
APPLICABILITY OF MOBILE PHONES FOR
TELE-DERMATOLOGY
A Pilot Study
Scheibböck Christian
1
, Dreiseitl Stephan
2
1
Vienna University of Technology, Karlsplatz 13, 1040 Vienna, Austria
2
Department of Software Engineering, Upper Austria University of Applied Sciences at Hagenberg
Softwarepark 11, 4232 Hagenberg, Austria
Binder Michael
Department of Dermatology, Division of General Dermatology, Medical University of Vienna, Austria
Keywords: Telemedicine, Tele-dermatology, Mobile phones, Camera phones, Colour fidelity, MMS, Illumination.
Abstract: Examination in dermatology is primarily based on visual inspection. Since this visual information can be
stored and transmitted easily through digital images, tele-consultation and tele-diagnosis are predestined
methods especially in the field of dermatology. Nowadays mobile phones represent the most important
communication tool around the world. To study how the process of acquiring, transmitting and diagnosing
images can be implemented by using cheap and widely available devices, such as mobile phones, we
conducted several experiments at the Medical University of Vienna. Material and Methods: In a study
patients were asked to take one or more photos of their dermatoses with the camera of a mobile phone.
Images were transmitted electronically by using the MMS function of the phones. All participants were
examined routinely at the outpatient department, establishing the gold standard diagnosis. Three different
phone models were evaluated with regard to colour fidelity, illumination effects, and terms of resolution.
Images for tests were produced at not standardized conditions. Results:
In all three phones high resolution
images are compressed. Resolution was skilled down to 640x480 while sending via MMS. Colour fidelity
was different depending on the manufacturer. Colour fidelity increased proportional with increasing
illumination.
1 INTRODUCTION
The use of telemedicine, especially tele-
dermatology, can be of great advantage for patients
and doctors. The following points show where tele-
dermatology can be of use:
Outlying territories with a low density of
dermatologists
Patients without access to a car or public
transportation
Patients who want to save time
Patients who are in foreign countries and want
to receive a diagnosis and therapy advice in
their native language
Patients who want to avoid or shy personal
contact to doctors due to several reasons (e.g.
religion, agitation, shame, etc.)
Patients who want to obtain a fast (and
reliable) second opinion
Some examples where tele-dermatology can be
of use for doctors:
Second opinion: with telemedicine it is
possible to receive another specialized opinion
without time delay
Temporally optimized advanced training:
images can be stored and used as instruction
material for medical students and doctors
Further possibilities of tele-dermatology:
Selection of patients - the urgency of cases
can be judged, in order to achieve a faster and
more efficient treatment (triage)
474
Christian S., Stephan D. and Michael B. (2009).
APPLICABILITY OF MOBILE PHONES FOR TELE-DERMATOLOGY - A Pilot Study.
In Proceedings of the International Conference on Health Informatics, pages 474-477
DOI: 10.5220/0001550504740477
Copyright
c
SciTePress

Optimal resource use through purposeful
transfer: patients mustn’t wait for
investigation at a “mismatching” department.
They are passed on to the appropriate
specialists.
Follow-up assistance: the patient can receive
further assistance economically and fast (e.g.
wound inspection)
The university clinic has the advantage of always
being on the newest state of the art and science. This
results in some disadvantages for the patient, e.g.
long waiting times for an appointment at the
outpatient’s department. Particularly in dermatology
there is the possibility of reducing these waiting
periods to achieve a better time management. The
patient can photograph his skin lesions at any
location – either through a digital or mobile phone
camera, and then forward the provided image by
MMS or email to a dermatologist, who examines it.
Tele-dermatology has the potential to optimize
time management. Costs can be reduced in
comparison to the actual standard diagnostic way.
Efficiency of the outpatient clinics could be
increased with regard to economic considerations
and patient friendliness.
Recently published studies showed that cell
phones can be used in tele-dermatology. They are
very useful devices to produce photos easily. But
cell phones are not subject to medical device law. A
standard for produced images does not exist. So it
was necessary to test some cell phones and analyze
the produced images.
The impulse of this research was a tele-
dermatological pilot study at the Department of
Dermatology, Division of General Dermatology.
Photos were produced with cell phone cameras. The
major question was: Can camera phones produce
acceptable image quality for dermatology.
Before the study we analyzed three cell phones
with regard to quantitative and quality criteria.
1.1 Previous Work
Herrmann et al. got throughout positive results in a
study about tele-dermatological (TD) and face to
face (FTF) consultation. In a comparison of
diagnoses from 120 patients by tele-dermatologists,
agreement was from 46.4% respectively 70,2%
without additional information and 64,3%
respectively 76,6% with additional information. This
shows the absolute necessity of additional
information. Dermatologists felt certain with their
diagnoses in most cases. Sureness was evaluated
with a visual analogical scale from 0 to 10. Cases
difficult to assess with a tele-dermatologist were also
difficult for standard diagnoses and were therefore
identified with “doubtful diagnosis”. Furthermore,
image quality influenced the diagnosis. In 70% it
was possible to make a diagnosis. (Herrmann, 2005)
In 2004 Tai Khoa Lam tried to create photos
with two randomized mobile phones (Nokia 7650).
These photos were sent between a medical specialist
and an archivist. Photography was limited to the
hand trauma, radiographs or both. At the beginning
there was a discussion between the medical
specialist and the archivist who created a
management plan. After that, photos were sent via
mobile phone and multimedia. Now there was
another discussion and then the management plan
had to be modified. Within the following two
months 39 photos were sent. During the course of
the study there were four cases in which the
management plan had to be modified. (Lam TK,
2004)
Authors of „Telemedical Wound Care” devised a
study in which leg ulcers were photographed. 61 feet
were examined by three dermatologists. One of them
made FTF consultation and the other two were
responsible for mobile phones. They transmitted
images via e-mail. The result of the study was that
the image quality in 36 cases was “good” and in 12
cases “very good”. 50 of the involved parties felt
well and only one felt unwell. Three photos were of
poor-quality. (Braun RP, 2005)
In a cooperation of the Medical University of
Graz, Vienna and L’Aquila, diagnoses from camera
phone images and face-to-face dermatology were
compared. Two dermatologists examined these
images from 58 patients. In 48 patients a diagnosis
was provided. Six were immediately sent to a
dermatologist and four patients were advised to
come again a few days later.
During the following comparison of diagnoses in
41 cases, diagnosis was correct (full agreement). In
15 cases the diagnosis was wrong but still in the
same category of diagnoses (relative agreement). In
only three cases diagnosis was wrong
(disagreement). (Jauk B, 2006)
The Medical University of Graz (Austria) ran a
study researching the agreement between
teledermatology based on images from a cell phone
camera and face-to-face (FTF) dermatology. With a
quantity of 58 subjects two tele-dermatologists (TD)
analyzed the images produced. After checking, the
concordance between tele-diagnosis and FTF
diagnosis represented almost three-quarters (TD1:
71%, TD2: 76%). Nearly all diagnoses were in the
same diagnostic category (TD1: 97%; TD2: 90%).
(Ebner C, 2008).
APPLICABILITY OF MOBILE PHONES FOR TELE-DERMATOLOGY - A Pilot Study
475

2 MATERIAL AND METHODS
Image quality can be rated through different
methods. In this paper two kinds of analysis are
used. First an objective method with measurement
methods and second the subjective view of the
images.
2.1 Technical Methods
To acquire more information about colour fidelity,
illumination and MMS altering, some tests were
realized.
The tests involved three different cell phones.
Device 1 (D1) and Device 2 (D2) include a 3.2
megapixels camera. Device 3 (D3) includes a 5
megapixels camera and a “Tessar-lens” by order of
Carl Zeiss. These devices were selected randomly.
Tests were produced at the same settings and
conditions.
For photo analysis “Adobe Photoshop” was used
which produced histograms and relevant data.
Illumination was measured with “Minolta Auto
Meter IV F”. Scale unit is “exposure value” (ev)
which designates a number of combinations of glare
number (Relationship of the focal length f to the
diameter D of the entrance pupil) and exposure time,
which are equivalent to each other in photography
and photometry.
The colour fidelity test involves photographing a
single-coloured photo which was sent via mail.
Tolerance was 70. By the size of this parameter one
determines how large a colour area is in the selection
and the number of partly selected pixels increased or
reduced. (Selection range: 0-200)
Three series of tests were created at various
illuminations (5.3ev, 7.7ev and 9.1ev). Every
situation included 5 photos. The flash and the
camera light were always deactivated.
Every picture was analyzed with regard to
central pixel, mean pixel, standard deviation and
colour range. First a colour range was selected,
which includes the area with the most similar pixel.
In this area there is a central pixel and a mean pixel
with different standard deviations. All values are
derived from RGB spectrum.
2.2 Clinical Study
In a tele-dermatological pilot study at Department of
Dermatology, Division of General Dermatology,
Medical University of Vienna, 915 photos were
produced by 300 patients. Patients took photos of
their own dermatoses. If the dermatose was
unreachable, an assistant took the photo. Patients
only received a short instruction in the usage of the
mobile phone camera but they did not receive any
information how to obtain the best photo. Images
were created in a badly lit examination room without
any daylight.
3 RESULTS
3.1 Technical Results
The first test refers to colour fidelity. The following
three tables demonstrate the cumulative average
results of five photos per device. The “central pixel”
stands for the colour value which appears most in
contrast, “mean value” describes the average
brightness value. “Standard deviation” indicates how
strongly the brightness values vary. “Relative value”
is the amount of total pixel in percent. Central pixel
of template was 173 in RGB spectrum.
Table 1: Results at 5.3ev in a badly lit room.
central
pixel
mean
value
standard
deviation
relative
value
D1 150.80 151.35 23.74 94.44%
D2 83.20 90.80 22.17 99.03%
D3 140.80 139.52 13.97 73.69%
In Table 1 D1 and D3 nearly reached the original
pixel value. But D3 only includes 73.69% of the
mean value 139.52. D2 resulted in a mean pixel
value of 90.80 in an area of 99.03%.
Table 2: Results at 7.7ev with lateral illumination.
central
pixel
mean
value
standard
deviation
relative
value
D1 152.40 148.54 23.84 86.17%
D2 119.80 122.77 20.00 99.51%
D3 151.20 156.00 21.83 71.52%
With 7.7ev D1 and D3 reached a mean pixel value
of 148.54 (D1) or rather 156.00 (D3). D2 also
increased central pixel. It is about 122.77.
Table 3: Results at 9.1ev with vertical illumination.
central
pixel
mean
value
standard
deviation
relative
value
D1 150.60 148.95 24.14 88.91%
D2 77.80 101.97 44.44 90.57%
D3 160.00 163.37 16.46 56.48%
HEALTHINF 2009 - International Conference on Health Informatics
476
At maximum illumination (9.1ev) D1 reached a
mean value of about 148.95 (88.91% of image pixel)
and D3 reached 163.37 (only 56.48% of image
pixel). D2 reached a mean value of about 101.97.
Table 4: Average results at 5.3ev, 5.7ev and 9.1ev.
central
pixel
mean
value
standard
deviation
relative
value
D1 151,27 149,61 23,91 89,84%
D2 93,60 105,18 28,87 96,37%
D3 150,67 152,96 17,42 67,23%
In an area of 67.23% D3 took photos with a mean
standard deviation of 17.42. Mean pixel value was
nearly the original value. In contrast 96.37% at D2
had mean pixel of about 105.18. The average
standard was from 17.42 (D3) to 28.87 (D2).
Additional light sources can influence the
brightness distribution. In some areas in which light
reflect pixel, values are extremely falsified.
While sending MMS or email the original high
resolution photo stored on mobile phones will not
always remain unaffected. Usually, original images
were altered by lossy compression algorithms.
Images will be compressed, during sending via
MMS to a size of 640x480.
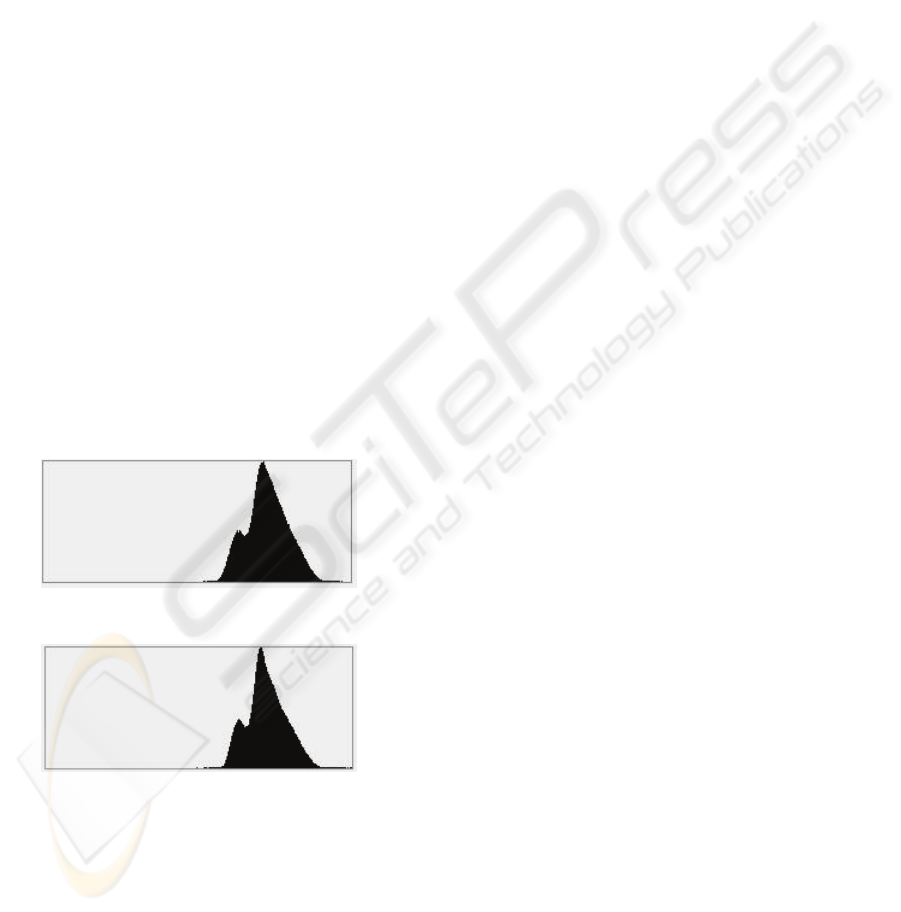
The following histograms present the
comparison between the original photo and
compressed photo after sending via MMS.
Figure 1: Histogram of original photo.
Figure 2: Histogram of MMS-photo.
Comparing the original photo with the MMS
photo, the histograms show that there is a minor
difference.
This reveals that colour distribution is nearly the
same. Mean pixel value changed from 185.63 to
183.89. After compression, central pixel value is 183
(before 185).
Image compression effects dimension and file
size. The following table shows the dimension and
file size of the images before and after sending via
MMS.
Table 5: Dimensions and file size.
dimensions file size
original MMS before after
D1 2048x1536 640x480 695 kb 13 kb
D2 2048x1536 640x480 748 kb 13 kb
D3 2592x1944 640x480 1852 kb 32 kb
3.2 Results of the Clinical Trial
Every phone produced about 22 blurred photos. In
total this results in only 66 photos.
15 photos were overexposed and therefore waste.
One of the three cell phones produced only one and
the worst only 8 overexposed photos.
4 DISCUSSION
Test results indicated that a homogeneously bright
illumination allows preventing errors and noise
artefacts. Diffuse illumination is the best scenario
for camera phone photos. Concentrated light creates
the most defects. It produces extremely bright pixels
in a wide area. Illumination had a considerably
unfavourable effect on colour fidelity.
While sending MMS, the original high resolution
photo stored on the mobile phone will not always
remain unaffected. Usually, original images are
altered by lossy compression algorithms.
The results of this pilot study show that the ability to
acquire close-up images and optimum illumination
are very important to obtain photos that are of
sufficient quality for tele-diagnosis.
REFERENCES
Herrmann, FE., Sonnichsen, K., Blum, A., 2005.
Teledermatology versus consultations--a comparative
study of 120 consultations. Hautarzt
Lam, TK., Preketes, A., Gates, R., 2004. Mobile phone
photo messaging assisted communication in the
assessment of handtrauma. ANZ J.Surg
Braun, RP., Vecchietti, JL., Thomas, L., 2005.
Telemedical Wound Care: Using a New Generation of
Mobile Telephones. Arch Dermatol
Ebner, C., Wurm, EM., Binder, B., Kittler, H., Lozzi, GP.,
Massone, C., Gabler, G., Hofmann-Wellenhof, R.,
Soyer, HP., 2008. Mobile teledermatology: a
feasibility study of 58 subjects using mobile phones. J
Telemed Telecare
APPLICABILITY OF MOBILE PHONES FOR TELE-DERMATOLOGY - A Pilot Study
477
