensors in order to be in a situation closest as pos-
sible as between hand covered by cotton material and
body (Figure 6). A plate of metal covered with a poly-
mer layer realises the distribution of the applied force.
We made comparative calibration to highlight the im-
pact of the substrate. Dead loads in range of 0.1 kg to
1 kg were applied to the active surface of each sensor.
With the same applied force but with different im-
plementations, the sensor’s response is strongly dif-
ferent. Figure 7 shows the calibration curves for the
same sensor; alone (a) and implemented on the glove
(b). In the end, keeping in mind that the stiffness of
the hands of two physiotherapists may be very dif-
ferent, we decided to calibrate the sensor with identi-
cal impementation for all measurements. So, we use
the static calibration curve obtained with the bench
described before, the FSR being implemented on the
cotton glove and covered with a medical glove.
However, the calibration gives the part-to-part re-
peatability but is not able to provide the absolute force
magnitude during the measurement on newborn ba-
bies.
Figure 6: Calibration System.
4.2 Measurement Results
The measurement with the whole system was per-
formed in a physiotherapist consulting room from
Figure 7: FSR calibration curves: (a) alone; (b) imple-
mented on the glove.
January to March 2007. The study was managed tak-
ing into account a population of 25 infants aged from
5 to 7 months suffering from bronchiolitis. This ran-
dom trial was performed by the same expert physio-
therapist, J.C. Jeulin.
Figure 8(a) shows the sensors responses acquired
on the thoracic hand glove during two compressions
on the chest of a 5-month-old infant, for a sequence
of the gesture called ”fast IEF”. The FSR responses
evolve synchronously. They are repeatable since the
rising time of the applied pressure and the magnitude
of the forces remain constant for each sensor in each
compression. The displacement of the thoracic hand
in the direction perpendicular to the table plane dur-
ing one compression of a ”fast IEF” is reported on
Figure 8(b). These first results are consistent with
the gesture qualitatively described as the referent one
by the expert.
5 CONCLUSIONS
The measuring system, designed and created to record
hands applied pressures and displacement during the
act, has been validated. The choice of the sensors
and their implementation respect the medical environ-
ment. Specific calibration according to the use has
been achieved. Low cost portable hardware is used
to acquire sensors signals. Custom optimized soft-
ware has been developed with LabVIEW to process
and display the data as in real time. The first results
obtained are reproducible and consistent with the ex-
pert sensations. Our ongoing work in the framework
INSTRUMENTATION AND LABVIEW BASED CONTINUOUS PROCESSING FOR CHEST PHYSIOTHERAPY
45
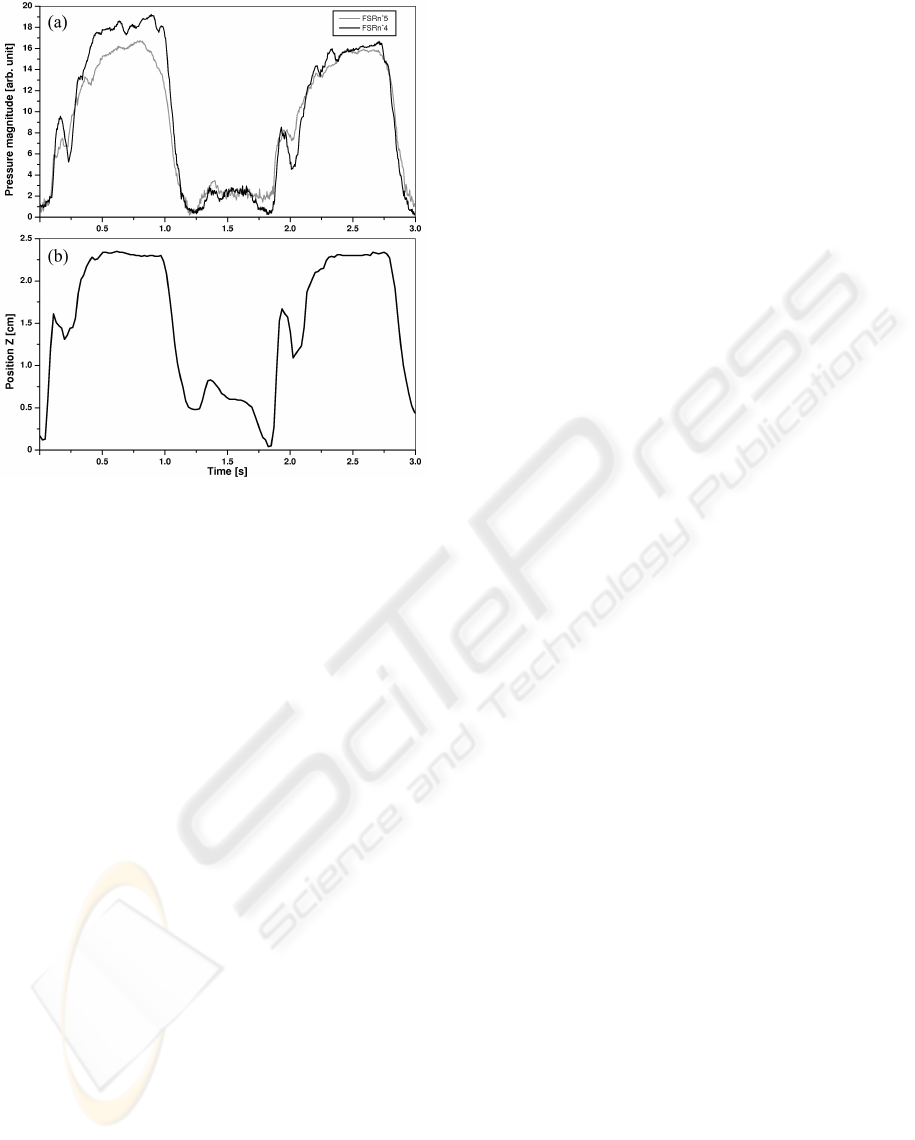
Figure 8: (a) Pressure (two FSR) and (b) displacement
(FoB) responses of sensors on the thoracic glove.
of CPT enables quantitative investigations of the ges-
ture.
ACKNOWLEDGEMENTS
Authors thank Laboratory Amp
`
ere (Lyon, France),
for lending us one Flock of Birds device, and the As-
sembl
´
ee des Pays de Savoie for funding this project.
REFERENCES
ANAES (2000). Consensus conference of management of
bronchiolitis in infant. Arch.Ped2001.
Castro, M. and CliquetJr, A. (1997). A low-cost instru-
mented glove for monitoring forces during object ma-
nipulation. IEEE Trans. Rehab. Eng., 5(2):140–147.
Ch
ˆ
alons, J. (2001). Acquisition and processing, daq-sc-01-
jmc-a40119. SAPHIR. www.saphir.fr.
Davidson, K. (2002). Airway clearance strategies for the
pediatric patient. Respir Care, 47(7):823–830.
Fausser, C., Breheret, V., and Lopes, D. (2002). Aug-
mentation du flux expiratoire (afe) et tol
´
erance. KS,
(428):21.
Interlink (2004). Force sensing resistor integration guide.
Interlink Electronics.
LaScalza, S., Arico, J., and Hughes, R. (2003). Effect of
metal and sampling rate on accuracy of flock of birds
electromagnetic tracking system. Journal of Biome-
chanics, 36(1):141–144.
Mar
´
echal, L., Lottin, J., Barthod, C., Gautier, G., Goujon,
L., and Jeulin, J. (2007). Instrumented gloves for ges-
ture characterization during chest physiotherapy act
on babies. In 8th International workshop on Research
and Education in Mechatronics, Tallin, pages 171–
176.
Morris, S., LaStayo, P., Dibble, L., Musselman, J., and
Raghavendra, S. K. D. (2006). Development of a
quantitative in-shoe measurement system for assess-
ing balance: sixteen-sensor insoles. In 28th IEEE
EMBS annual International Conference, New York,
pages 6041–6044.
Nikonovas, A., Harrison, A., Hoult, S., and Sammut, D.
(2004). The application of force-sensing resistor sen-
sors for measuring forces developed by the human
hand. Proc Inst Mech Eng, 218(2):121–126.
Postiaux, G., Dubois, R., Marchand, E., Denay, M., Jacquy,
J., and Mangiaracina, M. (2006). Chest physiother-
apy in infant bronchiolitis: a new approach - ncpt
including elpr-expiration lente prolong
´
ee and tp-toux
provoqu
´
ee. Kinesither. Rev., (55):35–41.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
46
