
A DESIGN OF DIAGNOSIS SYSTEM FOR MENTAL DISORDER
Mariko Sasakura, Kenichi Iwata and Susumu Yamasaki
Department of Computer Science, Okayama University, 311, Tsushima-Naka, Kita-ku, Okayam, Japan
Keywords:
Knowledge engineering, Diagnosis.
Abstract:
We propose a web application system which helps experts to make a diagnosis of mental disorders. We
construct a knowledge base from DSM and SCID which are diagnosis manuals made by psychiatrists. We
have two stages in our diagnosis system. In the first stage, our application picks up suspicious disorders. In
the second stage, the application checks the suspicious disorders according to a flow chart generated by the
knowledge base. We discuss problems gained by our experiment of constructing the knowldge base.
1 INTRODUCTION
Diagnosis can be included an area of knowledge en-
gineering. This view is supported by the existance of
many medical expert systems (Phuong et al., 2000;
Starita et al., 1995).
In this paper, we present an experiment system to
construct a prototype system for assisting to make a
diagnosis of a mental disorders. Diagnosis of men-
tal disorders is difficult because of a lack of objective
biological markers. Therefore, to make a diagnosis,
psychiatrists are required a great deal of knowledge
of disorders and symptoms.
To assist to make an accurate diagnosis, we con-
struct a system by rearranging knowledge from DSM
(Diagnostic and Statical Manual of Mental Disor-
der) and SCID (The Structured Clinical Interview for
DSM), which are manuals to make a diagnosis of
mental disorder. DSM and SCID are a kind of knowl-
edge base constructed by experts: psychiatrists. The
original DSM or SCID are designed for checking all
disorders’ criteria. The process is time-consuming. In
order to decrease the time, our system is designed to
make a diagnosis by two stages. In the first stage, the
system lists up suspicious disorders from symptoms.
In the second stage, the system assists an expert in
making a diagnosis of the selected disorders from the
result of the first stage. In this stage, the expert checks
the criteria of suspicious disorders according to the
description of SCID, which are displayed on the com-
puter screen. To implement the system, we have to
reconstruct the knowledge of DSM for the first stage.
In Section 2, we introduce the details of DSM and
SCID. In Section 3, we describe the knowledge base
we constructed. In Section 4, we show the prototype
system we developed. In Section 5, we discuss prob-
lems we find out during our experience, and in Sec-
tion 6, we give a conclusion.
2 DIAGNOSIS MANUAL OF
MENTAL DISORDER
In this section, we mention the details of DSM (Amer-
ican Psychiatric Association, 2000) and SCID (First
et al., 2002) which are basis of our knowledge base.
2.1 DSM
Diagnosis of mental disorders has difficulties because
most of symptoms are subject of patients and not ob-
jective. Psychiatrists must give a diagnosis which dis-
order a patient has by major complaints and an obser-
vation of the patient. Therefore, the different patients
used to be given different diagnosis to the same symp-
toms.
American Psychiatric Association organizes the
relation of symptoms and the names of disorder as
a manual called “Diagnostic and Statical Manual of
Mental Disorder” (DSM). In this manual, psychia-
trists give the same disorder to the same symptoms.
The latest version of DSM is DSM-IV-TR published
in 2000.
368
Sasakura M., Iwata K. and Yamasaki S. (2009).
A DESIGN OF DIAGNOSIS SYSTEM FOR MENTAL DISORDER.
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development, pages 368-371
DOI: 10.5220/0002271203680371
Copyright
c
SciTePress
Table 1: DSM example : a part of criteria of panic disorder
without Agoraphobia.
A. Both (1) and (2):
(1) recurrent unexpected Panic Attacks
(2) at least one of the attacks has been followed
by 1 month (or more) of one (or more) of the fol-
lowing:
(a) persistent concern about having additional
attacks
(b) worry about the implications of the attack
or its consequences (e.g., losing control, having a
heart attack, “going crazy”)
(c) a significant change in behavior related to
the attacks
B. Absence of Agoraphobia.
(The rest is omitted.)
In DSM, a diagnostic criteria is given to each dis-
order in a natural language.
Table 1 shows a part of criteria of panic disor-
der. The criteria are declarative description. To judge
whether symptoms of a patient satisfy the criteria, the
knowledge of experts is needed. Therefore, only ex-
pert psychiatrists should be permitted to make a diag-
nosis using DSM.
2.2 SCID
”The Structured Clinical Interview for DSM-IV”
(SCID) is a semi-structured interview for the forth
version of DSM.
SCID is a list of questions which are constructed
like a flowchart. An expert can make a diagnosis fol-
lowing SCID. SCID has same contents of DSM but
the contents are described in a procedural way. It
shows a procedure of a diagnosis.
Table 2 shows a part of list of panic disorder cri-
teria. Some questions in the list need specialized
knowledge to answer. SCID also needs expert psy-
chiatrists to perform.
The two problems for SCID have been pointed
out. DSM also has the problems because SCID and
DSM are same essentially. The first problem is that
it is time-consuming to deliver, because it is designed
to check all disorders’ criteria in order. The second
problem is that the quality of the diagnosis depends
on the expert who uses it, because some questions in
SCID needs expert knowledge to answer.
Table 2: SCID example: a part of list of panic disorder with-
out Agoraphobia.
No. Questions Next question
F1 recurrent unexpected
panic attacks
if negative goto F25,
else goto F2
F2 at least one of the
follwoing: (b) worry
about the implications
of the attack; (a) con-
cern about having ad-
ditional attack; (c) a
significant change in
behavior
if negative goto F25,
else goto F3
F3 Four (or more) of the
following panic attack
symptoms developed
abruptly and reached
a peak within 10
minutes
if negative goto F25
F4 (1) palpitations
F5 (2) swaeting
(The rest is omitted.)
3 A DESIGN OF KNOWLEDGE
STRUCTURE
Both DSM and SCID aim to diagnose a specified dis-
order. Usually, a psychiatrist may see a patient, and
check a criteria of the disorder of DSM or SCID. The
problem of DSM or SCID is time-consuming to de-
liver, because they are constructed for cheking all dis-
orders’ criteria.
Therefore, we divide a process of diagnosis into
two stages. The first stage based on declarative
knowledge, DSM, is used to find suspicious disor-
ders. The second stage based on procedural knowl-
edge, SCID, is used to diagnose the disorders.
3.1 The First Stage
In the prototype system we developed, the first stage
is implemented simply.
1. The system lists up all symptoms related disor-
ders.
2. An expert decides a threshold rate.
3. An expert checks all symptoms that a patient has.
4. If the number of checked symptoms related to a
disorder goes over the threshold rate, the system
picks up the disorder.
5. All disorders the system picked up are displayed
on the screen for the second stage.
A DESIGN OF DIAGNOSIS SYSTEM FOR MENTAL DISORDER
369

3.2 The Second Stage
The second stage will start at a disorder that is listed
up by the first stage of the system. The expert looks
the list of the suspicious disorders at first, then picks
up a disorder that seems to be the possibly true dis-
order of the patient. Then the verification stage (the
second stage) starts on here.
The system asks a question that follows SCID,
and then the expert answers. This answer includes
a thought of the expert. The expert interacts with
the patient, and judges how to answer to the ques-
tion from the system. This means the expert interacts
with the system also, not only with the patient. The
system stored the answer to the database, then shows
a new question to the expert. The system shows also
the process of the flow. This helps the expert to judge
the disorder of the patient. The expert is possible to
think about the answer of the question from the sys-
tem too.
The cycle is continued until the flow reaches to the
end. At the end of the flow, the system shows if the
suspicious disorder of the patient would truly match
to the symptoms, or not.
The questions in the second stage of SCID have
3-valued logic. The answer for the question is one of
?, -, or +. The answer is interpreted in : ? means inad-
equate information, - means absent or sub-threshold
(negative), and + means present (positive). If the an-
swer is +, the patient has the symptom asked by the
question.
The questions of SCID can be categorized into
two types following:
Type 1. The next question is decided by the answer
of the this question.
Type 2. The next question is decided by the answers
of the previous questions including this question.
In this type of question, sometimes more than 10
previous questions are related to decide the next
question.
The system supports these two types of nodes and
controls flows of questions in the second stage.
4 SYSTEM DESIGN
The proposed system aims to assist psychiatrists in
making a diagnosis. It is designed as a Web-based
system. The architecture of the system is shown in
Figure 1.
The system consists of four parts: Back End DB,
Suspicious Disorders List Up Engine, SCID engine
Back End
DB
Expert
Patient
Suspicious
Disorders
List Up
Engine
SCID Engine
The System
The First Stage
The Second Stage
Browser
Figure 1: The system architecture.
Figure 2: The first step.
and Browser. Back End DB keeps knowledge for di-
agnoses and records of diagnoses. Suspicious Disor-
ders List Up Engine is an implementation of the first
stage mentioned in subsection 3.1. SCID engine is
an implementation of the second stage described in
subsection 3.2. Browser is an interface between the
system and psychiatrists. Any popular web browser
can be used as the Browser.
Figures 2, 3 and 4 show snapshots of the system.
Figure 2 is a snapshot of the first stage. A psychi-
atrist asks and observes symptoms of a patient and
checks in boxes of present symptoms. Figure 3 show
the result of Figure 2: a list of suspicious disorders.
When the psychiatrist click the “go” button in Figure
3, the second stage starts. Figure 4 is a snapshot of
the second stage. In the second stage, questions are
displayed on the screen in sequence. The psychiatrist
inputs answers for the questions by checking an ap-
propriate item, then the result flows: the patient has
the suspicious disorder or not.
5 DISCUSSION
By constructing the system, we find the following
problems in DSM and SCID.
1. Knowledge for diagnosis described in DSM or
SCID has ambiguity. In DSM or SCID, the am-
KEOD 2009 - International Conference on Knowledge Engineering and Ontology Development
370
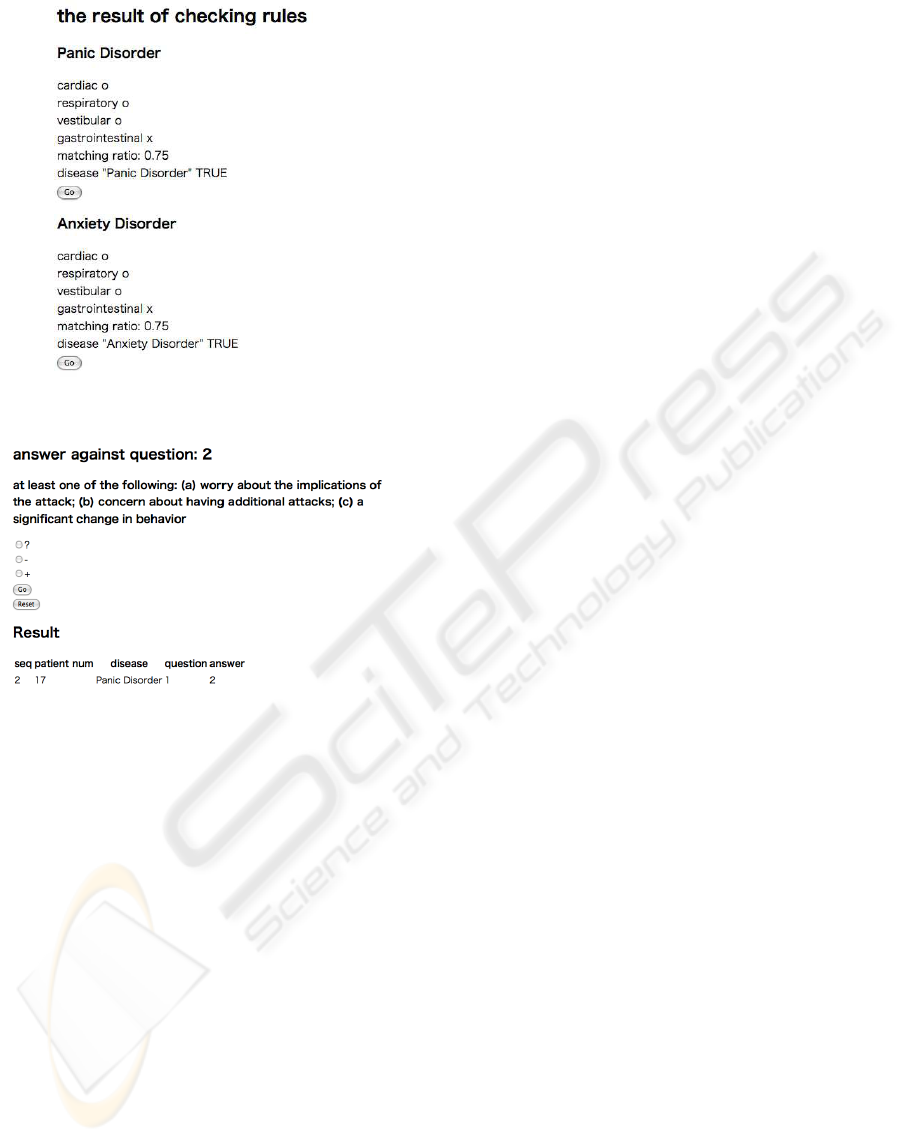
Figure 3: The suspicious disorders.
Figure 4: The second step.
biguity should be resolved by psychiatrists when
they make a diagnosis for a patient. That is a rea-
son why only psychiatrists should be permitted to
make a diagnosis using DSM or SCID.
2. Knowledge for diagnosis is still growing and
changing. DSM has been upgraded in three
times from the first published year, 1952, the sec-
ond:1968, the third:1980 and the forth:1994. And
next upgrade is under contemplation.
3. Knowledge described in DSM and SCID is strict
and exhaustive. Therefore the most serious prob-
lem of DSM or SCID for making a diagnosis is
time-consuming to deliver.
For the problems, our system can provide a partial
answer.
• For 1, the system does not resolve the ambiguity,
because the ambiguity is involved the knowledge
we use.
• For 2, the system should be designed flexibly for
the change of knowledge. We will try to solve this
problem.
• For 3, we design two stages diagnosis so that the
system is expected to be shorten time for diagno-
sis. Our next work will verify this point.
For the first stage of the system, we extract symp-
toms from the description of DSM by hand. In future,
we would like to extract them by computer. There are
problems in DSM to extract symptoms by computer.
They are natural language processing problems.
• Too many symptoms are mentioned so that it is
hard to distinguish which symptoms are “main”
or “critical”.
• Sometimes the same or similar symptoms are de-
scribed different representations. Therefore, for
the first stage, we have to reduce them to repre-
sentative symptoms.
At first, we will check whether our manual procedures
work well in practical cases, then, consider how the
work is done automatically.
6 CONCLUSIONS
We propose a web-based system which assists psychi-
atrists in making a diagnosis. We design a knowledge
base by reconstructing knowledge organized in man-
ual, DSM and SCID. We divide a process of making
a diagnosis in two stages. In the first stage, a psychia-
trist selects suspicious disorders from the list provided
by the system. In the second stage the psychiatrist
makes a diagnosis of the selected disorders. We also
discuss problems we find out during our experience.
REFERENCES
American Psychiatric Association (2000). Diagnostic and
statistical manual of mental disorders fourth edition
text revision DSM-IV-TR. American Psychiatric Pub-
lishing, Inc.
First, M. B., Spitzer, R. L., Gibbon, M., and Williams, J.
B. W. (2002). User’s Guide for the structured clini-
cal interview for DSM-IV axis I disorder. American
Psychiatric Press Inc.
Phuong, N. H., Dang, J. H., and Prasad, N. R. (2000). De-
veloping a supporting expert system for lung-disease
diagnosis using fuzzy logic. Biomedical Soft Comput-
ing and Human Science, 5(2):37–44.
Starita, A., Majidi, D., Giordano, A., Battaglia, M., and
Cioni, R. (1995). A tutorial expert system for the di-
agnosis of neurogenic diseases of the lower limb. Ar-
tifcial Intelligence in Medicine, 7(1):25–36.
A DESIGN OF DIAGNOSIS SYSTEM FOR MENTAL DISORDER
371
