VIRTUAL MEDICAL DOCTOR SYSTEMS
Status Progress Report on Virtual Medical Doctor System (VDS)
Interaction Interface
Hamido Fujita, Jun Hakura and Masaki Kurematsu
Iwate Prefectural University, Iwate, 020-0193, Japan
Keywords: Emotional reasoning, Human user interaction, Intelligent interface, Facial analysis, Ego gram.
Abstract: Human computer Interaction based on emotional modelling is investigated and reported in this paper.
Human personality is analyzed based on ego-gram analysis and accordingly human "SELF" emotional
model is created. We have created as one part a computerized model which reflects a human user (in this
paper Diagnostician model) impeded as a computer based reasoning model and through it, an emotional
interaction between that model and the real human user is established. The interaction is based on a screen
mask attached to manikin head resemble the diagnostician, that through it the system can act to speak (i.e.,
mimicking diagnostician) with the patient user. In this paper the interaction scenarios and reasoning of the
virtual medical doctor or diagnostician are based on transactional analysis concept. We have implemented
the system and empirically, examined it, as experiment in public space for revision and evaluation. The
paper is reporting on the project outline, the usage of physiological issue in human reasoning through the
virtual system is developed.
1 INTRODUCTION
Recently there have been extensive move to towards
changing the way health care is delivered, financed
and regulated (Smith, 2000) Medical innovations
have become an important lever inquest of
improving efficiency. The main purpose is to
improve the efficiency so that more patients could
receive treatment more quickly without reducing the
quality of care (Mikkola, 2003). How to cope with a
rise in the need for the elderly care services is a
formidable issue facing all the industrialized
countries.
Unfortunately, Japan's health care system has not
been prepared enough to respond to the needs ahead.
Particularly Japan's home care services have heavily
been relying on voluntary labour of family members
with little social services available. The proportion
of the population 65 years and over has doubled
from 10% in 1985 to 20% in 2005, and is projected
to be 30% in 2023. (2006, NIPSSR).
In June 2006, the Diet (Japanese Congress) passed a
comprehensive package of reform to make the
delivery system more efficient. First, the average
length of stay in hospitals is to be decreased. To
achieve this goal, the number of long term care
Figure 1: Simple outline of the VDS.
(LTC) hospital beds will be reduced from the 2006
level of 380,000 to 150,000 by the end of fiscal year
2011 and converted to LTC Insurance facility beds
and assisted living (Leflar, 2005).
The system proposed in this paper participates in
helping physicians to manage the diagnosis
procedure using the same knowledge that physicians
have by copying (mimic) his/her style, mentality,
diagnosis routines and medicine recipes. It is not
replacing the physicians but it would participate to
utilize his/her knowledge for preliminary diagnosis
38
Fujita H., Hakura J. and Kurematsu M. (2010).
VIRTUAL MEDICAL DOCTOR SYSTEMS - Status Progress Report on Virtual Medical Doctor System (VDS) Interaction Interface.
In Proceedings of the Third International Conference on Health Informatics, pages 38-45
DOI: 10.5220/0002712000380045
Copyright
c
SciTePress
and health care services for patient for efficiency
purpose.
This paper contributes to present part of our
experimental work on building a virtual system
based or what we called as Virtual medical Doctor
System (for short VDS) to act as medicinal
diagnostician doctor, and interact with human
patient. The Worldwide, the prevalence of diabetes
is rising due to population growth, aging,
urbanization, and increasing prevalence of obesity,
and physical inactivity. We propose a system that
can participate in the care processes inside a medical
organization, by utilizing virtually the medical
doctor experience and knowledge for health care
services.
1.1 System Conceptual Outline
The VDS system is to work together with the
corresponding human medical doctor. So the system
(VDS) and the MD (Medical Doctor) are working
together in comprehensive coherency; the former is
complementary to the latter but not vice versa. The
former is to diagnose outpatient 1
st
and classify these
diagnosis into classes. Simple cases classes that the
VDS would take conclusion and set the diagnosis
procedure and accordingly take action (e.g., issue
drugs to the patient). The overall procedure is
supervised by the MD later on in a report. There are
other cases which the system concludes to have the
MD to participate in the final decision. In such cases,
the system sends the diagnosis reports to the MD
and provides an appointment to the patient in the
hospital queue. The system reads the queue data at
the management centre of the hospital reception.
And assign the patient to the queue. If the Doctor
found the assignment is appropriate (check mark
OK) then the system learned that the decision is
appropriate, however, by certain feedback from the
doctor the system can learn from the doctor’s
feedback. We provide a window at the doctor office
to fill a sheet of evaluation to enforce the learning
procedure for the system. Such evaluation sheet
would provide a learning mechanism to increase the
reasoning procedure for the diagnosis. However
such knowledge management would be based (i.e.,
mimic) on Medical Doctor A, therefore, it would be
stored in knowledge management on the top of the
management system. So when another doctor is
doing the outpatient diagnosis then the profile of
decision making related to that Doctor would be
used (i.e., recalled). So there is a general diagnosis
and on top of it there are diagnosis categorized on
physicians actual practices.
The paper is showing the state of art in making a
system that can interact with human user based on
new concept named as mental cloning mentioned in
(Fujita 2009). The cloning is based on analysis of
human medical doctor (HMD). The analysis is
projected using his/her observed styles as a person
and also as expert in medical diagnosis related
practices. So there are different style of categorized
knowledge reflecting such representation and related
reasoning.
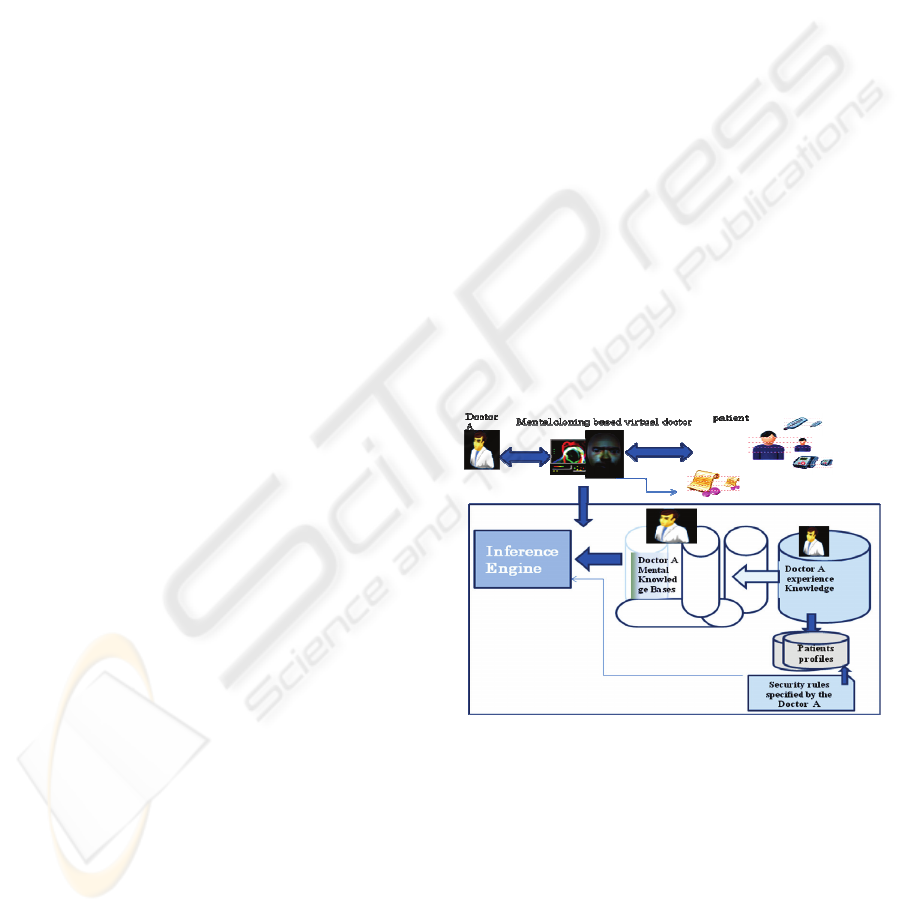
As shown in Fig.1. The system would to create
a virtual face (i.e., screen mask) of an actual doctor
that through it the patient communicates with pre-
assigned virtual version of that medical doctor.
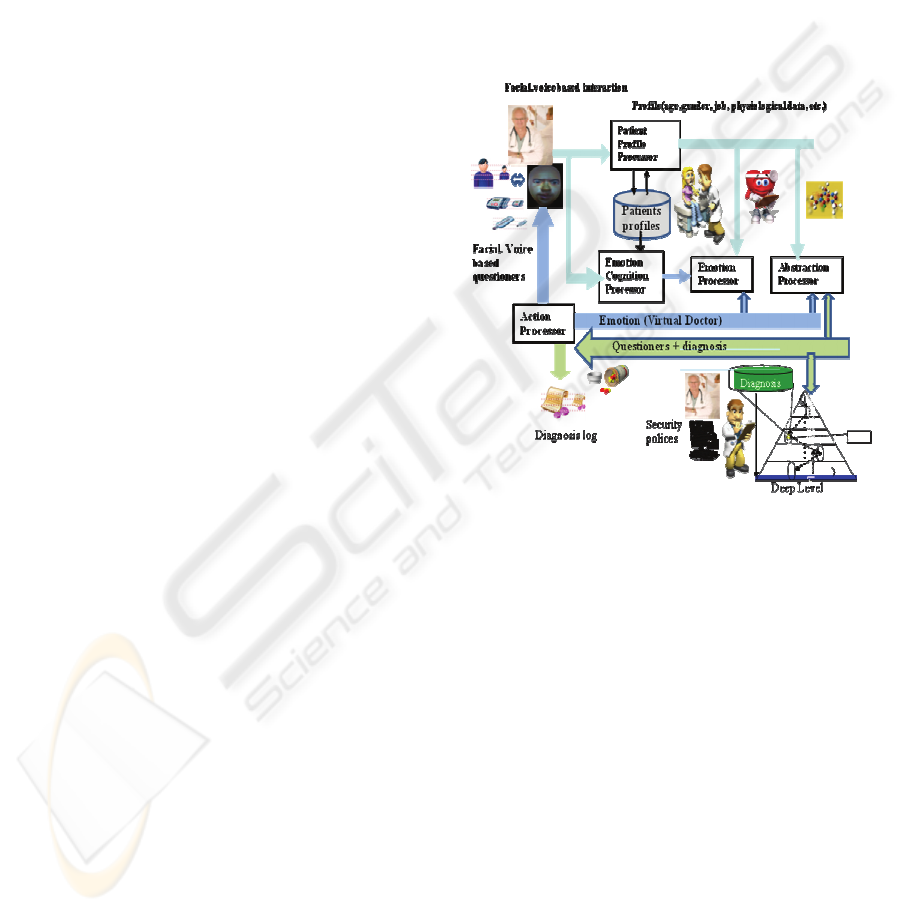
Figure 2: The VDS outline.
Physical doctor face is a mask copied and
attached on manikin.
Inside it there is a projector that reflects the 3
dimensional generated images on the mask screen
that reflects the actual facial real-time created
images of the medical doctor namely, Doctor A (Fig.
1). These animated facial image synchronized with a
spoken language in the same style of the actual
physical doctor is created. The style mimics the
actual doctor emotional expression as well his/her
diagnosis style. Also the MD speaks in natural
accent with emotions based on the patient mental
mode, estimated by the patient profile (age, gender,
ego data), and his/her situation automatically
measured by data resembles (blood pressure, body
weight, body temperature, and thermal analyzer).
These devices (equipments) are assembled to a
patient desk chair that the patient would sit on, and
automatically these measurements are collected and
transferred through serial connection to the virtual
VIRTUAL MEDICAL DOCTOR SYSTEMS - Status Progress Report on Virtual Medical Doctor System (VDS)
Interaction Interface
39
doctor system. These data are all measured and send
online to the VDS together with the mental status
(situation) of the user (patient), with estimated ego
state retrieved from the databases.
This system is been built by a support from Ministry
of Interiors affairs and communications of Japan
under SCOPE project. The security rules are
specified through an interface by the hospital staff
depends on patient portfolio related status.
We need to emphasis here that the diagnosis and
treatment done by the VDS is based on the actual
diagnosis and guidelines specified by the actual
doctor based scenarios that we have collected in
advance and specified in the system using Arden
Syntax which is open standards and representation
of medical knowledge. The Doctor A diagnosis
guidelines are represented as a collection of medical
logic modules (MLMs). Each MLM represents a
single decision that is grouped into three categories:
Maintenance, library, and knowledge. The
maintenance and library categories describe the
MLM’s paramedic issues, keywords.
The knowledge category describes the logic of
the MLM. We are investigating to use ASBRU for
knowledge diagnosis based on Doctor A and
generalizing them into diagnosis guidelines
representation of schemata at various levels of
details. This is the role of inference engine. We
would explain briefly, this in Sec. 4. On more details,
please refer to other paper in this proceedings
elaborating on the inference issues.
2 VIRTUAL DOCTOR SYSTEM
In our project computer systems (machine)
understand our emotion and interact with us based
on internal psychological reasoning and type of
information. The mind can be viewed as community
of selves (Horowitz, 1985). A state of mind is a
relatively coherent pattern a composite of diverse
forms of experience and expression that appear
almost simultaneously. These states of mind are
accompanied by characteristic expressive behaviors,
tone of voice, facial expression, and also other
invariants, like type of color, type of current
employment, and other invariants that collectively
estimate the emotional state of the patient.
The objective of the system is to have hollow
gram that interacts with the patient based on the
mental cloning of the subject person through the
hollow gram (i.e., HMD), and accordingly we can
have the human user (patient) to interact with the
system based on facial based analysis The whole
system outline is shown in Fig.2.
The user age and gender is estimated using a tool
developed with OKI Co. The tool can estimate the
gender and the age of the user. Also, at the moment
our system simultaneously has a touch panel that the
patient can enter his/her other personality related
information through icons based interface on a
screen beside his/her desk. The system
measures/collects the user personality based on a
concept we called it universal templates (Fujita,
2008) that is used to estimate the user profile based
on the collected data. The user information related to
his/her, set of invariants that specified, by answering
questionnaires related to his favourite colours,
hobbies and type of employment (Hakura, 2009).
The interaction is based on projection of the system
(Medical Doctor) on a person onto oneself.
The reasoning between the patient and VDS, is
based on projection on a patient onto doctor’s self.
From this prospective as the doctor is expertise
person, she/he is projecting someone (i.e., patient)
onto him/her self, bounded by the circular space,
specified by the interaction space between the
system (VDS) and the patient. It is a reflective
interaction based on projection between the subject
(patient) and the object is (VDS), by sharing the
experience of the system projected into the patient
related states. For that purpose, we have used
modular approach. Emotional module, inference
module and other modules that all synchronously,
are interacting with the user based on patient
projection for diagnosis purposes. We have
psychologically cloned the user main “self”, based
on the user physiological analysis, and modelling.
Mental cloning ( Fujita, 2009) is aconcept specifying
the type of harmony and the connection between the
subject user mentality and other object. The subject
of the user type mentality purposes specify the type
of engagement that the object should have for
successful interaction. The specialization of such
engagement; in the context of mental cloning
typifies the style of mental reasoning in the object
(VDS) as the subject (patient) progresses and
behaves.
Figure 3: The five ego states.
AC
Parent Ego state
P
A
C
Child Ego state
Adult Ego State
Adapted Child
Ego State
CP
NP
Critical Parnet
Ego State
Nurturing Parnet
Ego state
FC
Free Child
Ego state
HEALTHINF 2010 - International Conference on Health Informatics
40
The synchronic view (high degree of emotional
representation to the environment) of self is also
presented. The example of the mental user cloning
we used was for Medical doctor mentality analysis
and technical background on how to do diagnosis on
people. These introjections are to specify the
physiological view of both the work outcome and
mentality of the object physical doctor.
2.1 Ego Gram based Transactional
Analysis based Model
Transactional analysis is a development approach of
self perception and its impact. The theory discovered
first by (Eric Berne, 1971) and it stated that much
can be discovered about an individual by analyzing
the type of interactions (transactions) engaged in.
TA (Transactional Analysis) suggested that we each
had an Inner Parent, an Inner Child, and an Inner
Adult personality parts that collectively determined
our feelings, beliefs, and behaviour. The
Transactional analysis life position is a function of
the performance of a person and the attention
received from other party (VDS System). The
assumption is that all people want attention
preferably positive (praise, encouragement). But if
positive attention is not given, negative attention is
selected. Self perception is an essential issue
specifying attributes related to behaviour.
Acceptance of self, ability to accept and relate to
others in positive prospective is a desirable outcome.
It is essential to foster a positive view of self for
Figure 4: The system implementation outline.
0
5
10
15
20
CP NP A FC A C
Label
HMDEgogram
Affliation
Figure 5: Ego gram of Doctor A.
each user. (Dusay, 72) narrowed the large number of
potential ego states to five: Nurturing Parent,
Critical Parent, Adult, Adapted Child, and Natural
Child. TA
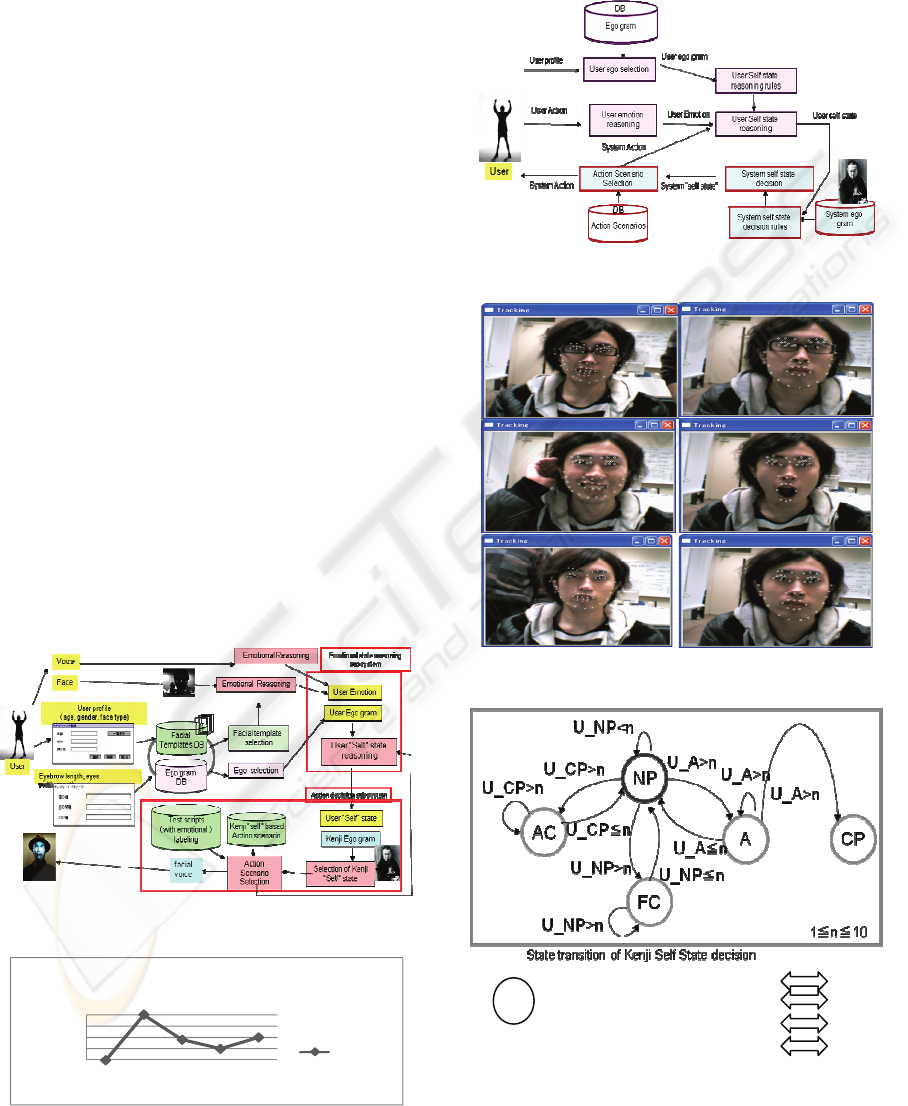
Figure 6: The mental cloning based system components.
Figure 7: The facia extraction of user patient states.
Figure 8: States transitions between patient and doctor.
MD self state
U: User (patient) self state
N: number of appearance
FC
NP
CP AC
A
FC
AC
A
VIRTUAL MEDICAL DOCTOR SYSTEMS - Status Progress Report on Virtual Medical Doctor System (VDS)
Interaction Interface
41

conceptualizes personality in terms of five
functional ego states: Critical Parent (CP), Nurturing
Parent (NP), Adult (A), Free Child (FC), and
Adapted Child (AC). These five ego states have
been widely researched with varying degrees of
scientific rigor. A number of researchers have
attempted to demonstrate reliability and construct
validity for these ego states. The Tokyo University
Egogram is reportedly in use in Japan. Egogram is a
sort of psychological scales theoretically based on
Transactional Analysis. Tokyo University Egogram
(TEG) published in 1984 was a questionnaire with
reliability and validity. Since then, it has been
widely used in various fields such as medical care,
education, and industry. The second edition of TEG
was published in 1993 after three years of basic
studies. In this study, we investigated the use of
TEG 2.0 for its personality application to predict the
self of HMD and the patient user for best interaction
based on the finding of the self through experimental
analysis of the egogram using TEG2.0. The TA has
been studied (Trautmann, 1981) for personality
analysis, reflected in the TEG system for studying
human personality.
As specified by Berne and modified by (Dusay,
1982) the five ego states are as below:
1. A nurturing parent subself: supports care,
attention, and positive reinforcement.
2. An evaluative parent subself; critic, pusher, it
reflects the norms and values of the society and
set up standards and measures.
3. A central organizing subself, who is the self that
often works with the observer and act as the
leader.
4. A good socialized adapted child subself. This is
obedient, conforming child who tries to please
authorities, and it lacks creativity.
5. A natural child sub self, creative, nonconforming,
spontaneous and playful. (As shown in Fig.3.)
A state of mind is a relatively coherent pattern a
composite of diverse forms of experience and
expression that appear almost simultaneously. A
survey has been carried out to collect data on
Japanese subject persons of different gender (male,
female), and different ages (children, adults and old
age). Each person has entered their responses for
questionnaires (TEG 2.0 based 60 questions).
The object doctor and subject patient users (in
advance for database personality construct purposes)
after entering the user profile information (gender,
age range), would answer (response) to these 60
questions as Yes, Yes/No and No. The Scoring
answers as specified by TEG would be 2, 1, and zero,
respectively. The collected sum answer would
represent their ego state as number. One example for
Doctor A ego gram is shown as in Fig.5. The highest
value would represent the best estimation of self
state of that person as one of the any state in Fig.3.
These ego grams for personality extraction for
patient purposes are stored in database and indexed.
There are five categories of age class and these are:
Child (6 to 12) years, junior young (12 to 18), senior
young (18~26), adult (26~45), senior adult (45~60),
Old (61~). These categories are set according to the
educational system and working structure in Japan.
1
st
category to be related to elementary school class,
2
nd
category is related to intermediate school and
high school. The 3
rd
category is relative to university
class and young inexperienced workers. The 4
th
category is related to middle class workers of
different slices.
The 5
th
class is relative to experienced workers and
advanced middle class. The last class is the old
and retired class people. Such classifications reflect
the relative social characteristics of people as
general class reflecting each class personality and
its relative characteristics as specific specialization
on each class.
3 ACTION DECISON MODEL
Our system outline is as presented in Fig.4, and
Fig.7. The patient user when visiting VDS is sitting
on chair where there is touch panel beside him/her.
The patinet enters information by clicking on check
box, on his gender selection box and age class box.
The system uses a generative program to comput the
user personality using what we have called a
universal template (Fujita, 2008). The user’s face;
using the active appearance technology (Fujita,
2007) is been the computation subject to compute
and categorize the searching keys to localize the best
estimation to select the best “fit” of the human user
from the template data base for emotional based
reasoning. The Templates data base is a collective
database of samples data of categorized according to
user personality type. Each template is a set of six
emotions (sad, happy, disgust, surprise, angry, fear)
as shown in Fig.7, and neutral (no emotion). These 7
types of face templates set are been categorized
according the user gender key and age class key.
The localization and detection of the user emotion is
based a systematic estimation approach using OKI
FSE V4, SDK (OKI). For the eyes centre there is
one feature point for each eye. For the eyelids there
are 5 feature points for each eye. For the eyebrows
there are three points for each eyebrow. There are 8
feature points for the mouth and three feature points
HEALTHINF 2010 - International Conference on Health Informatics
42
for localizing the nose. Also, there are 12 feature
points specifying the contour of the face from the
ears down around. Using these feature points we
can track the emotional feature of the human user
based on the value difference between the tracked
point and the labelling dictionary in the database
specifying the best emotional estimation and the
selection of the emotional state among the six
Ekman universal emotional states (Fujita, 2009).
4 HCI FOR VDS SYSTEM
In this part we would discuss how to define and
establish the “self” or internal mental mechanism
through which the system (VDS), would use to
interact with the mental self of the human user. We
have used an experimental survey to collect data.
Based on these collected data we have created the
mental self.
The Doctor Ego gram has been studied and
experimentally brought up using empirical analysis.
Doctor A personality and his/her answer related to
the TEG Questionnaires have been carried using an
empirical study analysis and analytical based
observations. This has been done by asking the
doctor to fill and answer questions based on TEG 60
questionnaires, and defined in the same way as
shown on Fig.5.
The action scenario between the patient and the
VDS would be based on the styles and wordings that
are used by the MD him/her self in actual and other
diagnosis practices. This part is not yet reported here
in this status report paper due to space. However the
style would be related to looking to the issues from
minutes things to larger parts, collecting the micro
views and macro views in different prospective for
analytical based reasoning. These collected images
are analyzed and reasoned in VDS related to the
style that the MD usually do during his routines
diagnosis. As the MD is in nature is a Japanese
character, so this also would be considered in the
system reflecting the psychological and cultural side
into the reasoning process. This conceptual
interaction is based on transactional analysis as
shown in Fig. 8, assuming that the style of
communication between the user and VDS system is
Rogerian style (based on Cal Rogers’ work in
psychology) which
encourages the involved two
parties in positive style of engagement based on
empathic position assuming that they share to
explore common ground related to medical
diagnosis. As shown in Fig. 9 the state transition of
VDS’s self change due to emotion state change of
the patient user. Fig. 7 observes the user emotion
state by computing the change in the feature points,
and accordingly MD system can estimate the
emotion state of the patient and integrate it with in
the diagnosis for inference with other observation
extracted from the keywords. The system
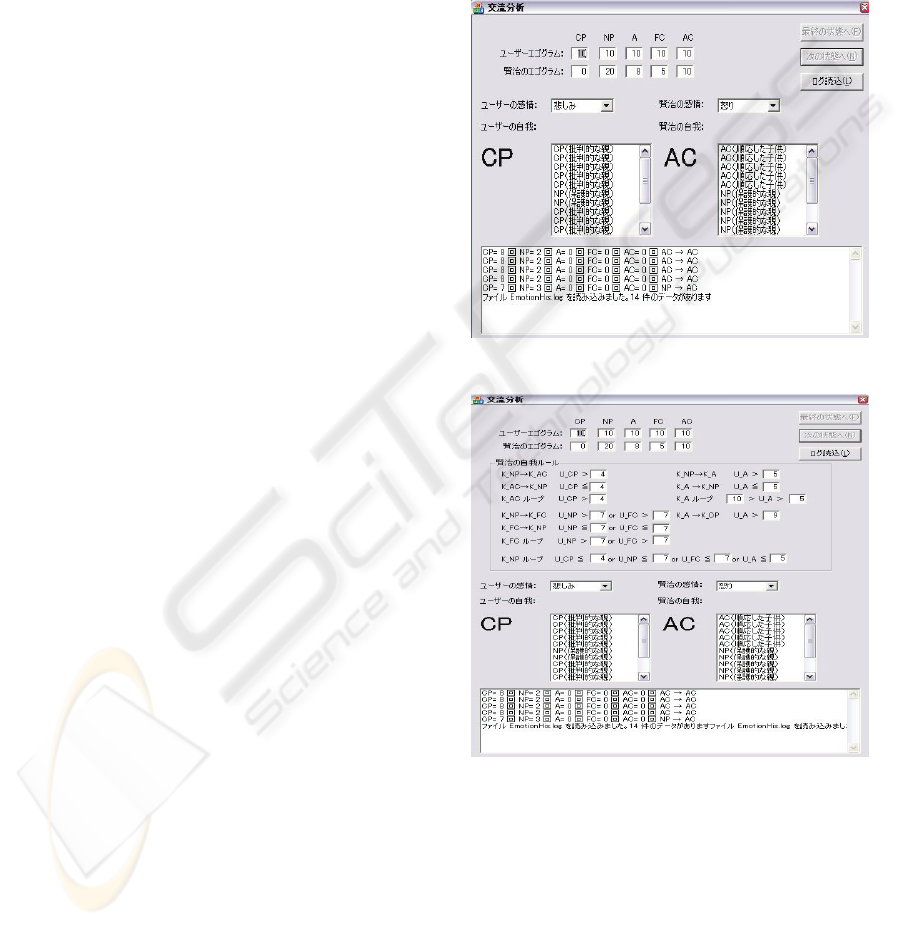
implementation is as shown in Fig.9 and Fg.10.
That shows the snapshot of the system
implementation.
Figure 9: Implementation of Doctor A self and patient self.
Figure 10: State Transition implementation of VDS.
The system observes to the user in cyclic time
period of 10 sec margin for incremental type
reasoning. VDS system is the initiative to talk with
the user. The system estimate and compute the
emotional state of the patient user while VDS
system is talking, to collect if there is any change in
the emotional state of the user and the appropriate
keywords for inference purposes.. At the initial state
the user emotional state is set as determined by the
best match of that user with the best estimate for the
VIRTUAL MEDICAL DOCTOR SYSTEMS - Status Progress Report on Virtual Medical Doctor System (VDS)
Interaction Interface
43

selected ego gram that set with the user personality.
Then the user initial personality set is been selected.
The system (i.e. VDS) would talk (with emotion)
and check and collect if there is any change in the
user emotion according to the rules shown below. If
there is a change then Doctor A would record this
state and select the appropriate action and related
scenario to that state. The action can be represented
by appropriate transaction state, selected among the
5 states mentioned in Fig. 3. The system should have
a trace to all states so that it can return back to its
original state when there is no specific emotional
state change in the user emotions. If the patient user
emotion state is neutral, this reflects that the user is
adult state. If the user is happy state, then the user is
nurturing parent state. If both the VDS system
emotion state and the estimated patient user emotion
state are the same, then the patient user emotion
state is NP. If the estimated patient user emotion
state is surprise then the user state is FC. If the
estimated patient user emotion state is «angry» or
«sad» or «disgust» (negative response) then the
patient user emotion state is CP. The
implementation is shown in Fig. 9 and Fig.10 and it
is as follows:
Self state Condition
K_NP→K_AC U_CP>4
K_AC→K_NP U_CP≦4
K_AC loop U_CP>4
K_NP→K_FC U_NP>7 or U_FC>7
K_FC→K_NP U_NP≦7 or U_FC≦7
K_FC loop U_NP>7 or U_FC>7
K_NP→K_A U_A>5
K_A →K_NP U_A≦5
K_A loop 10>U_A>5
K_A →K_CP U_A>9
(Transition finish)
※ K_CP→K_A and K_CP Loop not exist.
K_NP loop: U_CP≦4 or U_NP≦7 or U_FC≦7 or
U_A≦5
We need to mention here due to space limitation we
have not discussed the issue of voice (speak)
generation and emotional extraction of
voice(Kurematsu et.al 2009). The voice and face is
been synchronized in real time and articulated to the
generated scenario by the VDS according to CIGs.
5 REASONING SCENARIOS
The paper reports here part of our project outcome
that is related to interaction between VDS avatar and
Patient. The voice recognition issues is been also,
discussed in (Fujita, 2009). The action scenario is to
create a diagnosis based on the guidelines given by
the Doctor A. Doctor A is a nominated Doctor which
is the object system would mimic to interact with
patient through VDS avatar. Implementing medical
guidelines of Doctor A in active computer-based
decision participates to enhance the best practices of
medical services on behalf of Doctor A. Our system
reported here briefly, participates to provide
cognitive interaction between real patient and
specialized doctor A (avatar) through computer
interpretable guidelines (CIGs).
We have to represent various types of diagnosis
guideline using formal representation. Consequently,
acquire, verify and evaluate these formalized
guidelines for daily routines diagnosis.
The system would be facilitated at hospital A where
Doctor is working. So the system would use the
computer interpretable guidelines (CIG) based on
Doctor A as first diagnosis procedure to specify and
categorize (classify) patients according to their
status and profile. Please note that the classification
and diagnosis is based on Doctor A cognitive
interaction. The reasoning knowledge (eg. Doctor A
methods and Doctor B methods) should be separated
from domain knowledge (eg. laboratory tests, used
drugs). Also the representation should support the
use of standard data model and medical
terminologies like HL7 UMLS (Tanaka, 2000)
We are using semantic net for representing the
reasoning part. The domain knowledge is specified
by automatic retrieval by establishing a link between
the ontology and the patient database. This is
reported in another paper in this conference.
6 CONCLUSIONS
This paper is reporting a progress status of our
project related to mental cloning based concept on
how to reason and represent human emotion in
scientific way and use that emotion to reason with
human user. We articulate realization to MD
objective machine. The MD is usually a real person
that based on interviews, we extract his personality
that is to be used into the system and act on his
behalf on mental basis using his/her routine
diagnosis procedure. The MD views have been
integrated into our representation in MD ego gram.
Using this with other related information we create
a system that can interact with the patient user based
on Transaction analysis protocol. The system would
be examined in Beta space at a hospital where that
MD is working.
This would have people (patient users) interact
with VDS system to experience his/her (i.e., MD)
emotional transition to the MD created personality
HEALTHINF 2010 - International Conference on Health Informatics
44

and his/her transactional based analysis with patient
users. The collected data of the evaluation would be
examined to revise the VDS’s personality and
diagnosis knowledge. The personality is reflected
from majority of answers that reflect how people
can look to the VDS through his work and the
gathered cognitive thinking on him/her. We think
this approach may contribute to create the
foundation of mental cloning based computing that
can contribute to establish the best engagement and
harmony between human and machine taking into
consideration the human emotional recognition as
computational mechanism in this interaction, for
medical services.
The inference engine of the knowledge bases of
the VDS knowledge hierarchy is briefly, reported in
a companion paper in this proceedings. The
prototype version of the system is to be used in
medical practices in Kitamatuzono clinic, Morioka,
Japan. The related statistical data on experimenting
the work is to be reported in the near future.
ACKNOWLEDGEMENTS
This research is supported by the Ministry of
Internal Affairs and Communications of Japan
under the Strategic Information and
Communications R&D Promotion Programme
(SCOPE). We appreciate the supports provided by
Medical Doctors in Iwate region Hospitals to mimic
the diagnosis procedure into our system for testing
purposes.
REFERENCES
Fujita, H., Hakura, J. Kurematsu, M. 2009 “Intelligent
human interface based on mental cloning-based
software” International Journal on Knowledge-Based
Systems, Elsevier, 22 (3), pp. 216-234, April.
Pierre-Yves Oudeyer: 2003 «The production and
recognition of emotions in speech: features and
algorithms» , International Journal of Human
Computer Interaction, Vol.59(1-2) pp.157-183.
Fujita, H., Hakura, J. Kurematsu, M. Chida, S. and
Arakawa, Y. :2008 “Empirical based Techniques for
Human Cognitive Interaction Analysis: Universal
Template Design”,the 7th New Trends in Software
Methodologies, tools and Techniques (Proceedings of
SoMeT_08), pp.257-277. IOS press, ISBN: 978-1-
158603-916-5
Fujita, H., Hakura, J. Kurematsu, M.: 2007 “Virtual
Human Interaction based on Emotional Cognition”,
Innovations 07, IEEE Computer Society, publication
Horowitz: 1988: Introduction to Psychodynamics. A New
Synthesis: By Mardi J. Horowitz. New York: Basic
Books, Inc.
David Lester 1993 «On the disunity of the self: A systems
theory of personality», J. Current Psychology,
Springer New York, Volume 12, Number 4/ Dec.
pp312-325
Berne, E. 1961 Transactional analysis in psychotherapy:
A systematic individual and social psychiatry London:
Souvenir Press (Originally published in 1961 by N.
Y.: Grove Press)
Dusay, J. M. 1972 Egograms and the “constancy
hypothesis” Transactional Analysis Journal, 2, 37-42.
Stewart, I. 2001 Ego states and the theory of theory: The
strange case of the little professor Transactional,
Analysis Journal, 31, 133-147.
Trautmann, R. L. & Erskine, R. G. 1981 Ego state
analysis: A comparative view Transactional Analysis
Journal, 11, 178-185.
Woollams, S. & Brown, M. 1978 Transactional Analysis:
A modern and comprehensive text of TA theory and
practice MI: Huron Valley Institute Press.
J.Weizenbaum, 1966 "ELIZA - A Computer Program for
the Study of Natural Language Communication
Between Man and Machine", Communications of the
Association for Computing Machinery, Vol.9, pp.36-45.
Hakura, J., Kurematsu, M., Fujita, H., 2008 An
Exploration toward Emotion Estimation from Facial
Expressions for Systems with Quasi-Personality,
International Journal of Circuits, Systems and Signal
Processing, Vol. 1, No. 2, 137-144.
Hakura, J., Kurematsu, M., Fujita, H 2009 «Facial
Expression Invariants for Estimating Mental States of
Person» Frontiers in Artificial Intelligence and Appli-
cation series, Volume 199, New Trends in Software
Methodologies, tools and Techniques (SoMeT_09),
pp.518-530, IOS press, ISBN: 978-1-60750-049-0.
Kurematsu, M., Ohashi, M. Kinoshita,O. Hakura, J. And
Fujita, H., 2009: “An Approach to implement Listeners
Estimate Emotion in Speech” Frontiers in Artificial
Intelligence and application series, Volume 199, New
Trends in Software Methodologies, tools and
Techniques (SoMeT_09),.pp531-540, IOS press,
ISBN: 978-1-60750-049-0.
OKI FSE Ver. 4, A Face Recognition Middleware for
Embedded System: http://www.oki.com/en/press/
2008/07/z08019e.html
Tanaka, M., Noguchi, M 2000: Concept Retrieval of
Medical Text using UMLS, Japan Journal of Medical
Informatics, Vol.20, pp.934-935.
Smith, 2000, Reforming Markets in Health Care-An
Economic Perspective, Open University Press,
Buckingham, 2000.]
Mikkola, 2003, Hospital Pricing reform in the public
health care system- an empirical case study from
Finland, International journal of Health Care Finance
and Economics, 3 (4) 267-286.
NIPSSR, 2006; National Institute of Population and Social
Security Research, “Population Statistics of Japan,”
2006; Tokyo: NIPSSR.
Leflar,2005: Leflar, R.B and F. Iwata, “Medical Error as
Reportable Event, as Tort, as Crime: A Transpacific
Comparison,” Widener Law Review 189, no.25 (2005).
VIRTUAL MEDICAL DOCTOR SYSTEMS - Status Progress Report on Virtual Medical Doctor System (VDS)
Interaction Interface
45
