REPRESENT
ATION AND EFFICIENT MANAGEMENT
OF MULTI-VERSION CLINICAL GUIDELINES
Fabio Grandi
Dip. di Elettronica, Informatica e Sistemistica, Alma Mater Studiorum, Universit
`
a di Bologna
Viale Risorgimento 2, I-40136, Bologna, Italy
Keywords:
Clinical guidelines, Document retrieval, Temporal database, Ontologies, Personalization, Versioning, XML.
Abstract:
While the world wide web user is suffering from the disease caused by information overload, for which
personalization is one of the treatments which works, a physician accessing web-based clinical guideline
repositories is not immune from contagion. This seems a good reason to prescribe a personalization treatment
also to the professional user of a computerized clinical guideline library. To this end, we apply to clinical
guidelines solutions we previously developed for norm texts in the legal domain, and show how multi-version
representation capabilities and personalization query facilities can be added to their management.
1 INTRODUCTION
Clinical guidelines are definitions of “best practices”
encoding and standardizing clinical procedures for a
given disease. The advantages of adopting computer-
based guidelines as a support for improving the
work of physicians and optimizing hospital activi-
ties have been acknowledged by many authors and
several computer systems have been developed (see
e.g. (Fridsma, 2001; Gordon and Christensen, 1995)).
Clinical guidelines are subject to continuous develop-
ment and revision by committees of expert physicians
and health authorities and, thus, multiple versions co-
exist as a consequence of the clinical and healthcare
activity.
In this paper, we propose to apply to the manage-
ment of clinical guidelines some techniques we pre-
viously developed for norm documents in the legal
domain (Grandi et al., 2005; Grandi et al., 2009b),
which present strong similarities. Hence, we will in-
troduce solutions to model and to provide personal-
ized access to multi-version clinical guidelines, which
can be stored both in textual and in executable for-
mat in an XML repository. The XML language has
already been proposed by many authors and adopted
in several research projects (e.g. (Dubey and Chueh,
2000; Shiffman et al., 2000; Buchtela et al., 2008)) as
a suitable means to encode clinical guidelines. Hence,
our approach can be considered as a compatible ex-
tension of such proposals, to which we aim at adding
multi-version representation capabilities and person-
alization query facilities.
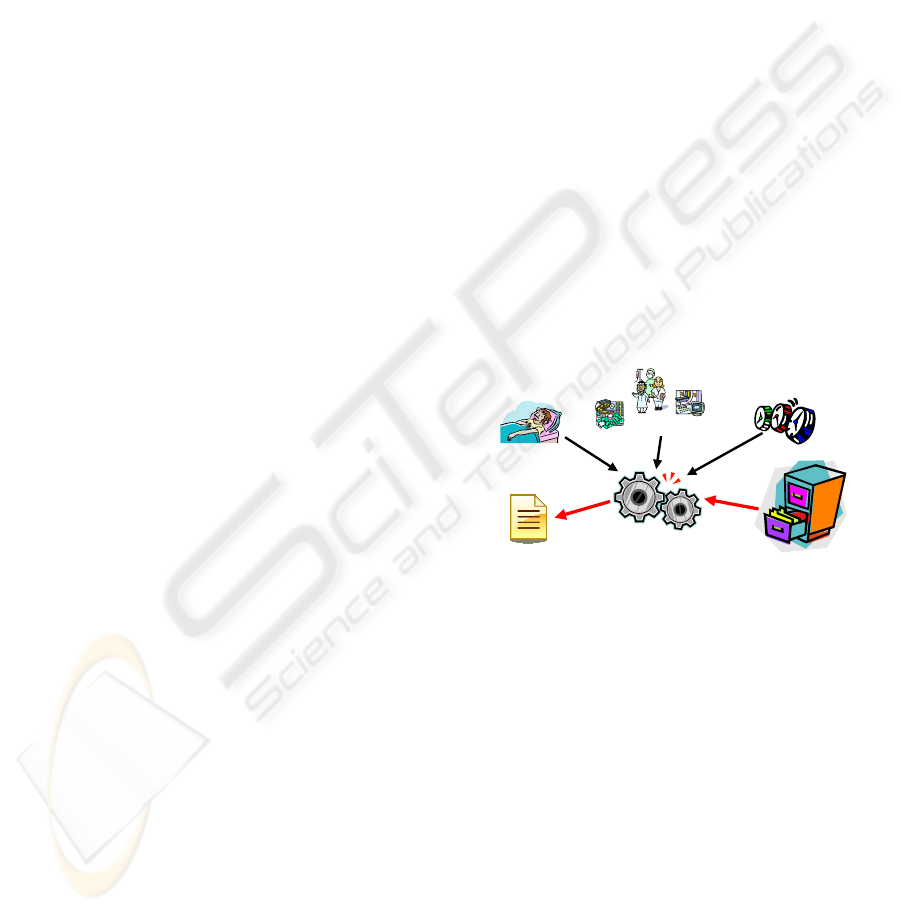
PATIENT PROFILE
CONTEXT INFO
TEMPORAL PERSPECTIVE
MULTI-VERSION
GUIDELINE REPOSITORY
PERSONALIZATION ENGINE
PERSONALIZED
GUIDELINE VERSION
Figure
1: Personalized access to multi-version guidelines.
To this end, we will describe how a multi-version
XML data model and the prototype system we devel-
oped for e-Government applications can be applied to
the representation and management of multi-version
clinical guidelines. In this way, multiple temporal
perspectives, patient profile and context information
can be used by an automated personalization service
to build a guideline version tailored to a specific use
case (see Fig. 1).
The paper is organized as follows. In Section 2,
temporal and semantic versioning of clinical guide-
lines is introduced with reference to advanced appli-
cation requirements. Section 3 is devoted to the de-
scription of a multidimensional XML data model sup-
porting temporal and semantic versioning of guide-
lines. In Section 4, a prototype system efficiently
implementing the personalization engine sketched in
54
Grandi F. (2010).
REPRESENTATION AND EFFICIENT MANAGEMENT OF MULTI-VERSION CLINICAL GUIDELINES.
In Proceedings of the Third International Conference on Health Informatics, pages 54-61
DOI: 10.5220/0002727400540061
Copyright
c
SciTePress

Fig. 1 is briefly described. Conclusions will finally be
found in Section 5.
2 MULTI-VERSION GUIDELINES
The fast evolution of medical knowledge and the dy-
namics involved in clinical practice imply the coex-
istence of multiple temporal versions of the clini-
cal guideline documents stored in a repository, since
guidelines are continually subject to amendments and
modifications. In fact, it is crucial to reconstruct, bor-
rowing the term from the legal field, the consolidated
version of a guideline as produced by the application
of all the modifications it underwent so far, that is the
form in which it currently belongs to the state-of-the-
art of clinical practice and, thus, must be applied to
patients today. However, also past versions are still
important, not only for historical reasons: for exam-
ple, a physician might be called upon to justify his/her
actions for a given patient P at a time T on the basis
of the clinical guideline versions which were valid at
time T and applicable to the pathology of patient P. In
other words, temporal concerns are important in the
medical domain as they are in the legal domain and,
thus, a guideline management system should be able
to retrieve or reconstruct on demand any temporal ver-
sion of a given clinical guideline to meet advanced
application requirements.
Moreover, another kind of versioning, which we
will call semantic versioning, plays a fundamental
role, because clinical guidelines or some of their parts
have limited applicability with respect, for instance,
to the population of patients. In fact, a given guide-
line (e.g. involving treatment of heart diseases) may
contain different recommendations which are not uni-
formly applicable to the same classes of patients: one
general therapy may be non applicable to persons who
suffer from some metabolic disorders (e.g. diabetes
mellitus) or chronic diseases (e.g. kidney failure)
or present some addiction (e.g. cocaine); one first-
choice drug may not be given to patients who are al-
ready under treatment with possibly interacting drugs
(e.g. anticoagulants), or show genetic or acquired hy-
persensitivity or intolerance to some substances (e.g.
patients with enzymatic defects or documented aller-
gies), and so on. Hence, when dealing with a specific
patient case, a physician may be interested in find-
ing a personalized version of a clinical guideline, that
is a version tailored to the patient’s health state and
anamnesis, only containing recommendations which
are safely and effectively applicable to his/her per-
sonal case.
In addition to linking guidelines to classes of pa-
tients, semantic versioning can also involve more
generic applicability contexts (e.g. hospitals without
PET diagnostic equipment, or selected centers taking
part to a clinical trial), which might require the appli-
cation of a particular version of the general guideline,
which may also no longer be part of the consolidated
state-of-the-art guideline. For instance, consider ver-
sion v1 of a clinical guideline G which prescribes a
biopsy to confirm a cancer diagnosis but has been su-
perseded by a new version v2 which introduces a PET
scan for the same cancer diagnosis, making in most
cases the biopsy unnecessary. However, in some hos-
pital H which is not equipped with a PET scanner, the
right version of G to be followed is v1, although no
longer considered valid by the medical community.
Therefore, the applicable version of the guideline for
context H is G(v1), with biopsy as a mandatory diag-
nostic means. This example also shows how temporal
and limited applicability aspects may also interplay in
the production and management of versions.
2.1 Temporal Versioning
As far as temporal versioning is concerned, several
independent time dimensions are involved in the rep-
resentation and management of clinical guidelines, in
particular when we consider an environment also sup-
porting the guideline authoring and approval process.
Relevant time dimensions include valid, event, avail-
ability, proposal and acceptance times (Combi and
Montanari, 2001; Terenziani et al., 2005). Even con-
sidering an environment where only approved guide-
lines are stored, and retrieved by final users to be con-
sulted or followed, at least two time dimensions are
relevant:
Validity Time. It is the time the guideline is con-
sidered in force by the medical community and, thus,
is applied to patients. It has the same semantics of
valid time as in temporal databases (Jensen and et al.,
1998), since it represents the time the guideline actu-
ally belongs to the state-of-the-art of clinical practice.
Efficacy Time. Borrowing the term from the legal
domain, it is the time the guideline can be applied to a
concrete case. It usually corresponds to validity, but it
might be the case that an obsolete, superseded guide-
line continues to be applicable to a limited number of
cases. While such cases exist, the guideline continues
its efficacy though no longer considered in force.
Notice that validity and efficacy time both have
the semantics of valid time but represent different and
independent valid time notions. Both are necessary
to correctly deal with cases as the one in the last de-
REPRESENTATION AND EFFICIENT MANAGEMENT OF MULTI-VERSION CLINICAL GUIDELINES
55
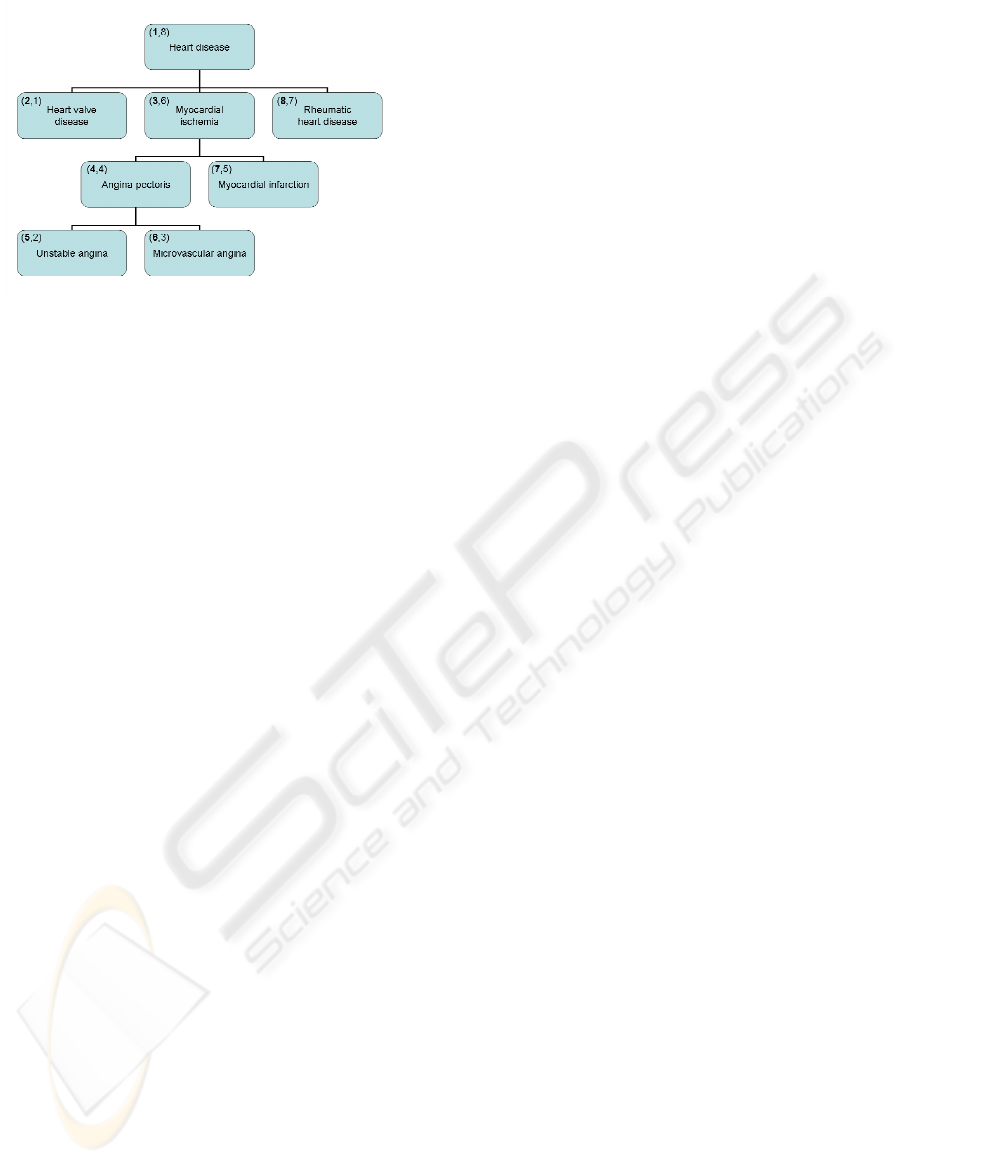
Figure 2: A sample ontology, where each class has a name
and is associated to a (pre-order,post-order) pair.
scribed example: the guideline version G(v1) for the
applicability context H can still be selected today as
its efficacy includes current time, although its validity
does not. Furthermore, in addition to the time dimen-
sions which model the dynamics of guidelines in the
real world, transaction time (Jensen and et al., 1998)
plays an important role when automatic management
of information through computer systems is involved
and, thus, should never be neglected, since it allows to
execute retro- or pro-active modifications and to keep
track of their execution for audit purposes. For ex-
ample, it might be the case that a physician makes a
wrong decision in choosing a drug following the pro-
visions of a guideline retrieved from the system when
the returned consolidated version is actually out-of-
date; the decision is taken while a modified version
of the guideline (e.g. involving the adoption of some
more effective and less potentially dangerous drug) is
already available but has not been stored in the infor-
mation system yet. Hence, transaction time is needed
to ascertain a posteriori that the correct version was
stored retroactively and, thus, the physician acted in
good faith.
Temporal versioning along multiple time dimen-
sions can be added to documents in an XML reposi-
tory by making temporal the XML encoding (Dyreson
and Grandi, 2009), that is introducing timestamps as
annotations in the XML document.
2.2 Semantic Versioning
Semantic applicability of multi-version resources can
be defined with reference to domain ontologies.
Ontologies (Guarino, 1998; Gruber, 2009), which
are conceptualizations of a domain into a machine-
understandable format, have recently become quite
popular with the advent of the semantic web (Berners-
Lee et al., 2001), where the introduction of common
reference ontologies is necessary to allow information
and its interpretation to be shared by both human and
automatic agents.
Appropriate applicability of clinical guidelines to
individual patients can be defined according to a con-
sensual taxonomy of diseases, like the ICD-10 en-
dorsed by the World Health Organization (ICD-10,
2009) or the MeSH Section C maintained by the US
National Library of Medicine (MeSH-C, 2009). For
instance, consider Fig. 2, which depicts a small por-
tion of a medical ontology representing a classifica-
tion of principal heart diseases. Notice that, at this
stage of the research, we deal with “tree-like” ontolo-
gies defined as class taxonomies induced by the IS-
A relationship. This will allows us to exploit during
query processing the pre-order and post-order prop-
erties of trees in order to enumerate the nodes and
check ancestor-descendant relationships between the
classes; such codes are displayed in the upper left cor-
ner of the ontology classes in the Figure, in the form:
(pre-order,post-order). For instance, the class “My-
ocardial ischemia” has pre-order “3” which is also its
identifier, whereas its post-order is “6”. Before the
personalization engine can be used to build a guide-
line version tailored to a specific patient, the patient
must be classified with respect to the disease ontol-
ogy, on the basis of medical records by means of
a suitable reasoning service (Grandi et al., 2009b),
or through a profile explicitly supplied by the physi-
cian. Moreover, additional semantic versioning coor-
dinates, referencing specific domain ontologies, can
also be considered to model context-dependent appli-
cability of guidelines.
Hence, in XML resource repositories, reference
to ontology concepts (e.g. using class identifiers like
those in Fig. 2) can be added to the resource represen-
tation and storage as a new versioning coordinate. In
this way, applicability annotations can be embedded
in the guideline documents to be used by automatic
personalization tools. Obviously, also the annotation
of clinical guidelines which defines their semantic
versioning must be effected by medical domain ex-
perts, as part of the guideline drafting and approval
process itself. Whenever an ontology definition is
changed, temporal versions of the ontology also must
be maintained, as the temporal perspectives for nav-
igating the ontology and for searching the guideline
repository must be same for consistency reasons. The
ontology temporal versioning techniques introduced
in (Grandi and Scalas, 2009) can be used to this pur-
pose.
One of the global effects of versioning is an in-
crease in the number or size of the documents to
be stored, also depending on the fact that different
versions of the same document are stored as sepa-
rate XML files or are arranged into a single multi-
HEALTHINF 2010 - International Conference on Health Informatics
56

version XML file, owing to a uniform encoding of
variant parts within the document structure. The lat-
ter solution, which is our choice, is often unavoid-
able in order to keep the growth of the storage space
under control, especially when different versions of
the same document may differ by a few nodes only.
Personalization, which has shown to be a powerful
tool to cope with information overload on the inter-
net (Riecken, 2000), can also be particularly effective
when used in the management of large XML reposito-
ries of versioned documents (Grandi et al., 2009b). In
this case, the adoption of personalization techniques
can prevent in most cases users to have to go through
a huge amount of irrelevant information to find out
the right version(s) of the one of interest and, thus,
might help to make their search faster and more accu-
rate. Hence, personalization based on semantic ver-
sioning may improve the quality of the interaction
with the user by further focusing the search on re-
ally relevant versions only, which is a desirable fea-
ture for clinical guideline management. For example,
one of the acknowledged most relevant obstacles in
the use and dissemination of guidelines (Cabana et al.,
1999) is the need for adapting them to constraints
in local settings (e.g. concerning available hospital
resources and practitioners’ skills). Management of
multi-version guidelines with context-based semantic
personalization might help to overcome this problem
(Fridsma et al., 1996; Terenziani et al., 2004). Other
use cases requiring a sort of location-based semantic
personalization can also be found: for instance, con-
sider a guideline involving the recommendation of a
new drug non yet registered in a given country, or in-
troducing a new protocol only available in selected
medical centers participating to an experimental pro-
gram: the actual contents of the guideline should be
changed according to the place where the guideline is
retrieved or executed.
3 AN XML DATA MODEL FOR
MULTI-VERSION GUIDELINES
In this Section, we introduce a multi-version XML
document model supporting multiple temporal and
semantic versioning coordinates. In doing this, we do
not refer to a specific document structure (e.g. defined
via a DTD or XML Schema), but we rather introduce
a versioning annotation scheme which can be applied
to any generic XML resource. In particular, it can
be easily adapted to available proposals for the XML
encoding of clinical guidelines, including those de-
scribed in (Dubey and Chueh, 2000; Shiffman et al.,
2000; Buchtela et al., 2008).
RECOMMENDATIONS
1. IDENTIFICATION OF PATIENTS
WITH RISK OF UNSTABLE ANGINA
...
2. INITIAL EVALUATION AND MANAGEMENT
...
3. EARLY HOSPITAL CARE
3.1. Initial Treatment Strategy
...
3.2. Drug Therapy
3.2(v1). Anti-Ischemic and Analgesic Therapy
3.2(v1).1. Therapy with nitrates
...
3.2(v1).2. Therapy with beta-blockers
3.2(v1).2(v1). ...administration of drug D1...
3.2(v1).2(v2). ...administration of drug D2...
3.2(v1).2(v3). ...administration of drug D3...
...
3.2(v1).3. Therapy with ACE inhibitors
...
3.2(v2). Antiplatelet/Anticoagulant Therapy
...
4. CORONARY REVASCULARIZATION
...
5. LATE HOSPITAL CARE
...
Figure 3: The structure of a fragment of a sample multi-
version clinical guideline.
We start by formally defining as version a piece
of text within a guideline document, with a common
temporal and semantic pertinence. Owing to the def-
inition, a version can be assigned a timestamp and an
applicability annotation to uniquely define its tempo-
ral and semantic pertinence. Obviously, different ver-
sions of the same object must differ in their temporal
and/or semantic pertinence.
For the sake of simplicity, but without loss of gen-
erality, we only consider in the examples which fol-
low one time dimension (i.e. validity) and one se-
mantic dimension (i.e. reference to classes in an on-
tology of diseases like the one in Fig. 2). Let us con-
sider as running example the clinical guideline frag-
ment in Fig. 3, involving recommendations for the
treatment of unstable angina patients. The figure dis-
plays the text organization, which has a three-level
section structure, where section 3.2. has two differ-
ent versions, namely 3.2(v1) and 3.2(v2), whereas
section 3.2(v1).2 has three different versions, namely
3.2(v1).2(v1), 3.2(v1).2(v2) and 3.2(v1).2(v3). The
multi-version XML encoding of such guideline frag-
ment is shown in Fig. 4.
In the XML encoding, we use the
<version>
ele-
ment to delimit the boundaries of a version within the
document. The
<valid>
and
<applies>
elements
REPRESENTATION AND EFFICIENT MANAGEMENT OF MULTI-VERSION CLINICAL GUIDELINES
57

...
<recommendations>
<version number="1">
<applies to="C3"/>
<valid from="1980-01-01" to="9999-99-99"/>
...
<section number="3">
<version number="1">
<applies to="C4"/>
<title>Early Hospital Care</title>
...
<section number="2">
<title>Drug Therapy</title>
<version number="1">
<applies to="C5"/>
<title>Anti-ischemic and Analgesic Therapy</title>
...
<section number="2">
<title>Therapy with beta-blockers</title>
<version number="1">
<valid from="1980-01-01" to="1990-12-31"/>
...
administration of drug D1
...
</version>
<version number="2">
<valid from="1991-01-01" to="1998-12-31"/>
<valid from="2001-01-01" to="2003-12-31"/>
...
administration of drug D2
...
</version>
<version number="3">
<valid from="1985-01-01" to="9999-99-99"/>
...
administration of drug D3
...
</version>
...
</section>
...
</version>
<version number="2">
<applies also="C7"/>
<title>Antiplatelet/Anticoagulant Therapy</title>
...
</version>
...
</section>
...
</version>
...
</section>
...
</version>
</recommendations>
...
Figure 4: An XML fragment showing the multi-version en-
coding of the guideline in Fig. 3.
are then used to assign the temporal and semantic per-
tinence, respectively, to the version which contains
them. Validity and applicability properties are inher-
ited by descendant nodes in the XML tree-structure
unless locally redefined with a new version definition.
Therefore, there is no reason to repeat the valid or ap-
plies annotation when the pertinence is not changed
from the ancestor version in the XML tree-structure.
In general, redefinition may involve only a subset of
the versioning dimensions, while the others dimen-
sions are inherited.
With reference also to Fig. 3, the XML frag-
ment in Fig. 4 shows, within the outermost
<recommendations>
element, a hierarchical struc-
ture based on three levels of sections. The
<recommendations>
element is composed of one
version, which defines its global semantic and tempo-
ral pertinence, that is applicable to class C3 in the on-
tology in Fig. 2 (patients with myocardial ischemia)
and valid from 1980 on. It is made of several first-
level sections (see also Fig. 3), of which only section
3 is evidenced in the Figure. Such a section, made of
only one version to specify applicability to ontology
class C4 (patients with angina pectoris), deals with
Early Hospital Care. Its temporal pertinence is inher-
ited from the container element.
In general, by means of redefinitions we can in-
troduce, for each part of a document, complex valid-
ity and applicability properties including extensions
or restrictions with respect to ancestors. For instance,
the applicability assignment to section 3 which we
just described is a restriction and the attribute
to
is
used to this end. Actually, the applicability assigned
to the version is the intersection of the
to
value and
of the value inherited by the ancestor version (in this
case C4∩C3, which equals C4 since it is a subclass
of C3). The same applies to second-level section 3.2
(entitled “Drug Therapy”), whose first version (enti-
tled “Anti-ischemic and Analgesic Therapy”) applies
to class C5 (unstable angina), which is also a re-
striction, whereas the second version (entitled “An-
tiplatelet/Anticoagulant Therapy”) is also applicable
to class C7 (myocardial infarction), which is an exten-
sion indeed. Attribute
also
is used in this case, and
the applicability assigned to the version is the union
of the
also
value and of the value inherited by the
ancestor version (class C4∪C7). In other words, the
contents of section 3.2(v2) both apply to angina pec-
toris and myocardial infarction patients.
The third-level section 3.2(v1).2 entitled “Ther-
apy with Beta-blockers” is made of several versions,
each one dealing with the administration of a specific
drug and having its own temporal pertinence, whereas
the (inherited) applicability is the same (namely C5,
unstable angina). In order to derive the validities of
the three drugs shown in the Figure, we assume the
recommendations underwent the evolution which fol-
lows. Drug D1 was introduced in 1980 and then re-
placed by the drug D2 in 1991. However, the use of
drug D2 was suspended from 1999 to 2000, period
during which it had been under investigation since
suspected of causing adverse reactions. In 2004, due
to evidence of long-term adverse effects, D2 was def-
initely withdrawn. Drug D3 has been introduced in
1985. Hence, the resulting history of recommended
beta-blockers according to the guideline in Fig. 3
(which will in fact correspond to the answers to a
sequence of snapshot queries issued on the multi-
version document) is the following:
− from 1980 to 1984: drug D1
− from 1985 to 1990: drugs D1 and D3
− from 1991 to 1998: drugs D2 and D3
− from 1999 to 2000: drug D3
HEALTHINF 2010 - International Conference on Health Informatics
58

− from 2001 to 2003: drugs D2 and D3
− from 2004 on: drug D3
As for 3.2(v1).2(v2) in the Figure, versions can be as-
signed multiple intervals as validity: this corresponds
to adopt temporal elements (Gadia, 1988; Jensen and
et al., 1998), that is disjoint union of intervals, as
timestamps.
3.1 Operations
The multi-version XML data model can be equipped
with two basic operators for the management of
guideline authoring and maintenance: one devoted to
change the textual content of a guideline portion and
the other to allow modifications to the temporal and
semantic pertinence of a given version. The former
can be used for deletion of (a part of) the guideline
(abrogation), or the introduction of a new part of the
guideline (integration), or the replacement of (a part
of) the guideline (substitution). The latter can be used
to deal with the time/applicability extension or restric-
tion of (part of) the guideline. Such operators, in order
to preserve the well-formedness of the version struc-
ture and the inheritance semantics, can be defined in
a similar way as the ones defined for multi-temporal
norm documents in (Grandi et al., 2005).
Clinical guideline repositories, like the US Na-
tional Guideline Clearinghouse (NGC, 2009) or the
UK National Library of Guidelines (NLG, 2009), are
usually managed by traditional information retrieval
systems where users are allowed to access their con-
tents by means of keyword-based queries expressing
the subjects they are interested in. Adopting a system
like the one described in (Grandi et al., 2009b) that we
developed for norm documents, users are offered the
possibility of expressing temporal and semantic spec-
ifications for the reconstruction of a consistent version
of the retrieved guideline.
In particular, the queries can contain four types
of constraints: temporal, structural, textual and appli-
cability. Such constraints are completely orthogonal
and allow the users to perform very accurate searches
in the XML guideline repository. Let us focus first on
the applicability constraint. Consider again the ontol-
ogy in Fig. 2 and guideline fragment in Fig. 4: for
the treatment of John Smith, an “infarctuated” patient
(i.e. belonging to class C7), the sample recommenda-
tions in Fig. 3 will be selected as pertinent, but only
the second version of Section 3.2 will be actually pre-
sented as applicable. Furthermore, the applicability
constraint can be combined with the other three ones
in order to fully support a multi-dimensional retrieval.
For instance, a physician (or an health insurance offi-
cer) could be interested in all the guidelines ...
• ... which have a section whose title (structural
constraint) contains the word anticoagulant (tex-
tual constraint), ...
• ... which were valid between 2007 and 2008 (tem-
poral constraint), ...
• ... and which are applicable to a patient suffering
from unstable angina (applicability constraint).
More precisely, the system is able to answer
queries having the XQuery syntax in Fig. 5, where
textConstr
,
tempConstr
, and
applConstr
are suit-
able functions allowing the specification of the tex-
tual, temporal and applicability constraints, respec-
tively (the structural constraint is implicit in the XPath
expressions used in the XQuery statement).
4 IMPLEMENTATION
The personalization engine in Fig. 1, which is ca-
pable to execute queries like the one in Fig. 5, has
been implemented as a prototype Multi-version XML
Query Processor. The prototype code is written in
Java JDK 1.5 and employs ad-hoc data structures (re-
lying on embedded “light” DBMS libraries) and algo-
rithms which allow users to reconstruct on-the-fly the
desired personalized version of the XML guideline,
by means of a multi-version extension of the holistic
twig join approach (Bruno et al., 2001). Guidelines
are stored in the XML repository using an indexing
scheme based on multi-version inverted indices, that
is an extension with timestamps and semantic anno-
tations of the indexing solution proposed in (Zhang
et al., 2001). In practice, the query processing al-
gorithm implements the temporal slice operator pro-
posed in (Mandreoli et al., 2006), to which the pro-
cessing of semantic constraints has been added, with-
out an appreciable overhead. In fact, thanks to the
properties of the adopted pre- and post-order encod-
ing of the ontology classes, applicability constraints
can be very efficiently tested during query processing
by means of simple comparisons. A detailed presen-
tation of the deployed data structures and holistic join
techniques, together with a related work discussion on
these topics, can be found in (Grandi et al., 2009a).
As a result, we obtain a high overall query pro-
cessing efficiency mated with low memory require-
ments. In order to evaluate the performance of the
prototype, a specific query benchmark was built and
several exploratory experiments were conducted to
test the personalization engine behavior under dif-
ferent workloads. The experiments have been ef-
fected on a Pentium 4 3Ghz Windows XP Profes-
sional workstation, equipped with 1GB RAM and a
REPRESENTATION AND EFFICIENT MANAGEMENT OF MULTI-VERSION CLINICAL GUIDELINES
59

FOR $a IN guidelines.xml
WHERE textConstr ($a//section/title/text(), ’anticoagulant’)
AND tempConstr (’vTime OVERLAPS PERIOD(’2007-01-01’,’2008-12-31’)’)
AND applConstr (’C5’)
RETURN $a
Figure 5: An XQuery-equivalent query executable on a clinical guideline personalization system.
160GB EIDE disk with NT file system (NTFS). Test
were performed on three XML document collections
of increasing size (namely 5,000, 10,000 and 20,000
guidelines, with a total size of 120MB, 240MB and
480MB, respectively). In all collections the guide-
lines were synthetically generated by means of a suit-
able tool, which is able to produce XML documents
compliant to our multi-version model under different
parameter configurations. For each collection, the av-
erage, minimum and maximum document size was
24KB, 2KB and 125KB, respectively. Experiments
were conducted by submitting queries of five differ-
ent types, mixing in various ways structural, textual,
temporal and applicability constraints.
The system behavior showed a good efficiency in
every context, providing a response time (including
query analysis, retrieval of the qualifying guideline
parts and reconstruction of the result) of a few sec-
onds for most of the queries. Moreover, the selec-
tivity of the query predicates does not impair per-
formances, even when large amounts of documents
containing some (typically small) relevant portions
have to be retrieved. The system is able to deliver
a fast and reliable performance in all cases, since it
practically avoids the retrieval of useless document
parts. For the same reasons, the main memory re-
quirements of the Multi-version XML Query Proces-
sor are quite limited, less than 5% with respect to an
approach like the one adopted in (Grandi et al., 2005),
where complete documents are retrieved with a tra-
ditional XML engine working on structural and tex-
tual constraints, and then temporal and applicability
constraints are applied using a DOM representation
to prune out non-qualifying XML nodes. Notice that
this property is very interesting for a system which is
likely to run in a highly concurrent multi-user envi-
ronment, since memory requirements are not crucial
for performance. The prototype system also showed
a good scalability behavior in every type of query set-
ting, as the computing time for the same query al-
ways grows linearly with the number of documents.
Full details on performance evaluation can be found
in (Grandi et al., 2009a; Grandi et al., 2009b).
5 CONCLUSIONS
In this paper, we applied to the representation and
management of clinical guidelines some techniques
we previously developed for norm documents in the
legal domain (Grandi et al., 2009a; Grandi et al.,
2009b). In particular, we introduced solutions to
model and to provide personalized access to multi-
version guidelines, supporting multiple temporal and
semantic versioning coordinates. The proposal in-
volves the definition of a multi-version XML data
model and the implementation of a prototype person-
alization engine.
Preliminary experimental work on query perfor-
mance, with repositories of syntectic XML docu-
ments, showed encouraging results. In particular, the
personalization engine proved to be very efficient in a
large set of experimental situations and showed excel-
lent scale-up figures with varying load configurations.
We underline that the very same techniques we
presented for personalized access to multi-version
textual guideline documents can also be applied to the
enactment of workflows implementing multi-version
clinical guidelines, provided that workflows are spec-
ified using an XML-based definition language, like
BPEL (WS-BPEL, 2009) or XPDL (XPDL, 2009),
which can be enriched as well with temporal and se-
mantic annotations in order to define versions (Grandi
et al., 2009b).
Future work will consider the improvement of the
approach to cope with more advanced application re-
quirements (e.g. relaxing of constraint of tree-like
ontologies) and the completion of the technological
infrastructure required to set up the personalization
platform with the design and implementation of aux-
iliary services (e.g. for automatic patient classifica-
tion with respect to the disease ontology). Further
work will also include the assessment of our devel-
oped system in a concrete working environment, with
real users and in the presence of a repository of real
clinical guidelines.
HEALTHINF 2010 - International Conference on Health Informatics
60

REFERENCES
Berners-Lee, T., Hendler, J., and Lassila, O. (2001). The
semantic web. Scientific American, 284(5):34–43.
Bruno, N., Koudas, N., and Srivastava, D. (2001). Holistic
twig joins: Optimal xml pattern matching. In Proc. of
SIGMOD 2001, pages 310–321.
Buchtela, D., Pele
ˇ
ska, J., Vesel
´
y, A., Zv
´
arov
´
a, J., and
Zvolsk
´
y, M. (2008). An xml-based format for guide-
line interchange and execution. In Proc. of MIE 2008,
pages 151–156.
Cabana, M., Rand, C., Powe, C., Wu, A., Wilson, M., Ab-
boud, P., and Rubin, H. (1999). Why don’t physicians
follow clinical practice guidelines? a framework for
improvement. Journal of American Medical Associa-
tion, 282(15):1458–1465.
Combi, C. and Montanari, A. (2001). Data models with
multiple temporal dimensions: Completing the pic-
ture. In Proc. of CAiSE 2001, pages 187–202.
Dubey, A. and Chueh, H. (2000). An xml-based format for
guideline interchange and execution. In Proc. of AMIA
2000, pages 205–209.
Dyreson, C. and Grandi, F. (2009). Temporal xml. In
¨
Ozsu,
M. and Liu, L., editors, Encyclopedia of Database
Systems. Springer-Verlag (in press).
Fridsma, D. (2001). Special issue on workflow management
and clinical guidelines. AIM Journal, 22(1):1–80.
Fridsma, D., Gennari, J., and Musen, M. (1996). Mak-
ing generic guidelines site-specific. In Proc. of AMIA
1996, pages 597–601.
Gadia, S. (1988). A homogeneous relational model and
query languages for temporal databases. ACM Trans.
on Database Systems, 13(3):418–448.
Gordon, C. and Christensen, J. (1995). Health Telematics
for Clinical Guidelines and Protocols. IOS Press.
Grandi, F., Mandreoli, F., and Martoglia, R. (2009a). Is-
sues in personalized access to multi-version xml doc-
uments. In Pardede, E., editor, Open and Novel Issues
in XML Database Applications, pages 199–230. IGI
Global.
Grandi, F., Mandreoli, F., Martoglia, R., Ronchetti, E.,
Scalas, M., and Tiberio, P. (2009b). Ontology-based
personalization of e-government services. In Mourlas,
C. and Germanakos, P., editors, Intelligent User Inter-
faces, pages 167–203. IGI Global.
Grandi, F., Mandreoli, F., and Tiberio, P. (2005). Tem-
poral modelling and management of normative docu-
ments in xml format. Data & Knowledge Engineering,
54(3):327–354.
Grandi, F. and Scalas, M. (2009). The valid ontology: A
simple owl temporal versioning framework. In Proc.
of SEMAPRO 2009, pages 98–102.
Gruber, T. (2009). Ontology. In
¨
Ozsu, M. and Liu, L.,
editors, Encyclopedia of Database Systems. Springer-
Verlag (in press).
Guarino, N., editor (1998). Formal Ontology in Information
Systems. IOS Press.
ICD-10 (2009). International statistical classification of dis-
eases and related health problems. World Health Or-
ganization, http://www.who.int/classifications/icd/en/.
Jensen, C. and et al., C. D. (1998). The Consensus Glos-
sary of Temporal Database Concepts - February 1998
Version. In Etzion, O., Jajodia, S., and Sripada, S., ed-
itors, Temporal Databases — Research and Practice,
pages 367–405. Springer-Verlag.
Mandreoli, F., Martoglia, R., and Ronchetti, E. (2006). Sup-
porting temporal slicing in xml databases. In Proc. of
EDBT 2006, pages 295–312.
MeSH-C (2009). Medical subject headings - section
c: Diseases. US National Library of Medicine,
http://www.nlm.nih.gov/mesh/2009/mesh browser/
MeSHtree.C.html.
NGC (2009). National guideline clearinghouse. US
Agency for Healthcare Research and Quality,
http://www.guideline.gov.
NLG (2009). National library of guidelines. UK Na-
tional Institute for Health and Clinical Excellence,
http://www.library.nhs.uk/GUIDELINESFINDER/.
Riecken, D. (2000). Personalized views of personalization.
Communications of the ACM, 43(8):27–28.
Shiffman, R., Karras, B., Agrawal, A., Chen, R., Marenco,
L., and Nath, S. (2000). Gem a proposal for a more
comprehensive guideline document model using xml.
Journal of AMIA, 7(5):488–497.
Terenziani, P., Montani, S., Bottrighi, A., Molino, G., and
Torchio, M. (2005). Clinical guidelines adaptation:
Managing authoring and versioning issues. In Proc.
of AIME 2005, pages 151–155.
Terenziani, P., Montani, S., Bottrighi, A., Torchio, M.,
Molino, G., and Correndo, G. (2004). A context-
adaptable approach to clinical guidelines. In Proc. of
MEDINFO 2004, pages 169–173.
WS-BPEL (2009). The web services business pro-
cess execution language. WfMC Coalition,
http://www.wfmc.org/standards/docs.htm.
XPDL (2009). The xml process definition lan-
guage. OASIS Organization, http://www.oasis-
open.org/committees/tc home.php?wg abbrev=wsbpel.
Zhang, C., Naughton, J., DeWitt, D., Luo, Q., and Lohman,
G. (2001). On supporting containment queries in re-
lational database management systems. In Proc. of
SIGMOD 2001, pages 425–426.
REPRESENTATION AND EFFICIENT MANAGEMENT OF MULTI-VERSION CLINICAL GUIDELINES
61
