
TOWARDS FULLY AUTOMATED PSYCHOTHERAPY
FOR ADULTS
BAS - Behavioral Activation Scheduling Via Web and Mobile Phone
Fiemke Both
1
, Pim Cuijpers
2
, Mark Hoogendoorn
1
and Michel Klein
1
1
Dept. of Artificial Intelligence, VU University Amsterdam, De Boelelaan 1081a, 1081HV Amsterdam, The Netherlands
2
Dept. of Clinical Psychology, VU University Amsterdam, van Boechorststraat 1, 1081 BT Amsterdam, The Netherlands
Keywords: Automated psychotherapy, Agent model.
Abstract: Behavioural activation treatment has been found to be an effective psychological treatment for depression,
also if delivered as self-administered psychotherapy via the internet. However, the role of supporting
professionals remains important for successful application of the therapy. In this paper a system is presented
that delivers automated behavioural activation therapy via both a mobile phone and a personal website. The
system motivates the client to continue with the treatment and helps him/her through the different
procedures of the treatment. The architecture of the system follows a generic ambient agent architecture. A
first pilot study of the system indicates that it is technically feasible and perceived as useful.
1 INTRODUCTION
Dozens of well-designed studies and meta-analyses
have shown that psychological interventions are
effective in the treatment of depressive disorders in
adults (Cuijpers et al., 2007; Churchill et al., 2001;
Leichsenring, 2001; Gloaguen et al., 1998). There is
also a growing number of studies showing that self-
administered psychotherapies are effective in the
treatment of depression. In such a therapy, a patient
can read in a book or on a website step-by-step what
he can do to apply a generally accepted
psychological treatment to himself.
Although self-administered treatments are
mainly conducted by clients themselves, the role of
supporting professionals remains important for
successful application of the therapy (Spek et al.,
2007a). In general it is assumed, that professional
support is needed to motivate the client to continue
with the treatment and to help him/her through the
different procedures of the treatment.
It would be attractive to develop a psychological
treatment that does not need a professional therapist,
but still has some automated actor involved to
interact frequently with the client. The current
project addresses the development of an automated
interactive psychotherapy for depression: BAS
(behavioural activation scheduling). The core is a
systematic internet intervention in which the patient
plans her daily activity (based on the principles of
behavioural activation therapy, see below). The
patients use a mobile phone which will help them
during the day to work through the behavioural
activation treatment. This daily support (through the
mobile phone) is fully automated.
In this paper, the design of the BAS automated
psychotherapeutic system as instantiation of
intelligent ambient agent system is presented
(Section 3) and first experiences within a pilot study
are reported (Section 4). First the psychological
intervention activity scheduling that is the basis of
the current project is described in Section 2. Finally,
the paper is concluded with a discussion.
2 ACTIVITY SCHEDULING
Activity scheduling (AS, also called behavioural
activation) is an intervention for clinical depression
based on a theory by Lewinsohn, Youngren &
Grosscop (1979) who say that a low rate of
behaviour (often caused by inadequate social skills)
is the essence of a depression and the cause of all
other symptoms. Part of his theory is the hypothesis
that there is a causal relationship between lack of
positive reinforcement from the environment and the
depression. A depression can be treated by
increasing the positive reinforcement through
375
Both F., Cuijpers P., Hoogendoorn M. and Klein M. (2010).
TOWARDS FULLY AUTOMATED PSYCHOTHERAPY FOR ADULTS - BAS - Behavioral Activation Scheduling Via Web and Mobile Phone.
In Proceedings of the Third International Conference on Health Informatics, pages 375-380
DOI: 10.5220/0002688503750380
Copyright
c
SciTePress
increasing the quantity and quality of (social)
activities. Many studies have shown that this type of
intervention works just as well as or even better than
other popular treatments (Dimidjian et al, 2006;
Jacobson et al, 1996). Recently, it is shown that
interventions of this type offered via the internet are
very effective (Christensen et al, 2004; Andersson et
al, 2005, Spek et al, 2007b).
There are two stages in AS treatment: the first
stage is observing that pleasant activities and a good
mood come together by writing down all pleasant
activities and mood level. The second stage is
changing the activity schedule so that the patient
participates in more pleasant activities with the goal
of increasing the mood level. The mood increases on
a short term, and by learning that pleasant activities
influence mood level positively, patients are more
capable of dealing with future situations.
For the BAS intervention, this intervention as
been implemented in a five-step plan: 1) rating the
mood via a mobile phone or via a website; 2)
registering their current pleasant activities and rate
them; 3) actively planning more pleasant activities
and setting a goal for the desired mood level at the
end of the intervention; 4) encouraging to keep
doing more pleasant by giving automated weekly
feedback; 5) continue scheduling pleasant activities.
In addition, a plan for the future can be made to help
prevent relapse and reoccurrence of depression.
3 AGENT MODEL
Automated psychotherapy via website and mobile
phone can be seen as an instance of Ambient
Intelligence applications, where software has
knowledge about human behaviours and states, and
(re)acts on these accordingly (
Aarts et. al., 2003). For
this class of applications an agent-based generic
model has been developed (Bosse et. al., 2009). This
model can be instantiated by case-specific
knowledge to obtain a specific model in the form of
executable specifications that can be used for
simulation and analysis. In this section, the
automated psychotherapeutic intervention will be
described using this generic framework.
3.1 Generic Framework for Human
Ambience applications
For the global structure of the generic model for
human ambient applications, first a distinction is
made between those components that are the subject
of the system (e.g., a patient to be taken care of), and
those that are ambient, supporting components.
Moreover, from an agent-based perspective, a
distinction is made between active, agent
components (human or artificial), and passive, world
components (e.g., part of the physical world or a
database).
Second, interactions between model elements are
defined. An interaction between two agents may be
communication or bodily interaction, for example,
fighting. An interaction between an agent and a
world component can be either observation or action
performance. An action is generated by an agent,
and transfers to a world component to have its effect
there. An observation results in transfer of
knowledge from the world component to the agent.
Combinations of interactions are possible, such as
performing an action and observing the effect of the
action afterwards.
Finally, ambient agents are assumed to maintain
knowledge about certain aspects of human
functioning in the form of internally represented
dynamic models, and information about the current
state and history of the world and other agents.
Based on this knowledge they are able to have a
more in-depth understanding of the human
processes, and can behave accordingly.
3.2 Agent System Overview
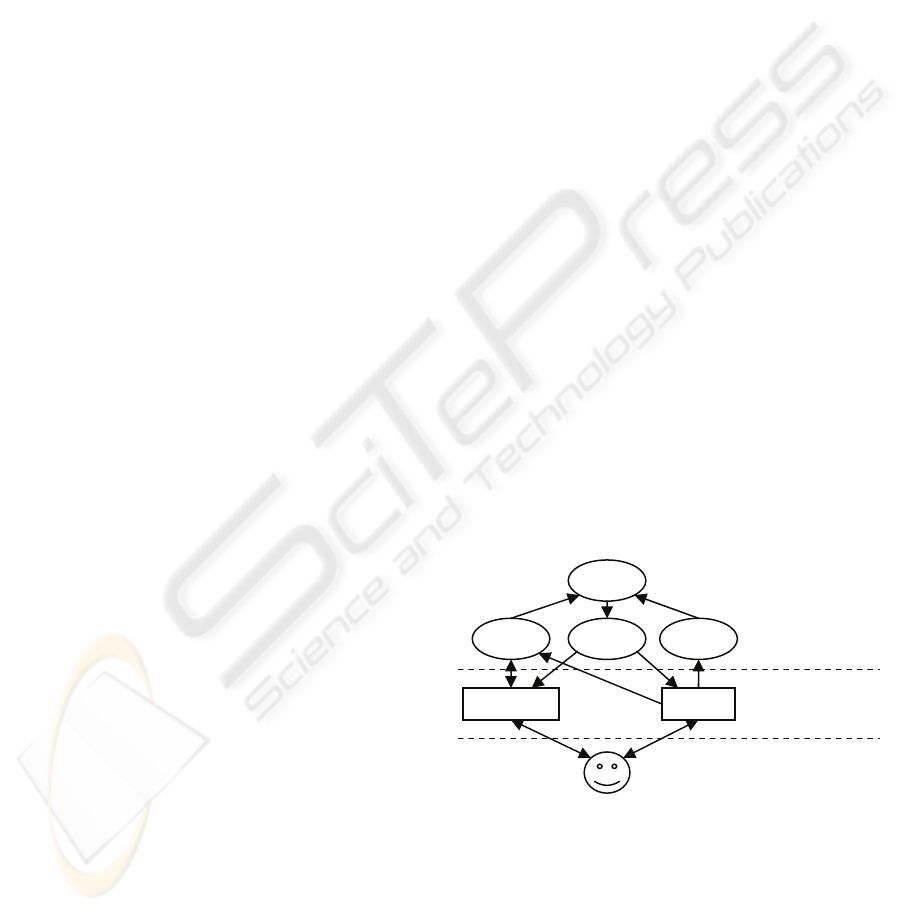
Figure 1 gives an overview of the different
components in the ambient agent model. In the
remainder of this section, the components and their
specific interactions are described. In Section 3.3,
the internal knowledge of the specific agents is
given.
Figure 1: Components in the ambient agent model.
The subject components are the following:
Subject agents: participant suffering from a
depression.
Subject world components: mobile phone of the
participant, computer of the participant with a
dedicated website.
The subject interactions:
AMA
mobile phone website
PA FBA
PAA
subject agent (patient)
subject
world components
ambient agents
HEALTHINF 2010 - International Conference on Health Informatics
376

Observations and actions by subject agents:
Participant inputs information requested for therapy
into either the mobile phone or the website via a
computer. This includes:
Mobile phone actions by participant:
• Mood rating (number between 1 and 10)
• Activity rating (number between 1 and 10)
• Request advice
Mobile phone observations by participant:
• Activity schedule
• Tips
Web site actions:
• Planning activities
• Planning rewards
• Adding possible activities to a list
• Setting goals for the week
Web site observations
• Information about therapy, explanation
• Outcome of all actions performed (see above)
The ambient components are the following:
Ambient agents: activity monitoring agent (AMA),
patient assessment agent (PAA), feedback agent
(FBA), activity planning agent (APA)
The following ambient interactions are
distinguished:
Communication between ambient agents: the
AMA sends the information about the monitoring
and rating of activities to the PAA, APA sends
schedule and information to the PAA, PAA sends
feedback to the FBA.
And finally, the following interactions between
subjects and the ambient components:
Reminders
• Planned activities (AMA – mobile phone)
• Rating of mood (AMA – mobile phone)
• Rating of performed activities (AMA – mobile phone)
Reporting about ratings and activities
• Rating of mood (website / mobile phone – AMA)
• Rating of performed activities (website / mobile phone
– AMA)
• Planned activities (website – APA)
Feedback
• Motivational remarks (FBA – website / mobile
phone)
• Weekly feedback (FBA – website / mobile phone)
o Plots of mood versus number of activities
and rating of activities
o Remarks about mood during week
o Remarks about activities during week
o Remarks about combination of mood and
activities
o Feedback on targets set for week
3.3 Individual Agents
AMA: Activity Monitoring Agent
This agent is responsible for monitoring which
activities have been performed by the patient and
what the mood of the patient was at different
moments (specifically after doing activities).
Maintenance of Agent Information. Maintain the
ratings of the mood and the list of performed
activities. Maintain preferences concerning how
frequent reminders should be sent and the reminders
that have already been sent.
Agent Specific Task. Based upon the information
present: derive reminders. There are two types of
reminders, namely (1) reminding the participant of
the planned activities, and (2) reminding the
participant to rate the activity and the mood.
Reminders for planned activities
The agent sends out such a reminder in case:
1. The participant requested a reminder (by indicated it
in the activity schedule).
2. In case of a pattern of missed activities:
a. If the participant has missed a specific activity 2
times in a row, or 2 out of 3 times. The reminder
is then sent half an hour before the activity is
planned.
b. If the participant has missed two activities in
general on a particular part of the day (e.g. never
performs activities in the morning). Again the
reminder is sent half an hour before the activity
has been planned.
Reminders for mood and activity rating
Next to the monitoring of activities being followed,
reminders of the rating of these activities are also
sent. This is done when during the past three days
less than 50% of the planned activities have been
rated. Reminders for mood rating are sent based on
the following mood rating frequency settings.
World Interaction Management. Process the
information about performed activities, ratings and
mood inserted into the mobile phone or via the
website. Send reminders to the mobile phone (i.e.
the patient).
Agent Interaction Management. Communicate the
fact that ratings have been given to the PAA.
APA: Activity Planning Agent
The APA keeps track of the planned activities and
reports this to the PAA.
Maintenance of Agent Information. Maintain
information about the activities that are planned by
the patient.
Agent Specific Task. Based upon the information
provided by the user and the options in the phase of
TOWARDS FULLY AUTOMATED PSYCHOTHERAPY FOR ADULTS - BAS - Behavioral Activation Scheduling Via
Web and Mobile Phone
377
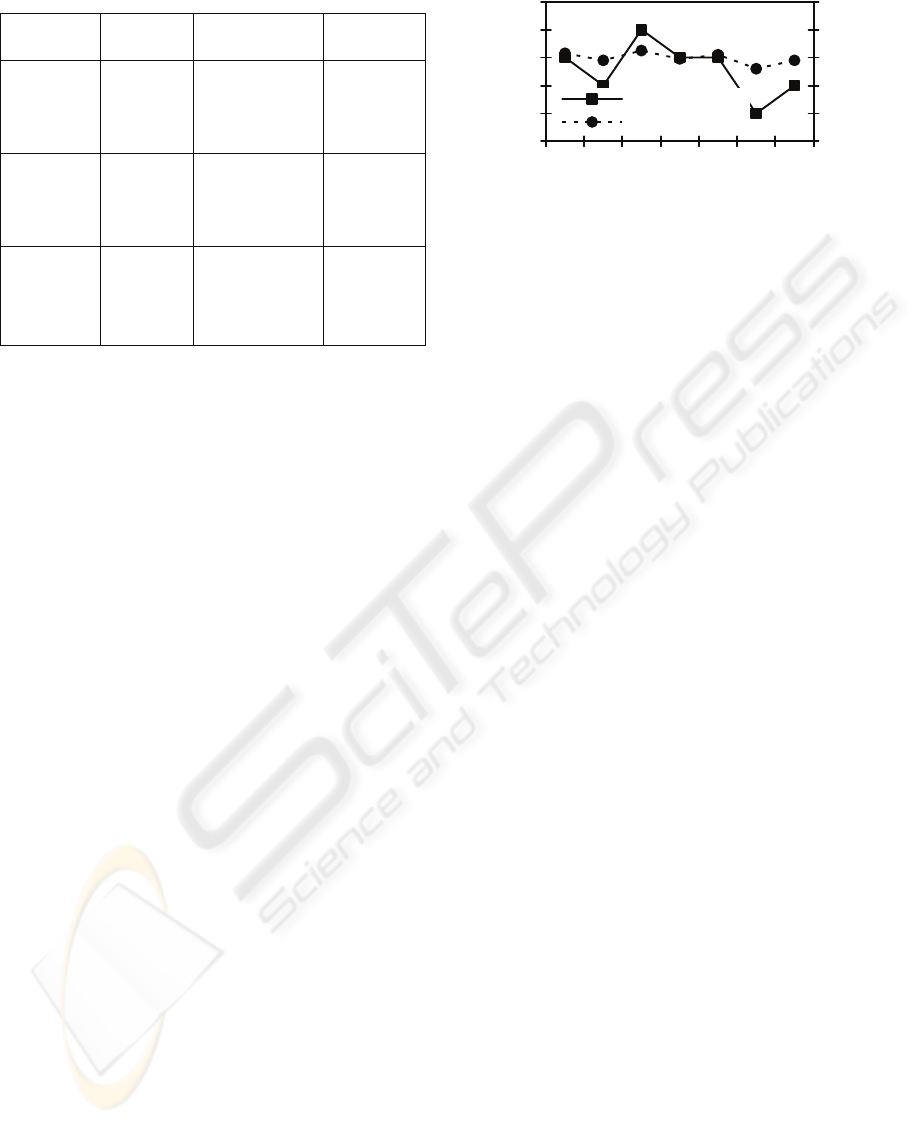
Table 1: Reminder frequency for mood rating.
Mood rating
setting
First
reminder
Second reminder
(email)
Contact care
taker
3 times per day
After four
misses,
afternoon of
day 2
After a full day
without response
upon first reminder
After a full day
without
response on the
second
reminder
1 time per day
After one
miss, evening
of day 2
After a full day
without response
upon first reminder
After a full day
without
response on the
second
reminder
1 time per 2
days
After one
miss, end of
day 3
After a full day
without response
upon first reminder
After a full
day without
response on
the second
reminder
the therapy: maintain a schedule of activities.
World Interaction Management. Process the
information inserted into the website.
Agent Interaction Management. Communicate the
schedule on request to the PAA.
FBA: FeedBack Agent
The role of this agent is to communicate information
via either the mobile phone or the website based on
the analyses of the PAA. This can be weekly
feedback, daily motivational remarks or general
conclusions about the progress of the therapy
derived by the PAA.
Maintenance of Agent Information. Maintain
preferences with respect to the media that is
preferred (and suited) for specific type of feedback,
and keep track of the feedback that has been sent.
Agent Specific Task. Triggered by the PAA:
generate weekly feedback, select motivational
messages, or forward analysis from PAA to the
patient.
Weekly feedback
The weekly feedback is meant to create awareness
of the participant that there is a relationship between
mood and the activities being performed. First of all,
in week one and two of the therapy overviews are
given of the number of activities in relation with the
mood (see Figure 2) as well as a similar figure
showing the relation between the rating of the
activities and mood.
Motivational remarks
Furthermore, also motivational remarks are sent; this
is triggered by the PAA when it receives information
from the AMA that the patient has rated either
his/her mood or activities. Maximum of one
message per day:
0
1
2
3
4
5
mon tue wed thu fri sat sun
# activities
0
2
4
6
8
10
avg. mood rating
# activities
avg. mood rating
Figure 2: Number of activities and mood rating per day.
1. Communicate the highest mood of the past three days
if this is higher than ‘6’, also communicate the
activities during that particular day: “Your highest
mood during the last three days was on X: a Y! That
day you performed the following activities: [list of
activities and rating].
2. Communicate an encouraging message in case the
rating for mood just inputted was ‘6’: “You rated
your mood at X now, how nice!”. In case it was ‘7’:
“You rated your mood at X now, that’s really nice!”.
Or in case of an ‘8’ or higher: “You rated your mood
X, that’s excellent!”.
3. Communicate the percentage of tasks that have been
performed, given that during the last 3 days at least 2
activities have been performed. In case more that
70% of the activities have been performed: “The last
three days your adherence to the planning was very
good, you performed X activities, which is Y% of the
scheduled activities”. In case less than 50% has been
performed: “You did not adhere that well to the
planning during the last 3 days, you performed X% of
the activities, which totals to Y activities. Try to
adhere to your agenda somewhat better”. In all other
cases: “During the last 3 days you performed X% of
your planned activities”.
4. If the average mood of day 4 of the week is at most
0.5 of the goal mood (in case applicable in the stage
the participant is in): “Your average mood this week
is X, you’ve almost achieved your goal. Keep this up
till the end of the week! Thereafter you can reward
yourself with Y”. Note that the last part of the remark
is only communicated in case specific rewards have
been specified.
In case none of the above hold or are sent on the
current day a tip is sent (from a list of expert tips).
World Interaction Management. Sends messages
to the website or the mobile phone.
PAA: Patient Assessment Agent
The task of the PAA is to assess the status of the
patient and to guide which feedback is given at what
moment to the patient via the FBA.
Maintenance of Agent Information. Maintain
information about the history of the patient, in terms
of prior mood ratings, activities performed, and
ratings for the activities. Maintain information
HEALTHINF 2010 - International Conference on Health Informatics
378

about the phase of the therapy.
Maintenance of World Information. Keep track of
the time.
Agent Specific Task. Based upon the information
present: derive conclusions about the performed
activities and ratings in the past week. When
considering the reported mood of the patient and the
performed activities, the following abstracted
remarks can be generated and sent to the FBA:
• Mood: “Your average mood during this week was A,
on day C your mood was lowest, namely B”.
• Activities: “You performed E fun activities this week,
on average this is D fun activities per day”.
• Mood in combination with activities: “Your low
mood on day C corresponds with few pleasant
activities, namely F. This shows that doing less fun
activities can decrease your mood level”.
After the two week period more elaborate
conclusion are generated. For the sake of brevity,
these rules are not shown.
Agent Interaction Management. Send messages to
be communicated to the patient to the FBA.
4 PILOT STUDY
4.1 Participants and Method
A total of nine participants joined the pilot study for
the system, all students at the VU University
Amsterdam, age ranging between 18 and 24
(average 21.2). They followed the intervention
during three weeks after a start-up meeting. During
that meeting, they received a Sony Ericsson M600i
mobile phone, a link to the website and a brief
explanation of the intervention. All participants were
instructed to follow all assignments and to test the
system. In addition, they were asked to describe any
technical errors in detail. After every week the
participants provided feedback about the
intervention. These interviews were semi-structured,
The questions were structured in five groups: look
and feel, technical, textual, reminders and weekly
feedback. In the end, the participants handed over
their phones and received €100 participation fee and
an online questionnaire was filled in.
4.2 Results
4.2.1 Weekly Feedback Sessions
Look and Feel. Most comments on the look and feel
of both the website and the application on the phone
were made after the first week. Negative comments
were about broken and illogically placed links, the
layout of the menu and the font size of some of the
forms. Four of the nine participants complained
about the simple agenda feature: they would have
liked to see more functionality such as a week
overview, setting an end time for activities and a
warning message when two activities are planned at
the same time. Remarks about the mobile phone
application were about functionalities people
missed, such as changing the comments about a
mood rating after saving the rating and adding or
changing agenda activities. Some participants had
difficulties interacting with the mobile phone itself.
Technical. The participants did not find many
technical problems with both applications. Some
complaints: the option ‘I did not do this activity’ was
missing, and it was possible to give a mood rating of
days in the future. Two participants received an error
message on their phone after saving a mood or
activity rating; this had to do with the motivational
remark that was shown afterwards.
Textual. Apart from some spelling and grammar
mistakes, the texts on the website were found very
clear. However, more explanation about the mobile
phone application and about when reminders could
be expected was required according to most
participants. In addition, no information about the
transition between steps was provided and some
participants were surprised when they automatically
started with the next step.
Reminders. The reminders for rating mood and
activities were judged as useful but the frequency
(see Table 1) could be improved. Some participants
found that the first reminder came too soon; others
found that it came not soon enough.
Reminders before a planned activity also showed
a pattern, although none of the participants noticed
it. They all said these reminders seemed random, but
were useful despite the randomness.
Weekly Feedback. Eight out of nine participants
said that they enjoyed reading the weekly feedback
and that the content matched their own experience
during that week. A few of the automatically
generated sentences needed more explanation, and
the percentages should be rounded.
4.2.2 Evaluation Questionnaire
The results of the final evaluation questionnaire
about how much the course was enjoyed are shown
in Table 2. To the question ‘how useful was the
course for you’ only one participant answered no,
six answered a little and two answered a lot. A
surprising result since none of the participants was
diagnosed with depression. Apart from the
TOWARDS FULLY AUTOMATED PSYCHOTHERAPY FOR ADULTS - BAS - Behavioral Activation Scheduling Via
Web and Mobile Phone
379

complaints about the frequency, the reminders that
the participants received on their phone were judged
as very useful. In general, the participants found
using the mobile phone for mood rating a nice
functionality, mostly because a mobile phone made
it easier to rate mood several times a day compared
with using a computer. The participants were also
asked to score the overall intervention on a scale of
1 to 10: the mean score was 7.1.
Table 2: Results of the evaluation, the scale is from 1
(totally disagree) to 5 (totally agree).
Question Mean answer
the information was new 2.7
I enjoyed viewing the website 3.8
I enjoyed working with the phone 3.8
the course was interesting 4.3
5 DISCUSSION
Based on the results of the pilot study, some changes
have been made in a new version of the BAS
system. The few technical issues are solved and
some texts were revised. Based upon the critic of the
participants on the weekly feedback and the
unexpected evolving to the next step, three new
general messages have been added. Furthermore,
the agenda functionality on the website is extended.
The rating system on the mobile phone is changed
slightly, so that people can edit the comment field
after saving the rating. The final adjustment is made
in the reminder system: besides the mood rating
setting (see Table 1), there is also a reminder
frequency setting with the options low, medium and
high. A combination of the two settings determines
when a reminder is sent. When the reminder
frequency is set to high, the participant receives a
reminder after missing two rating moments, when
set to medium, a reminder is sent after three missed
rating moments and when set to low after four
missed rating moments.
The pilot study indicates that advanced support
via a website and mobile phone during activity
scheduling intervention is technically feasible and
perceived as useful. In the near future, a second pilot
study will be conducted with between five and ten
participants who suffer from a depression. The
participants will be questioned in the same manner
as described in this paper. After processing the
results, an efficacy study will be performed with
around 100 participants with a depression to
determine whether their depression is lessened by
the BAS intervention system.
REFERENCES
Aarts, E.; Collier, R.; van Loenen, E.; Ruyter, B. de (eds.)
(2003). Ambient Intelligence. Proc. of the First
European Symposium, EUSAI 2003. LNCS, vol. 2875.
Springer Verlag, 2003, pp. 432.
Andersson, G., J. Bergstrom, F. Hollandare, P. Carlbring,
V. Kaldo & L. Ekselius (2005). Internet-based self-
help for depression: randomised controlled trial.
British Journal of Psychiatry, 187, 456-461.
Bosse, T., Hoogendoorn, M., Klein, M.C.A., and Treur, J.,
A Generic Architecture for Human-Aware Ambient
Computing. In: Mangina, E., Carbo, J., and Molina,
J.M. (eds.), Agent-Based Ubiquitous Comp. Amb. and
Perv. Int. book series., pp. 35-62, Atlantis Press, 2009.
Churchill R, Hunot V, Corney R, Knapp M, McGuire H,
Tylee A, Wessely S. (2001) A systematic review of
controlled trials of the effectiveness and cost-
effectiveness of brief psychological treatments for
depression. Health Technol Assess, 2001; 5: 35.
Cuijpers P, van Straten A & Warmerdam L. (2007)
Behavioral treatment of depression: A meta-analysis
of activity scheduling. Clin Psychol Rev; 27: 318-326.
Dimidjian, S. et al., Randomized trial of behavioral
activation, cognitive therapy, and antidepressant
medication in the acute treatment of adults with major
depression, J. Consult. Clin. Psychol. 74 (2006), pp.
658–670.
Gloaguen V, Cottrauxa J, Cucherata M & Blackburn IM.
(1998) A meta-analysis of the effects of cognitive
therapy in depressed patients. J Affect Dis; 49: 59-72.
Jacobson, N.S., Dobson, K.S., Truax, P.A., Addis, M.E.,
Koerner, K., Gollan, J.K., Gortner, E., & Prince, S.E.
(1996). A component analysis of cognitive-behavioral
treatment for depression. Journal of Consulting and
Clinical Psychology, 62, 295-304.
Lewinsohn, P.M., Youngren, M.A., & Grosscup, S.J.
(1979). Reinforcement and depression. In R. A. Dupue
(Ed.), The psychobiology of depressive disorders:
Implications for the effects of stress (pp. 291-316).
New York: Academic Press.
Leichsenring F. (2001) Comparative effects of short-term
psychodynamic psychotherapy and cognitive-
behavioral therapy in depression: A meta-analytic
approach. Clin Psychol Rev 2001; 21: 401-419.
Spek, V.R.M., Nyklicek, I., Smits, N., Cuijpers, P., Riper,
H., Keyzer, J.J., & Pop, V.J.M. (2007a). Internet-based
cognitive behavioural therapy for subthreshold
depression in people over 50 years old: A randomized
controlled clinical trial. Psy. Med., 37(12), 1797-1806.
Spek V, Cuijpers P, Nyklíček I, Riper H, Keyzer J & Pop
V. (2007b) Internet-based cognitive Behavioral
Therapy for mood and anxiety disorders, a meta-
analysis. Psy. Med. 2007; 37: 319-328.
HEALTHINF 2010 - International Conference on Health Informatics
380
