
OPHTHALMOLOGIC ELECTRONIC HEALTH RECORDS
SYSTEM USING HL7/CDA AND DICOM - TELEOFTALWEB
Isabel de la Torre, Roberto Hornero, Miguel López
Department of Signal Theory and Communications, University of Valladolid, Campus Miguel Delibes, Valladolid, Spain
María Isabel López
University Institute of Applied Ophthalmobiology (IOBA), University of Valladolid
Edificio Ciencias de la Salud, Valladolid, Spain
Keywords: Clinical Document Architecture (CDA), Digital Imaging and Communications in Medicine (DICOM),
Electronic Health Record (EHR), Extensible Markup Language (XML), Health Level 7 (HL7), Java.
Abstract: Electronic Health Record (EHR) refers to the complete set of information that resides in electronic form and
is related to the past, present and future health status. Health Level Seven (HL7) and Digital Imaging and
Communications in Medicine (DICOM) are intensively influencing EHRs standardization. This article
describes the development, experience and evaluation of a web-based application, TeleOftalWeb 3.2, to
store and exchange EHRs in ophthalmology. We apply HL7 Clinical Document Architecture (CDA) and
DICOM standards. EHRs and fundus photographs are stored in a database Oracle 10g. The application has
been built on Java Servlet and Java Server Pages (JSP) technologies. For security, all data transmissions
were carried over encrypted Internet connections such as Secure Sockets Layer (SSL) and HyperText
Transfer Protocol over SSL (HTTPS). The application verifies the standards related to privacy and
confidentiality. TeleOftalWeb 3.2 has been tested by ophthalmologists from the University Institute of
Applied Ophthalmobiology (IOBA), Spain. Nowadays, more than one thousand health records have been
included to verify the web application usability.
1 INTRODUCTION
Electronic Health Records (EHRs) are a secure, real-
time, point-of-care and patient-centric information
resource for physicians (HIMSS, 2003). EHRs
include information such as observations, laboratory
tests, diagnostic imaging reports, treatments,
therapies, drugs administered, patient identifying
information, legal permissions and allergies.
Currently, this information is stored in all kinds of
proprietary formats through a multitude of medical
information systems available on the market
(Eichelberg et al., 2005). EHR systems can
incorporate clinically useful features such as
electronic alerts, guideline reminders and automatic
monitoring of quality of care indicators (Bostrom et
al., 2006). The primary purpose of EHR is the
support of continuing, efficient and quality
integrated health care. Amongst EHRs benefits are
their universal access, coding efficiency and
efficacy, easier and quicker navigation through the
patient record (Smith and Newell, 2002). There are
several barriers to their adoption such as training,
costs, complexity and lack of a national standard for
interoperability (Gans et al., 2006).
Ophthalmology is an ideal specialty for testing
EHRs due to the use of images and objective
measures during diagnosis of eye diseases. It is an
ideal speciality for telemedicine. EHRs systems can
assist ophthalmologists in improving the quality of
care being provided as well as assist the
ophthalmologists in building solid relationships with
their patients. Physicians who have shared EHRs
available yet fail to consult them before beginning
treatment could face increasing liability in the future
(Yogesan et al., 1998).
International and European institutions are
working in EHR standardization such as the
International Standards Organization Health
Informatics Standards Technical Committee
99
de la Torre I., Hornero R., López M. and López M. (2009).
OPHTHALMOLOGIC ELECTRONIC HEALTH RECORDS SYSTEM USING HL7/CDA AND DICOM - TELEOFTALWEB.
In Proceedings of the International Conference on Health Informatics, pages 99-104
DOI: 10.5220/0001120500990104
Copyright
c
SciTePress

(ISO/TC) 215, European Committee for
Standardization Technical Committee (CEN/TC)
251, Health Level Seven (HL7), Extensible Markup
Language (XML), Digital Imaging and
Communication in Medicine (DICOM) and others
(Bott, 2004). The development of HL7 and DICOM
standards has also been of great benefit in the
telemedicine services and applications.
HL7 standard is used for many different medical
environments. It is a not-for-profit organization
involved in development of international healthcare
standards. HL7 Document is intended to be the basic
unit of a document-oriented EPR. The patient
medical record is represented as a collection of
documents. HL7 Clinical Document Architecture
(CDA) is a XML-based document markup standard
that specifies the structure and semantics of EHR for
the purpose of exchange. Clinical Document
Architecture – Release One (CDA–R1), became an
American National Standards Institute (ANSI)–
approved HL7 Standard in November 2000,
representing the first specification derived from the
HL7 Reference Information Model (RIM). CDA –
Release Two (CDA–R2), became an ANSI-
approved HL7 Standard in May 2005 (Dolin et al.
2006). CDA standard provides an exchange model
for clinical documents. Many CDA documents
comprise an individual EHR.
DICOM is a cooperative standard. It was
developed from 1990 to 1996, mainly by the
American College of Radiology (ACR) and National
Electrical Manufacturers Association (NEMA)
committee in the United States, with contributions
from European standardization organizations, the
Japanese Industry Radiology Apparatus (JIRA), the
Institute of Electrical and Electronics Engineers
(IEEE), HL7 and ANSI as well as from European
manufacturers and societies. This standard allows
the exchange of medical images and related
information between systems from different
manufacturers.
EHRs have a great potential to improve
safety,
quality and efficiency in medicine. EHRs systems
often involve many institutions. Most previous
studies addressing this issue have been done in
primary care (Lo et al., 2007). In our application,
EHRs are shared between ophthalmologists,
endocrinologists, and primary care physicians.
We reviewed articles about EHR systems in
different specialities such as pediatric (Ginsburg,
2007), emergency departments (Amouh et al.,
2007), ophthalmology (Chew et al., 1998) and
oncology (James et al., 2001). In these systems,
HER standardization applying HL7/CDA and
DICOM was not presented.
We have designed, developed and evaluated a
web-based application to store and exchange EHRs
in ophthalmology, TeleOftalWeb 3.2. We apply
HL7/CDA and DICOM standards. The application
has been built on Java Servlet and Java Server Pages
(JSP) technologies. EHRs and fundus photographs
are stored in Oracle 10 g database. Its architecture is
triple-layered. The application server is Tomcat
5.5.9. The application is platform-independent
thanks to using Extensible Markup Language
(XML) and Java technologies. For security, all data
transmissions were carried over encrypted Internet
connections such as Secure Sockets Layer (SSL) and
HyperText Transfer Protocol over SSL (HTTPS).
The application verifies the standards related to
privacy and confidentiality. It has been tested by
ophthalmologists from the University Institute of
Applied Ophthalmobiology (IOBA), Spain.
Currently, more than one thousand health records
have been included.
2 METHODS
Firstly, we describe the application data modeling in
Oracle 10g database. Then, we show the application
architecture.
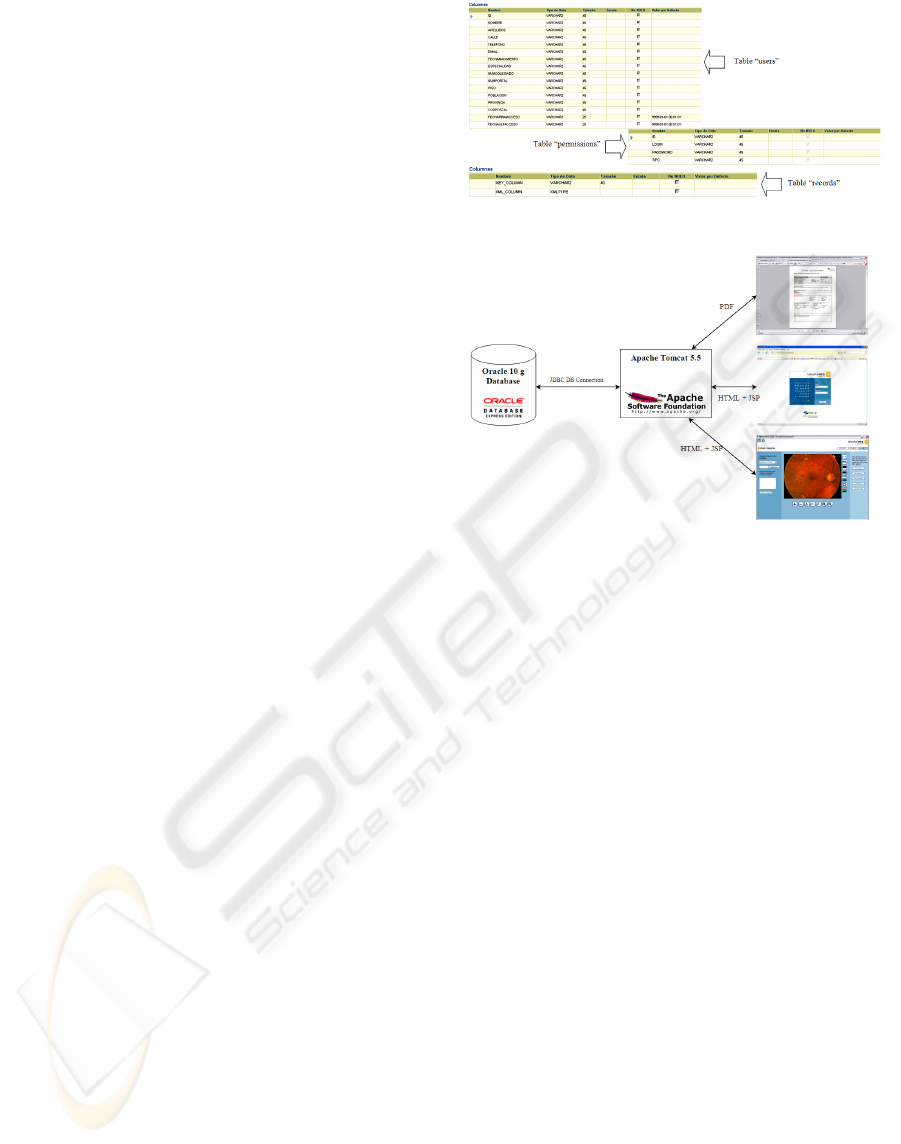
2.1 Data Modeling
In Oracle 10g database, we stored all the user data
and access information to the web application. It has
three tables: “users”, “permissions” and “records”.
The table “users” contains personal user data. The
user identification, user name, password, and user
type appear in table “permissions”.
EHRs are stored in Oracle 10g database
according to the ANSI/HL7 CDA R2.0-2005
template. The data modeling in the Oracle database
is shown in Figure 1.
Oracle 10g introduced a new datatype,
XMLType, to facilitate native handling of XML
data in the database. It supports comprehensive
models (i.e., structured, unstructured and binary
XML storage models) to server diverse XML use
cases with different requirements. For table
“records” (see Figure 1), we use this datatype.
XMLType is stored in Large Objects (LOBs). LOB
storage maintains content accuracy to the original
XML (whitespaces and all). When we create an
XMLType column without any XML schema
specification, a hidden CLOB column is
HEALTHINF 2009 - International Conference on Health Informatics
100
automatically created to store the XML data. The
XMLType column itself becomes a virtual column
over this hidden CLOB column. It is not possible to
directly access the CLOB column.
Oracle XML database provides efficient support of
SQL/XML XMLTable function and its COLUMNS
clause for mapping XML data into relational views.
By taking advantage of XQuery rewrite technology,
storage models, indexing schemes, downstream
processing on a relational view created with
XMLTable function can approach pure-relational-
performance (Oracle, 2008).
2.2 Application Architecture
TeleOftalWeb 3.2 architecture is a triple-layered.
Oracle 10g is used as database server and Apache
Tomcat 5.5 as application server. Figure 2 shows the
application architecture. Oracle 10g provides high-
performance, native XML storage and retrieval
technology.
We employ an Oracle Java Database Connectivity
(JDBC) driver to connect to the database instance. A
free open-source application server to process the
requests is used. The web-based system was built on
Java Servlet and JSP technologies, which enables
rapid development of web-based applications. In
Oracle database, we stored all the user data, access
information to the web application and records with
fundus photographs.
The development environment was NetBeans
IDE 4.1 of Sun Microsystems. The application is
platform-independent thanks to using XML and Java
Technologies. Java was the basis application
programming language. XML is an open standard
that provides a unified model for data, content and
metadata. It is being used to manage mission critical
information.
We included all tools and Application
Programming Interface (API) as Javascript, JSP,
Java Servlets and JDBC. The evolution of Java
Technology brings more features to the Java
development tools. This facilitates the creation of
telemedicine applications and reduces the time of
developing programs (Fedyukin et al., 2002). XML
technology is employed to store and exchange
EHRs. Some XML advantages are: easily readable,
self-describing and interoperable.
Figure 1: Data Modeling.
Figure 1: Application Architecture with Oracle 10g.
Figure 2: Architecture Application with Oracle 10g.
CDA Release 2 model is richly expressive,
enabling the formal representation of clinical
statements (such as observations, medication
administrations and adverse events) such that they
can be interpreted and acted upon by a computer
(Dolin et al., 2006).
As it was indicated in the introduction, CDA
documents are encoded in XML. The CDA is only
the first example of HL7's commitment to the
advancement of XML-based e-healthcare
technologies within the clinical, patient care domain.
The CDA specification prescribes XML markup for
CDA Documents: CDA instances must be validated
against the CDA Schema and may be subject to
additional validation. The document can be sent
inside or outside a HL7 message. CDA also supports
the semantically interoperable exchange of complex
medical information between healthcare applications
by virtue of its adherence to the HL7 V3
development methodology (Chronaki et al., 2002).
CDA does not specify the creation or management
of documents, only their exchange mark-up.
The XML-based architecture described in the
CDA v2.0 standard has been used to define the
health information format. Thanks to the use of
XML-based technologies and HL7 specifications,
our application fulfils the EHR standards. Its
development methodology is a continuously
evolving process that seeks to carry out
OPHTHALMOLOGIC ELECTRONIC HEALTH RECORDS SYSTEM USING HL7/CDA AND DICOM -
TELEOFTALWEB
101

specifications that facilitate interoperability between
healthcare systems.
3 RESULTS
We present the two application modules: manager
and user. Then, we describe the experience of
introducing diabetic patient’s health records from a
screening program of diabetic retinopathy in a rural
area of Spain (Hornero et al., 2003).
3.1 Manager Module
The manager can access the web platform with any
browser. Login and password have to be introduced
by users. The two user roles are: manager and user.
Application manager allows to:
Create new users.
Show user information.
Erase users.
Modify physician’s information.
Show user statistics.
Show the user patient records.
Search users by different criteria such as
surname, identification number, type of user,
and member number.
3.2 User Module
The authorized physicians can access to this module.
They have their login and password. They can do
the following actions:
Create new records (see Figure 3). They have
to introduce the necessary data: patient
affiliation information, patient precedents,
medical exploration and diagnostic.
Erase records and revisions.
Create new revisions in a record.
Search different EHRs and revisions,
Add new images in different records.
Physicians can add new images in an EHR.
These may be in different formats such as
DICOM, Joint Photographic Experts Group
(JPEG), Graphics Interchange Format (GIF),
DIB file format (BMP), Tagged Image File
Format (TIFF) amongst others.
Search images according to different criteria:
image identification number, surnames, image
creation and comments.
Figure 3: Exploration in a new EHR.
Figure 4: DICOM fundus photograph.
Edit and erase images. The images editor (see
Figure 4) shows images and allows us to
change their shape and colour, zoom in or
zoom out. It supports image editing of
brightness and contrast. Other editor functions
are: RGB (Red, Green, Blue) scale, add and
delete text, and arrows. It supports all type of
images (DICOM, JPEG, GIF, etc.).
Print EHRs in Portable Document Format
(PDF). We employ Extensible Stylesheet
Language Formatting Objects (XSL-FO) to
format XML data. XSL-FO is a complete
XML vocabulary for laying out text on a page.
An XSL-FO document is a well-formed XML
document that uses this vocabulary. EHR
output format is a PDF. First, the XML must
be fed to an XSLT processor with an
appropriate stylesheet in order to produce
another XML document which uses the XSL-
FO namespace. It is intended for an XSL-FO
formatter. The second stage is to feed the
output of the first stage to the XSL-FO
formatter that can produce a printable
document styled for visual presentation
(Pawson, 2002).
HEALTHINF 2009 - International Conference on Health Informatics
102
3.3 Practice Case
TeleOftalWeb 3.2 has been tested by physicians
from the University Institute of Applied
Ophthalmobiology (IOBA), Spain. Nowadays, more
than one thousand health records were introduced.
All the patients were diabetic and they participated
in a telemedicine program for diabetic retinopathy
screening in a rural area of Spain (Hornero et al.,
2003). Diabetic retinopathy is the most common
diabetic eye disease and a leading cause of blindness
in adults. It is caused by changes in the blood
vessels of the retina (National Eye Institute, 2008).
Our application allows to store and exchange all the
records and fundus photographs. Physicians used the
application with different web browsers to store and
exchange the EHRs. In each record there are the
following parts: anamnesis, exploration, diagnosis
and treatment. The EHR is associated with the
fundus photographs in all type of digital formats.
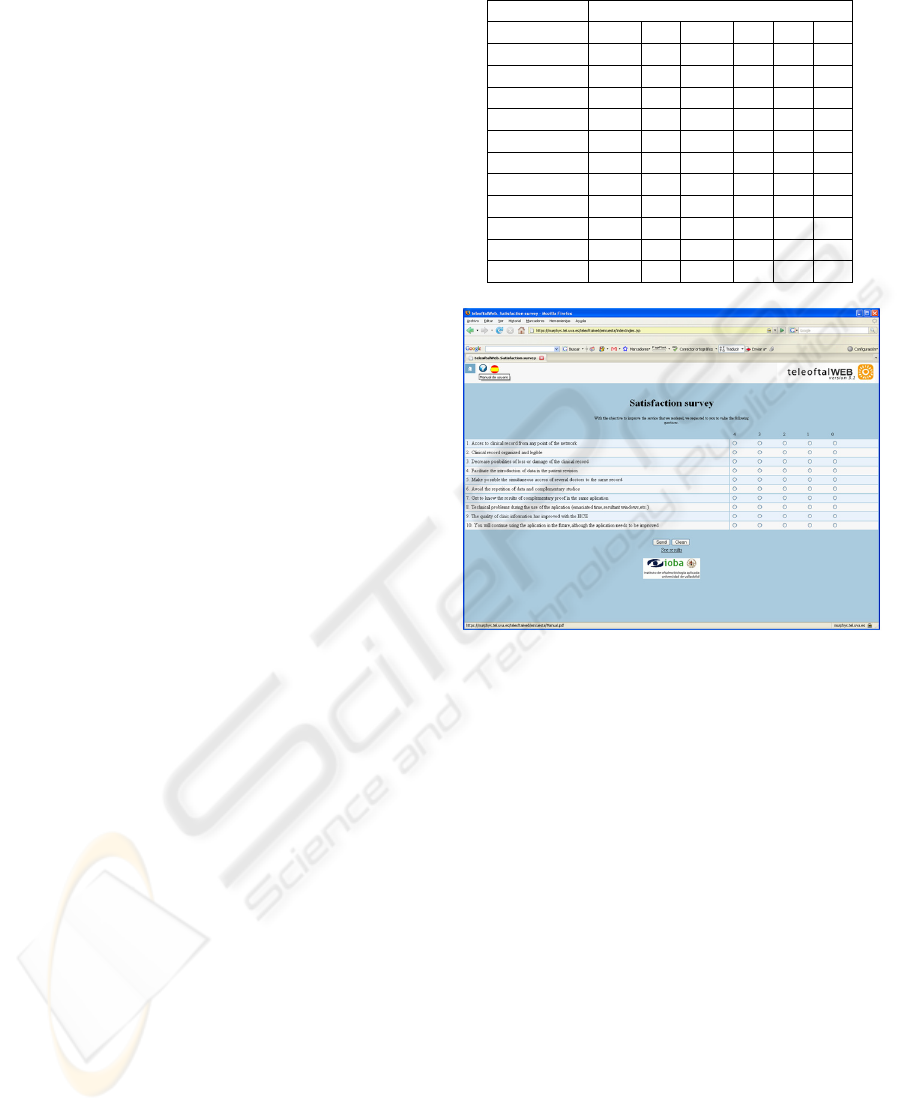
A survey with ten questions about the application
usability was done (see Figure 5). We used System
Usability Scale (SUS) to make the questionnaires. It
is a Likert scale. SUS has proved to be a valuable
evaluation tool, being robust and, reliable. It
correlates well with other subjectives measures of
usability (Brooke, 1996). Six physicians used the
application. The SUS score is major than fifty for all
the physicians. Its average value is seventy four. The
questions such as: clinical records are organised and
legible, access to EHRs from any place, information
quality in the application were strongly agreed. The
results can be viewed in Table I. According to these
results, our web-based application is useful for the
physicians because SUS score is always major than
50.
4 CONCLUSIONS
In this study, a web-based application has been
developed to store and exchange EHRs and fundus
photographs in Ophthalmology by using HL7/CDA
and DICOM standards. EHRs have several distinct
advantages and disadvantages over paper health
records. One advantage is the fact that there are
increased storage capabilities for longer periods of
time. EHRs can also provide medical alerts and
reminders. Some of the disadvantages include such
items as the startup costs, which can be excessive.
Another disadvantage to an EHR is that there is a
substantial learning curve and it is helpful when the
users have some type of technical knowledge
(Gurley, 2004).
Table 1: Satisfaction survey results.
Questions Physicians
1 2 3 4 5 6
1 4 4 4 4 4 4
2 3 4 4 3 4 4
3 3 4 4 4 3 3
4 3 3 3 4 3 3
5 4 3 3 3 4 4
6 4 4 4 4 4 4
7 4 4 4 4 4 2
8 2 2 1 2 2 4
9 2 2 2 2 2 2
10 4 4 3 4 4 4
SUS Score 67,5 75 67,5 80 80 75
Figure 5: Users satisfaction survey.
TeleOftalWeb 3.2 advantages are: its adaptation
to the HL7/CDA and DICOM standards, the
interoperability facilitation between institutions and
applications and its security. The physicians can
analyze EHRs everywhere. The application verifies
the standards related to privacy and confidentiality.
However, the application speed depends mainly on
the Internet connection and the number of users in
the system. When this number is high, the
application speed is lower.
DICOM and HL7 are well-accepted healthcare
industry standard. DICOM is used in diferent
medical fields, such as pathology, endoscopy,
dentistry, ophthalmology and dermatology. It is a
success for radiology and cardiology, and it is now
beginning to be used for other clinical specialties
(Kuzmak and Dayhoff, 2003).
According to our review, we analyzed several
studies about EHR systems. These systems have
been presented using XML-based Clinical
Document Architecture to exchange discharge
summaries (Paterson et al., 2002). There are EHR
applications in different specialities such as pediatric
OPHTHALMOLOGIC ELECTRONIC HEALTH RECORDS SYSTEM USING HL7/CDA AND DICOM -
TELEOFTALWEB
103

(Ginsburg, 2007), ophthalmology (Chew et al.,
1998), emergency departments (Amouh et al., 2007)
and oncology (James et al., 2001). In the telematic
system for oncology, they use a data warehouse as
EPRs server. The authors do not present a EHRs
standardization process. Information system for
emergency department has been implemented by
prototyping a web-based application. It makes uses
the XML-based openEHR standard.
In summary, we have designed, developed and
evaluated a web-based application to store and share
EHRs in ophthalmology by using HL7/CDA and
DICOM standards. Our application treats to solve
some of the barriers to the EHRs adoption in
ophthalmology. The records and the fundus
photographs in all type of formats are continuously
updated and are available concurrently for use
everywhere. We verified that the application was
useful for the physicians.
REFERENCES
Amouh, T., Gemo, M., Macq, B., Vanderdonckt, J.,
Wahed, A., Reynaert, M.S., Stamatakis, L., Thys, F.,
2005. Versatile Clinical Information System Design
for Emergency Departments. IEEE Transactions on
Information Technology in Biomedicine, vol. 9, no. 2,
pp. 174-183.
Bostrom, A.C., Schafer, P., Dontje, K., Pohl, J.M.,
Nagelkerk, J., Cavanagh, S.J., 2006. Electronic health
record: implementation across the Michigan Academic
Consortium. Comput Inform Nurs, vol. 24, pp. 44–52.
Bott, O.J., 2004. Electronic Health Record:
Standardization and Implementation. In 2nd
OpenECG Workshop, pp. 57-60.
Brooke, J., 1996. SUS: a "quick and dirty" usability scale.
Chew, S.J., Cheng, H.M., Lam, D.S.C., Cheng, A.C.K.,
Leung, A.T.S., Chua, J.K.H., Yu, C.P., Balakrishnan,
V., Chan, W.K., 1998. OphthWeb-cost-effective
telemedicine for ophthalmology. Hong Kong Medial
Journal, vol. 4, no. 3, pp. 300-304.
Chronaki, E., Lelis, P., Demou, C., Tsiknakis, M.,
Orphanoudakis, S.C., 2002. An HL7/CDA framework
for the design and deployment of Telemedicine
services. In Proceedings of the 23rd Annual EMBS
International Conference, pp. 3504-35-07.
Dolin, R.H., Alschuler, L., Boyer, S., Behlen, F.M., Biron,
P.V., Shabo, A., 2006. HL7 Clinical Document
Architecture, Release 2. J Am Med Inform Assoc, vol.
13, pp. 30-9.
Eichelberg, M., Aden, T., Riesmeier, J., 2005. A survey
and Analysis of Electronic Healthcare Record
Standards. ACM Computing Surveys, vol. 5, no. 14,
pp. 1-47.
Fedyukin, I., Reviakin, Y.G., Orlov, O.I., Doarn, C.R.,
Harnett, D.M., Merrell, R.C., 2002. Experience in the
application of Java Technologies in telemedicine.
eHealth International, vol. 1, no. 3, pp. 1-6.
Gans, D., Kralewski, J., Hammons, T., Dowd, B., 2006.
Medical groups’ adoption of electronic health records
and information systems. Health affairs (Project
Hope), vol. 24, no. 5, pp. 1323-1333.
Ginsburg, M., 2007. Pediatric Electronic Health Record
Interface Design: The PedOne System. In Proceedings
of the 40th Hawaii International Conference on
System Sciences, pp. 1-10.
Gurley, L., 2004. Advantages and disadvantages of the
Electronic Medical Record. American Academy of
Medical Administrators.
HIMSS Electronic Health Record Committee, 2003. EHR
Definition, Attributes and Essential Requirement
Version 1.0.
Hornero, R., López, M.I., Acebes, M., Calonge, T., 2003.
Teleophthalmology for diabetic retinopathy screening
in a rural area of Spain. In Eighth Annual Meeting of
the American Telemedicine Association (ATA’2003),
pp. 111.
James, A., Wilcox, Y., Naguib, R.N.G., 2001. A
Telematic System for Oncology Based on Electronic
Health and Patient Records. IEEE Transactions on
Information Technology in Biomedicine
, vol. 5, no. 1,
pp. 16-7.
Kuzmak, P.M., Dayhoff, R.E., 2003. Experience with
DICOM for the clinical specialities in the healthcare
enterprise. In Proceedings of the SPIE, vol. 5033, pp.
18-29.
Lo, H.G., Newmark, L.P., Yoon, C., Volk, L.A., Carlson,
V.L., Kittler, A.F., Lippincott, M., Wang, T., Bates,
D.W., 2007. Electronic Health Records in Specialty
Care: A Time-Motion Study. Journal of the American
Medical Informatics Association, vol. 14, no. 5, pp.
609-15.
National Eye Institute, 2008. Available at:
http://www.nei.nih.gov.
Oracle Database Online Documentation 10g Release 2,
2008, Available at: http://youngcow.net/doc/
oracle10g/index.htm.
Paterson, G.I., Shepherd, M., Wang, X., Watters, C.,
Zitner, D., 2002. Using the XML-based Clinical
Document Architecture for Exchange of Structured
Discharge Summaries. In Proceedings of the 35th
Hawaii International Conference on System Sciences,
pp. 119-128.
Pawson, D., Editor, 2002. XSL-FO Making XML Look
Good in Print. O’Reilly Media.
Smith, D., Newell, L.M., 2002. A Physician's Perspective:
Deploying the EMR. Journal of Healthcare
Information Management, vol. 16, no. 2, pp. 71-79.
Yogesan, K., Constable, I., Eikelboom, R., van Saarloos,
P., 1998. Tele-ophthalmic screening using digital
imaging devices. Aust NZJ Ophthalmol, vol. 26, pp. 9-
11.
HEALTHINF 2009 - International Conference on Health Informatics
104
