
AN AGENT-BASED SYSTEM FOR HEALTHCARE
PROCESS MANAGEMENT
Bian Wu, Minhong Wang
Division of Information and Technology Studies, The University of Hong Kong, Hong Kong, China
Hongmin Yun
Ophthalmological Department, Shengzhen Hospital, Beijing University, China
Keywords: Healthcare, Process Management, Software Agent.
Abstract: An effective approach for healthcare process management is the key to delivery of high-quality services in
healthcare. An agent-based and process-oriented system is presented in this study to facilitate dynamic and
interactive processes in healthcare environment. The system is developed in three layers: the agent layer for
healthcare process management, the database layer for maintenance of medical records and knowledge, and
the interface layer for human-computer interaction. The treatment of primary open angle glaucoma is used
as an example to demonstrate the effectiveness of approach.
1 INTRODUCTION
In healthcare organizations, there are a variety of
processes, such as hospital administration by
managers, registration for treatment by patients, test
report generation by technicians, and diagnosis
decision making by doctors. There is a trend to view
healthcare in a multidisciplinary perspective, as
numerous interactions and cooperation take place
across different functional units in terms of
information sharing, consultation, and combined
treatments. These interactive and collaborative
activities should be well organized and managed,
without which the efficiency of healthcare service
cannot be easily guaranteed. To meet these
requirements, a process-oriented and cooperation-
supported healthcare system is needed, especially
with computer and information technology support.
To facilitate healthcare process management,
workflow technology (van der Aalst and van Hee,
2002) has been applied in a number of studies (Lenz
and Reichert, 2007). In the recent years,
organizational environments have been changing
from stable-and-closed to dynamic-and-open.
Business processes are becoming increasingly
complex and dynamic as they seek to cope with a
wide range of internal and external interactions and
changes. Traditional workflow technologies for
process management are often inadequate for
complex and dynamic situations due to the lack of
flexibility and adaptability (Wang and Wang, 2006).
This change has also happened in the healthcare
sector. Frequent changes of clinical pathways and
increased interactions between different units have
become a big challenge in healthcare process
management. This change has also happened in the
healthcare sector. Due to newly discovered
symptoms of a specific disease or need of further
diagnosis, pre-planned clinical schedules always
request adjustment; ad hoc changes of medical
process are needed during execution. Besides, to
fulfill a simple task such as gonioscopy for
glaucoma diagnosis, cooperation among different
functional units is required. In sum, frequent
changes of clinical pathways and increased
interactions between different units have become a
big challenge in healthcare process management.
To develop a computer-based system that enables
effective process management in healthcare, an
agent-based cognitive approach is presented in this
study. The term “agent” refers to a piece of software
that can perceive its environment through its sensors
and can act upon that environment through the
effectors (Wooldridge and Jennings, 1997).
A
healthcare management unit has similar
characteristics with software agent, which has a set
45
Wu B., Wang M. and Yun H. (2009).
AN AGENT-BASED SYSTEM FOR HEALTHCARE PROCESS MANAGEMENT.
In Proceedings of the 11th International Conference on Enterprise Information Systems - Artificial Intelligence and Decision Support Systems, pages
45-50
DOI: 10.5220/0001859000450050
Copyright
c
SciTePress

of goals (e.g., treatment effects and costs),
perceptions of the environment (e.g., symptoms and
records), and actions to take (e.g., recommendations
for test or treatment, and inquiry).The highly
dynamic and unpredictable nature of organizational
processes makes agent-based approaches appealing.
Using agent-based technology, we may decompose a
complex process into a number of loosely coupled
tasks and delegate the tasks to a number of software
agents, each of which works autonomously and
collaboratively in performing tasks and managing
the whole process (Wang and Wang, 2006).
In this study, an agent-based and process-oriented
healthcare system is developed. The system consists
of three layers, the agent layer for healthcare process
management, the database layer for maintenance of
medical records and knowledge, and the interface
layer for human-computer interaction. The emphasis
is placed on dynamic clinical and administrative
process management, and knowledge building as the
foundation for process management. This agent-
based and process-oriented healthcare system
distinguishes from other healthcare systems in terms
of continuous awareness of the healthcare
environment, real-time dynamic decision making of
healthcare processes, and rule-based knowledge
engineering. The treatment of primary open angle
glaucoma (POAG) is used as an example to
demonstrate the effectiveness of this approach.
2 SYSTEM ARCHITECTURE
To meet the requirements arising from dynamic
processes and cooperative functions in healthcare, an
agent-based healthcare process management system
is presented with a three-layer architecture.
2.1 Interface Layer
This layer supports various interactions between
human users (administrators, doctors, nurses, and
medical technicians) and the computer system.
Different type of user may access and interact with
the system through specific interfaces.
2.2 Agent Layer
In the system, a group of software agents are
proposed to perform healthcare tasks. Various
interactions take place between the autonomous
agents or between the agents and human users
including doctors, nurses, technicians, and
administrators. The design of software agents is
process-oriented, i.e., agents are able to execute
tasks according to process rules. What’s more,
process rules can be edited in a graphical form,
which makes it easy to specify and update the rules.
The details of each agent are elaborated as follows.
Clinical Decision Agent works with doctors. It
consists of three components: a knowledge base that
captures glaucoma knowledge into a set of rules for
clinical diagnosis decision making; a reasoning
engine that generates diagnosis decision or treatment
recommendations based on patient records and test
results; and an interpreter that interprets the
decisions or recommendations generated by the
computer.
Patient Management Agent works with clinical
administrators and nurses, managing patient records
and coordinating treatment processes. It also
interacts with other agents for communication of
patient records, test reports, and treatment records
throughout the healthcare process.
Medical Examination Agent works with doctors,
medical technicians, or nurses, as well as
communicates with Patient Management Agent and
Clinical Decision Agent throughout the medical
examination process. The medical examination
process may go through several steps including
patient records access, test scheduling, notification
and reminder, and finally test report generation and
delivery.
Ward Treatment Agent works with doctors and
nurses, as well as communicates with Patient
Management Agent or Clinical Decision Agent
during the inpatient treatment process. The activities
include treatment scheduling, notification and
reminder, information inquiry, and treatment report
generation and delivery. The agent also maintains
the information of treatment activities, progress, and
patient states during the treatment process.
Operation Agent works with doctors and nurses,
as well as communicates with Patient Management
Agent or Clinical Decision Agent to manage the
operation process. The process may go through
several steps including patient records retrieval,
operation scheduling, notification and reminder, and
operation report generation and delivery.
2.3 Database Layer
Medical information is stored in a database to
support the healthcare functions. The information
includes patient records, treatment records,
examination records, diagnostic knowledge, and
treatment knowledge. Considering information
security and maintenance issue, different agents are
ICEIS 2009 - International Conference on Enterprise Information Systems
46
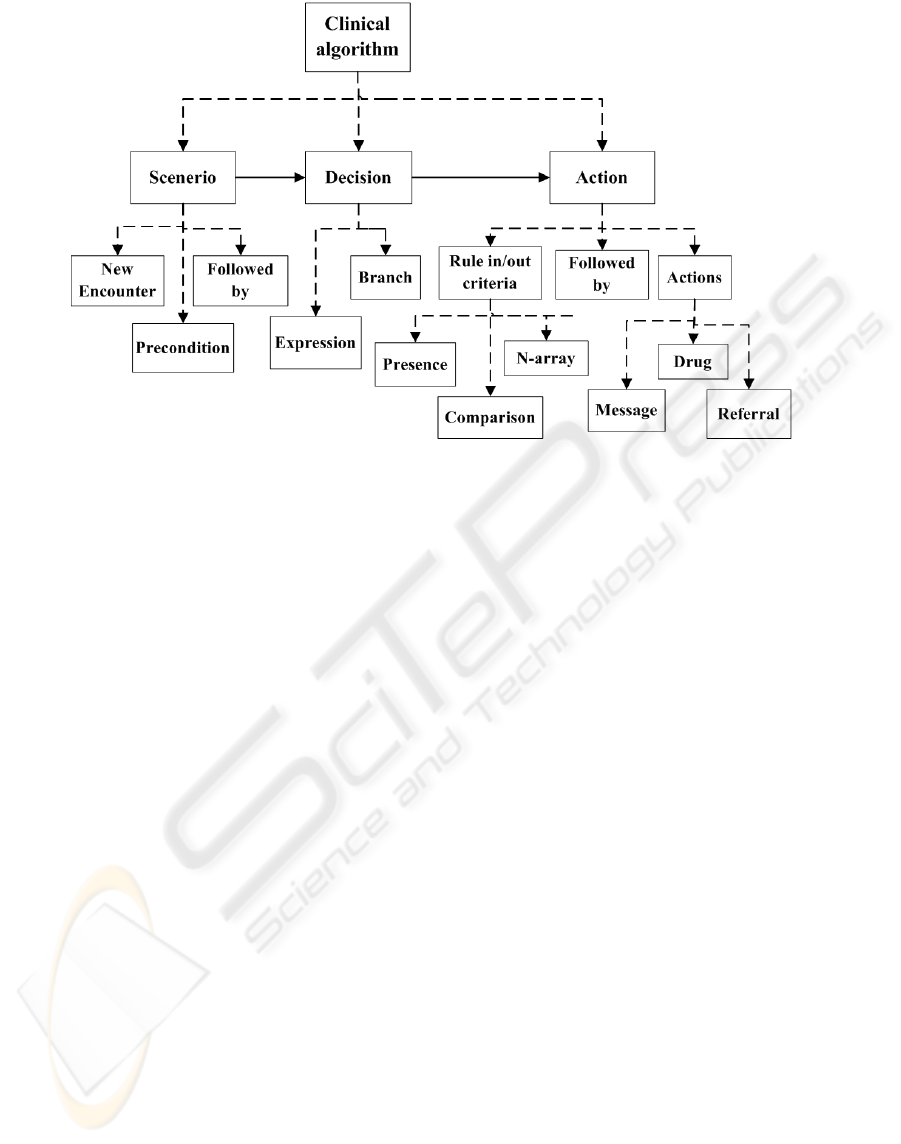
Figure 1: Hierarchy of clinical algorithm ontology.
associated with different data, with different rights
to access or update the data. For example, Patient
Management Agent has the right to access patient
records; while other agents can acquire patient
records via communication with Patient
Management Agent. Differing from data records,
knowledge for clinical and administrative process
management is more complicated. Relevant
techniques and tools are used to capture and model
the knowledge into a set of rules or guidelines.
3 KNOWLEDGE-BASED
PROCESS MANAGEMENT
To facilitate dynamic and interactive clinical
processes, we need to capture a large amount of
information and knowledge as the foundation for
process management. In addition to clinical
information such as patient records and treatment
data, it is crucial to identify or set up the rules or
guidelines as the knowledge for diagnosis and
treatment decision making and clinical
administration. To capture and represent the
knowledge in the system, ontology-based
technology is adopted in this study. Using ontology,
the narrative paper based guidelines or rules are
encoded into computerized specifications. To build
the ontology, we use Protégé (O’Connor et al., 2007)
as the ontology representation tool. Protégé is a free
and open-source platform that provides a suite of
tools to construct domain models and knowledge-
based applications with ontology. In developing the
proposed system, we use Protégé for knowledge
building by way of class modelling, goal and criteria
building, clinical algorithm construction.
In this study, we choose glaucoma treatment as
an example to demonstrate the proposed approach.
Glaucoma is a leading cause of blindness in most
countries; the irreparable loss of vision by glaucoma
requires lifelong healthcare. Meanwhile, the disease
of glaucoma is well investigated; the process of the
treatment is documented as various kinds of
guidelines that can be used as reference for
knowledge building in this case. There are many
types of glaucoma, from which we choose the
primary open angle glaucoma (POAG) for
illustration.
3.1 Knowledge Modelling
We model the rules or guidelines for clinical
decision-making into clinical algorithms (see Figure
1). Based on the clinical algorithms,
recommendations such as messages, drugs, and
referrals can be generated for diagnosis, treatment,
and other clinical process.
Each algorithm includes three nodes: scenario,
decision, and action. Scenarios are mutually
exclusive entry points for clinical algorithms, which
exhibit unambiguous definition of patient states. A
scenario contains several major properties called
slots: a) the new encounter slot is used to
enable/disable this scenario as a starting point; b) the
precondition slot is to qualify the scenario as a
AN AGENT-BASED SYSTEM FOR HEALTHCARE PROCESS MANAGEMENT
47
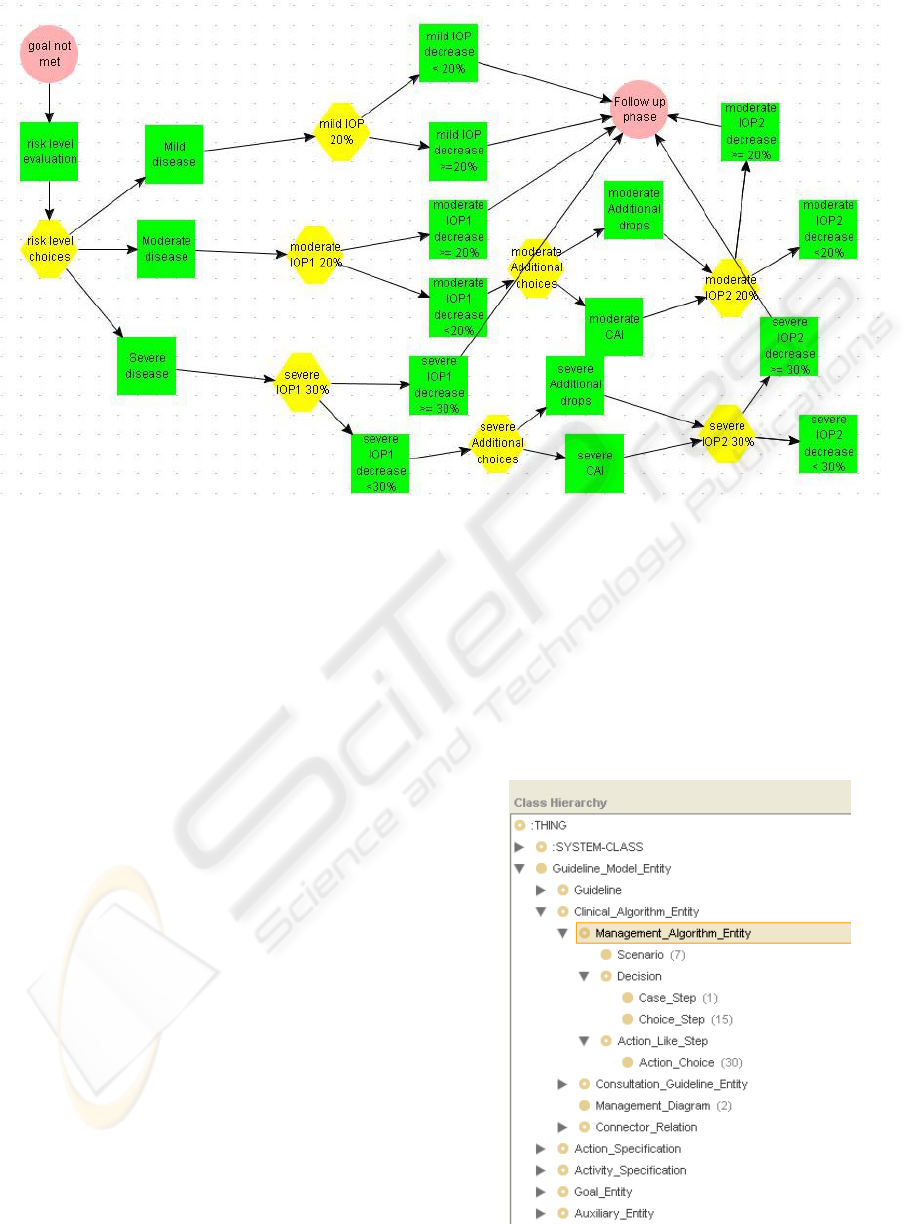
Figure 2: POAG treatment algorithm after topical therapy.
starting point; and c) the followed by slot is a next
step in the algorithm. A decision node contains: a) a
choice step (e.g., severe IOP1 decrease <30%)
which may lead to more than one choice; or b) a
case step which has an evaluated expression to
enable the execution of the next step node. An
action is a node with a rule in/out criteria slot (e.g.,
if risk level = severe and IOP decrease >= 30%) and
a defined action slot (e.g., Filtration surgery) in
forms of message, drug recommendations, or
referrals.
3.2 Knowledge-based Clinical Process
The diagnosis and treatment process of glaucoma
can be divided into several steps:
1) Comprehensive eye examination should be
carried out to differentiate POAG or suspect.
2) Further examinations are taken for establishing a
baseline of intraocular pressure (IOP) and designing
the initial treatment.
3) After establishing a good baseline, it is obliged to
set up a reasonable goal of intraocular pressure
(IOP).
4) Based on the goal established in step 3, an initial
topical therapy is carried out to lower the pressure.
5) If necessary, follow-up treatment is required after
the initial topical therapy. Due to the space
limitation, we only provide details of step 5 as
follows.
In the initial treatment of POAG (step 4), the first
step topical therapy may not reach the initial
intraocular pressure goal. Therefore, treatment
algorithm after topical therapy (Hodapp et al., 1993)
should be followed. Figure 2 shows the modeling of
this specific algorithm in Protégé. Pink circle
indicates a scenario; yellow polygon indicates a
decision; and green square indicates an action
choice.
Figure 3: Class hierarchy in Protégé.
ICEIS 2009 - International Conference on Enterprise Information Systems
48

They are linked by one direction arrow to show a
follow-up relation with each other and form an
algorithm chart. After implementation, the POAG
treatment algorithm after topical therapy is
represented as an instance of Management
Algorithm Entity shown in Figure 3. The pink
circles, yellow polygons, and green squares in
Figure 2 are mapped to three subclasses (Scenario,
Choice step, and Action Choice) of Management
Algorithm Entity, respectively in Figure 3.
4 SYSTEM IMPLEMENTATION
In our system, five agents are developed, Patient
Management Agent, Medical Examination Agent,
Ward Treatment Agent, Operation Agent, and
Clinical Decision Agent. For implementation of a
multi-agent system, we adopted JADE (Bellifemine
et al., 2007), a widely used open source middleware
developed by TILAB for the development of
distributed multi-agent applications based on the
peer-to-peer communication architecture.
In addition to multi-agent architecture, the
implementation concerns the individual agent. After
specifying clinical guidelines and process rules
using Protégé, we use a plug-in called
beangenerator, implemented by C.J. van Aart, to
create the ontology definition class and the
predicates, agent actions, and concepts classes
(Caire and Cabanillas, 2006) for implementation of
individual agent. Agents can retrieve information
and knowledge to perform tasks under control of
rules or guidelines. Two types of rules are specified,
one for clinical decision and another for
administrative process control.
5 CONCLUSIONS
This paper has presented a three-layer architecture of
an agent-based healthcare process management
system. The agent-based cognitive approach is
applied to facilitate dynamic and interactive
processes in healthcare management. The treatment
of primary open angle glaucoma is used as an
example for demonstration. After the
implementation of the prototype, we will evaluate
the effectiveness of the approach in terms of support
for clinical and administrative process management
in healthcare environment. Relevant clinical and
administrative staff will be invited to use this system
and give feedback and evaluation on the system.
ACKNOWLEDGEMENTS
This research is supported by UGC GRF Grant
(716907) from the Hong Kong SAR Government
and Seeding Funding for Basic Research
(200711159052) from The University of Hong
Kong.
REFERENCES
Bellifemine, F., Caire, G., and Greenwood, D., 2007.
Developing Multi-Agent Systems with JADE,
Chichester, England; Hoboken, NJ: John Wiley.
Caire, G. and Cabanillas, D., 2004. Jade Tutorial
Application-defined content languages and ontologies,
Manual, TILAB.
Hodapp, E.M.D., Parrish, R.G.M.D., and Anderson, D.G.,
1993. Clinical decision in glaucoma, Mosby-Year
Book, Inc.
Lenz, R. and Reichert, M., IT support for healthcare
processes– premises, challenges, perspectives. Data &
Knowledge Engineering, 61 (1), 39-58, 2007.
O’Connor, M., Shankar, R., Tu, S., Nyulas, C., Das, A.,
and Musen, M., 2007. Efficiently Querying Relational
Databases Using OWL and SWRL The First
International Conference on Web Reasoning and Rule
Systems. Innsbruck, Austria, Springer.
van der Aalst, W.M.P. and van Hee K.M., 2002. Workflow
Management: Models, Methods, and Systems, MIT
press, Cambridge, MA.
Wang, M. and Wang, H., 2006. From Process Logic to
Business Logic - A Cognitive Approach to Business
Process Management. Information & Management, 43
(2), 179-193.
Wooldridge, M. and Jennings, N.R., 1999. Software
Engineering with Agents: Pitfalls and Pratfalls, IEEE
Internet Computing, 3(3), 20-27.
AN AGENT-BASED SYSTEM FOR HEALTHCARE PROCESS MANAGEMENT
49
