
DEVELOPMENT OF STRATHCLYDE UNIVERSITY DATA
LOGGING SYSTEM (SUDALS) FOR USE WITH FLEXIBLE
ELECTROGONIOMETERS
Vivek Padmanaabhan Indra Mohan, G. Valsan and P. J. Rowe
Health Qwest, Bioengineering Unit, University of Strathclyde, Wolfson Centre, Glasgow, G4 0NW, U.K.
Keywords: Flexible electrogoniometer, Activities of daily living (ADL), User-friendly system, Remote control,
Wireless data transmission.
Abstract: We have developed a 6 channel battery operated remote control microprocessor based system that collects
data from flexible electrogoniometers and force sensing resistors attached to the lower extremities of the
body. During functional activities, the user-friendly system stores the data from these transducers and
transfers the same to a PC at the end of the recording period via a bluetooth connection. Software on the PC
then displays the angular displacement and allows visual inspection of the entire sequence of recordings or
particular events of interest. This system was tested on 10 normal subjects and the pattern pertaining to the
flexion/extension of knee during range of activities of daily living (ADL) such as walking, ascending and
descending stairs, in and out of a chair and deep squatting were recorded and found to be reproducible and
similar to those reported in the literature.
1 INTRODUCTION
Normal lower limb activity and goal directed
movements are essential for the well-being of an
individual. However, such movements and efficient
functioning of the lower limb can be seriously
affected for a variety of reasons and one such
common cause is Osteoarthritis. This degenerative
joint disorder is often disabling and is characterized
by pain and physical limitation. (Rowe et al, 2005).
As a result, functions of lower limb are affected,
causing individuals to have problems with ADL
such as; walking, climbing stairs, getting in and out
of chair, getting in and out of bath etc. At this point
of time, rehabilitation and health care professionals
play a very crucial role by improving the functional
ability of their clients. Periodic assessment of the
individuals is necessary to aid the health professions
in assessing efficiency of their interventions.
Currently, two types of assessment techniques are
available for this purpose: questionnaire based
assessment and assessment based on clinical gait
analysis.
The former technique makes use of knee scoring
questionnaires such as the Western Ontario and
McMaster Universities Osteoarthritis Index
(WOMAC) and Knee Society Clinical Rating
System. (Rowe et al, 2005). Even though, these
questionnaires are popular, easy to administer and
characterize the overall performance of an
individual, research reveals that they are highly
subjective and do little to reveal any objective
information regarding the actual restoration of the
knee function required by an individual to perform
ADL.
On the other hand, clinical gait analysis is an
expensive and time consuming process. (Rowe et al,
2005). Alternatively, researchers have started using
electrogoniometry to record the dynamic knee joint
movement during a range of functional activities due
to its simpler, cheaper and reproducible nature.
(Rowe et al, 2005, Rowe et al, 2001) Mostly, such
body mounted transducers are used in combination
with information storage devices known as “Data
Loggers”. (Rowe et al, 2005).The role of these
devices is not merely to store the data collected from
these transducers but also to convert the signals
obtained from the transducers to an understandable
form. Many such devices have been developed in the
past and are also being currently used along with a
wide range of transducers such as flexible
electrogoniometers, accelerometers and strain
198
Padmanaabhan Indra Mohan V., Valsan G. and J. Rowe P. (2009).
DEVELOPMENT OF STRATHCLYDE UNIVERSITY DATA LOGGING SYSTEM (SUDALS) FOR USE WITH FLEXIBLE ELECTROGONIOMETERS .
In Proceedings of the International Conference on Biomedical Electronics and Devices, pages 198-203
DOI: 10.5220/0001533301980203
Copyright
c
SciTePress

gauges for mobility assessment, recording of plantar
pressure etc. (Zhu et al, 1991). Wireless
communication is finding its way into various
medical technological applications (Zhang.Z &
Liu.P, 2004), but most data loggers remain
hardwired. It was the premise of this work that the
data logger currently used with flexible
electrogoniometers needs further improvement in
functionality so that, the process of collecting a large
stream of data and extracting the relevant sections
could be carried out more efficiently. Further, such a
system should be able to be used by any allied health
professional in a multi centered clinical trial
evaluating post-operative rehabilitation. The lack of
such a system merits the development of a user
friendly system, whereby pushing a button would
start, stop, collect multiple data sets and transmit the
same without any physical contact between the
subject and the operator.
We have developed a portable, battery operated,
remote control microprocessor based system that
allows recording, deleting and transmitting the data
obtained from two flexible electrogoniometers and
four force sensing resistors. The data is stored in
static random access memory (SRAM) and can
subsequently be transferred via Bluetooth to a PC
which processes and analyzes the data.
2 METHOD
2.1 Overall System
The flexible electrogoniometer consists of a strain
gauged shim (a thin flexible strip) which runs the
length of the device. Damage to the device and
injury to the test subjects is prevented by enclosing
the shim in a spring. To facilitate the attachment of
device to the subjects, two light weight plastic plates
are fastened to the ends of the shim. The resulting
transducer does not have a specific centre of rotation
and is flexible in both medio-lateral and anterior-
posterior directions. Each electrogoniometer was
attached using double sided medical grade tape
laterally to the shank and thigh of individuals via
two flexible plastic strips – adjusted to the length of
their shank and thigh. In addition to this, light
weight force sensing resistors (FSR) or footswitches
were attached to the first metatarsal area of the toe
and to the heel for marking the events by indicating
the contact between the foot and the floor. Since the
transducer was mounted in the sagittal plane of the
knee, the output of the device represented the
flexion-extension angle of the knee. Both the
electrogoniometers and footswitches were interfaced
to SUDALS via thin flexible cables.
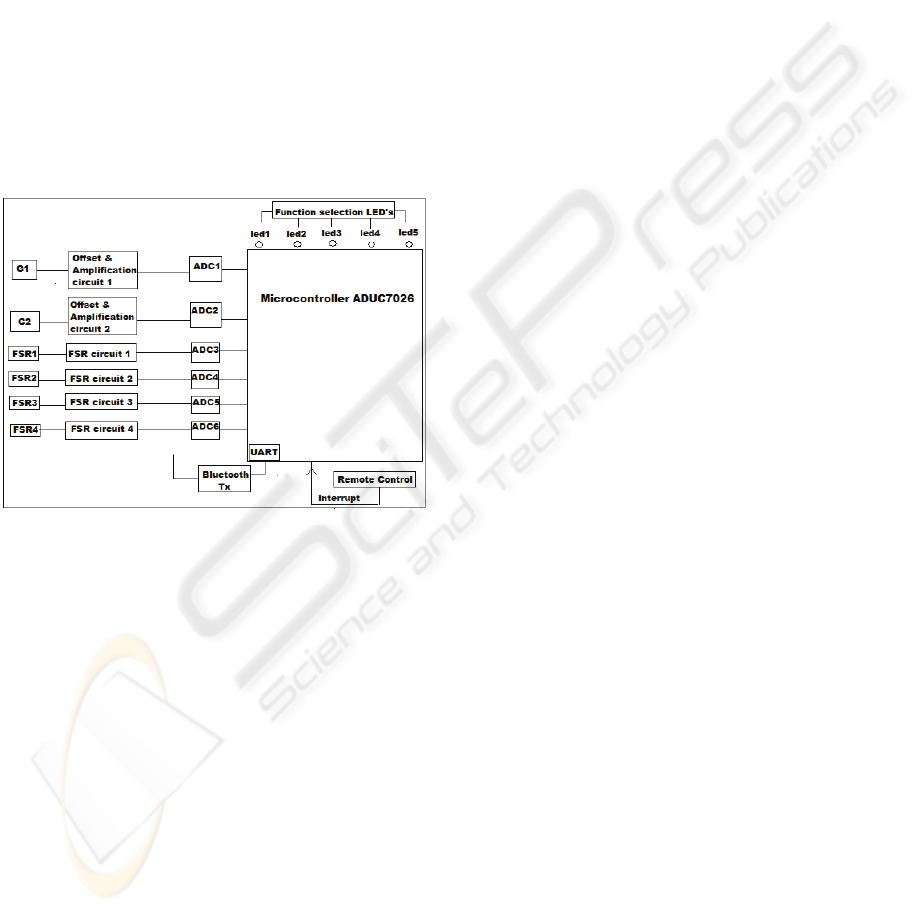
2.2 Hardware Design
The entire prototype was built on an evaluation
board – Eval ADUC7026 which consists of a 12 bit
successive approximation type Analog to Digital
converter (ADC), with an on chip 32 bit
microcontroller. The microcontroller provides both
high performance and low power consumption. The
microcontroller has several on chip facilities
including programmable watchdog timer and 12
channel multiplexer. Hence, an additional
multiplexer or a sample or hold circuit was not used
in our system. The ADC chip analogue input range
is 0 to 2.5V DC, whereas, the output of the flexible
electrogoniometer is a differential voltage. As a
result, the voltage signals from these transducers
were conditioned using high precision
Instrumentation amplifier (INA101) with suitable
gain resistors so as to make these signals compatible
with the input range of ADC. Due to the low
temperature drift feature of this amplifier, the system
will not be significantly affected by ambient
temperature. Six 1.2V alkaline AA batteries are used
for powering the evaluation board, which is
regulated via an on chip voltage regulator to 3.3V.
This is used to drive the digital side of the board and
the same voltage is being filtered by the on chip
features to drive the analog side of the board. In
addition to this, the output from the batteries is
stepped down to +/- 5V via DC-DC converter to
power the amplifiers, the transducers and other
signal conditioning components on board. The data
from two flexible electrogoniometers and from the
four force sensing resistors are sampled at 50 HZ
and the digital values are stored in a 32KB x 16
static RAM – an external memory chip interfaced
via the footprint provided on the evaluation board.
To the same memory, the data from the FSR
channels are compressed to on/off data and saved as
a single byte.
The data from the external memory is transferred
to a personal computer via a bluetooth transmitter
(HDWBTRS232 – wireless RS232 Transceiver)
interfaced to the Eval ADUC7026 via the universal
asynchronous transmitter (UART) terminal provided
on board and a transmitter line driver ADM202. The
transmitter works on a voltage range of 5V-9V DC,
which is being provided using the same AA batteries
on board. Due to high power draining application
(wireless transmission), batteries chosen for the
operation of this system has a high power rating of
DEVELOPMENT OF STRATHCLYDE UNIVERSITY DATA LOGGING SYSTEM (SUDALS) FOR USE WITH
FLEXIBLE ELECTROGONIOMETERS
199
2400 mah. A Baud rate of 19200 was used to
transmit the collected data to a personal computer
(PC) in less than a minute. At the PC end a software
code written in MATLAB is used to receive the
transmitted data and store the data in the format of
excel files which are analyzed further depending
upon the user requirement. We simultaneously
measured the knee flexion / extension angles during
activities of daily living such as; walking, ascending
and descending the stairs, sitting in and out of a
chair and deep squatting and established that the
portable system could faithfully reproduce the
signal. The obtained data is analyzed for maximum
and minimum knee flexion / extension during these
activities and the results are compared against the
normal knee range of motion during these activities
published in the literature. The overall block
diagram of the system is as shown in Figure 1.
Figure 1: System block diagram.
2.3 System Functionality
The system is aimed to perform 5 functions
corresponding to data collection. These include;
recording a test, scrapping a failed test, transmitting
the collected data from the electrogoniometers and
footswitches and resetting the entire system. In
addition to this, the system also facilitates zeroing of
the electrogoniometers prior to each recording
depending upon the user requirements. This is
accomplished by making use of an Operational
amplifier 3240 at the hardware end.
Initially, when the system is connected to the
sensors and switched on, the system is ready to zero
the sensors and to record the data corresponding to
the knee flexion/extension. Once, a singe recording
is completed, then the system facilitates the user to
make use of other functions such as; scrapping the
recorded data ‘if needed’, else transmit the collected
data via wireless and reset the entire system for next
set of data collection. Each of these above
mentioned functions can be accomplished by
providing interrupt service routines (ISR) to the
microcontroller to start or stop that specific function
via an Infra red remote transmitter and receiver
interfaced with the microcontroller, when the LED
corresponding to that function illuminates. Since, all
these functions operate within a loop arrangement;
the user can perform single recording or multiple
recording, store it in the external memory and then
transmit it to the PC via wireless. The functional
flow chart of this system is as shown in Figure 2.
2.4 System Evaluation
The system was evaluated by carrying out a pilot
study, during which the data pertaining to the
flexion/extension of the knee of the 10 young
normal healthy subjects who volunteered for this
study was collected via the flexible
electrogoniometer interfaced with this portable unit.
All the 10 subjects were asked to perform the
following 6 activities – Walking, In and Out of a
Chair, Stair ascent, Stair descend and deep squat
corresponding to daily living.
Start and stop commands were given at the
beginning and completion of each task and the
subjects were asked to repeat these tasks three times
for reproducibility and repeatability purposes.
Further, the event marking was taken into account
by the FSR’s attached to the toes and heels of each
subject.
After data collection a 4
th
order low pass
Butterworth filter at a cut-off frequency of 6 Hz was
used to eliminate the noise present in the data. The
data collected during these activities were averaged
for each subject individually and were analyzed for
maximum and minimum knee flexion. The
excursion of the knee during these activities for each
individual was obtained by calculating the difference
between the maximum angle and minimum angle.
This procedure was carried out for both the left and
right knees and was then averaged to provide the
group mean. The excursion of the knees from
SUDALS is as shown in Table 1. Table 2 shows the
maximum knee flexion angle reached during each of
these ADL. The results were compared against the
values published in the literature as shown in Table
3.
The mean normalized gait cycle obtained by
SUDALS during the experimentation is shown in
figure3.
BIODEVICES 2009 - International Conference on Biomedical Electronics and Devices
200
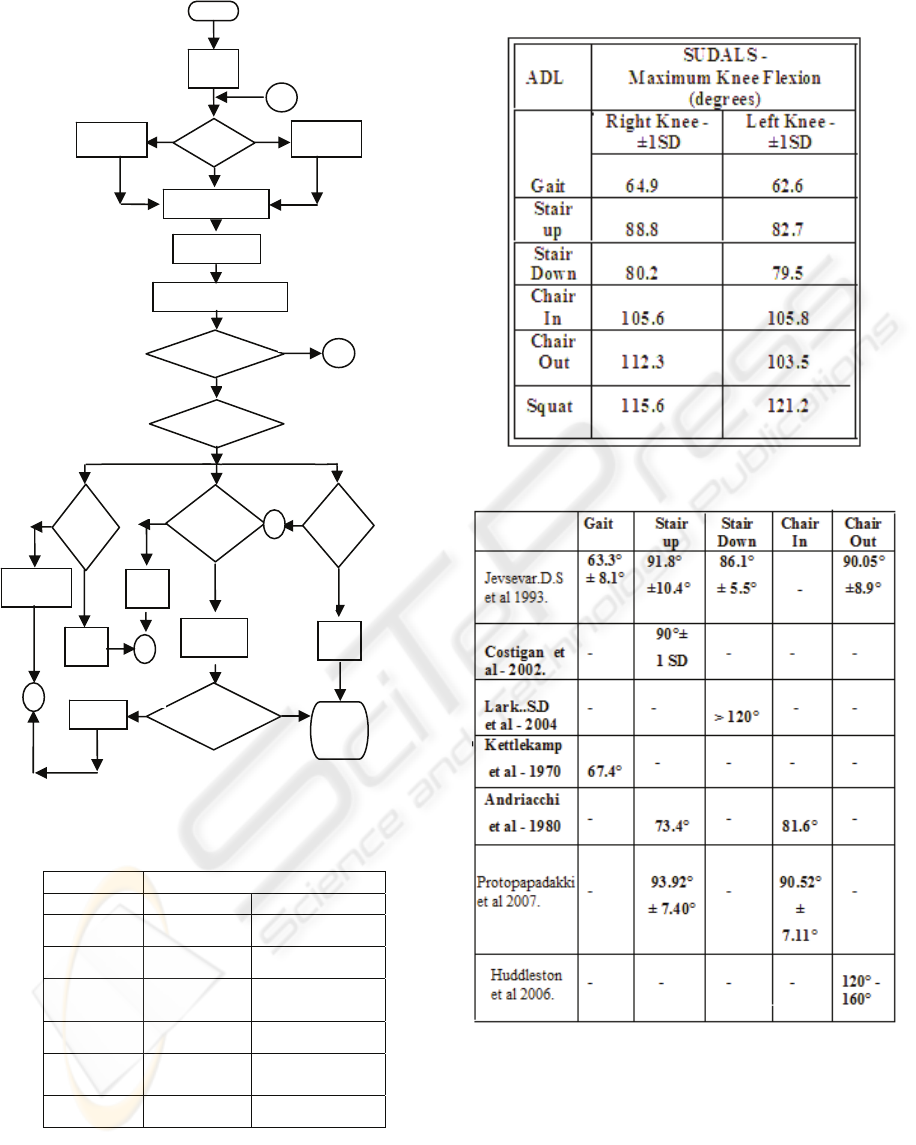
Figure 2: System functional flowchart.
Table 1: Knee ROM during ADL from SUDALS.
ADL SUDALS - excursion
Left Knee Right Knee
Gait 66.0° 66.4°
Stair up 71.3° 71.8°
Stair
Down
69.7° 61.5°
Chair in 101.7° 100.9°
Chair
Out
102.4° 107.1°
Squat 116.4° 111.7°
Table 2: Knee Flexion angles during ADL from SUDALS.
Table 3: Knee flexion angles from literature.
2.5 Discussion
The system described here was able to record, store
and transmit the data corresponding to the ADL.
Our results indicate that, the average maximum
knee flexion angle for all the 10 subjects during the
above mentioned ADL lies within the results
published in the literature as shown in Table3.
Transmit
Start
Switch
on
s
y
ste
m
Record
/Zero?
Zeroing
Recording
Enable trigger via
Remote Control to
Start performing
desired function.
Enable trigger to stop
p
erformin
g
the functio
n
A
Is 1 recording
com
p
lete?
Scrap/
transmit/reset?
Scrap?
Transmit?
Reset?
Reset
Data
Transmit
Data
Scrap
Data
Has all
recordings
t
r
a
n
s
mi
tted?
Switch
off the
System.
Retransmit
Data
A
A
A
A
Reset
N
Y
N
Y
N
Y
N
Y
Y N
DEVELOPMENT OF STRATHCLYDE UNIVERSITY DATA LOGGING SYSTEM (SUDALS) FOR USE WITH
FLEXIBLE ELECTROGONIOMETERS
201
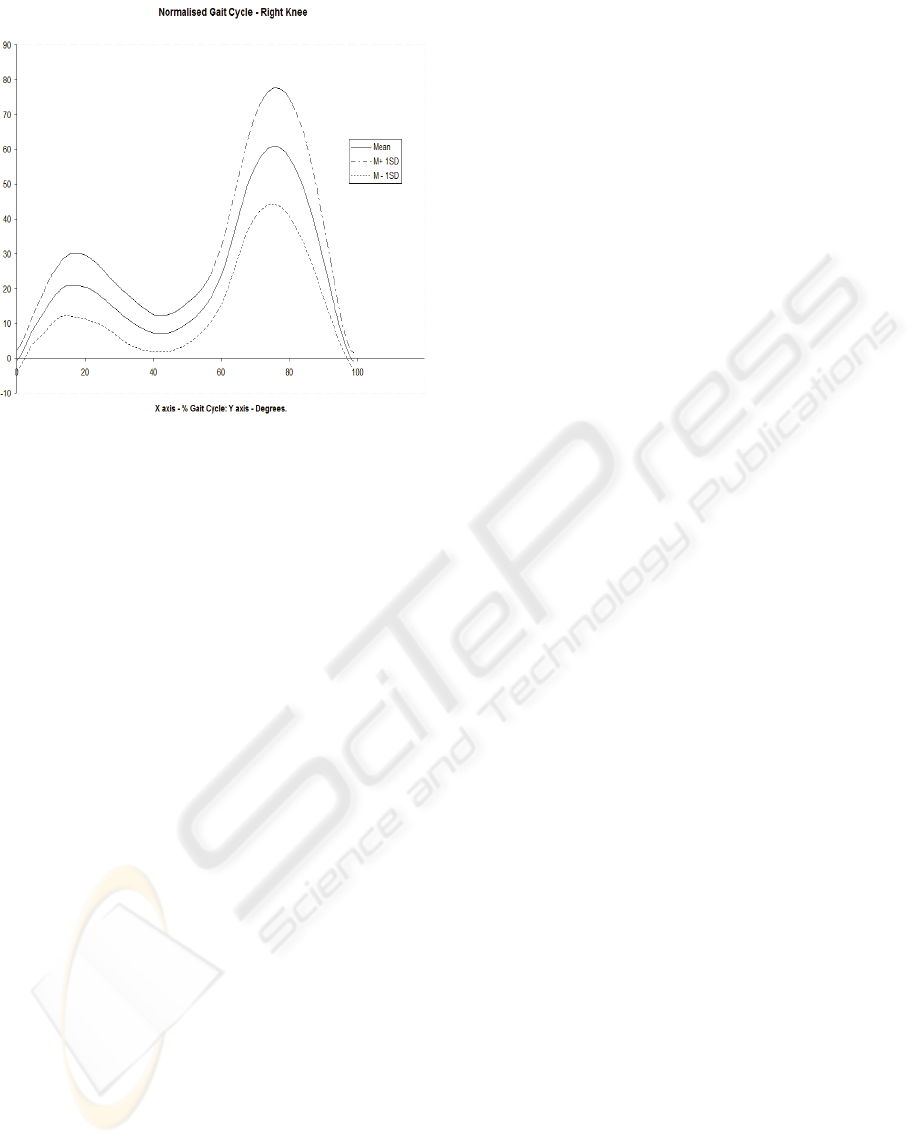
Figure 3: Normalized average Gait Cycle.
However, the knee flexion angles obtained
during squatting seem to be a little lower than the
values published in the literature. One of the
possible reasons for this could be the way in which
the subjects performed this activity. Though, the
subjects were shown what they were suppose to
perform during the process of recording, certain
subjects were unable to completely squat as it was a
difficult task and required a lot of effort. Due to this,
certain subjects performed half squat instead of a
complete squat. As a result, the knee flexion angle
recorded during this activity would be different from
those reported by Wyss.U et al - 2003, where the
subjects have performed a complete squat.
Moreover, most of the authors, other than
Huddleston.J et al - 2006, haven’t used flexible
electrogoniometer for measuring the knee flexion
angles. At the same time, though these authors have
reported the maximum knee flexion angles during
ADL, none of them have reported the knee
excursion of the subjects during these activities. On
the other hand, most of the studies by Rowe.P.J et al
– 2005, have reported the obtained knee excursion
during various ADL, but most of his studies are
concerned with the follow-up of TKA and elderly
population. Hence, the results from this study of
young healthy subjects were unable to be compared
with those published by Rowe et al. Most of the day
to day activities can be accomplished in less than a
minute.
Evidently, during our experimentation, we
noticed that the time taken to complete a single trial
of all the above mentioned six ADL by all the
subjects was less than a minute. Henceforth, despite
the usage of a 512 KB SRAM as prescribed by the
manufacturers of the evaluation board, we were able
to record, store and transmit the biomechanical
motions corresponding to six ADL with a little
difficulty. This ability to record, store and then
rapidly transmit the data facilitates data collection in
a free living environment and enables the user to
check whether the data recorded is reliable or not. In
this case, the user can re-record the activity
immediately unlike the commercially available
Biometrics data acquisition systems with flash
memory, where the user has to wait until the entire
data collection process is completed to check for
reliability and reproducibility of the data.
Currently, most of the portable data acquisition
systems that are used with flexible
electrogoniometer do not facilitate remote control
operation. Consequently, every time the users have
to physically change the settings of the data logger
such as starting, stopping or resetting; once it’s
being worn by the subjects. However, we were able
to control the entire process of data collection by
staying at a convenient distance of less than a foot
from the subjects. This would not only avoid any
physical contact with the subjects, but at the same
time, it would also minimize the degree of
inconvenience to the subjects. None of our subjects
reported any discomfort with SUDALS during the
process of data collection. Due to high power
draining application (wireless transmission of data),
we have used 6 x 1.2 V AA high wattage batteries of
2400 mah in our system. Further, unlike the
commercially available systems, SUDAL also has a
provision similar to the car battery charger for
recharging the batteries without removing them from
the system. Charging these batteries for 2 hours
enables us to use the system for more than 8 hours.
Though our system doesn’t facilitate real time
waveform display, simultaneous data collection and
transmission almost replicates those systems with
real time waveform display. Thus, the users would
be able to analyze the transmitted data stored in the
form of excel files. Figure 4 shows the usage of
SUDALS in an experimental set up.
3 CONCLUSIONS
In summary, the system worked without any
technical difficulties and was able to accurately
measure the knee flexion/extension during activities
of daily living in healthy subjects. The results of the
present study in conjunction with the literature
review support the use of SUDALS together with
BIODEVICES 2009 - International Conference on Biomedical Electronics and Devices
202

flexible electrogoniometers as a complimentary
instrument along with other functional assessment
questionnaires in providing objective data to the
clinicians. This would in turn help the rehabilitation
professionals to improve their intervention. In the
future, we plan to validate SUDALS against vicon
system (Gold standard) and use the system to
evaluate the functional outcomes of patients
following Total Knee Arthroplasty. The system can
be further developed to interface with mobile
devices and provide real time display of data
collected. Thus, a flexible, compact, powerful and
portable multi-channel data collecting system of
flexible electrogoniometry has been designed and
developed.
Figure 4: SUDALS mounted on a subject during
experimentation.
ACKNOWLEDGEMENTS
I would like to thank the University of Strathclyde
for funding my PhD with the Overseas research
student award (ORSA) and I would also like to
thank Mr. John Mcclean (Technician –
Bioengineering Unit, University of Strathclyde),
who has dedicated his time in assisting us with all
technical issues that were present during the
development of the system.
REFERENCES
Andriacchi.T.P. et al, vol 62-A, no: 5, 749-757, 1980. A
study of lower-limb mechanics during stair climbing,
Journal of bone and joint surgery.
Costigan.P.A et al, vol16, 31-37, 2001. Knee and hip
kinetics during normal stair climbing. Journal of Gait
and posture
Huddleston.J et al, 3:21, 2006. Ambulatory measurement
of knee motion and physical activity: preliminary
evaluation of a smart activity monitor. Journal of
neuroengineering and rehabilitation
Jevsevar.D.S et al, vol73, no: 4, 1993. Knee kinematics
and kinetics during locomotor activities of daily living
in subjects with knee arthroplasty and in healthy
control subjects. Journal of physical therapy
Kettlekamp et al, vol 52, 775-790, 1970. An
electrogoniometric study of knee motion in normal
gait. Journal of bone and joint surgery
Lark S.D et al, vol 91, 287-295, 2004. Knee and ankle
range of motion during stepping down in elderly
compared to young men. European journal of applied
physiology
Protopapadakki.A. et al, vol22, 203-210, 2007, Hip, Knee,
ankle kinematics and kinetics during stair ascent and
descent in healthy young individuals, Clinical
Biomechanics.
Rowe P.J et al, vol 87, no: 9, 479 – 487, 2001. Validation
of FEG as a measure of joint kinematics. Journal of
Physiotherapy
Rowe P.J et al, vol13, no: 2, 131-138, 2005.The effect of
TKA on joint movement during functional activities
and joint range of motion with particular regard to
higher flexion users. Journal of Orthopedic surgery
Wyss.U et al, 2003, High range of motion activities of
daily living: Differences in the kinematics between
Hong Kong and Chennai, India Subjects. ISB XXth
Congress – ASB 29
th
Annual Meeting, Ohio
Zhu.H et al, vol 38, No: 7, July 1991.A Microprocessor-
Based Data acquisition system for measuring plantar
pressures from ambulatory subjects. IEEE
TRANSACTIONS ON Biomedical Engineering
Zhang.Z&Liu.P, 2004. Application of bluetooth
technology in ambulatory wireless medical
monitoring. 4th international conference on
microwave and millimeter wave technology
proceedings
DEVELOPMENT OF STRATHCLYDE UNIVERSITY DATA LOGGING SYSTEM (SUDALS) FOR USE WITH
FLEXIBLE ELECTROGONIOMETERS
203
