
INSTRUMENTED SPLINT FOR THE DIAGNOSIS OF BRUXISM
Pilar Lafont Morgado, Andrés Díaz Lantada, Alexander Martínez Álvarez, Antonio Barrientos Cruz
Héctor Lorenzo-Yustos, Pedro Luis Castedo Cepeda, Roberto González Herranz
Julio Muñoz García and Javier Echavarri Otero
Universidad Politécnica de Madrid
C/ José Gutiérrez Abascal, nº 2. 28006 – Madrid, Spain
Keywords: Telemedicine, Electroactive Polymers (EAPs), Biomaterials, Bruxism, Temporomandibular Joint.
Abstract: Bruxism is a health problem consisting in grinding or tightly clenching the upper and lower teeth. Both the
grinding and sliding lead to wear of the teeth and produce a noise during the night that is sufficiently loud to
disturb the sleep of anyone sharing the bedroom. The tension produced causes problems in the muscles,
tissues and other structures surrounding the jaw, ear pain, headaches, lesions to the teeth and disorders in the
jaw joints.
For an early, rapid, effective and economical diagnosis of bruxism, we propose the use of instrumented
splints to detect and record the intensity and duration of interdental pressure episodes. This paper sets out
the design, manufacture and testing of an instrumented splint for diagnosing the signs of bruxism.
The system stands out for its use of piezoelectric polymeric sensors which, because of their reduced
thickness, do not cause any alteration to the patient’s bite. It lets a quantitative assessment of intraoral
pressure be made and bruxism behaviour be diagnosed at an early stage, so as to being able to programme
corrective actions before irreversible dental wear appears. The first “in vitro” simulations and “in vivo”
trials performed served to demonstrate the feasibility of the system in accordance with the initial objectives.
1 BRUXISM:
CHARACTERISTICS AND
PREVALENCE
Bruxism is a health problem consisting in grinding
or tightly clenching the upper and lower teeth. Both
the grinding and sliding lead to wear of the teeth and
produce a noise during the night that is sufficiently
loud to disturb the sleep of anyone sharing the
bedroom. The tension produced causes problems in
the muscles, tissues and other structures surrounding
the jaw, ear pain, headaches, lesions to the teeth and
disorders in the jaw joints. All these symptoms as a
whole are usually described as temporomandibular
joint problems (TMJ) or also as Craniomandibular
Disfuntion Pain Syndrome.
The phenomenon was introduced to dental
literature as bruxomania by Marie and Pietkiewkz in
1907. They described the habit of grinding the teeth.
The term bruxism was introduced by Frohman in
1931. In 1936 Miller proposed using the term
bruxomania for daytime grinding and bruxism for
night time grinding. The terms traumatic neuralgia,
the Karolyi effect and occlusive habit neurosis have
all been used to refer to some form of teeth grinding
or clenching.
According to a study by the Canadian Sleep
Society nocturnal bruxism affects 8% of the adult
population and 14% of the child population. A
decrease in the population affected can be
appreciated with age, attaining 3% for people over
60. However, for researchers like Melis and Granada
prevalence is around 25%.
As to differences by sex there is no general
agreement since there are publications that describe
a greater bruxism activity in men (Quirch, Ozaki),
others in women (Barreto, De los Santos) while
others deem it to be an insignificant factor (Hayden,
Kononean).
To summarise Nishigawa’s study on the bite
force produced during bruxism episodes, this can
frequently reach 1100 N exceeding the maximal
voluntary bite force. Pressures reached on the teeth
surface can reach 40 MPa, high enough to cause
high levels of wear and even breakages.
As to the duration of bruxism episodes, an
average time of around 7 seconds has been found
and when developing sensors it is necessary to
216
Lafont Morgado P., Díaz Lantada A., Martínez Álvarez A., Barrientos Cruz A., Lorenzo-Yustos H., Luis Castedo Cepeda P., González Herranz R., Muñoz
García J. and Echavarri Otero J. (2008).
INSTRUMENTED SPLINT FOR THE DIAGNOSIS OF BRUXISM.
In Proceedings of the First International Conference on Biomedical Electronics and Devices, pages 216-221
DOI: 10.5220/0001051802160221
Copyright
c
SciTePress

distinguish bruxism episodes from mioclonus or
rapid contractions (< 0.5 s) of the jaw muscles.
However, it is important to point out that
everybody subconsciously clenches their teeth at
some time of the day and this could be considered as
bruxism activity. The term bruxism is only used
though when the duration and intensity of this
activity has a bearing on dental wear and the
appearance of TMJ problems.
One of the main problems associated with the
traditional diagnosis of bruxism is that it is
frequently made when the teeth are already highly
worn and the prognosis of the illness is more severe.
Bruxism activity can also be recorded by an EEG
(electroencephalogram) as well as by EMG
(electromiography) and S-EMG (surface
electromiography). In many cases video-cameras are
used in the study to distinguish the bruxism episodes
of the mioclonus or rapid contractions (< 0.5 s) of
the jaw muscles.
However, in order to be able to make an earlier,
more rapid, more effective and economical diagnosis
of bruxism, the research team that have written this
paper propose using instrumented splints for
detecting and recording the intensity and duration
of interdental pressure episodes. Explained below
are the design, manufacture and trials of an
instrumented splint for the diagnosis of bruxism
activity. It has been developed by researchers at
Universidad Politécnica de Madrid in collaboration
with Ibex Estética Dental S.L..
2 DESIGN OF THE DEVICE FOR
DIAGNOSING BRUXISM
USING ELECTROACTIVE
POLYMERS AS SENSORS
Traditionally discharge splints or protection devices
are used to treat bruxism and prevent the associated
dental wear. As a diagnostic device we propose
introducing pressure sensors into a splint so that
patients’ bite episodes can be recorded and the
extent of their pathology be assessed. Piezoelectric
polymers are used as pressure sensors for the
reasons set out below.
Piezoelectric Electroactive Polymers as
Pressure Transducers: PVDF (Polyvinylidene
Fluoride)
Piezoelectricity was discovered in 1880 by
Pierre and Paul-Jaques Curie, who observed that
when certain crystals were compressed, like quartz
or tourmaline, depending on certain directions they
produced a voltage between zones on their surface.
When force was applied the relative positions of the
crystal molecules changed producing an internal
displacement of charges which was the cause of this
voltage.
These crystals also underwent the inverse effect
since they became deformed when a voltage
difference was applied. This property is found in
materials lacking a centre of symmetry and the
phenomenon is called ferroelectricity when a non-
conductor crystal or dielectric material exhibits
spontaneous electric polarisation.
Polyvinylidene fluoride or PVDF -(CH
2
-CF
2
)-
n
and its co-polymers such as poly(vinilydenefluoride-
trifluoroethylene) or P(VDF-TrFE), are the polymers
of this kind with the largest number of industrial
applications. They posses partial crystalinity with an
inactive amorphous phase and an elastic modulus
close to between 1 and 10 GPa. Their use as
actuators is limited by the need to apply high electric
fields (around 20 V/μm for a 3% deformation), but
their use as pressure sensors is taking the place of
traditionally used piezoelectric ceramic materials.
Figure 1: Metallized PVDF sheets. Piezotech S.A..
The use of this type of sensor was considered
because of its reduced thickness, which does not
cause any alteration to the patient’s bite and because
of its greater resistance and sensitivity compared to
ceramic piezoelectrics. To make the sensors, we
took PVDF 40 μm thick sheets from Piezotech S.A.
with Au-Pt coated electrodes. These sheets were cut,
joined to the connecting wires and suitably
encapsulated to protect them and be inserted into the
splint (see manufacturing process). The sensors
obtained are shown below, together with the
behaviour model allowing them to be simulated and
the first results obtained in the trials carried out.
INSTRUMENTED SPLINT FOR THE DIAGNOSIS OF BRUXISM
217
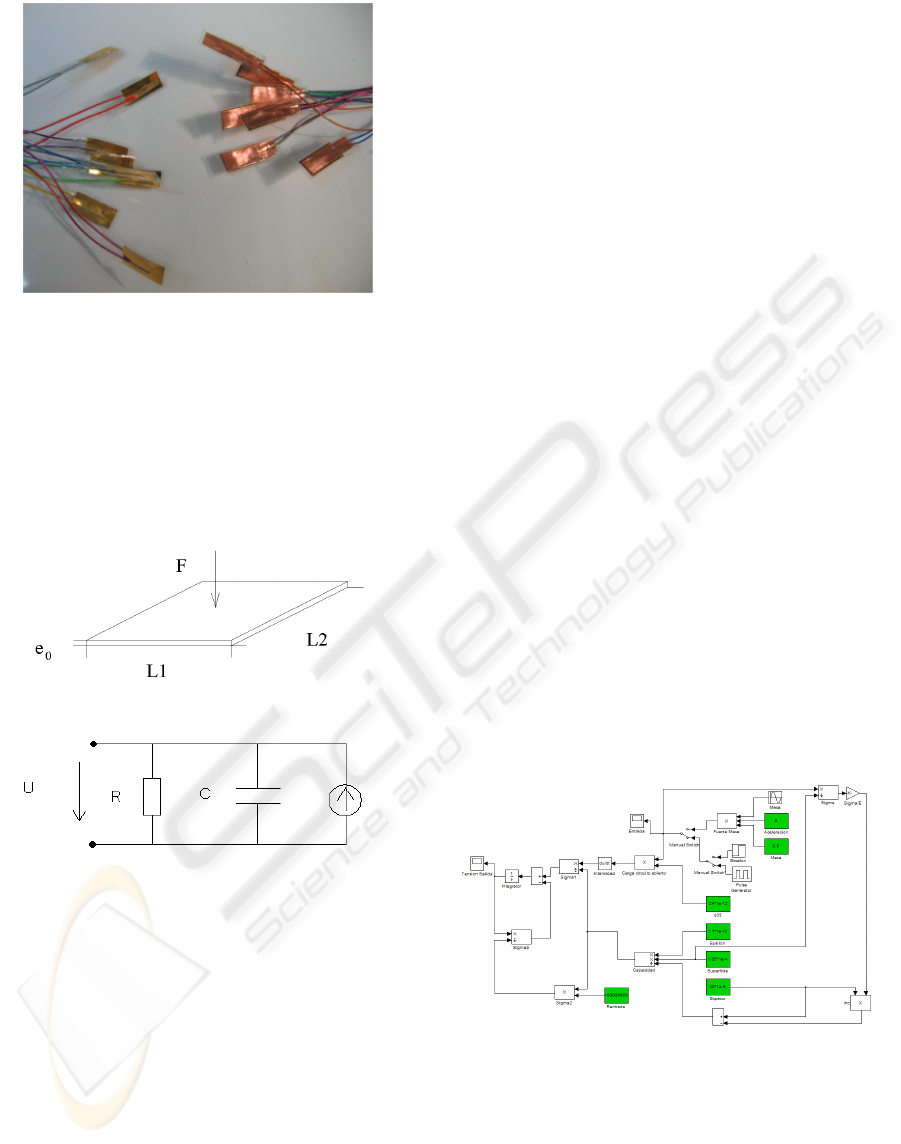
Figure 2: Piezoelectric sensors manufactured. Product
Development Laboratory. Universidad Politécnica de
Madrid.
Figure 3: a) shows the piezoelectric sensor
layout. The charge displacement produced when a
force is applied to the piezoelectric sensor can be
represented using the equivalent electric circuit
depicted in Figure 3 b).
a)
b)
Figure 3: a) Piezoelectric Sensor. b) Electrical behaviour
circuit diagram of the piezoelectric sensor.
Force F on the sensor acts as a generator of
intensity powering a C capacity condenser. Ec (1).
C = C(F) = ε · (L1·L2) / e (1)
Where:
ε.- The dielectric constant of the sensor.
L1·L2.- The effective area of the sensor.
e.- The thickness of the sensor.
The thickness of the sensor, e, depends on the
initial thickness, e
0
, on the pressure applied, σ = F /
(L1·L2), and the Young modulus of the material, E,
using the following expression Eq. (2):
e = e
0
· (1 – σ / E) (2)
Current intensity, I, generated by applying force
F, depends on the transversal piezoelectric
coefficient of sensor d33 according to Eq. (3).
Q = d33 · F Æ I = dQ / dt = d33 · dF / dt (3)
When the sensor is connected to an external
circuit, as is shown in Figure 3 b), it discharges in
accordance with the equivalent R resistance of this
external circuit (the oscilloscope input resistance in
the first trials carried out). The intensity is given by
Eq. (4).
I = d33 · dF / dt = U / R + C · dU / dt (4)
With the above equations and previous data a
model was made in Simulink which permits a rapid
assessment of the effect of modifying the
parameters. The model and the results of the
simulation are shown below, together with the first
real trials carried out with the piezoelectric sensor
connected directly to the oscilloscope when it was
subjected to levels of pressure.
For the first simulations and trials with the
sensors manufactured (Figures 5, 6 and 7) we have:
Piezoelectric coefficient (when applying forces
perpendicular to the sensor plane).- d33 = 24 pC/N
Dielectric constant.- ε = 1,1 · 10
-10
F/m;
Elasticity modulus of the PVDF.- E = 2000
MPa
Effective sensor area.- L · L2 = 4 · 10
-4
m
2
Sensor thickness.- 40 μm
Oscilloscope input resistance.- R = 10 MΩ
Figure 4: Simulink model for simulating piezoelectric
polymer behaviour.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
218
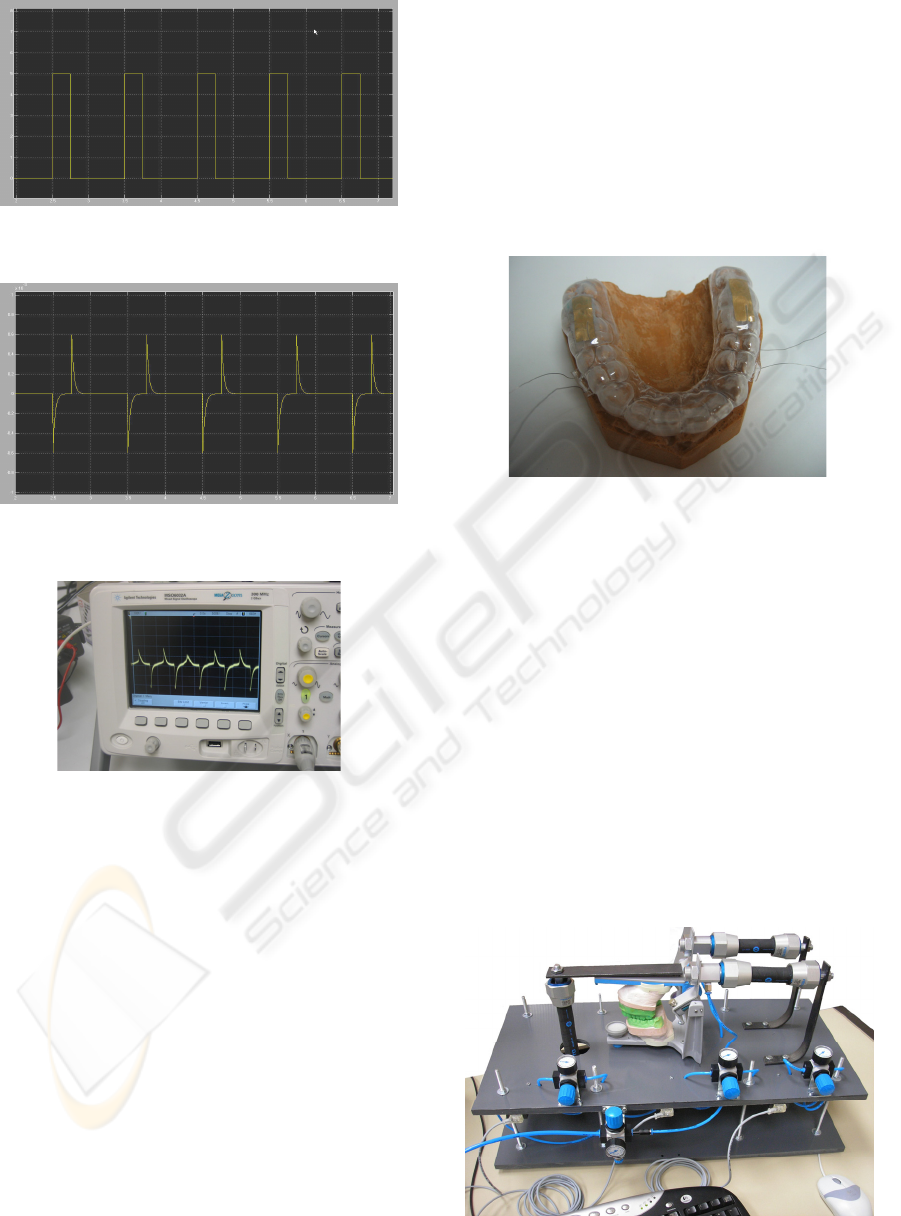
Figure 5: Simulation of levels of pressure as simulator
input.
Figure 6: Output obtained (voltage) according to the
simulation.
Figure 7: First trials: The oscilloscope shows sensor output
voltage on applying levels of pressure as input.
3 MANUFACTURING THE
DEVICE FOR DIAGNOSING
BRUXISM
To obtain the instrumented splint some of the steps
followed in the manufacture of thermoformed splints
are followed. A model of the patient’s teeth needs to
be made, usually by shape copying. This model is
put into a vacuum thermoforming machine in which
a polymer wafer heated to a temperature higher than
its softening temperature covers the model and
reproduces the teeth geometry when a vacuum is
applied on cooling.
The piezoelectric sensors are then placed on
this first thermoformed layer and the operation is
repeated with a second polymer wafer, whereupon
the sensors become embedded within the two layers.
It is important to control the thermoforming
temperature since piezoelectric polymers used as
sensors begin to lose their electromechanical
coupling at temperatures above 80 ºC.
Finally the excess parts are trimmed off and the
splint is subjected to an adjustment and polishing
process to adapt it to the patient. In this way a splint
is obtained like the one shown below in Figure 8,
which enables interdental pressures to be detected
for the purpose of diagnosing bruxism.
Figure 8: Splint with piezoelectric sensors for diagnosing
bruxism.
4 FIRST “IN VITRO” AND “IN
VIVO” TRIALS
4.1 “In Vitro” Trials
To simulate biting in “in vitro” trials, a
pneumatically operated system was constructed in
which moulds could be placed that reproduce
patients’ teeth, and on which the instrumented
splints could be placed. The pneumatic system’s
actuators allow both perpendicular and transversal
bruxism to be simulated with operating pressures of
up to 6 bar in the pneumatic actuators providing bite
forces of 750 N. This is shown in Figure 9.
Figure 9: Bruxism simulator with pneumatic operation for
the “in vitro” trials.
INSTRUMENTED SPLINT FOR THE DIAGNOSIS OF BRUXISM
219
To carry out the “in vitro” trials moulds of the
teeth of 3 patients taking part in the research were
done. Resin reproductions of these teeth were made
as a support for manufacturing the splints, which
could also be placed in the bite simulator to
artificially operate these instrumented splints.
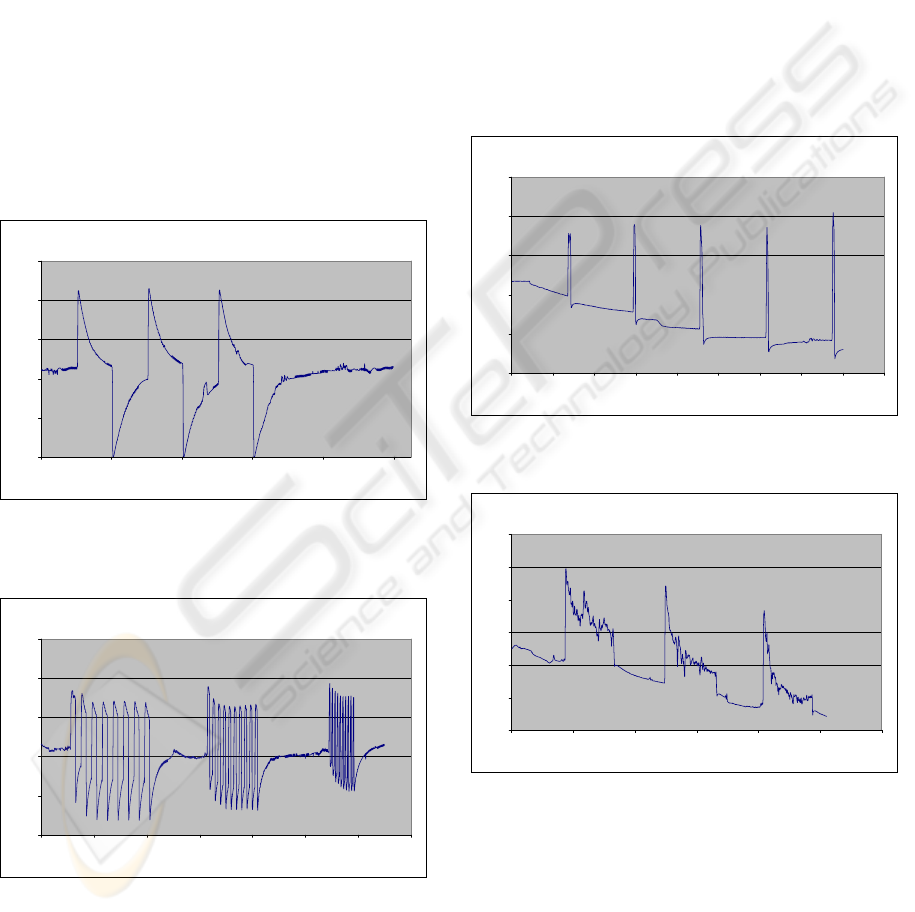
Figures 10 and 11 show the response of the
instrumented splints on being placed in the bite
simulator and subjected to pneumatic operation. The
connectors coming from the splint attached to the
sensors were connected to a charge amplifier and an
analogical-digital converter. This system’s output
was recorded using a data acquisition card
commercially available known as “Measurement
Computing USB 1208-FS”.
The response to prolonged 10-second bites was
studied for with 10-second relaxation between bites.
The sensor response capacity and that of the A/D
amplifier-converter system were also assessed, with
successive bite episodes of different frecuencies.
Response vs. Time
0
0,5
1
1,5
2
2,5
0 20406080100
s
V
Figure 10: Simulation of 3 successive bites: Operation at 1
bar ≈ 150 N of bite during 10 s and relaxation during
another 10 s.
Response vs. Time
0
0,5
1
1,5
2
2,5
0 20 40 60 80 100 120 140
S
V
Figure 11: Simulation of successive bite episodes
(operation at 1 bar ≈ 150 N of bite): First episode.- 8 bites
with 2 s clenching and relaxation time. Second episode.-
10 bites with 1 s clenching and relaxation time. Third
episode.- 10 bites with 0.2 s clenching and relaxation time.
After a positive assessment of the properties of
the intrabucal pressure detection system and signal
adjustment, processing and recording, “in vivo”
trials were carried out, the results of which are
presented below.
4.2 “In Vivo” Trials
The splints used for the previous trials were used
again with the 3 patients taking part in the research
for the first “in vivo” trials. They enabled the
response of splints in actual mouths to be assessed
and their resistance and duration to be tested, as well
as their water-tightness to avoid any deterioration of
the sensors. The responses recorded both of sudden
and prolonged bites are shown in Figures 12 and 13.
Response vs Time
0
0,5
1
1,5
2
2,5
0 102030405060708090
s
V
Figure 12: Output voltage in response to bite impacts
every 15 seconds.
Response vs Time
0
0,5
1
1,5
2
2,5
3
0 20 40 60 80 100 120
s
V
Figure 13: Output voltage with prolonged bites every 15
seconds and 15 seconds of relaxation.
The results of the trials carried out with the
patients’ splints show that it is possible to detect
bruxism episodes of different intensities and
duration which, combined with the ability to record
and store the data, converts the system into a
“Holter” for diagnosing bruxism and evaluating
intrabucal pressures.
BIODEVICES 2008 - International Conference on Biomedical Electronics and Devices
220

5 RESULTS ASSESSMENT AND
FUTURE ACTIONS
The complete development of a splint to assess
intrabucal pressure and diagnose bruxism and other
occlusive pathologies has been presented. The
system stands out for its use of polymeric
piezoelectric sensors which, on account of their
reduced size, do not produce any alterations to the
patient’s bite. The design process, modelling,
simulation, manufacture and first trials have been
described in detail, both in the pneumatic simulator
and in 3 patients taking part in the research.
Currently, additional trials are being carried out
with a total of 15 patients, with similar results to
those shown in Figure 7. The electronics used
(analogical-digital converter module and charge
amplifier) need to be improved in order to optimise
system response. The results of the “in vivo” trials
are being compared with the behaviour models set
out in order to improve control over the factors
influencing the diagnosis of bruxism using
instrumented splints.
However, what should be highlighted is the
possibility to obtain a device that will enable
intrabucal pressure to be quantitatively assessed and
bruxism behaviour to be diagnosed at an early stage,
so that corrective actions can be programmed before
the appearance of irreversible dental wear. The first
“in vitro” simulations and “in vivo” trials carried out
serve to demonstrate the feasibility of the system in
accordance with the initial objectives.
This work was partial result of “FEMAB
Project: Micro-instrumented Anti-bruxism Splint”
subsidised by the Spanish Ministry of Education and
Science with Reference PROFIT (Promotion of
Technical Research) CIT-020400-2005-17. It has
been carried out in collaboration between
Universidad Politécnica de Madrid and Ibex Estética
Dental S.L..
REFERENCES
S. Ashley, Artificial Muscles. Scientific American 2003.
Y. Bar-Cohen, Electroactive Polymer (EAP) Actuators as
Artificial Muscles. SPIE Press, Second Edition.
Washington 2004.
Y. Bar-Cohen, et al. Characterization of the
Electromechanical Properties of EAP Materials. Jet
Propulsion Laboratory (JPL)/Caltech. SPIE. Newport,
CA, 2001.
P. Dubois, et al., Microactuators based on ion-implanted
dielectric electroactive polymer membranes (EAP).
Microsystems for Space Technologies Laboratory,
Lausanne. IEEE Transducers 2005.
M. Hafez, Course on Polymer Based Actuators as
Artificial Muscles. FSRM (Swiss Foundation for
Research in Microtechnology). Zurich 2006.
G. Lavigne et al., Bruxism: Epidemiology, diagnosis,
patho-physiology and pharmacology. Advances in
pain research and treatment 1995.
G. Lavigne et al., Neurobiological mechanisms involved in
sleep bruxism. Faculté de Médecine, Université de
Montréal 2003.
G. Lavigne et al., Sleep bruxism: validity of clinical
research diagnostic criteria in a controlled
polysomnographic study. Journal of Dental Research
1996.
Measurement Specialties, Inc., Piezo Film Sensors
Technical Manual. Sensor Products Division 1999.
K. Nishigawa, et al., Quantitative study of bite force
during sleep associated bruxism. Journal of Oral
Rehabilitation 2001.
D. Cosme, et al., Bruxism and voluntary maximal bite
force in young dentate adults. The International
Journal of Prosthodontics 2005.
K. Baba, Bruxism force detection by a piezoelectric film-
based recording device in sleeping humans. Journal of
Orofacial Pain 2003.
INSTRUMENTED SPLINT FOR THE DIAGNOSIS OF BRUXISM
221
