
TOWARDS AN AUTOMATIC DIAGNOSIS SYSTEM
FOR ACUTE ABDOMINAL PAIN
Support Vector Machines for the Diagnosis of Diverticulitis
and Non-specific Abdominal Pain
Malin Bj
¨
ornsdotter
˚
Aberg
Institute of Neuroscience and Physiology, University of Gothenburg, Box 432, SE-405 30 G
¨
oteborg, Sweden
Kajsa Nalin
Centre of Interdisciplinary Research/Cognition/Information, SE-405 30 G
¨
oteborg, Sweden
Lars-Erik Hansson
Department of Surgery, Sahlgrenska University Hospital/
¨
Ostra, SE-416 85 G
¨
oteborg, Sweden
Helge Malmgren
Department of Philosophy, University of Gothenburg, SE-405 30 G
¨
oteborg, Sweden
Keywords:
Support vector machines, computer-aided diagnostics, acute abdominal pain.
Abstract:
The process of medical diagnosis is highly complex, and automatic decision support systems are appealing. In
this study we investigate the feasibility of automating one such decision-making process, namely the diagnosis
of patients seeking care for acute abdominal pain, and, specifically the diagnosis of acute diverticulitis. We
used a linear support vector machine (SVM) to classify diverticulitis from all other reported cases of abdomi-
nal pain and from the important differential diagnosis non-specific abdominal pain (NSAP). Using a database
containing 3 337 patients, the SVM obtained results comparable to those of the doctors. The distinction be-
tween diverticulitis and non-specific pain was substantially better for the SVM. Here the doctor achieved a
sensitivity of 0.714 and a specificity of 0.963. When adjusted to the physicians results, the SVM sensitiv-
ity/specificity was higher at 0.714/0.985 and 0.786/0.963 respectively. Age was found as the most important
factor for diagnosis, closely followed by C-reactive protein level and various pain indicators on the left hand
side. Thus, the support vector machine is a promising tool in the diagnosis of acute abdominal pain.
1 INTRODUCTION
The process of medical diagnosis and decision-
making, that is, the classification of patients into
disease groups based on various symptoms, is a
highly complex problem – as evidenced by the near
decade-long training required by specialist physi-
cians. Computer-based decision support systems are
therefore appealing tools in medical diagnostics, and
in this study we investigate one such decision-making
process, namely the diagnosis of patients seeking care
for acute abdominal pain (AAP).
Emergency ward doctors face a highly demand-
ing situation, where medical decisions with substan-
tial impact on patients must be made under time
pressure. The large number of potentially relevant
physical measurements, from blood factors to face
color, in combination with a stressful situation yields
a challenging decision-making process. Moreover,
physicians have reported lack of relevant experience
and continuous feedback among other factors that af-
fect the decision-making process negatively (Nalin,
2006). In addition, disease symptoms are highly vari-
able between individuals, leaving the doctor to rely
heavily on experience (Hansson, 2002).
Standardized, computer-based decision support
systems, automatically identifying typical disease
patterns in patient data, are thus appealing as a com-
plement to the trained physician. These systems
generally consist of computer models, or classifiers,
which are trained to discover patterns related to a
given disease in supplied patient data where the final
51
Björnsdotter Åberg M., Nalin K., Hansson L. and Malmgren H. (2009).
TOWARDS AN AUTOMATIC DIAGNOSIS SYSTEM FOR ACUTE ABDOMINAL PAIN - Support Vector Machines for the Diagnosis of Diverticulitis and
Non-specific Abdominal Pain.
In Proceedings of the International Conference on Health Informatics, pages 51-57
DOI: 10.5220/0001546200510057
Copyright
c
SciTePress

diagnosis is known. The classifiers are then applied
to new patients, where an instantaneous diagnosis is
made in order to assist the doctor.
Results on computer-aided diagnosis of abdomi-
nal pain were reported as early as in 1972, where de
Dombal reported a surprisingly high diagnostic accu-
racy (91.8% vs. 79.6%) using decision support com-
pared with the unaided examination (de Dombal et al.,
1972). Moreover, a large British multi-center study
with more than 16.000 patients confirmed the utility
of computer aided diagnostic with accuracies of 65%
vs. 46% (Adams et al., 1986).
A common acute abdominal disease, often a rea-
son for emergency hospital admission – especially in
elderly patients — is diverticulitis of the colon (Am-
brosetti et al., 1994; Ferzoco et al., 1998; Young-
Fadok et al., 2000; Laurell et al., 2006). The diag-
nosis is typically made at the emergency department,
based on both medical history and clinical indica-
tions. The clinical presentation of acute diverticulitis
was recently described by Laurell and colleagues, as
well as the natural short-term development of the dis-
ease (Laurell et al., 2007). Primary diagnosis sensi-
tivity, by the physician, was reported to be 64%, with
a specificity of 97%. Moreover, Laurell et. al. iden-
tified non-specific abdominal pain (NSAP) as one of
the most important differential diagnoses. For NSAP,
the primary diagnosis sensitivity was reported to be
43%, with a specificity of 90%.
In the current study, we investigate the feasibility
of using a decision support system for the automatic
diagnosis of acute diverticulitis, contrasted with all
other reported cases of abdominal pain and from the
diagnosis category non-specific abdominal pain. Us-
ing a state-of-the-art classifier, namely (linear) sup-
port vector machines and feature selection, we also
attempt to understand the underlying factors that are
key to identifying diverticulitis.
2 METHODS
2.1 Data Acquisition
Mora Hospital in northern Sweden is a district hos-
pital serving a population of 87 000 individuals, pro-
viding full emergency services. During the period of
February 1997 to June 2000, all patients older than
one years of age admitted to the hospital with abdom-
inal pain of duration of up to 7 days were registered
in a database. Details were registered according to a
standardized form for history, clinical indications and
laboratory results. The attending physician suggested
a diagnosis, and a final diagnosis was given when the
patient left the hospital. A definitive diagnosis was
later established by a follow-up study of the patient’s
journal. Data for 3 337 patients was thus acquired.
A non-reported value can be assumed irrelevant
and within the normal range, and missing data was,
therefore substituted by estimated normal values.
Moreover, normal values can be used in practical ap-
plications of decision support systems, without any
knowledge of the statistics of the present sample.
Thus, a data-set consisting of 3 337 patients with
117 measured variables and an initial diagnosis by a
trained physician was obtained. Out of the 3 337 pa-
tients, 148 obtained diverticulitis as a definitive (ret-
rospective) diagnosis, whereas 1340 were diagnosed
as having non-specific abdominal pain. In the train-
ing of the automatic system and in the performance
analysis, these definitive diagnoses were the desired
output of the system.
2.2 Support Vector Machines
Support vector machines (SVMs) is a type of clas-
sification algorithm which maximizes the geometric
margin between the data classes and the separating
hyperplane (Suykens et al., 2002).
Given our training data:
D = {(x
i
, y
i
)|x
i
∈ R
p
, y
i
∈ {−1, 1}}
n
i=1
(1)
where y
i
is the disease category (-1 or 1) to which pa-
tient x
i
belongs, the hyperplane that maximally sepa-
rates the data points must fulfill the following inequal-
ities:
ω · x
i
+ b ≥ d for all i where y
i
= 1 (2)
ω · x
i
+ b ≤ −d for all i where y
i
= −1 (3)
where ω is the weight vector, b is the bias and d is the
separating margin.
The SVM model is trained by adapting it’s
weights to the data at hand, using an algorithm
that finds the optimal hyperplane that maxi-
mizes the margin d. Here, the matlab toolbox
LS-SVMlab, developed by the group SCD/sista
in the department ESAT at the KULeuven,
Belgium (Suykens et al., 2002), available at
http://www.esat.kuleuven.be/sista/lssvmlab/, was
used.
2.3 Performance Measure
As a fitness measure indicative of classification per-
formance, the receiver operating characteristic curve
(ROC; a plot of the sensitivity versus 1-specificity for
varying classifier thresholds) was computed and the
area under the curve (AUC) is obtained. Larger AUC
HEALTHINF 2009 - International Conference on Health Informatics
52

values indicate better classifier performance. More-
over, the specificity and sensitivity of the results were
also computed for comparison with the physician’s
initial diagnosis.
In the Results section, histograms representing the
discrimination ability of the classifier are presented.
These are produced by plotting the estimated classi-
fier output (aiming towards -1 or 1, that is, class 1 or
class 2) frequencies color-coded according to the true
class, that is, the better the classification performance,
the more clustered is either color and the more dis-
tinctly separated are the clusters. The ROC is plotted
in these figures as well, further illustrating classifier
performance.
2.4 Variable Ranking
Although the database is substantial and there is a sat-
isfactory number of instances (patients) compared to
the number of available variables, feature selection,
that is, the identification of a lower number of highly
discriminatory features, can boost classification per-
formance (Bellman, 1961; Blum and Langley, 1997).
A simple method was therefore implemented for
variable ranking and subsequent selection as follows:
v
i
= abs(
µ
0
− µ
1
σ
0
+ σ
1
) (4)
where µ
0
and µ
1
represent the mean value of variable
i over the patterns (patient data) belonging to class 0
and 1 respectively, and σ
0
and σ
1
are the standard de-
viations within each class. The variable ranking value
is thus a measure of variable stability, over the pat-
terns, as well as how well each variable taken by itself
separates the data classes. For subsequent variable
selection, the variables were thus ranked and a given
number was selected accordingly (see the results sec-
tion, figure 2).
2.5 Class Imbalance Correction
Compared to the remaining diseases, diverticulitis
is heavily under-represented (148 instances out of
3 337), and this also holds in relation to the cate-
gory of non-specific abdominal pain (1340). In or-
der to lessen the effect of the imbalance a simple
under-sampling scheme was used, where a number of
instances (patients) of the over-represented category
was removed until both categories were equally rep-
resented.
3 RESULTS
The patients were divided into a training (90%) and
a validation data set (10%), after which the training
data was adjusted for class imbalance. All results re-
fer to the validation data set, unless otherwise spec-
ified. The support vector machine (SVM) classifier
was trained on the training data, and subsequently
applied to the validation data, for all variable sub-
sets formed from the feature ranking, ranging from
1 through all 117 variables. The performance of the
physician’s initial diagnosis was also computed on the
same datasets.
3.1 Classification Performance
The classification performance results are summa-
rized in table 1. First, the SVM was applied to attempt
discrimination between diverticulitis and the pool of
all other diseases for a varying number of included
variables. A maximum AUC of 0.95 was found for
64 variables, and a histogram illustrating the result-
ing discrimination ability of the classifier is shown in
figure 1A. At this optimal point, the SVM obtained a
substantially higher sensitivity of 1.00 – that is, cor-
rectly identified all of the diverticulitis cases – than
the physician at 0.571. However, as is obvious from
figure 1A, given this high sensitivity the specificity
suffers, and a high amount of false positives are in-
evitable: the SVM obtained a specificity of 0.823, as
opposed to the doctor who produced a much higher
specificity of 0.987. When adjusted to the physician’s
values, the SVM achieved a sensitivity/specificity of
0.571/0.981 (at 105 variables) and 0.5/0.987 (at 111
variables) respectively – lower than the physician in
both cases.
Non-specific abdominal pain (NSAP) appears
more difficult to distinguish from the pool of all other
diseases than diverticulitis. Not even the SVM train-
ing data (figure 2B) effectively achieves separation
between the classes, and the highest SVM valida-
tion sensitivity and specificity are low at 0.687 and
0.721 respectively. Similarly, the doctor’s diagnosis
achieves a very low sensitivity of 0.455 but, again, a
high specificity of 0.909. Also here, when adjusted to
the physician’s results, the sensitivity/specificity ob-
tained was lower for the SVM than the physician at
0.455/0.878 (at 16 variables) and 0.41/0.909 (at 16
variables).
The discrimination between diverticulitis and non-
specific pain, however, was substantially better. The
doctor achieved a sensitivity of 0.714 and a speci-
ficity of 0.963, whereas the best SVM resulted in a
substantially higher sensitivity of 1 and a satisfactory
TOWARDS AN AUTOMATIC DIAGNOSIS SYSTEM FOR ACUTE ABDOMINAL PAIN - Support Vector Machines
for the Diagnosis of Diverticulitis and Non-specific Abdominal Pain
53
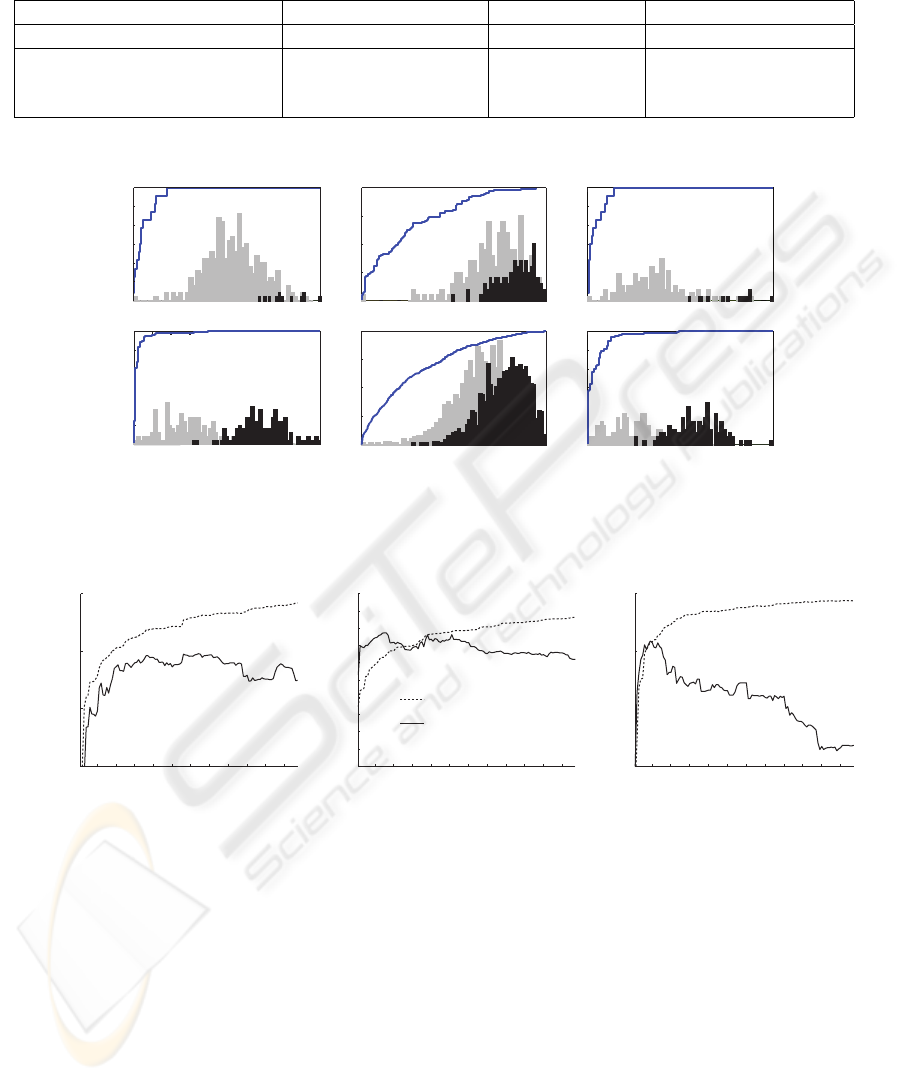
Table 1: Summary of performance results for the diagnosis of diverticulitis and non-specific abdominal pain (NSAP): sensi-
tivity/specificity.
diverticulitis vs. others NSAP vs. others diverticulitis vs. NSAP
Physician 0.571/0.987 0.455/0.909 0.714/0.963
SVM at maximum AUC 1/0.823 0.687/0.721 1/0.858
SVM at physician’s sensitivity 0.571/0.981 0.455/0.878 0.714/0.985
SVM at physician’s specificity 0.5/0.987 0.41/0.909 0.786/0.963
Diverticulit vs all others
Non-specific vs all others
Diverticulit vs non-specific
Train data Validation data
A B C
Figure 1: Histogram illustrating the separability of A) Diverticulitis (dark) vs. all other diseases (light), B) Non-specific
abdominal pain (dark) vs. all other diseases (light) C) Diverticulitis (dark) vs. non-specific abdominal pain (light). The blue
line represents the receiver operating characteristic curve.
0.6
0.64
0.68
0.72
0.76
0.8
Non-specific vs all others
0.85
0.9
0.95
1
Diverticulitis vs Non-Specific
Diverticuluitis vs all others
0.85
0.9
1
10 30 50 70 90 110
Number of included variables
Performance (AUC)
0.95
Validation data
Training data
10 30 50 70 90 110
Number of included variables
10 30 50 70 90 110
Number of included variables
A B C
Figure 2: Performance as a function of the number of included variables for A) Diverticulitis vs. all other diseases, B)
Non-specific abdominal pain vs. all other diseases C) Diverticulitis vs. non-specific abdominal pain.
specificity of 0.858 (AUC: 0.959). As can been seen
in figure 1C, the validation data is distinctly separa-
ble. Also, when adjusted to the physicians levels, the
SVM sensitivity/specificity was higher in both cases
at 0.714/0.985 (at 44 variables) and 0.786/0.963 (at
19 variables), respectively.
3.2 Variable Selection
The variable selection proved to have substantial im-
pact on all data sets (figure 2). For the discrimination
between diverticulitis and all other diseases, the ad-
dition of variables from 1 through 30 had a large ef-
fect on classifier performance, after which it declined.
Similarly, on the non-specific abdominal pain vs. all
other diseases task, going from one to two features
shows a dramatic increase in performance, whereas
further addition does not have a large effect. On the
other hand, for the more specific case of diverticuli-
tis vs. non-specific abdominal pain, it is obvious that
some variables contain large amounts of information
regarding the categories – there is a sharp increase
in performance up to nine variables, and an equally
sharp decrease after the addition of 15 more variables.
A closer inspection of the highly rated features
(see table 2-4) reveals that, for any data set combi-
HEALTHINF 2009 - International Conference on Health Informatics
54
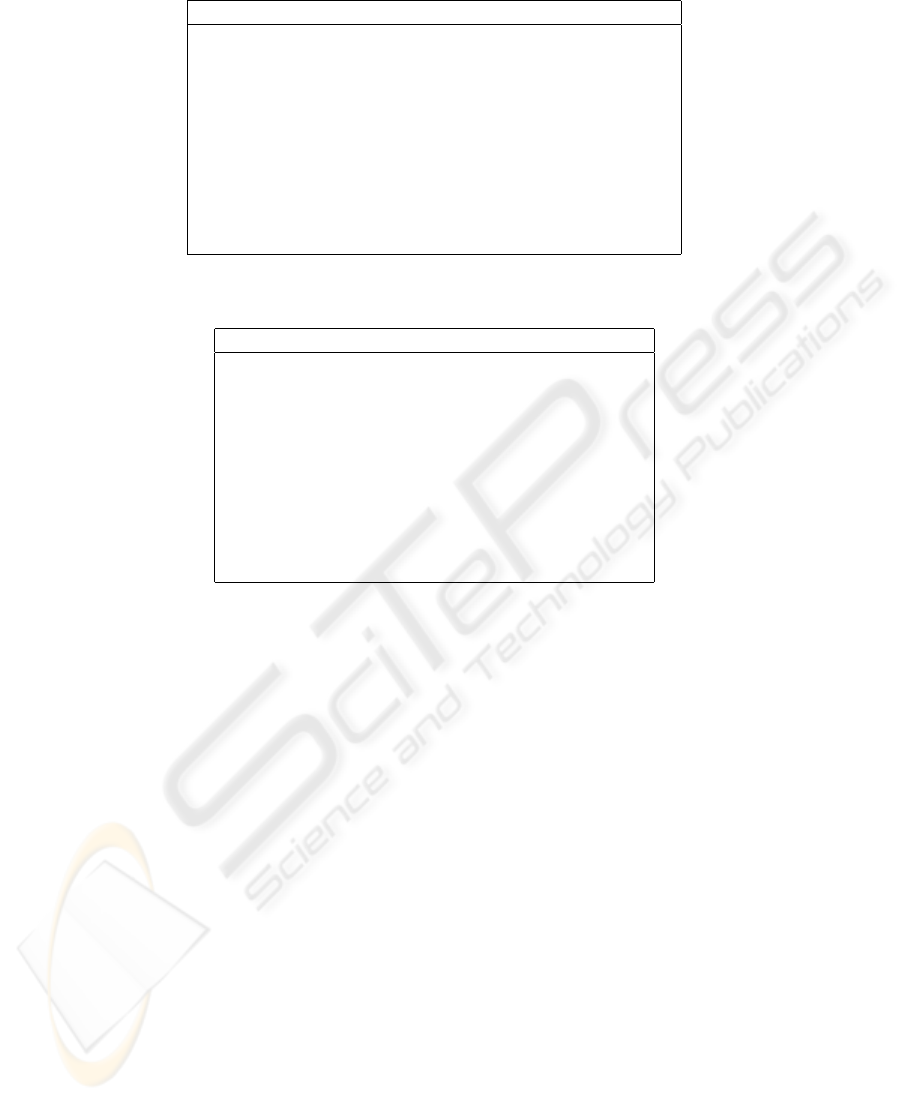
Table 2: The top 10 ranked variables for diverticulitis vs. all other diseases.
Variable Weight
Age 1.22099
C-reactive protein level 1.05363
Initial pain localization; left lower quadrant 0.917118
Tenderness on palpation 0.901306
Current pain localization; lower left quadrant 0.89903
Current pain localization; right upper quadrant 0.634565
Initial pain localization; right upper quadrant 0.604262
Vomiting 0.588099
Previous abdominal surgery 0.562905
Abdominal scars 0.551697
Table 3: The top 10 ranked variables for non-specific abdominal pain (NSAP) vs. all other diseases.
Variable Weight
Age 0.605346
C-reactive protein level 0.369473
Serum bilirubin level 0.350293
Systolic blood pressure 0.303903
Decrease/absence of bowel movements 0.286566
Visible bowel movements 0.28654
Development of pain intensity; increase 0.277085
Localized swelling 0.267
S-amylase level 0.264904
Serum alanine aminotransferase level 0.251346
nation, age is the most important factor for discrim-
ination, closely followed by C-reactive protein level.
As can be expected, similar variables are important
for the discrimination between diverticulitis and all
other diseases and diverticulitis vs. non-specific ab-
dominal pain, namely: initial pain localization (both
in the left lower quadrant and the right upper quad-
rant), current pain localization (in the lower left quad-
rant) and tenderness on palpation (in the left lower
quadrant). The focus on left side pain in the diag-
nosis of diverticulitis agrees with previous research
(Laurell et al., 2006). However, in the case of non-
specific abdominal pain vs. all other diseases, other
variables, predominantly various fluid measurements,
are highly rated. Moreover, the resulting rating coef-
ficients are much smaller, thus indicating lower dif-
ferentiation between variables.
4 DISCUSSION
We have investigated the utility of using a decision
support system for the computer aided diagnosis of
acute diverticulitis and non-specific abdominal pain
(NSAP), as well as for the discrimination between the
two, using the Mora acute abdominal pain database.
The general performance of the SVM was compa-
rable to that of the doctor. Moreover, both sensitivity
and specificity were higher than those of the physi-
cian in the distinction between diverticulitis and non-
specific abdominal pain.
The discrimination between diverticulitis and the
pool of other diseases, as well as that between non-
specific pain and the other diseases, was substantially
worse than the differentiation between the two disease
categories. This suggests that incorporating known
information about the other disease categories, in-
cluding their respective distribution, in the training
of the classifier model can aid in the subsequent di-
agnosis of new cases. This can, for example, be
achieved using an ensemble of classifiers. For the
case of multi-class data, where the diagnosis of all
patients and thus all diseases is desired, this is, more-
over, required for inherently binary classifiers such
as SVMs. Standard schemes for ensemble encoding
include the one-against-all and one-against-one ap-
proach. The latter is more computer-intensive than
the former, but typically yields better results. Im-
portantly, it also provides insight into the distinction
between diseases. Moreover, the one-against-one is
a more well-defined problem, contrasting data cate-
TOWARDS AN AUTOMATIC DIAGNOSIS SYSTEM FOR ACUTE ABDOMINAL PAIN - Support Vector Machines
for the Diagnosis of Diverticulitis and Non-specific Abdominal Pain
55
Table 4: The top 10 ranked variables for diverticulitis vs. non-specific abdominal pain.
Variable Weight
Age 1.51921
C-reactive protein level 1.12222
Initial pain localization; left lower quadrant 1.03731
Current pain localization; lower left quadrant 0.944773
Tenderness on palpation; left lower quadrant 0.885332
Development of pain intensity; increase 0.762057
Current pain localization; right upper quadrant 0.677884
Local muscular defence 0.674493
Leukocyte level 0.664661
Initial pain localization; right upper quadrant 0.657553
gories with inherent similarities and differences, as
was evidenced by the findings in our study. The one-
against-all scheme, on the other hand, is more relevant
to the problem of diagnosis.
The class imbalance was adjusted by simple
under-sampling of the majority class. More sophis-
ticate methods could be employed to this end, such as
the SMOTE algorithm (Chawla et al., 2002).
The simple feature ranking and subsequent selec-
tion utilized in this study proved to be effective in
boosting classifier performance. However, more suit-
able approaches can be used to obtain optimal vari-
able subsets, such as evolutionary algorithms (Mar-
chiori et al., 2007;
˚
Aberg et al., 2008). Moreover,
there is reason to believe that non-linear relation-
ships pertaining to the disease category exist between
some parameters, and reducing the complexity of the
data structures can potentially allow for better perfor-
mance with non-linear classifiers (
˚
Aberg and Wess-
berg, 2007).
5 CONCLUSIONS
Automatic computer-based disease classification is a
promising tool for the diagnosis of acute abdominal
pain, but requires substantial research before a clin-
ical implementation is feasible. The support vector
machine is highly suitable for the discrimination be-
tween binary disease categories, and achieved results
comparable to the medical doctor. Moreover, the clas-
sifier obtained higher sensitivity and specificity than
the physician in the distinction between diverticulitis
and non-specific abdominal pain. Age and C-reactive
protein level, as well as left-hand side pain sensations,
were identified as important factors for the classifica-
tion of diverticulitis.
REFERENCES
˚
Aberg, M. C., L
¨
oken, L., and Wessberg, J. (2008). An evo-
lutionary approach to multivariate feature selection for
fMRI pattern analysis. Proceedings of the Interna-
tional Conference on Bio-inspired Systems and Signal
Processing.
˚
Aberg, M. C. and Wessberg, J. (2007). Evolutionary op-
timization of classifiers and features for single trial
EEG discrimination. BioMedical Engineering Online,
6(32).
Adams, I. D., Chan, M., Clifford, P. C., Cooke, W. M.,
Dallos, V., de Dombal, F. T., Edwards, M. H., Han-
cock, D. M., Hewett, D. J., and McIntyre, N. (1986).
Computer aided diagnosis of acute abdominal pain: a
multicentre study. British Medical Journal (Clinical
research ed.), 293(6550):800–804.
Ambrosetti, P., Robert, J., Witzig, J., Mirescu, D., Mathey,
P., Borst, F., and Rohner, A. (1994). Acute left colonic
diverticulitis: a prospective analysis of 226 consecu-
tive cases. Surgery, 115(5):546–50.
Bellman, R. E. (1961). Adaptive Control Processes. Prince-
ton University Press, Princeton, NJ.
Blum, A. and Langley, P. (1997). Selection of relevant fea-
tures and examples in machine learning. Artificial In-
telligence, 97(1-2):245–271.
Chawla, N., Bowyer, K., Hall, L., and Kegelmeyer, W.
(2002). Smote: synthetic minority over-sampling
technique. Journal of Artificial Intelligence Research,
16:321357.
de Dombal, F., Leaper, D., Staniland, J., McCann, A.,
and Horrocks, J. (1972). Computer-aided diagnosis
of acute abdominal pain. British Medical Journal,
2(5804):9–13.
Ferzoco, L., Raptopoulos, V., and Silen, W. (1998). Acute
diverticulitis. The New England Journal of Medicine,
338(21):1521–6.
Hansson, L.-E. (2002). Akut Buk. Lund: Studentlitteratur.
Laurell, H., Hansson, L., and Gunnarsson, U. (2006). Acute
abdominal pain among elderly patients. Gerontology,
52(6):339–44.
HEALTHINF 2009 - International Conference on Health Informatics
56

Laurell, H., Hansson, L., and Gunnarsson, U. (2007). Acute
diverticulitis clinical presentation and differential di-
agnostics. Colorectal Disease, 6(9):496–501.
Marchiori, E., Moore, J. H., and Rajapakse, J. C., editors
(2007). A Genetic Embedded Approach for Gene Se-
lection and Classification of Microarray Data, volume
4447 of Lecture Notes in Computer Science. Springer.
Nalin, K. (2006). Den ideala kliniska beslutsprocessen. en
studie av arbetsprocessen p en kirurgisk akutmottagn-
ing/The ideal clinical decison process. a study of the
work process in an acute surgical ward. in swedish.
masters thesis. Masters thesis in Cognitive Science,
University of Gothenburg.
Suykens, J., Gestel, T. V., Brabanter, J. D., Moor, B. D., and
Vandewalle, J. (2002). Least Squares Support Vector
Machines. World Scientific.
Young-Fadok, T., Roberts, P., Spencer, M., and BG, W.
(2000). Colonic diverticular disease. Current Prob-
lems in Surgery, (37):459514.
TOWARDS AN AUTOMATIC DIAGNOSIS SYSTEM FOR ACUTE ABDOMINAL PAIN - Support Vector Machines
for the Diagnosis of Diverticulitis and Non-specific Abdominal Pain
57
