
A TAXONOMY OF INFORMATION NEEDS
OF INFORMAL CARERS
An Empirical Investigation
Basil Alzougool, Shanton Chang
Department of Information Systems, Faculty of Science, The University of Melbourne, Australia
Kathleen Gray
Biomedical Multimedia Unit- Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne, Australia
Keywords: Information Needs, Informal Carers, Consumer Health Information, Diabetes, Children, Parents, Case
Study.
Abstract: Researchers and practitioners are increasingly aware of the importance of the information needs of informal
carers. However, little research has investigated their information needs comprehensively within the lived
experience of being an informal carer. This paper presents a taxonomy of information needs of informal
carers that assists in understanding their information needs more fully. This taxonomy divides information
needs of informal carers into four major conceptual categories: (i) information needs related to the persons
needing care, (ii) information needs related to the informal carers themselves, (iii) information needs related
to the interaction between the persons needing care and informal carers; and (iv) information needs related
to the interaction between informal carers and other parties. The usefulness of this taxonomy is
demonstrated empirically using the results of eight case studies of carers of children with Type 1 diabetes.
Evidence is provided to show how this taxonomy gives a multi-dimensional account of the information
needs of informal carers. These results are important for those who work with such carers and for those who
are concerned with addressing the information needs of informal carers in other healthcare contexts.
1 INFORMATION NEEDS OF
INFORMAL CARERS
Researchers and practitioners are increasingly aware of
the importance of the information needs of informal
carers. However, little research has explored their
information needs comprehensively within the lived
experience of being an informal carer. Moreover,
existing research has concentrated on carers’
information needs that are most directly related to their
patients’ needs. Information needs related to other
aspects of being a carer have hardly been addressed in
the literature. Drawing upon existing research on the
information needs of informal carers, the authors have
previously developed a taxonomy of information needs
of informal carers (Alzougool et al., 2007 & 2008) with
the aim of giving a richer, more multi-faceted account
of the information needs of this group.The aim of the
present paper is to illustrate the usefulness of this
taxonomy with empirical data gathered from eight cases
of informal carers of children with Type 1 diabetes.
These cases were selected as an example of a group of
healthcare information consumers whose information
needs are important because of the large and growing
impact of this health condition on the healthcare system.
Empirical evidence is provided to show how this
taxonomy assists in describing many more aspects of
the information needs of informal carers than are
commonly recognised.
Researchers generally use the term “informal carer”
to refer to “someone who actively participates in
sharing the patient’s illness experience on a practical
and / or emotional level” (Beaver & Witham 2007, p.
17). The core tasks of informal carers are varied
depending on the care situation (Zapart et al., 2007;
Pickard & Glendinning, 2002). Most tasks are done at
home. While caring for someone can be a positive
experience, many carers are harmed physically,
mentally, emotionally and socially by their caring roles
(Access Economics, 2005). In terms of diabetes, over
95% of care is done at home by people living with
diabetes and/or their informal carers. Managing
diabetes, especially in children, is difficult and
161
Alzougool B., Chang S. and Gray K. (2009).
A TAXONOMY OF INFORMATION NEEDS OF INFORMAL CARERS - An Empirical Investigation.
In Proceedings of the International Conference on Health Informatics, pages 161-167
DOI: 10.5220/0001512701610167
Copyright
c
SciTePress

challenging (International Diabetes Federation, 2007).
Although research has highlighted the importance of
information for informal carers (e.g. Zapart et al., 2007)
to do their tasks more effectively, informal carers
continue to report a number of unmet needs including
information needs (Pickard & Glendinning, 2002).
Research has also shown that information provision for
informal carers is still inadequate in many respects
(Hummelinck & Pollock, 2006; Kendall et al., 2004).
Topics of information that informal carers need vary
widely according to: the various tasks that they do, the
characteristics of informal carers, the illness’s duration
and stage and caring processes (Krishnasamy et al.,
2007; Janda et al., 2006). Moreover, the relationship
between informal carers and persons needing care is a
main barrier that inhibits informal carers from accessing
information that fulfils their information needs (Kendall
et al., 2004). Many informal carers hardly express their
information needs and some may not even know how to
articulate those needs (Hummelinck & Pollock, 2006).
Furthermore, informal carers may have some
information needs similar to those of the persons whom
they care for; nonetheless, they also have specific types
of information needs in order to be able to handle the
caring process more effectively (Beaver & Witham,
2007). Therefore, informal carers not only need
information to support the persons needing care, but
also they need information to support themselves.
Most studies specifically of informal carers of
children with diabetes have investigated the impact of
diabetes on the family, their worries, their coping
strategies to reduce their worries and to manage the
diabetes of their children at home (e.g. Carroll &
Marrero, 2006; Lowes et al., 2004). However, there is
little research that focuses on the information needs of
this group (e.g. Collier et al., 2001).
Although the literature covers many different
aspects of information needs of informal carers, little
research has attempted to give an integrated account of
these needs. Therefore, we propose a taxonomy of
information needs of informal carers which incorporates
the possible interactions and activities between the
informal carer and the person needing care, as well as
between the informal carer and other parties involved in
service provision.
2 A TAXONOMY OF THE
INFORMATION NEEDS OF
INFORMAL CARERS
In this section we present the taxonomy of the
information needs of informal carers adopted from our
previous studies (Alzougool et al., 2007 & 2008). The
primary purpose of the taxonomy is to provide a
framework that assists in understanding and including
the diversity of information needs that ensue from
informal carers’ interactions and activities and is
empirically testable. The taxonomy also provides a way
to investigate the information needs based on these
activities and interactions. This taxonomy divides
information needs of informal carers into four major
conceptual categories:
1) Information Needs related to the Persons
Needing Care. This information arises from the
condition of the patient or the person needing care
and may be similar to some of the information
needs of patients themselves especially the medical
information. Most research has explored these
information needs (e.g. Hepworth, 2004).
2) Information Needs related to the Informal
Carers Themselves. Informal carers need
information that draws their caring journey in
order to adjust with it and predict their actions and
activities. Since caring affects informal carers
emotionally and physically (Zapart et al., 2007)
they also need information to help them to be
carers without overwhelming their personal lives.
Moreover, informal carers need to maintain a
personal identity beyond their role as a carer
(NSW Department of Ageing, Disability and
Home Care, 2006). Furthermore, they need to
know their rights and obligations in terms of the
confidentiality and privacy restrictions on the
information related to the patient or the person
needing care
3) Information Needs related to the Interaction
between Informal Carers and Persons Needing
Care. Interaction between the informal carers and
the patient or the person needing care is central to
their role and relationship. This interaction
increases in certain situations, for example if the
person needing care is a child with chronic disease.
This interaction inevitably has some positive and
some negative aspects. Informal carers experience
a number of emotional reactions to their caring
role (Zapart et al., 2007). Informal carers need
information about how to interact with the patient
or the person needing care and information about
how to encourage the positive aspects of this
interaction and reduce and manage the negative
aspects of it.
4) Information Needs related to the Interaction
between Informal Carers and Other Parties
(Professionals, Nurses, Teachers, etc). Informal
carers may be required to interact with many
parties regarding the person needing care. These
interactions too may increase in certain situations,
such as when the person needing care is a child.
Informal carers need to know what services are
provided, by and for whom. They also need to
have the necessary skills to communicate with
service providers (Health Canada, 2005).
HEALTHINF 2009 - International Conference on Health Informatics
162

In general, individuals’ information needs do not exist
in isolation; they exist when people perform a role/task,
experience a problem or difficulty or are under some
pressure/stress. Understanding these dimensions is
crucial to identify the information needs associated with
them (Nicholas, 1996). To fully understand the
information needs of informal carers we must explore
their activities and interactions using all four categories
in our taxonomy.
3 METHOD
To test the usefulness of this taxonomy of the
information needs of informal carers, a study of eight
informal carers of children with diabetes was
undertaken, using a qualitative case study approach
(Yin, 2002). This study used a convenience sample,
identifying experienced informal carers of diabetic
children who were willing and able to give to a
researcher a full description of experiences that could be
analysed to build a comprehensive picture of their
information needs. Potential participants were recruited
through not-for-profit, non-clinical organizations.
Criteria for inclusion as a case study included any
person over the age of 18 years old who provided a
diabetic child with unpaid day to day caring services on
a practical and /or emotional level. The eight case
studies reflect a range of caring experiences. For
example, six of these informal carers were mothers and
two were fathers of a diabetic child. Four have African
ethnic background, three Anglo-Saxons and one
Arabian. The average age of these carers were
approximately 40 years old, and their average caring
experiences were approximately 6 years. Half of these
carers had a secondary school certificate or less. Six of
these carers were living in urban areas and two in rural
areas. The average age of diabetic children at time of
interview was approximately 11 years old.
Semi-structured interviews based on the taxonomy
described in this paper were conducted between
December 2007 and June 2008 with each of the carers
in their own homes. The interviews lasted for
approximately 40 to 150 minutes and explored a range
of topics including: information background, everyday
experiences and tasks with the persons needing care in
regards to their illness, treatment, managing illness, and
other aspects of everyday life, and their experiences in
regards to their own personal lives, interaction between
them and persons needing care and other parties (e.g.
physicians, nurses, diabetes educators).
The interview transcripts were analysed by a
researcher using two strategies (Berg, 2004): firstly,
inductive content analysis was used, reading and
rereading the transcripts, coding, preliminary
categorisation, and further classification of data into
categories and sub-categories, working backwards and
forwards between the data and the coding scheme; and
secondly deductive content analysis was used to sort the
categories that were identified into the four major
conceptual components of the taxonomy. A second
researcher was asked to evaluate the findings for
accuracy and completeness.
4 FINDINGS
This section presents each of the components of the
taxonomy with one or more representative excerpts
from the raw data to show that each one was supported
by data from the case studies. Each component also
includes a number of categories and sub-categories of
information needs that fall within it as well as the
number of times each sub-category emerged from the
data:
1) Information Needs Related to the Persons
Needing Care: The first component of the
taxonomy involves a number of categories and sub-
categories of information needs required by the
carers. Table 1 presents definitions for each of these
categories of information needs, frequencies of sub-
categories and example excerpts from transcripts to
illustrate the nature of information needs of informal
carers related to the person needing care. As shown
in Table 1, approximately 75% of sub-categories of
these information needs have been identified in at
least of six out of eight cases in the study. Other
sub-categories have been manifested in two to four
of the cases.
2) Information Needs Related to the Carers
Themselves: This component involves three
categories and twelve sub-categories of information
needs required by the carers. Table 2 presents
definitions for each of these categories of
information needs, frequencies of sub-categories and
example excerpts from transcripts. As shown in
Table 2, nine sub-categories of these information
needs have been identified in at least of seven out of
eight cases in the study. The other sub-categories
have occurred five or six times.
3) Information Needs Related to the Interaction
between the Carer and the Person Needing Care:
The third component involves a number of
categories and sub-categories of information needs
required by the carers. Table 3 presents definitions
for each of these categories of information needs,
frequencies of sub-categories and example excerpts
from transcripts. As shown in Table 3, ten sub-
categories of these information needs have been
highlighted by at least seven out of eight cases in the
study. The other three sub-categories have appeared
four to six times among the cases.
A TAXONOMY OF INFORMATION NEEDS OF INFORMAL CARERS - An Empirical Investigation
163
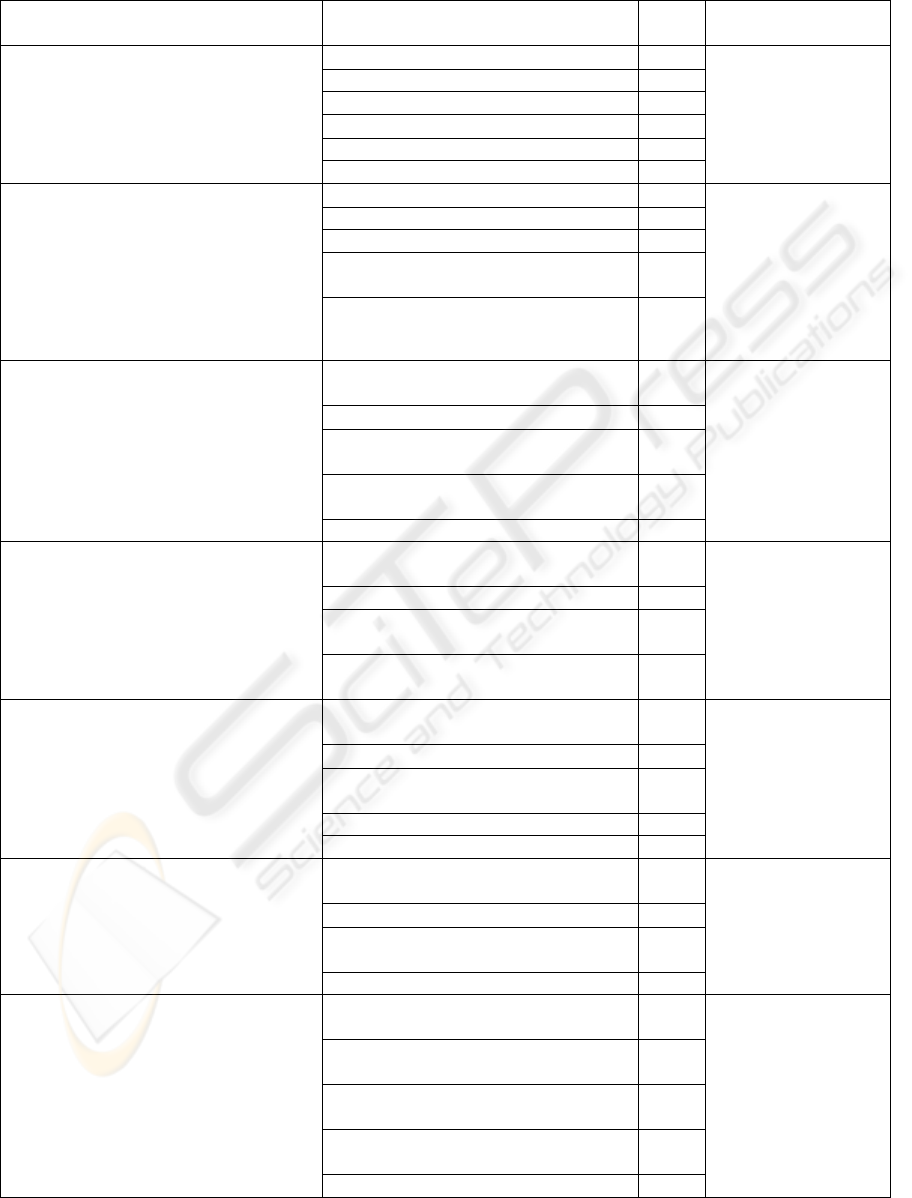
Table 1: Categories and sub-categories of information needs related to the person needing care, frequencies and
representative quotes from case studies.
Categories Sub-Categories
Frqcy
(n = 8)
Example Quotes from Case
Studies
(1) Information about the condition itself: This
refers to information about causes of the condition,
its symptoms, its types, and its possible
complications as well as if there are any precautions
to prevent the condition and how it is diagnosed.
Causes of the conditions 8 “At that time…we’ve never
known about type 1 and type
2, but people in the hospital
explained to us about type 1
and type 2” [Case 2].
Different types of the conditions 6
Symptoms of the condition 6
Precaution to prevent the condition 3
Possible complications of the condition 3
Diagnosis process of the condition 2
(2) Information about treatment of the condition:
This refers to information about treatment options
and their functionality and suitability of particular
treatments to the person needing care, advantages
and disadvantages of these options and technologies
used in treatment and management of the condition
and latest research findings about new treatments,
cure and trials.
Treatment options and their functionality 8 “We’ve (he and his wife)
asked them to explain to us
the positives and the
negatives (of the pump) and
different other options”
[Case 1].
Suitability of the treatment to the person 7
Advantages and disadvantages of the treatment 4
Technology used in the treatment and management
of the condition
4
Latest news about the treatment possibilities and
research, cure, and trials
4
(3) Information about ongoing management and
control of the condition: This includes information
that is related to guidelines, procedures, times and
places of managing and controlling the condition,
symptoms of controlling and non-controlling of the
condition, and things that carers should do to control
and manage the condition including guidelines that
help carers to take decisions to facilitate this process.
Guidelines and procedures to mange and control
the condition during the day and night
8
“No one told me how to
manage it, doctor told me
quickly but I’ve forgotten,
after that I’ve found other
parents and books (to learn
from them) [Case 4].
Times and places of controlling of the condition 8
Symptoms of controlling and non-controlling of the
condition
8
Guidelines for taking decisions during the condition
management and control
8
Things to be done to manage the condition 8
(4) Impact of the condition on personal and social
life of the person needing care: This refers to
information about effects of the condition on the
abilities, development, feelings, behaviour, attitude,
professional and family life of the person needing
care and their activities with friends.
Effects of the condition on the abilities and
development of person needing care
8
“How your child feels…A
psychologist's view on signs
of distress in my son…
difficulties within marriage
related to my son's diabetes
management” [Case 8].
Effects of the condition on the his/her feelings 8
Effects of the condition on the behaviour and
attitude of the person needing care
6
Effects of the condition on the professional and
family life of the person needing care
6
(5) Nutrition and diet requirements: This includes
information about choices, types, times, amounts of
food that are suitable for the person needing care
including recipes, shopping guidelines and places
that sell this food as well as effects of food, eating
and non-eating on the condition of person needing
care.
Choices and types of food that are suitable for the
person needing care
8
“You spend your time
wondering is that a serve or
is it not a serve…I don’t
really know…so it’s not
until you go eat it or you use
it” [Case 5].
Times and amounts of the food 8
Effects of food, eating and non-eating on the
condition of person needing care
8
Preparation and recipes of food 8
Shopping guidelines of food and places that sell it 3
(6) Exercise requirements: This refers to
information about choices, types, times and periods
of exercises that are suitable for the person needing
care including things to do, avoid and have during
the exercises as well as effects of exercise and non-
exercise on the person needing care.
Choices and types of exercises that are suitable for
the person needing care
8
“I…need more
…information related to just
how much her body needs
this (exercise) continually”
[Case 6].
Times and periods of the exercises 8
Effects of exercises and non-exercises on the
person
8
Things to do, avoid and have during the exercises 7
(7) Routine activities outside the home (school,
work, camping, travel): This refers to information
about things that persons needing care have to take,
do, avoid, have and will do while they are outside the
home, and the services available that are of interest to
the person needing care as well as the effects of the
condition on activities outside home and vice versa.
Things that persons needing care have to take with
them while they are outside the home
8
“The written materials that
we still have at home that
are explaining every thing
that child may be need, at
home, outside, at school,
every where’ [Case 7].
Things that persons needing care should do, avoid
or have while they are outside home.
8
Effects of the condition on activities outside the
home
7
Things that they will do while they are outside
home
4
what services available outside the home 2
HEALTHINF 2009 - International Conference on Health Informatics
164
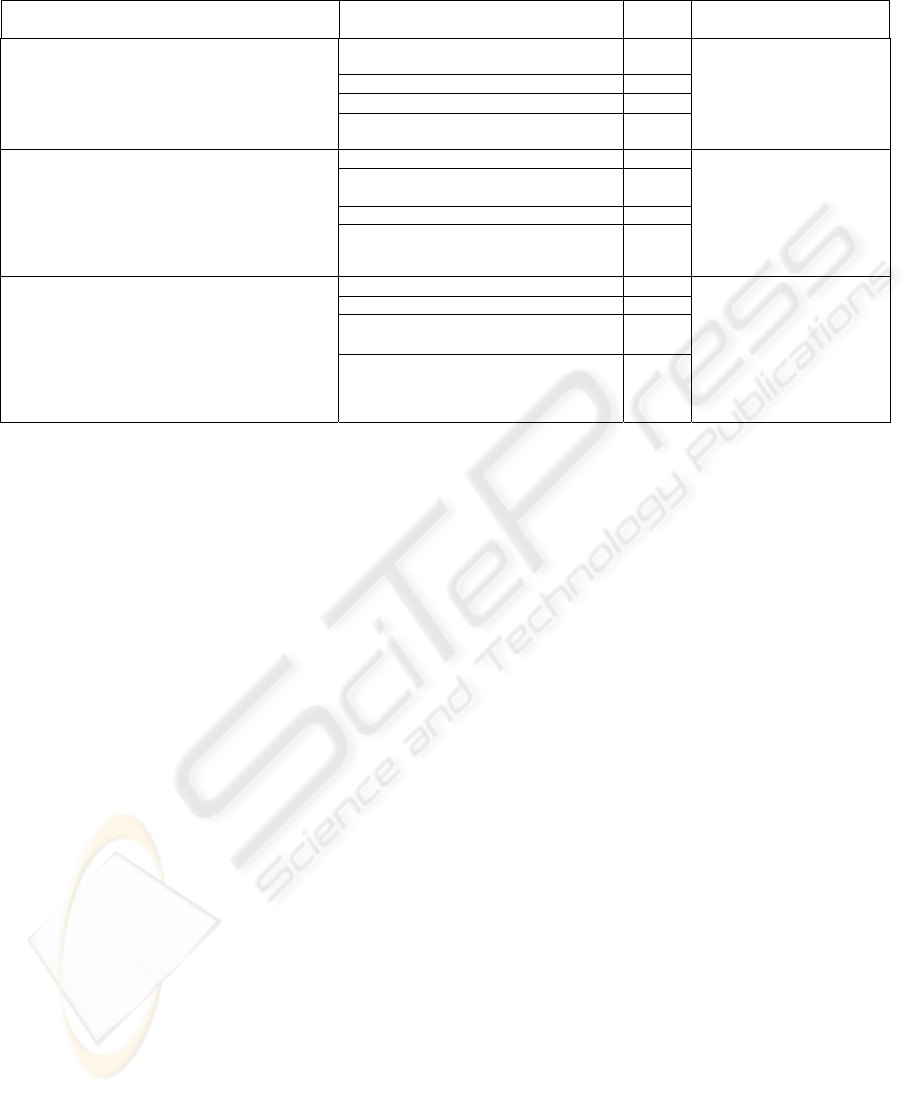
Table 2: Categories and sub-categories of information needs related to carers themselves, frequencies and representative
quotes from case studies.
Categories Sub-Categories
Frqcy
(n = 8)
Example Quotes from Case
Studies
(1) Information about caring process: This refers to
information that provides a step by step guide, times
and places of the caring process and things that carers
have to engage in, in order to care effectively and
possible scenarios that can happen and how to deal
with, supported with real examples from other carers.
A step by step guide for performing the caring
process
8
“The dietician and educator
have taught us how to…handle
him, how to prepare the
needle, when to give him
it…all you need to care about
him” [Case 1].
Times and places of caring process 8
Things that carers should do to care 8
Map of the caring journey with real examples
from other carers
7
(2) Coping with the condition and caring process:
This includes information about feelings and feelings
management, and strategies that help carers to cope with
the condition and look after themselves including verbal
support from any person who comes into contact with
carers, especially family, healthcare professionals and
other carers.
Feelings and feelings management of the carer 8 “It’s not like ok “do you find
it overwhelming? Get a diary
that will make it easier” or,
“there is no information for
you …sometimes how to cope”
[Case 5].
Coping strategies with the condition and
caring journey
8
Verbal support to the carer 6
Strategies for carers to look after themselves 5
(3) Information about new skills: This refers to
information that provides carers with kinds of skills,
applicable place and timeliness of skills, as well as
lengths of time the skills might be needed in order to
carry out the caring process effectively including the
purposes and reasons for learning these skills. This
information also includes carers’ rights and how to
negotiate with third parties.
Kinds of skills that carers have to learn to care 8 “I didn’t know before how to
inject the insulin…I couldn’t
do her finger test… (It took
her) about three…months to
learn … now I know how to do
it” [Case 3]. “I am not a
nurse…so I need (to learn to be
like a nurse)” [Case 7].
Purposes and reasons for learning these skills 7
Carers’ rights and how they interact with other
parties regarding the person needing care
7
Time, period, cost and place of skills training 6
4) Information Needs Related to the Interaction
between the Carer and other Parties: This
component involves two categories and six sub-
categories of information needs required by the
carers. Table 4 presents definitions for each of these
categories of information needs, frequencies of sub-
categories and example excerpts from transcripts.
As shown in Table 4, four sub-categories of these
information needs have been identified in all cases
in the study. The other two sub-categories have
been manifested in four to five of the cases.
5 DISCUSSION
This empirical investigation suggests that the research
method and the analytical framework applied here can
be used to add depth and breadth to previously reported
understandings of the information needs of informal
carers. By asking the carers about their every day tasks
and activities and interactions (with the person needing
care and other parties), it was possible to identify what
their information needs were. The taxonomy was useful
in revealing their information needs related to their
diabetic children, themselves, interaction between them
and their children, and interaction between them and
other parties in regards to their children.
More than half (as measured by number of
categories) of the information needs of these informal
carers were not directly related to the condition of the
person needing care, rather they were indirect than this.
Therefore, it is reasonable to suggest that the taxonomy
revealed a more holistic view of information needs of
carers than previous studies have done. In other words,
these findings suggest that the other three components
of the taxonomy maybe just as important as the first
component. This in turn may have an impact on the
way we provide information to informal carers and take
into consideration their wider information needs. This
means that in the education, support and networks of
information for informal carers, it is necessary to
provide more than basic diagnostic information about
the person needing care.
For example, in terms of providing support to
families where a child has been diagnosed with
diabetes, it is just as essential to provide timely
information on many aspects such as: child
development, social life, caring progress and coping,
and interactions inside and outside the home. This
emphasises the importance of ongoing support for
carers through the provision of information beyond the
initial diagnosis.
This study also confirmed some types of
information needs that researchers have identified. For
example, previous researchers have found that informal
carers need information regarding the condition of the
person needing care (e.g. Beaver & Witham, 2007),
treatment and medications (e.g. Hummelinck &
Pollock, 2006), physical, psychological and social
aspects of the caring services (e.g. Richardson et al.,
2007), coping strategies (e.g. Kendall et al., 2004), side
effects and diet (e.g. Hepworth, 2004), and illness’s
management plan (e.g. Hummelinck & Pollock, 2006).
Although there have been some information needs
identified by previous researchers that may fall into
some other components of the taxonomy, most of the
available literature has focused on the first component,
namely, the information needs related to the persons
needing care. The other three components of the
A TAXONOMY OF INFORMATION NEEDS OF INFORMAL CARERS - An Empirical Investigation
165
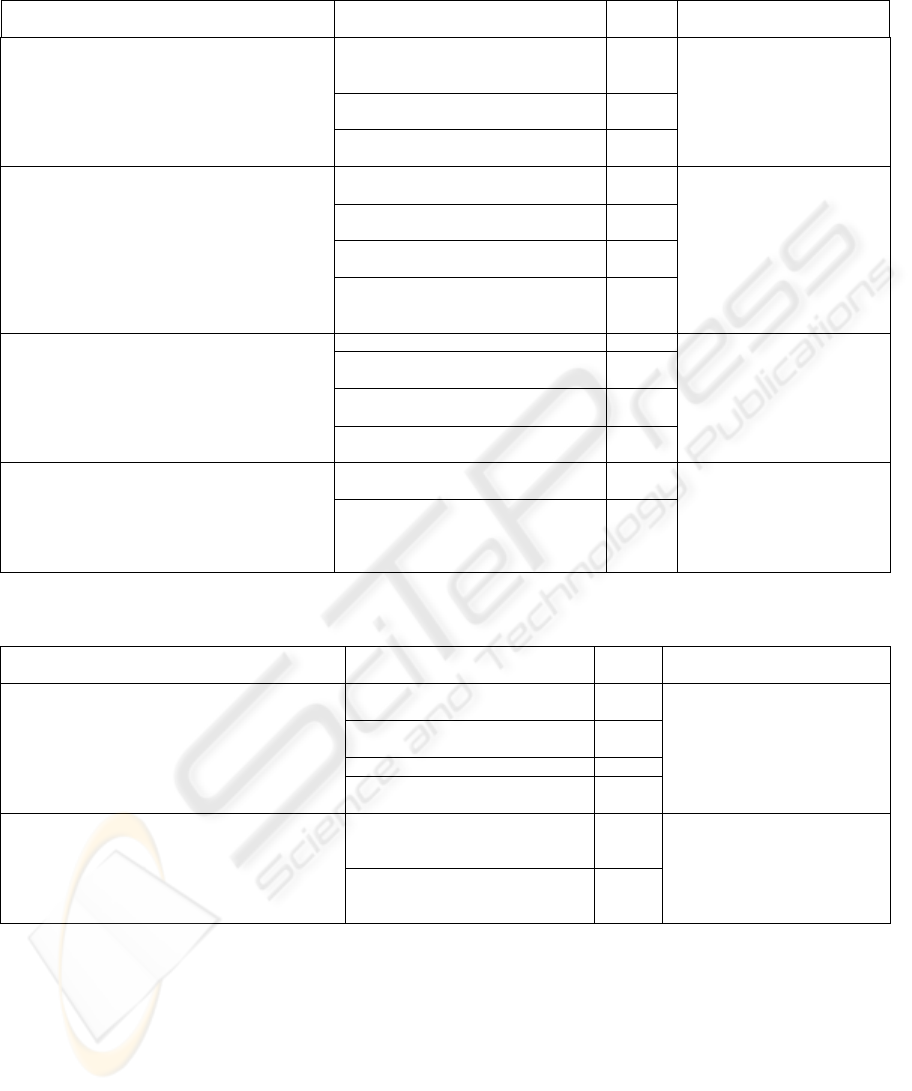
Table 3: Categories and sub-categories of information needs related to the interaction between the carer and the person
needing care, frequencies and representative quotes the case studies.
Categories Sub-Categories
Frqcy
(n = 8)
Example Quotes from Case
Studies
(1) Transferring information to the person needing
care: This refers to information about types, times and
amounts of information that carers have to give to the
person needing care, which is supported by strategies
on how to transfer these types of information to the
person needing care.
Types of information (what and how to) that
carers should give to the person needing
care
8 “The information to impart that
knowledge to him in such a way,
but it is not overbearing, and it
isn’t treating him like a little
child” [Case 8].
Times and amounts of information that
should be given to the person needing care
8
Strategies to transfer the information to the
person needing care
8
(2) Strategies of interactions with the person
needing care: This includes information that provides
carers with strategies that help them to convince
persons needing care to apply caring process, to deal
with and parenting persons needing care during
different stages, to build trust, to maintain self-esteem,
and address questions of persons needing care related
to their conditions.
Strategies to convince the person needing
care to apply caring process
8 “I have trouble with him not
rotating his needles, his
injections, he constantly wants to
have them in his thighs, so
I…sought information from
doctors about that…it’s a battle
it’s a fight…even with the food
it’s a fight to get him to eat”
[Case 5].
Strategies to deal with and parenting the
different stages of the person needing care
8
Strategies to build trust and maintain self-
esteem to the person needing care
7
Strategies to address questions of the
persons needing care related to their
conditions
5
(3) Impact of the condition on the whole and wider
family: This refers to information about consequences
of the condition on the family and information that
carers have to give to family including strategies to
achieve commitment of the family toward caring for
the person needing care and strategies to deal with and
parenting other siblings.
Consequences of the condition on the family 8 “I felt it was very important, very
early on, to make the girls aware
of what was going on…we went
through everything that I’d been
taught in hospital” [Case 6].
Information that should be given to the
family
8
Strategies to achieve family commitment
toward caring of the person needing care
6
Strategies to deal and parenting other
siblings of the person needing care
4
(4) Changing the routine life of the person needing
care, the carer and the family: This refers to
information that provides carers with kinds of routine
life that may be changed and strategies to do that. It
also includes the benefits of changing the routine life
and consequences of not changing it.
Kinds of routine life that should be changed
and the strategies to do that
8 “We have to wake up in certain
times…we must look after him
during the day… even the doctor
said to me…your life will not be
the same … that is really what
happened” [Case 2].
Benefits of changing the routine life and
consequences of not changing it
7
Table 4: Categories and sub-categories of information needs related to the interaction between the carer and other parties,
frequencies and representative quotes from case study.
Categories Sub-Categories
Frqcy
(n = 8)
Example Quotes from Case Studies
(1) Other parties that may interact with carer and the
person needing care: This refers to information that
provides carers with identity and services provided by
these parties, and their duties and responsibilities toward
the carers and persons needing care including carers’
expectations when they interact with them.
Duties and responsibilities of other
parties toward the person needing care
8 “I had an awful time with the
school…they didn’t get the
importance of it…they didn’t
understand that he has to eat every
2.5 hrs…I’ve fought them…lots of
letters to Department of
Education”[Case 5].
Carers’ expectations from other parties
when they interact with them
8
Services provided by other parties 5
Who are other parties that may interact
with the person needing care
4
(2) Transferring information about the person
needing care to other parties: This includes transferring
any relevant information about the person needing care
to third parties, including their specific needs and care
process supported by strategies on how to transfer this
information to these parties.
Types and times of information that
carers should give to other parties
regarding the person needing care.
8 “The information is… to check
whether school nurse or
teachers…would know what to do if
he had a hypo…to insist upon things
where they stored” [Case 8].
Strategies to transfer the information to
other parties regarding the person
needing care.
8
taxonomy have not been specifically explained and
adopted in the literature to date. These findings have
the potential to increase the effectiveness of carers and
service providers who deal with them, and to be
relevant for those with system-level interests in
meeting the information needs of informal carers in
many contexts.
For example, these findings may help community
organisations that currently work and support informal
carers or patients to be aware of these multi-
dimensional information needs and take account of
these needs in their future programs and events that
target these groups of people. These findings may also
help systems designers to take account of these
information needs when they design systems that target
patients or consumers in general.
6 CONCLUSIONS
This paper has reported findings from empirical testing
of a taxonomy of information needs of informal carers.
HEALTHINF 2009 - International Conference on Health Informatics
166

The method and analytical framework were shown to
be useful to systematise the detail and pattern of
information needs in eight case studies. The carers
were keen to talk about their lives and experiences and
they were able to cope very well during the interviews.
In this respect, the interview protocol was acceptable to
the carers and shows its applicability in uncovering
their lived experiences in different contexts. By using
the four-part taxonomy, it was possible to capture most
of the interview data regarding informal carers'
information needs associated with their daily tasks and
activities and interactions. Analysis of the case studies
shows information needs in all four components,
although not evenly distributed across them. This
research project is continuing to test the usefulness of
this taxonomy with more case studies of informal
carers of children with diabetes. Future research is also
needed to test the usefulness of this taxonomy with
other groups of informal carers.
REFERENCES
Access Economics, 2005. The economic value of informal
care. Report for Carers Australia. Available from:
http://www.carersaustralia.com.au/images/stories/Acc
ess%20Economics%20study%20full.pdf
Alzougool, B., Chang, S., & Gray, K., 2007, ‘Modeling
the information needs of informal carers’, in M.
Toleman, A. Cater-Steel, & D. Roberts (Eds.), ACIS
2007: Proceedings of the 18th Australasian
Conference on Information Systems (pp. 345-
355).Toowoomba, 5-7 December 2007, University of
Southern Queensland, Australia. Available from:
http://www.acis2007.usq.edu.au/assets/papers/62.pdf
Alzougool, B., Gray, K., & Chang, S., 2008, ‘Toward a
Taxonomy of Information Needs of Informal Carers:
A Case Study of a Carer of a Child with Diabetes’, in
H. Grain (Eds.), HIC 2008: Proceedings of Australia’s
Health Informatics Conference. Melbourne, 31
August-2 September 2008, Health Informatics Society
of Australia (HISA), Australia. Available from: http://
www.hisa.org.au/system/files/u2233/07-Chapter02.pdf.
Beaver, K., & Witham, G., 2007. Information needs of the
informal carers of women treated for breast cancer’
European Journal of Oncology Nursing, 11(1), 16-25.
Berg, B. L., 2004. Qualitative research methods for social
sciences, Pearson; Allyn and Bacon. Boston, Mass, 5
th
edition.
Carroll, A. E., & Marrero, D. G., 2006. How do parents
perceive their adolescent's diabetes: a qualitative
study. Diabetic Medicine, 23(11), 1222-1224.
Collier, J., Pattison, H., Watson, A., & Sheard, C., 2001.
Parental information needs in chronic renal failure and
diabetes mellitus. European Journal of Pediatrics,
160, 31-36.
Health Canada, 2005. The information needs of informal
caregivers involved in providing support to a critically
ill loved one. A synthesis report, prepared by Janet
Dunbrack. Available from: http://www.hc-sc.gc.ca
/hcs-sss/alt_formats/hpb-dgps/pdf/pubs/2005-info-
caregiver-aidant/2005-info-caregiver-aidant-eng.pdf
Hepworth, M., 2004. A framework for understanding user
requirements for an information service: Defining the
needs of informal carers. Journal of the American
Society for Information Science and Technology,
55(8), 695-708.
Hummelinck, A., & Pollock, K., 2006. Parents'
information needs about the treatment of their
chronically ill child: A qualitative study. Patient
Education and Counselling, 62(2), 228-234.
International Diabetes Federation, 2007. Diabetes Atlas,3
rd
edition. Available from: http://www.eatlas.idf.org/
Janda, M., Eakin, E. G., Bailey, L., Walker, D., & Troy,
K., 2006. Supportive care needs of people with brain
tumours and their carers. Supportive Care in Cancer,
14(11), 1094-1103.
Kendall, S., Thompson, D., & Couldridge, L., 2004. The
information needs of carers of adults diagnosed with
epilepsy. Seizure, 13(7), 499-508.
Krishnasamy, M., Wells, M., & Wilkie, E., 2007. Patients
and carer experiences of care provision after a
diagnosis of lung cancer in Scotland. Supportive Care
in Cancer, 15(3), 327-332.
Lowes, L., Lyne, P., & Gregory, J. W., 2004. Childhood
diabetes: parents’ experience of home management
and the first year following diagnosis. Diabetic
Medicine, 21(6), 531-538.
Nicholas, D., 1996.Assessing information needs: tools and
techniques. ASLIB know how series, edited by Sylvia
P. Webb. ASLIB, London.
NSW Department of Ageing, Disability and Home Care,
2006. Diverse Strategies for Diverse Carers: The
Cultural Context of Family Carers in NSW. A report,
prepared by Beatriz Cardona, Sharon Chalmers, Brett
Neilson (Centre for Cultural Research, University of
Western Sydney). Available from: www.uws.edu.
au/download.php?file_id=18052&filename=FINAL_R
EPORT_JULY.pdf&mimetype=application/pdf.
Pickard, S., & Glendinning, C., 2002. Comparing and
contrasting the role of family carers and nurses in the
domestic health care of frail older people. Health and
Social Care in the Community, 10(3), 144–150.
Richardson, A., Plant, H., Moore, S., Medina, J.,
Cornwall, A., and Ream, E., 2007.Developing
supportive care for family members of people with
lung cancer: a feasibility study. Supportive Care in
Cancer, 5(11), 1259-1269.
Yin, R.K., 2002. Case Study Research: Design and
Methods, Sage Publications. Newbury Park, 3
rd
edition.
Zapart, S., Kenny, P., Hall, J., Servis, B., & Wiley, Sh.,
2007.Home-based palliative care in Sydney, Australia:
the carer’s perspective on the provision of informal
care. Health and Social Care in the Community, 15(2),
97–107.
A TAXONOMY OF INFORMATION NEEDS OF INFORMAL CARERS - An Empirical Investigation
167
