
RESURE
Wireless Sensor Network for Health–Care Monitoring
Enrique A. Vargas Cabral, Vicente A. Gonzalez and Jean A. Guevara
Departamento de Electr
´
onica e Inform
´
atica, Facultad de Ciencias y Tecnolog
´
ıa
Univ. Cat
´
olica, Campus Univ.–Tte. Cantalupi y Villalon, Asunci
´
on, -Paraguay
Keywords:
Wireless Personal Area Network (WPAN), IEEE 802.15.4, Zigbee, Medical Care, Physiological signals.
Abstract:
This work presents a sensor system to monitoring a patient vital signs remotely. The proposed sensor network
architecture is based on IEEE 802.15.4 PAN technology with start topology. An experimental set-up was
implemented including the development of some biological sensors. In the implementation stage we use Xbee
modules, the remote sensors was configured as RFD devices and the network coordinator as FFD device. As
central device a smart phone was used. From the results, we conclude that the IEEE 802.15.4 technology is
appropriate for medical WPAN sensor network implementation.
1 INTRODUCTION
The World Health Organization (WHO) estimates that
by the year 2025, more than 1,000 million people will
be older than 60 years (WHO, 2004), in other words,
the average age of the world-wide population is in-
creasing. Normally, the aging comes accompanied
by non-transmissible chronic diseases, such as car-
diovascular disease and others that need a continuous
monitoring. This scenario presents many challenges
to modern societies; one of them is the design of sen-
sor systems that can continuously record physiolog-
ical variables, from these variables the health of the
people can be inferred (Woodward and Rasid, 2003).
Nowadays, the technological advances in micro-
electronics and instrumentation ease the development
of sophisticated, small size, low power consumption
and relative low cost monitoring systems. In addi-
tion, the WPAN technology allows easy and fast in-
terconnection of different kind of elements, i.e. ear-
pieces for mobile phones, video, camera, audio re-
producer, computers, etc. Therefore, the new tech-
nologies offer the possibility of transmitting physio-
logical signs for processing or visualization devices
(PCs, PDAs, screen, etc.) or to processing center
without limiting the patient mobility (Rodr
´
ıguez, J.
et al., 2005). Due to medical and economical rea-
sons, shorter periods of inpatient stay are desirable.
Patients’ monitoring at home environments is one of
the most attractive areas for WPAN applications (Karl
and Willig, 2005), because this technology can en-
able seamless connectivity in hospital and home en-
vironment. A WPAN central device can be imple-
mented as a wristwatch or a small belt-worn box.The
device could be able to communicate with the hos-
pital monitoring system using the home network ac-
cess points via wireless indoor communication sys-
tems like WLAN, DECT or Bluetooth. WPAN moni-
toring is also adequate for patients with chronic dis-
eases such as diabetes, asthma and cardiovascular dis-
eases. The employing of WPAN in the patient’ home
is useful for rehabilitation and post operational care.
A central WPAN device with modules for accessing
global wireless networks like GSM or UMTS can pro-
vide potentially worldwide mobility for WPAN users
(Istepanian, R. et al., 2001). Summarizing, we can
say that quality of life can be significantly improved.
2 REQUERIMENTS OF
A MEDICAL SENSOR
NETWORKS
A medical sensor network design greatly depends on
the application and deployment environment. A sen-
sor network designed for ad hoc deployment in an
emergency site has very different requirements than
one deployed permanently in a hospital. For exam-
ple, the latter can make use of fixed, wall powered
gateway nodes, which provide access to a wired net-
work infrastructure. In general, we can identify seve-
101
A. Vargas Cabral E., A. Gonzalez V. and A. Guevara J. (2008).
RESURE - Wireless Sensor Network for Health–Care Monitoring.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 101-106
DOI: 10.5220/0001050101010106
Copyright
c
SciTePress

ral characteristics that nearly all medical sensor net-
works should have (Shnayder, V. et al., 2005).
• Scalability: is the capability of a system to in-
crease performance when new nodes are added.
• Wearable Sensor Networks (WSN):Medical ap-
plications require very small, lightweight, and
wearable sensors. Power consumption in a WSN
is important since most or all devices must be bat-
tery powered. Replacing or recharging in short in-
tervals will be impractical, so power consumption
is of significant concern.
• Reliable communications:In medical settings, a
great emphasis is placed on data availability, al-
though intermittent packet loss due to interference
may be acceptable. However, persistent packet
loss would be a problem. Depending on the used
sensors, sampling rates may vary between 1 to
1000 Hz or more, placing heavy demands on the
wireless channel.
• Device mobility:Both patients and caregivers are
mobile, requiring that the communication layer
adapt rapidly to changes in link quality. For ex-
ample, if a multihop routing protocol is in use,
it should quickly find new routes when a doctor
moves from room to room during his rounds.
• Security:The security in wireless networks is al-
ways of great importance. In sensor networks, it is
especially important to have integrity and authen-
tication. Integrity means that data should not be
altered or destroyed in its way from the sender to
the receiver and the authentication should ensure
the identity of the sender and the receiver.
• Association:The service used to establish a de-
vice’s membership in a WPAN. How a WPAN
adds a new node is of interest in this kind of net-
works. As well as how one sensor is associated
with the correct output at the central monitor side.
• Cost:To be able to compete in the international
market it is essential that the components be at
the lowest possible price. This is most important
when the product shall be mass-produced.
3 SHORT RANGE WIRELESS
TECHNOLOGIES
Based on the above mentioned requirements of med-
ical WPAN systems, following the technical charac-
teristics of some wireless technologies are presented,
which according to the bibliographical review and our
criteria, can be used to design a medical WPAN.
3.1 IEEE 802.15.1 / Bluetooth
The IEEE 802.15.1 standard is derived from the Blue-
tooth specification (version 1.1). In fact, the IEEE
standard has added two clauses to the existing specifi-
cation; WPAN architecture overview and Service Ac-
cess Points (SAPs). In other words, the 802.15.1 stan-
dard presents a wireless personal area network that
utilizes the Bluetooth wireless technology. A PAN
is defined as a computer network used for communi-
cation among computer devices close to one person.
The Bluetooth WPAN operates in the unlicensed 2.4
GHz industrial, scientific and medical (ISM) band.
The Bluetooth 1.0 data rates include an asymmetric
data rate of 721 kbit/s while permitting 57.6 kbit/s
in the return direction; and a symmetric data rate of
432.6 kbit/s (IEEE Standard, 2002).
3.2 IEEE 802.15.4 /Low-Rate WPAN
IEEE 802.15.4 is a standard defined for low-rate (LR)
WPANs. A LRWPAN is a simple, low cost com-
munication network that allows wireless connectiv-
ity in applications with limited power and relaxed
throughput requirements. The main objectives of a
LR-WPAN are ease of installation, reliable data trans-
fer, short-range operation, extremely low cost, and a
reasonable battery life (IEEE Standard, 2003). Like
all IEEE 802 standards, the IEEE 802.15.4 standard
encompasses only those layers up to and including
portions of the data link layer (DLL). I.e. the standard
802.15.4 defines only the PHY and the medium ac-
cess layers (MAC). In particular, it defines two PHYs
representing three license-free frequency bands that
include sixteen channels at 2.4 GHz, ten channels at
902 to 928 MHz, and one channel at 868 to 870 MHz.
The maximum data rates for each band are 250 kbps,
40 kbps and 20 kbps, respectively. A WPAN consists
of several components; the most basic is the device.
There are two different device types, which can par-
ticipate in an LR-WPAN; a full-function device (FFD)
and a reduced-function device (RFD). A FFD can talk
to RFDs or other FFDs, while an RFD can talk only
to an FFD. An RFD is intended for applications that
are extremely simple, such as light switches or pa-
ssive infrared sensors; they do not have the need to
send large amounts of data and may only be associa-
ted with a single FFD at a time. Because of that, the
RFD can be implemented using minimal hardware re-
sources (Thraning, 2005).
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
102
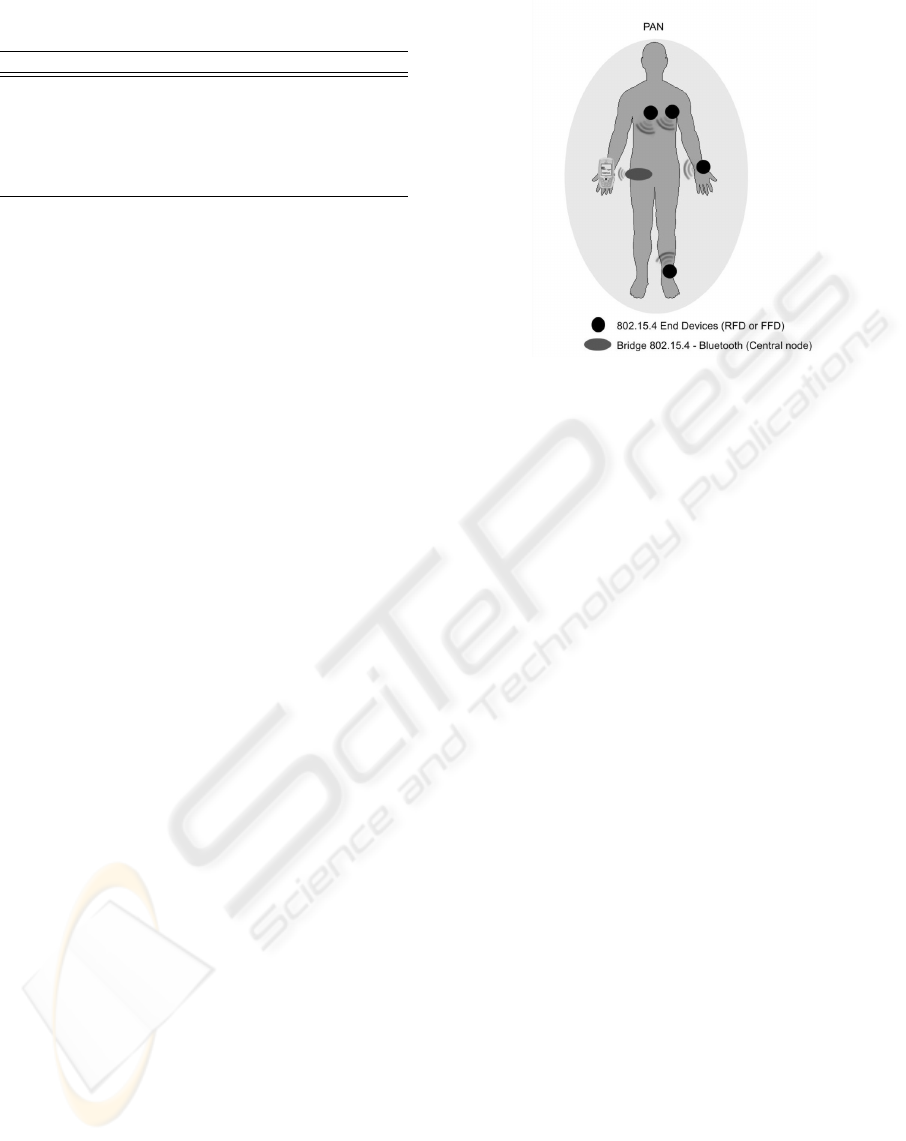
Table 1: Comparison of short–range low power wireless
technologies.
Bluetooth 802.15.4 ZigBee
Data rate(Mbit/s) 1 0.250 0.250
Range(m) 10-100 10-100 10-100
Power supply Medium Very low Low
Security High Medium High
Scalability 7 255 255
Cost Medium Very low Low
3.3 Zigbee
ZigBee was created to address a specific market need
for an industrial standard to support automation and
remote control applications. The ZigBee Alliance
decided to use the IEEE 802.15.4 standard as the
Physical layer and Media Access Control sub-layer,
while the ZigBee Alliance defines the upper layers.
The ZigBee network layer supports multiple network
topologies including star, cluster tree, and mesh. The
application layer consists of the application support
layer (APS), the ZigBee device object (ZDO) and the
manufacturer-defined application objects. The APS is
responsible for maintaining tables for binding and for-
warding messages between bound devices. A binding
is the ability to match two devices together based on
their services and their needs. The binding include the
device discovery, which is the procedure to discover
other devices that are operating in the same area (Zig-
Bee Alliance, 2005).
The different IEEE 802.15 standards were de-
signed with different purposes. Bluetooth was de-
signed to replace cabling connections between de-
vices, while 802.15.4 and ZigBee for network sen-
sor targeted to home automation. Therefore, none of
them was specifically designed to be used in medical
sensor network.
4 PROPOSED ARCHITECTURE
FOR THE SENSOR SYSTEM
In the absent of a specific standard, in this work we
propose the use of the IEEE 802.15.4 and Zigbee
standard as the more adequate solution for medical
WPAN sensor networks. Most Bluetooth modules are
not appropriate because its power requirement is high
for battery-operated devices that cannot be charged or
changed regularly. It is also restricted by its scalabil-
ity capacity; it can only have seven active nodes in one
network. 802.15.4 and ZigBee looks like a perfect fit,
except for its low data rate. This technology presents
low power requirement because the nodes are in sleep
mode most of the time.
Figure 1: Proposed network architecture for biological
signs monitoring.
By using ZigBee mesh topology supports (Thran-
ing, 2005) there is no need of a master node in the
WPAN, in this configuration every node/sensor can
communicate directly and each node acts as a router.
This way a data flow from one node can take multiple
routes to its destination, making it very resilient; if a
node drops out the flow, it is redirected through other
nodes. A routing algorithm is used to ensure that the
data takes the fastest possible route.
A drawback of mesh networking is synchroniza-
tion. Two or more data flows that need to be time syn-
chronized at the receiver may take different routes, re-
sulting in different time delays. If this delay is greater
than what is possible to buffer, data lost occur. To
overcome the above mentioned problem, in this work
we propose the use of IEEE 802.15.4 technology with
a star network topology. With respect to power con-
sumption, this technology has suitable characteristics
for medical WPAN application since it was originally
developed to have low power consumption; i.e. idea-
lly a node should work for months or years without
batteries changes. In addition, the standard was devel-
oped for the communication between sensors, which
reduces its complexity, allowing lower implementa-
tion costs than Bluetooth technologies.
5 EXPERIMENTAL SET-UP
In order to validate the proposed network an experi-
mental set-up was implemented, including the devel-
opment of some biological sensors. Figure 1 presents
the proposed network architecture. In the proposed
topology the sensors are RFD devices which commu-
nicate to a central node, configured as FFD.
RESURE - Wireless Sensor Network for Health–Care Monitoring
103

5.1 Hardware Components
There are many chips or modules manufacturers’
following this standard, including Texas Instruments,
Maxstream, FreeScale, among others. In this work,
we select an OEM module from Maxstream Com-
pany, the XBee. This module has a 100 meters range
for outdoor and 30 meters indoor, with a 1 mW of
power in antenna, consuming 45 mA in transmission
and 50 mA in reception modes. The XBee module
uses the MC13193 transceiver chip working in the
2,4GHz frequency band and a MC9S08GB60 micro-
controller, both from Freescale. In addition, the mi-
crocontroller has 8-channel analog to digital converter
with 10 bits resolution and an UART interface (Digi
International, 2006).
The WPAN central device is a mobile phone
(Nokia 6620), which collects and processes the sen-
sors signals, transmitting them to a central monitoring
system through the mobile phone network using SMS
and MMS protocols. Due to the novelty of IEEE
802.15.4 technology, the mobile phone does not sup-
port this standard, reason why we implemented an
IEEE 802.15.4-to-Bluetooth bridge for integrate the
phone to the sensor network. The Nokia 6620 was
selected because it has Bluetooth interface and runs
Symbian operating system, which allows the devel-
opment of applications in C++ or Java programming
languages.
In addition, a cardiac pulse sensor was imple-
mented. Actually, we are developing others biolog-
ical sensors such as ECG and pulse oximeter.The
cardiac pulse sensor is implemented using a piezo-
electric transducer that obtains the blood pressure
pulse waveform across an artery. The SDT1-028KD
PVDF piezoelectric transducer from MSI (Measure-
ment Specialties, 2006) was selected.
The analog circuit for transducer signal condition-
ing consists basically of a differential charge amplifier
which uses three op-amps in the classic instrumenta-
tion amplifiers configuration. The differential topol-
ogy reduces line-noise pickup, which is a problem
with high-gain circuits. Besides, an active guard has
been used to compensate unbalances in the transducer
terminals and a shield around the transducer behaves
like a Faraday cage, connected to the active guard.
The next amplifiers and filters stages are implemented
as single ended devices. In the Figure 2 a simpli-
fied schematic of the charge amplifier is shown. The
small pulses of charges are integrated and converted
to differential voltages pulses at the output of the first
stage. The second stage is a differential–to–single–
ended amplifier. The gain of the differential stage is
given by the ratio between C1 and C2, where C2 cor-
Figure 2: Charge amplifier schematic for the PVDF trans-
ducer.
Figure 3: Photo of the sensor node and the smart phone used
as the central device.
responds to the equivalent capacitance of piezofilm
(Maxim Inc., 2002). The circuit has a good perfor-
mance, with an S/N ratio of approximately 40 dB.
Figure 3 is a photo of the designed sensor node. It
can be seen the Xbee OEM module, the analog signal
conditioning circuit for the PVDF transducer and the
smart phone used as the central device.
5.2 Software Modules
On the Nokia 6620, both Java and C language can be
used for applications development. While both lan-
guages are capable of connecting to the Bluetooth
stack and communicate via GPRS, SMS or MMS;
Java applications are halted if the user receives an in-
coming call or loads another Java application. Writ-
ing code in C language allows our program to con-
tinue capturing data from the sensor network in the
background regardless of the task the mobile phone is
doing on the foreground. The used development en-
vironment was the Carbide V1.0 with the Nokia Se-
ries 60 SDK 2nd Edition. This platform integrates
a phone simulator for debugging purpose. Compiled
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
104
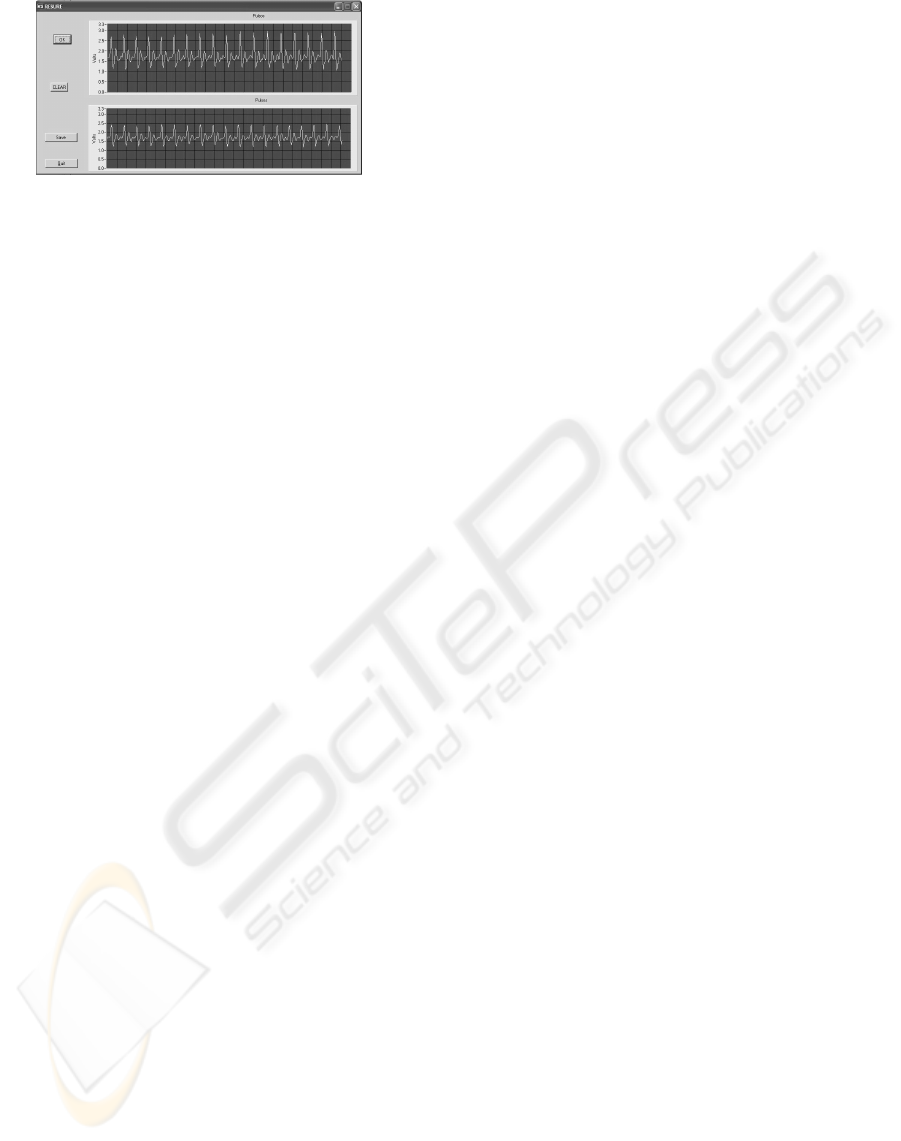
Figure 4: Measurements taken by two cardiac pulse sensors
located on two different positions of the neck.
code was packaged into a Symbian .SIS installation
file and downloaded to the phone via Bluetooth.
The Figure 4 shows some measurements taken by
two cardiac pulse sensors located on two different po-
sitions in the neck. The signals are displayed on the
screen of a test program developed using LabWin-
dows environment. It can be observed that the shapes
of the cardiac pulses are well defined and the sig-
nals have good signal–to–noise ratio. If analyzed by
a physician, these waveforms could give information
about the arteries’ state.
6 NETWORK PERFORMANCE
ANALYSIS
In order to validate the proposed network architecture
performance, we implement two cardiac pulse sen-
sors. From this test bench, we obtain some network
parameters and acquired two pressure signals simul-
taneously from two different positions of the body.
Following, some results are presented:
• Security: The 802.15.4 Default Security protocol
offers AES encryption with a 128-bit key. How-
ever, the use of this feature causes a packet over-
head reducing the available bandwidth. That’s
why, the AES encryption is disable in the carried
out experiments.
• Battery lifetime: With a 2400 mAh battery and a
transmitter consumption of 45 mA with duty cycle
of 100% we have a lifetime of 2400 mAh/45mA,
approximately 53 hours. The calculation assump-
tion of 100 % duty cycle is not realistic; it could
be a lot less in this kind of networks. The ques-
tion is how often do the sensors need to trans-
mit? To achieve best possible effective data rate
it is important to use the largest packet size pos-
sible. The Maxstream module can send up to
106 bytes per packet with a maximum 92 bytes
payload. Each sample has 10 bit resolution, this
means that 46 samples fit in each packet. The
sensor, with 500 Hz sampling rate, takes a sam-
ple every 2 ms (1/500 Hz). If the sensor does not
transmit until the packet is full (46 samples), the
sensor transmits every 46*2 ms = 92 ms. Trans-
mitting 106 bytes at 250 kbit/s takes 3.36 ms, to
wake up the transmitter from sleep mode takes 2
ms and to access the channel 10 ms. An ACK
frame of 11 bytes which takes 0.35 ms to be trans-
mitted. Summarizing, the radio activity time is 2
ms + 10 ms + 3.36 ms + 0.35 ms =15.71ms. Con-
sidering that the radio can sleep when it is not in
use and if no error occurs, the transmitter is in use
during 15.71ms per each 92 ms which gives a 17%
duty cycle. Beacon frames from the coordinator,
for time synchronization, is not take into account.
With the above considerations, the battery life-
time is approximately 2400mAh / (45mAh*0.17)
= 313.72 hours. This is an optimistic result; ac-
tual battery lifetime will likely be somewhat be-
low this. Also, note that sleep mode current is not
taken into account; it is approximately 50 uA and
his impact on the battery life will be minimal.
• Scalability: With a 500 sampling per second rate
and a 10 bit resolution, 5000 bits needs to be trans-
ferred each second. Each packet in the network
has 14 bytes overhead and 92 bytes payload. The
required data rate to transmit 5000 bits per second
is ((500/46)*106)*8 9.2 kbits/s; a very low data
rate considering the 250 kbits/s bandwidth avail-
able between each sensor and the PAN coordina-
tor. Theoretically, up to 25 nodes can be added
to the network, but this is not a true number be-
cause of the IEEE 802.15.4 medium access con-
trol mechanism.
From the above analysis we can conclude that the
IEEE 802.15.4 standard is appropriate for medical
WPAN sensor network.
7 CONCLUSIONS
In this work a wireless sensor network for medical ap-
plications is proposed based on IEEE 802.15.4 stan-
dard. To validate the proposal a prototype, composed
by two wireless blood pressure sensors, was build.
From the theoretical analysis and experimental
tests, we can conclude that the IEEE 802.15.4 stan-
dard is appropriate for medical WPAN sensor network
with respect to the following performance parameters:
battery lifetime, scalability and security.
Actually, we are working on the development of
other sensors, specifically an ECG and a oximeter
sensors, which will be added as nodes in the WPAN
sensors network. Also, we are working on a program
RESURE - Wireless Sensor Network for Health–Care Monitoring
105

for the mobile device that will analyze the different
signals in order to obtain useful information to be pre-
sented to the user.
REFERENCES
Digi International (2006). 802.15.4 Protocol-
Maxstream (version 1.xAx). Digi International,
www.maxstream.net.
IEEE Standard (2002). IEEE Standard for Infor-
mation technology - Telecommunications and in-
formation exchange between systems - Local and
metropolitan area networks - Specific requirements
Part 15.1: Wireless Medium Access Control (MAC)
and Physical Layer (PHY) Specifications for Wire-
less Personal Area Networks (WPANs). IEEE,
http://standards.ieee.org/.
IEEE Standard (2003). IEEE Standard for Infor-
mation technology - Telecommunications and in-
formation exchange between systems - Local and
metropolitan area networks - Specific requirements
Part 15.1: Wireless Medium Access Control (MAC)
and Physical Layer (PHY) Specifications for Wire-
less Personal Area Networks (WPANs). IEEE,
http://standards.ieee.org/.
Istepanian, R. et al. (2001). Advances in telemedicine using
mobile communications. Proceedings of the 23rd An-
nual EMBS International Conference,Istanbul,Turkey.
Karl, H. and Willig, A. (2005). Protocols and Architectures
for Wireless Sensor Networks. Wiley.
Maxim Inc. (2002). Amplifier provides signal con-
ditioning for piezofilm sensor. Maxim Inc.,
http://www.maxim.com/.
Measurement Specialties (2006). Sdt shielded piezo sensors
element with shielded cable. Technical report, MEA-
SUREMENT SPECIALTIES, www.meas-spec.com.
Rodr
´
ıguez, J. et al. (2005). Real-time classification of ECGs
on a PDA. IEEE Transactions on information technol-
ogy in Biomedicine, 9(1):23–34.
Shnayder, V. et al. (2005). Sensor networks for medi-
cal care. Division of Engineering and Applied Sci-
ences TR-08-05, Harvard University. Available at
http://www.eecs.harvard.edu/mdw/proj/codeblue.
Thraning, B. M. (2005). The Impact of ZigBee in a BioMed-
ical Environment. Agder University College.
WHO (2004). http://www.who.int/mediacentre/news/
releases/2004/pr60/es/.
Woodward, B. and Rasid, M. (2003). Wireless
telemedicine: The next step? Proc. of the 4th Annual
IEEE Conf. on Information Technology Applications
in Biomedicine.
ZigBee Alliance (2005). ZigBee Specification (Version 1.0).
ZigBee Alliance, www.zigbee.org.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
106
