
AUTOMATIC SCREENING OF ACCELERATION SIGNAL
DURING PIVOT-SHIFT TEST BASED ON PEARSON’S
CORRELATION COEFFICIENT
Cecilia Signorelli, Nicola Lopomo, Simone Bignozzi, Stefano Zaffagnini and Maurilio Marcacci
Biomechanics Lab, Rizzoli Orthopaedic Institute, 1/10 Di Barbiano Street, Bologna, Italy
Keywords: Pivot-Shift test, ACL reconstruction, Acceleration, Pearson’s correlation coefficient, Template.
Abstract: Anterior cruciate ligament injury produces a pathologic kinematics of the limb that can lead to the evidence
of a pivot-shift (PS) phenomenon. PS-test, specifically performed to highlighted this knee dynamic
instability, is however difficult to quantify. From a clinical point of view is therefore mandatory to find a set
of parameters able to quantitatively characterize PS phenomenon, thus distinguishing between pathologic
and healthy knees. This study proposed a methodology able to automatically quantify PS phenomenon,
analysing the signal recorded by means of a tri-axial accelerometer while executing PS-test itself. A signal
template, which reproduced the 3D acceleration average trend while PS phenomenon occurs, was passed
along the signal in order to recognise the presence of similar patterns. The recognition of the signal
interesting share was based on the calculation of the Pearson’s correlation coefficient between the template
and the corresponding part of the windowed signal. The data acquisition concerning to the first 35 patients
was used to testing the template; in this analysis we considered both the data relative to pathologic and
healthy knee, as well as pre- and post-anaesthesia data, in order to evaluate the influence of active muscular
resistance. The methodology followed had assured a recognition of PS repetitions with an accuracy of
96.7%, a sensitivity of 81.9% and a specificity of 99.3%; therefore can be considered a valid and easily
computable method for the automatic screening of the acceleration signal during PS test. In the future this
method will be uptake in order to quantify the possibility to discern between pathologic and healthy knee.
1 INTRODUCTION
Scientific literature agrees with the fact that pivot-
shift (PS) phenomenon is one of the essential sign of
knee dynamic instability, that can specifically
highlight an injury of the anterior cruciate ligament
(ACL). Moreover clinical results of PS test are more
correlated with functional outcomes, patient's
satisfaction, joint instability and relief of symptoms,
whereas clinical examinations addressing static
instabilities (i.e. Lachman and drawer tests) are less
related to patient’s subjective status (Kocher, et al.,
2009).
The main problem in using PS test is associated to
the difficulty of quantifying the test outcome; this
difficulty is in fact due to the complexity of the
manoeuvre itself, being based on a valgus stress
while flexing the limb and maintaining the foot
internally rotated (Jacob, et al., 1987). In fact,
surgeons who carry out PS test, usually affirm to
sense a sort of 'clunk' while testing a pathologic
knee; this qualitative evaluation is extremely
difficult to quantitatively define and thus
quantitatively differentiate an ACL-injured limb
with respect to a healthy one is a not simple task.
During the last decades qualitative methods and
several devices have been suggested to standardize
the level of ACL injuries correlated to joint dynamic
instabilities, but they revealed a quite complex and
bulky set-up for an outpatient’s clinical use or
allowed only a partial assessment of joint laxity
(Lopomo, et al., Kuroda, et al., Dierman, et al.,
Labbe, et al., 2008; Amis, et al., 2008, 2005;
Mushal, et al., 2007; Csintalan, et al., 2006; Bleday,
et al., 1998).
For these reasons a method which can provide a
reliable diagnosis of dynamic knee instability with
fewer and simpler measurements, can surely be of
benefit for clinical scope.
236
Signorelli C., Lopomo N., Bignozzi S., Zaffagnini S. and Marcacci M. (2010).
AUTOMATIC SCREENING OF ACCELERATION SIGNAL DURING PIVOT-SHIFT TEST BASED ON PEARSON’S CORRELATION COEFFICIENT.
In Proceedings of the Third International Conference on Bio-inspired Systems and Signal Processing, pages 236-239
DOI: 10.5220/0002720402360239
Copyright
c
SciTePress
As reported in literature (Colombet, et al.; Hoshino,
et al., 2007), one of the most interesting parameter to
investigate can be the acceleration reached by the
joint during the PS manoeuvres itself, representing a
possible correlation with the alteration in the fluidity
of the movement due to the presence of PS
phenomenon. The main objective of this study was
therefore to develop and validate a methodology
able to automatically quantify the PS test, giving
also a clinical reliability to the analysis. In particular
3D acceleration was recorded during PS manoeuvres
by means of a commercial triaxial accelerometer and
the output signal was automatically analysed in
order to filter the noisy part and to automatically
extract the clinical information related to the PS test.
2 METHODS
We conducted the presented study on 35 consecutive
patients, with acute or chronic ACL injury, that
underwent ACL reconstruction between August
2008 and August 2009 in our Institute. The
performed experimental procedure was established
on the first 15 patients that were not included in this
study. The applied clinical protocol was approved by
the Institutional Review Board of the Institute.
The system used to acquire 3D joint acceleration
during PS test was a triaxial accelerometer sensor
(Inertis-link, Microstrain Inc., Williston, VT, USA);
the device was connected wirelessly to a dedicated
laptop on which, by means of a simple interface, the
operator was able to monitor in real-time the
patterns of acceleration and to acquire the 3D data.
The sensor was not-invasively mounted on the skin
of the patient and securely fixed by means of a
specific strap between the lateral aspect of anterior
tuberosity and Gerdy’s tubercle, in order to achieve
an optimal stability. The PS test was repeated 3
times by an expert and a novice orthopaedic
surgeon. Each surgeon realized test repetitions, both
on pathologic limb and healthy one. The test was
repeated by the expert surgeon also before and after
the general or regional anaesthesia.
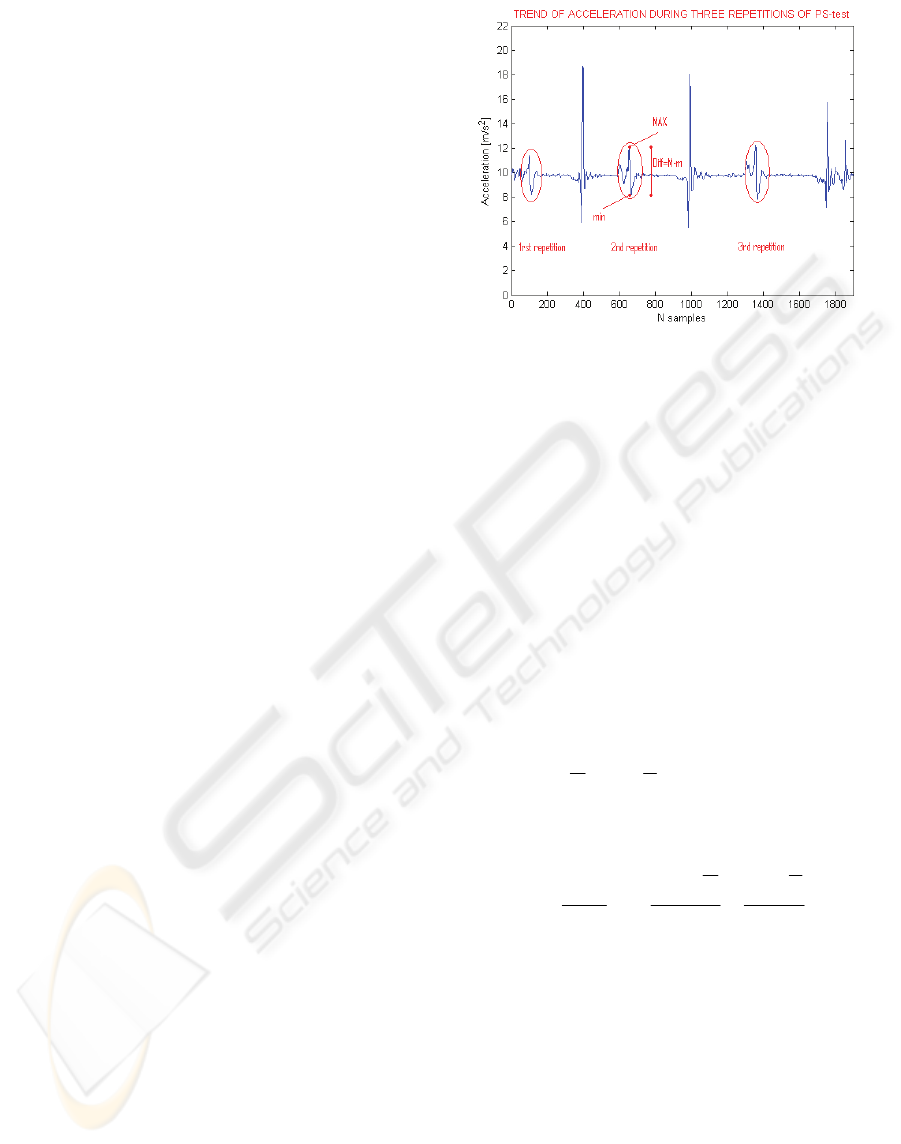
We used the module of 3D acceleration measured by
the sensor, as the most significant parameter to be
analysed during the PS manoeuvre. In particular we
proceeded to extract maximum (MAX) and
minimum (min) value of the acceleration, their
difference (Diff) and the first derivative of
acceleration (in physics indicated as “jerk”) as an
indication of the smoothness of the performed
movement. The processed signal and the parameters
chosen for the diagnosis are reported in figure 1.
Figure 1: Typical trend of acceleration during the three
repetitions of pivot-shift test. “MAX”, “min” and “Diff”
are the parameters, besides jerk, evaluated in this study.
The automatic data processing is based on the
calculation of Pearson’s correlation coefficient by
means of overlapping a specific template and the
signal recorded. The template was defined as the
average trend manually identifying the repetitions
obtained by the first 35 patients, that were thus used
as reference sample. As known, Pearson’s
correlation coefficient (R, with -1 ≤ R ≤ 1) generally
indicates the strength and direction of a linear
relationship between two variables; in our case the
first variable is the template and the second is the
corresponding window on the processed signal, so
that R can be helpful to recognize the presence of a
trend similar to what represented in the template. For
instance, supposing to have two variables X and Y,
with means
X
and
Y
respectively and standard
deviation Sx and Sy, n is the number of samples of X
and Y, the correlation R is computed as shown in the
equation 1:
⎟
⎟
⎠
⎞
⎜
⎜
⎝
⎛
−
⎟
⎟
⎠
⎞
⎜
⎜
⎝
⎛
−
−
=
∑
=
Sy
YYi
Sx
XXi
n
R
n
i 1
1
1
Equation 1: Calculation of Pearson’s correlation
coefficient (R).
During each iteration of the algorithm, the
evaluation took into account a shear of signal with
the same length of the template sample-by-sample
until the last one.
A threshold for the value of coefficient R over that
the algorithm recognize the PS repetition was
manually fixed to 0.7, on the basis of the reference
sample. Moreover in order to increase the reliability
of the algorithm specific thresholds were defined
relative to the clinical parameters chosen for the
AUTOMATIC SCREENING OF ACCELERATION SIGNAL DURING PIVOT-SHIFT TEST BASED ON PEARSON'S
CORRELATION COEFFICIENT
237
diagnosis, thus avoiding clinically meaningless false
identifications. In particular “MAX” must be ≤ 14.3
m/s^2, “min” must be ≥ 6.5 m/s^2 and “Diff” must
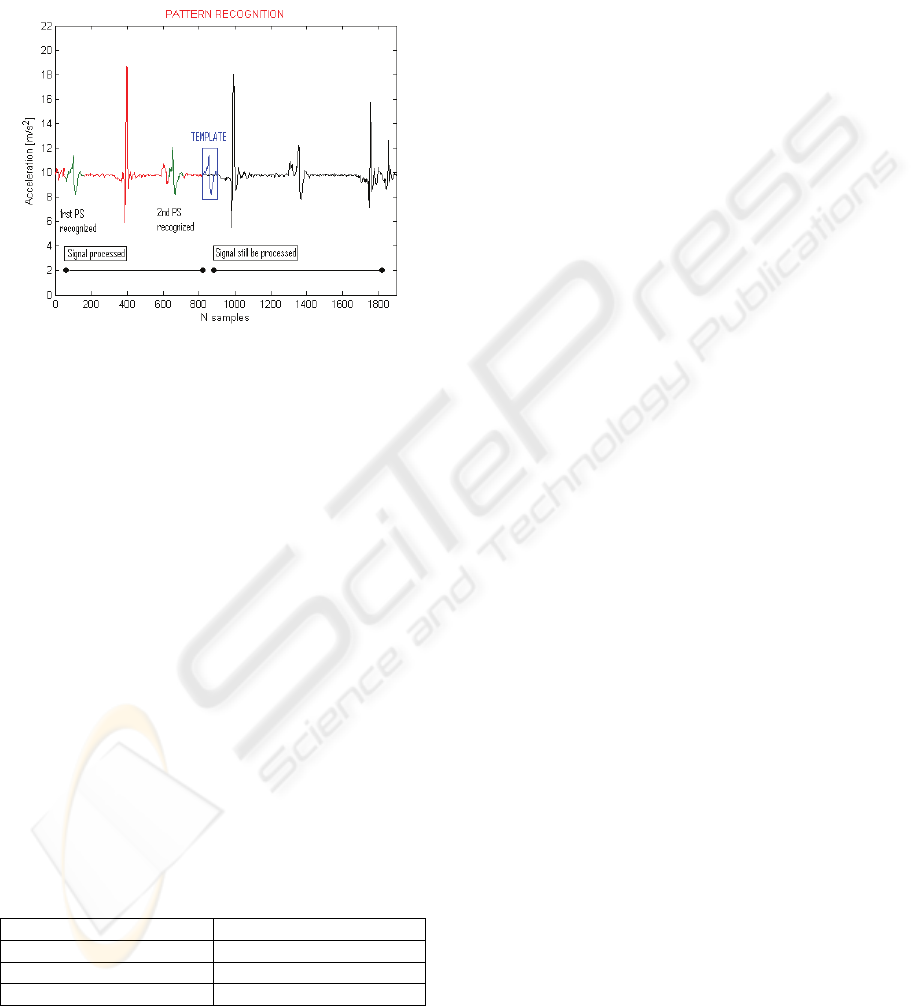
be ≥ 2.2 m/s^2. In figure 2 is reported the template
used for the automatic data processing while flowing
along the signal automatically recognizes the PS
repetitions.
Figure 2: The automatic analysis. In blue, inside the frame,
is represented the window chosen as template which is
flowing along the signal, in green the first end the second
repetition of PS recognized thanks to an high Pearson’s
correlation coefficient associated with the template (R ≥
0.7), while in red is underlined the shear of signal already
processed and in black the signal which is going under
processing.
The automatic method identification performance
was evaluated in terms of percentage sensitivity,
specificity and accuracy, applying the algorithm on
the entire set.
3 RESULTS
Using Pearson’s correlation coefficient, together
with the other mentioned thresholds, provided us a
classification accuracy around 96.7%. The
classification performance measures are presented in
table 1.
Table 1: Classification performance on the test for the
method used for the automatic recognition of the PS test.
% VALUE
Sensitivity
81.9
Specificity
99.3
Accuracy
96.7
For the evaluation of this classification a direct
method was used, i.e. the training set was classified
with a classifier built using the training set data
itself.
4 CONCLUSIONS
The goal of our study was to develop a methodology
able to provide a quantification of the PS test. We
defined therefore a method to easily analyse the
acceleration signal during PS test with the goal to
achieve non-invasive, portable and user-friendly tool
able to provide a quantitative and complete diagnose
of ACL deficient knee. This method used a
predefined template and the computation of
Pearson’s correlation coefficient between this
prototypical pattern and the signal under processing.
In literature there are different methods dedicated to
pattern recognition, even if they are more specific
and require a major computational load.
Being acceleration PS event quite readily
recognizable and identifiable from the remaining
parts of signal, we privileged the easiness of
computation, in order to apply the automatic
recognition also to real-time applications.
A limitation of this study was due to the template
form; its simple and linear waveform is quite easy to
generate also by a mistakenly moved tool. This
conditions could generate false positive (FP) cases.
On the other hand a sudden motion during the test
could falsify the typical trend of the signal,
provoking false negative (FN) cases. Moreover the
coupled loads applied by the surgeon were not
quantitatively controlled and the considered
parameters could be strongly affected.
We are convinced that provide to the surgeons an
accurate description of the movement to perform in
order to realize the pivot-shift test always in the
same way and limit the movements of the tested
limb, usually provoked by the operator to relax the
limb, could improve the performance of the model
regarding false-positive and false-negative.
Further analyses imply to verify the skill, in terms of
sensitivity, specificity and accuracy, of the clinical
method purposed to discern between pathologic and
healthy knee.
ACKNOWLEDGEMENTS
We would like to acknowledge the help of the
anaesthetists and all the staff of the IX Orthopaedic
Division of Istituto Ortopedico Rizzoli, for their
fundamental availability during this study.
BIOSIGNALS 2010 - International Conference on Bio-inspired Systems and Signal Processing
238

In particular we are thankful to Dr. Giovanni
Giordano for his professional support during the
execution of the PS-tests and the whole study.
REFERENCES
Kocher, M.S., Steadman, J.R., Briggs, K., Sterett, W.I. &
Hawkins, R.J., 2009. Relathionships between
objective assessment of ligament stability and
subjective assessment of symptoms and function after
anterior cruciate ligament reconstruction. Arthroscopy
and Sports Medicine, 129, pp.353-358.
Jakob, R.P., Staubli, H.U. & Deland, J.T., 1987. Grading
the pivot shift. Objective tests with implications for
treatment. The Journal of Bone and Joint Surgery,
69(B), pp.294-299.
Lopomo, N., Bignozzi, S., Zaffagnini, S., Giordano, G.,
Irrgang, J.J., Fu, F. & Marcacci, M., 2008.
Quantitative correlation between IKDC score, static
laxity and pivot-shift test: a kinematic analysis of knee
stability in anatomic double-bundle ACL
reconstruction. Operative Techniques in Orthopaedics,
18, pp.185-189.
Kuroda, R., Hoshino, Y., Nagamune, K. & Kubo, S.,
2008. Intraoperative measurement of pivot shift by
electromagnetic sensors. Operative Techniques in
Orthopaedics, 18, pp.190-195.
Musahl, V., Bell, K.M., Tsai, A.G., Costic, R., Allaire, R.,
Zantop, T., Irrgang, J.J. & Fu, F., 2007. Development
of a simple device for measurement of rotational knee
laxity. Knee Surgery, Sport Traumatology, Arthoscpy,
15, pp.1009-1012.
Amis, A.A., Cuomo, P., Rama, R.B.S., Giron, F., Bull,
A.M.G., Thomas, R. & Aglietti, P., 2008.
Measurement of Knee laxity and Pivot-Shift
Kinematics with Magnetic Sensors. Operative
Techniques in Orthopaedics, 18, pp.196-203.
Bleday, R.M., Fanelli, G.C., Giannotti, B.F., Edson, C.J.
& Barrett, T.A., 1998. Instrumented measurement of
the posterolateral corner. The Journal of Arthoscopic
and Related Surgery, 14 (5), pp.489-494.
Diermann, N., Schumacher, T., Schanz, M., Raschke,
M.J., Petersen, W. & Zantop, T., 2009. Rotational
instability of the knee: internal tibial rotation under a
simulated pivot shift test’. Arthroscopy and Sports
Medicine, 129, pp.353-358.
Csintalan, R.P., Ehsa, A., McGarry, M.H., Fithian, D.F. &
Lee TQ., 2006. Biomechanical and anatomical effects
of an external rotational torque applied to the knee.
The American Journal of Sports Medicine, 34,
pp.1623-1629.
Amis, A., Bull, A.M.J., Lie, D.T., 2005. Biomechanics of
rotational instability and anatomic anterior cruciate
ligament reconstruction. Operative Techniques in
Orthopaedics, 15, pp.29-35.
Labbe, D.R., De Guise, J.A., Godbout, V., Fernandes, J. &
Hagemeister, N. Development of an objective
measurement tool for the pivot shift phenomenon of
the knee. 16
th
Congress of the European Society of
Biomechanics, Lucerne, Switzerland, 2008.
Corthout, J., Van Huffel, S., Mendez, M.O.,Bianchi, A.M.,
Penzel, T. & Cerutti, S. Automatic screening of
obstructive sleep apnoea from the ECG based on
empirical mode decomposition and wavelet analysis.
30
th
Annual International IEEE EMBS Conference,
Vancouver, British Columbia, Canada, 20-24 August
2008.
Khandoker, A.H. Karmakar, C.K. & Palaniswami, M.,
2009. Automated recognition of patients with
obstructive sleep apnoea using wavelet-based features
of electrocardiogram recordings. Computer in Biology
and Medicine, 39, pp.88-96.
Colombet, P., Robinson, J., Christel, P., Franceschini, J.P
& Djian, P., 2007. Using navigation to measure
rotation kinematics during ACL reconstruction.
Clinical Orthopaedics and Related Research, 454,
pp.59-65.
Hoshino, Y., Kuroda, R., Nagamune, K., Yagi, M.,
Mizuno, K., Yamaguchi, M., Muratsu, H., Yoshiya, S.,
Kurosaka, M., 2007. In vivo measurement of the
pivot-shift test in the anterior cruciate ligament-
deficient knee using an electromagnetic device. The
American Journal of Sports Medicine, 35, pp.1098-
1104.
AUTOMATIC SCREENING OF ACCELERATION SIGNAL DURING PIVOT-SHIFT TEST BASED ON PEARSON'S
CORRELATION COEFFICIENT
239
