
AGENT-BASED SIMULATION TO SUPPORT DECISION MAKING
IN HEALTHCARE MANAGEMENT PLANNING
∗
Hayden Stainsby
1
, Manel Taboada
2
and Emilio Luque
1
1
Computer Architecture and Operating Systems Department (CAOS),University Autonoma of Barcelona, Spain
2
“Tom`as Cerd`a” Computer Science School, University Autonoma of Barcelona, Spain
Keywords:
Healthcare operational management, Agent-based modelling, Individual oriented simulation, Emergency de-
partment, Decision support systems.
Abstract:
Simulation has proved to be a useful tool in healthcare operational management, although up until now does
not appear to have reached its full potential within this area. An area in which simulation is increasingly
useful is as in aiding decision making of healthcare managers when planning constructing new Emergency
Departments or making changes to existing ones. A simulation based on Agent Based Modelling techniques
is proposed with an aim to produce a Decision Support System that takes into account the human and social
factors present within such departments and that can also be generalised to be used in multiple hospitals. Work
on the creation of this model has already began, with many of its concepts and structures presented.
1 INTRODUCTION
Throughout numerous years and a multitude of pub-
lished work, simulation has been shown to be a very
useful tool in healthcare operational management.
Why is it then that it has seemingly failed to rise to
the same level of importance as in other equally large
fields such as supply chain management and the man-
ufacturing industry. While many papers have been
published on the topic, few have given detailed re-
ports on the completed implementation of the simula-
tion discussed(Fone et al., 2003).
A number of theories have been presented as to
the reason for the current state of simulation in health-
care operational management. Many of these reasons
are social or educational barriers rather than tech-
nical issues, some healthcare modellers have gone
so far as to say that constructing the model may be
the easiest part of implementing simulation in health-
care(Lowery, 1996).
One of the reasons simulation may have failed
to gain a strong foothold in this area is the apparent
dehumanising factor of simulation. Healthcare man-
agers are also trained doctors, and the idea of reduc-
ing patients to numbers in a pool or tokens in a queue
goes strongly against their training.
∗
Supported by the MEC-Spain under contract TIN2007-
64974.
Another reason is the so-called “not invented
here” syndrome(Brailsford, 2007). The vast major-
ity of models described in the literature are created in
conjunction with staff from the relevant department of
a hospital, a practice that is advocated by most if not
all healthcare modellers. However this can leave the
model with a history that may give other institutions
the impression that they’re using a rehashed, second
hand model. This can restrict the spread of what may
be a valid generalised model further than the institu-
tions for which is was originally created.
When it is considered that in many countries
healthcare is nationalised and ultimately all hospitals
are part of a single system under a single strategic
leadership, it would appear unlikely that every one of
these institutions is so different as to require its own
individual model. To be certain, every institution has
its differences, but these differences should be able to
be described as differences in parameters and using
a simulation as a component of a Decision Support
System (DSS) in a new hospital should be a case of
tuning it for its new environment rather than begin-
ning the system analysis from scratch.
Emergency Departments, just like the hospitals
they are within, are under increasing pressure to han-
dle additional patients with the same or a reduced
level of staffing. At the same time both technolog-
ical and organisational changes are being proposed
436
Stainsby H., Taboada M. and Luque E. (2010).
AGENT-BASED SIMULATION TO SUPPORT DECISION MAKING IN HEALTHCARE MANAGEMENT PLANNING.
In Proceedings of the Third International Conference on Health Informatics, pages 436-441
DOI: 10.5220/0002739304360441
Copyright
c
SciTePress

to improve the efficiency of these departments, but
implementing these changes can be both costly and
dangerous if their full effects are not completely un-
derstood. One recent study of the impact of techno-
logical changes on the running of an emergency de-
partment(Ayatollahi et al., 2009) showed that while
the effects had been mostly positive, the introduc-
tion of computerised systems into the department had
also caused additional problems, specifically in the
learning phases and when the computer system ex-
perienced downtime.
This example highlights the need for modelling
and simulation to try and measure the impact of these
kinds of work flow changes in a specific department
before they are implemented, not just technological
changes but changes to staffing levels, patient num-
bers and arrival distribution, or operational proce-
dures would all be cases where a DSS could be used
to assist in planning for such occurrences. The type
of Decision Support System that can be provided by
computer simulation, and more specifically by Agent-
Based Simulation, is perfectly suited to balancing the
advantages and disadvantages of proposed changes,
giving healthcare managers a better position from
which to make these important decisions.
2 PRIOR WORK
As mentioned in section 1 there are a number of
examples of the use of simulation in healthcare op-
erational management in the literature. Within this
area the types of models the simulations are based on
can be split into two categories; department focussed
models and hospital or region wide models.
The department focussed models most often use
a technique called Discrete Event Simulation (DES),
which involves simulating only the important events
with a system. This is often characterised by a series
of tokens that wait in turn for a server which process
them before they continue on to the next part of the
system.This method can be particularly well suited to
predicting average waiting times of patients in emer-
gency department settings(Connelly and Bair, 2004).
The hospital or region wide models are more gen-
eralised simulations that focus on the system as a
whole. A popular simulation technique whose use
in healthcare operational management began more re-
cently than DES is System Dynamics (SD), which is
often used to simulate these larger systems. An SD
simulation does not model individuals, but rather the
quantity of patients or resources in pools which repre-
sent combined waiting rooms, hospital beds, or some
other place of rest for that entity. SD simulations can
illustrate how changes in one department can have
negative effects on other, apparently unrelated depart-
ments(Taylor and Dangerfield, 2005).
Another increasingly popular modelling tech-
nique is Agent-Based Modelling (ABM). This tech-
nique is used in biological simulations at both the
macro level - for example the movement of a fish
school(Gonz´alez et al., 2009) - and the micro level -
cell behaviour(Walker et al., 2004) - as well as in the
social sciences(Cederman, 2002). While ABM shows
a lot of promise in being able to model the individual
aspects of patients and hospital staff, up to this point
the authors have been unable to find any reference to
prior work involving the use of ABM in healthcare
operational management.
3 DECISION SUPPORT SYSTEM
Making decisions about the current and future opera-
tions of even a small sized emergency department is
a complicated and ever-changing task. One assistive
measure in these circumstances is a Decision Support
System(Wang et al., 2009). Such a tool, supplied with
the correct input data can provide insight into the in-
ner workings of a real world system that can be diffi-
cult, if not impossible to glean using traditional meth-
ods.
A DSS can take many forms, however its purpose
is the same; given information from a current or pro-
posed system and configured based upon the expec-
tations of the user, a DSS should be able to process
that information and present it in a form which aids
the decision making process. This tool may be com-
prised of a single programatic aid, or a number of
tools working in consort, although in this final case an
additional layer may be required to package the infor-
mation from all tools into a single coherent interface.
One example of a tool that is often employed as a
Decision Support System component is simulation. A
simulation, given correct configuration and input data
can allow the user to discover the interrelated effects
of changes in various parts of the system without the
need to try these changes in a live environment, a def-
inite advantage when the live system is so important.
The most effective Decision Support Systems are
those were the users are the ones who gain the most
advantages from the tool being in place.
The measure of the effectiveness of a Decision
Support System is the advantages that it gives to the
user of the system. In the case of a hospital emer-
gency department this would be the manager or de-
partment head who is planning improvements to an
existing department, or possibly even designing a new
AGENT-BASED SIMULATION TO SUPPORT DECISION MAKING IN HEALTHCARE MANAGEMENT
PLANNING
437

department. The goal of such a tool is to allow the in-
dividual to be able to adjust the the input parameters
themselves and receive timely feedback on the effects
of these changes in a form that they can easily inter-
pret.
In order to provide meaningful output, a simula-
tion based DSS must be able to describe a number of
physical and abstract entities. Physical entities can be
divided into two groups, the individuals, or agents,
and the environment in which they interact. Indi-
viduals represent the patients and hospital personnel,
while the environment is the emergency department
itself and possibly operationally adjacent sections of
the hospital. The abstract entities refer to the social
and economic factors that are as just importantas met-
rics such as how many patients can be processed by
the triage department per hour.
A Decision Support System centres around an-
swering questions in order to aid healthcare managers
make the best informed decisions possible. Obviously
asking the correct questions is an important part of the
process, and in most cases these questions can be di-
vided into two groups.
The first group are the simplest and require more
interpretation on the part of the user of the DSS. These
are the “what if...?” questions. Answering these ques-
tions is an attempt to divine what will happen to the
system as a whole if one or more changes are made
to the parameters that define it. In this case examples
may be:
• what if an additional triage nurse is present dur-
ing the busiest period of the day?; or
• what if a flu epidemic raises the number of pa-
tients seeking treatment by 40%?
While a manager may be able to answer some of
these questions based on their own experience, there
is the possibility that these changes will have addi-
tional and unexpected consequences which are more
likely to be revealed by the process of simulation.
The second group of questions are much more
complex, requiring both a better understanding of the
system as well as additional definitions within the
Decision Support System. These questions involve
the optimisation of the system given certain param-
eters and indices. The additional definitions in the
DSS are the indices involved, these may be concrete
numbers such as total cost of personnel or may be
much more fuzzy concepts such as patient satisfac-
tion. Once these indices have been defined it is im-
portant to also define what value for these indices is
considered optimal. Then the user of the DSS may
ask how to optimise the system based on a group of
indices, or how to optimise a given index while keep-
ing another above a certain threshold.
These optimisation tasks can be incredibly time
consuming on the part of the Decision Support Sys-
tem, especially when some of the indices under ex-
amination are represented differently from others. A
system comprising of both quantitative and qualita-
tive indices makes a simple formula based solution
impractical and the required processing power usu-
ally increases dramatically. It is important to take into
consideration that a DSS must provide timely feed-
back to a user.
When seen in the realm of healthcare operational
management the system response time must allow the
user to adjust variables and receive feedback while
they are working, this will allow them to more eas-
ily understand the relation between what they have
changed and the effects that change has on a system.
To achieve this degree of responsiveness when sim-
ulating a large complex system it is quite likely that
High Performance Computing (HPC) techniques, as
provided by Cloud Computing, will form an integral
part of the solution.
Decision Support Systems can be useful tools in
aiding the decision making process, however it is im-
portant that they are easily usable by the people who
are seeking answers from them and also must be able
to produce results within acceptable time frames.
4 MODEL OF AN EMERGENCY
DEPARTMENT
In order to solve the previously discussed problems a
number of strategies are being used to create a general
and validate-able model. Firstly the model is being
constructed in a modular fashion. The model itself
is comprised of a number of smaller sub models that
comprise each of the main arenas of interaction for
the individuals present in the system. The orientation
of these sub models within the larger model is shown
in figure 1.
Within the emergency department itself there are
four main areas for interaction as shown in figure 1;
Administration, Triage, Diagnosis / Treatment, and
the Waiting room. There is also a fifth sub model that
represents the laboratory tests, although this need not
be modelled with the same level of precision at this
time as it’s unlikely to involve such complex human-
human interactions, this multi-paradigm model type
is explored further in section 4.1.
Five classes of individuals have been defined.
These five classes are patients (ρ), companions of
patients (ς), administrative staff (α), nurses (η), and
doctors (δ). The individuals within these classes are
also heterogeneous with respect to one another, which
HEALTHINF 2010 - International Conference on Health Informatics
438
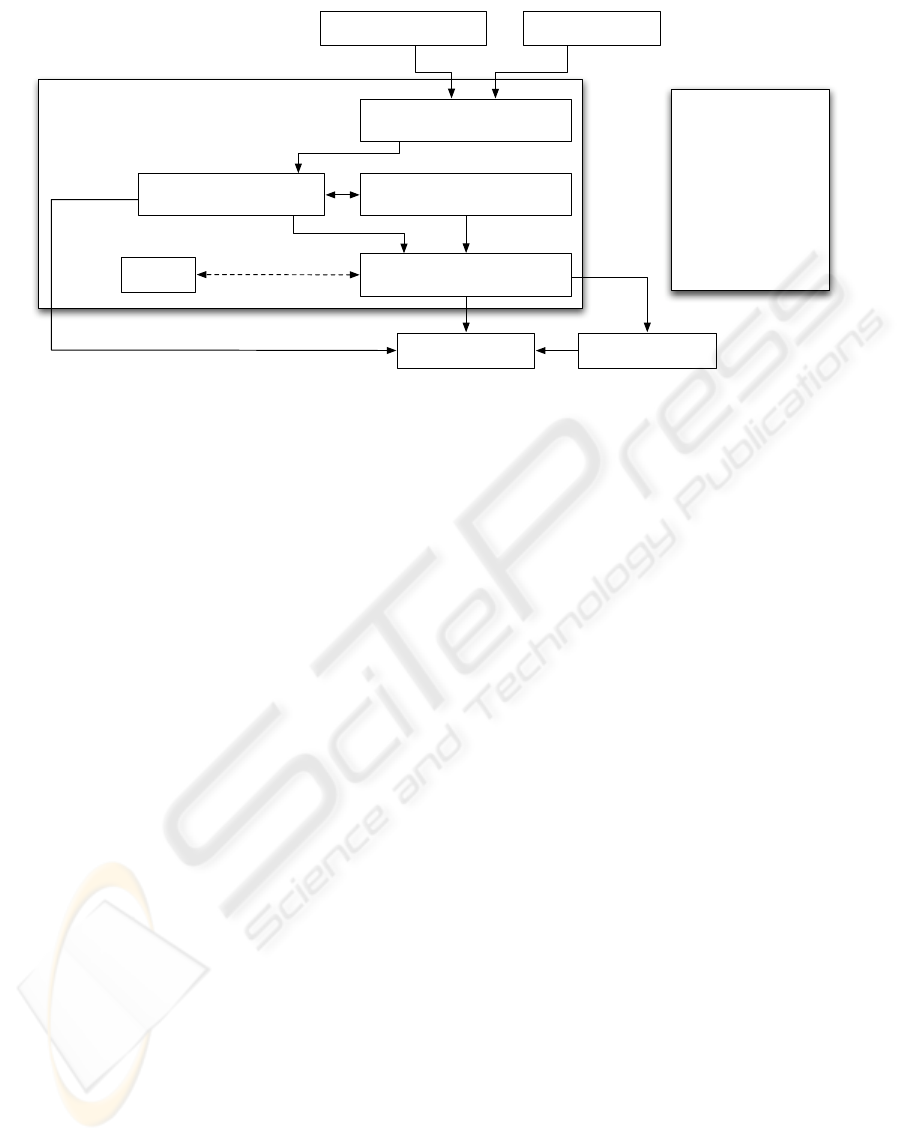
Emergency Department
voluntary exit
data
Legend
ρ - patient
ς - companion of
patient
α - administration
staff
η - nurse
δ - doctor
I( ) - interaction
between individuals
Laboratory
tests
Waiting room
I(ρ, ρ, Wai), I(ρ, ς, Wai)
Main Emergency
Department Entrance
Entrance via
Ambulance
inpatient
admission
Administration
I(ρ, α, Adm); I(ρ, ρ, Adm); I(ς, a, Adm)
Triage
I(η, ρ, Tri), I(ρ, ς, Tri), I(η, ς, Tri)
Diagnosis / Treatment
I(ρ, η, Dia); I(δ, ρ, Dia)
Exit Hospital
Figure 1: Overview of agent interaction stages within an emergency department.
is to say that each individual classified as a nurse
also has their own properties unique to themselves
amongst other nurses.
Interactions between two individuals is denoted
by the function I(x, y), where x and y represent the
class of individual. The order is meaningful in the
case of the interaction, the individual stated first (x in
this example) is the initiator of the interaction. So an
interaction between a doctor and a patient, initiated
by the doctor would be denoted by I(δ, ρ).
The environment where an interaction takes place
may well change the form and outcome of the interac-
tion. When describing an interaction within the entire
emergencydepartment as a whole we extend the inter-
action function to include a location attribute as well,
I(x, y, hloci). To extend our previous example of an
interaction between a doctor and a patient and specify
that it is occurring within the diagnosis and treatment
sub model we would define it like this, I(δ, ρ, Dia).
It is important at this stage to remember that what
is being represented is the interactions between real
people in real environments, a less technical descrip-
tion of the function defined here would be to say:
A doctor approaches a patient waiting in a
bed in the diagnosis area to begin a discussion
of the level of pain they are experiencing due
to what appears to be a broken leg.
The extra information given here is not lost in the
model, nor the representation in function form, it is
provided within the agents. It is an attribute of the
patient that they have a broken leg and an attribute
of the doctor that they are approaching the patient in
order to discuss the level of pain resulting from this
injury. Further details of the models of individuals
are discussed in section 5.
4.1 Modular Design and the
Multi-paradigm Approach
As stated previously, the model of the emergency de-
partment is made up of a number of smaller sub mod-
els. These design structure provides a number of ad-
vantages. The first is in breaking down the problem
into smaller and more manageable sections. Each sec-
tion has been separated out based on the interactions
involved within it, more specifically which hospital
staff are involved. While all staff will have a gener-
alised idea of how the emergency department works
the bulk of their knowledge is necessarily focussed
on their own area. By dividing the sub models in
this way the process of system analysis is simplified
because staff from different areas can be interviewed
separately, constructing each sub model in turn rather
than trying to build everything at once.
This scheme of building each sub model sepa-
rately also offers the advantages of unit testing, a pop-
ular method for separately verifying individual mod-
ules of code used in software engineering. Each sub
model is built and then tested using sample or sta-
tistical data to verify that it is accurate within itself.
This greatly reducing the time spent hunting for erro-
neous parts of the model if the whole model output is
not what is expected once all the separate sub models
have been attached to one another.
The third advantage of using a modular design for
the model is the ability to create a multi-paradigm
model in order to take advantage of modelling tech-
niques that best suit each part of the system(Stainsby
et al., 2009). The laboratory tests are a good example
of where this brings an advantage. Because the focus
of the model is the interactions the patient has while
AGENT-BASED SIMULATION TO SUPPORT DECISION MAKING IN HEALTHCARE MANAGEMENT
PLANNING
439

in an emergency department the laboratory is lacking
in any significant form of interaction. From a patient’s
point of view, a sample is taken and at some pointlater
it will be ready for collection. Each of these samples
could be modelled as an individual, but this is really
an unnecessary use of resources given that a labora-
tory sample has neither personality nor memory. In
this case it may make much more sense to create a
sub model defined by tokens waiting in a queue for
their turn to be processed, the output of this is then re-
turned to another part of the model where it is likely
to invoke the action of an individual.
Each sub-model has various attributes and outputs
which together form the larger picture of the reality of
an Emergency Department. Therefore the sub-models
may be made up of economic, logistic, and social
models, as well as other information required to solve
the optimisation questions of the DSS.
4.2 Social and Human Behavioural
Factors
Social factors are an important part of all human in-
teraction. A person may react differently to the ex-
act same situation depending on their current state of
mind, the environment they’re in or a range of other
factors. Many simulations do not take human factors
into account, this can lead to results that are unable to
fully represent all parts of an emergency department
that are effected by human decisions.
Research has shown that social and behavioural
factors can play an important role patient decision
making with regard to healthcare, from as early in the
process as whether or not they choose to seek out care
to begin with(Brailsford et al., 2006). The complex
social and psychological factors that drive the desires
and beliefs of people are made many times more com-
plex when they interact with others around them, it is
these interactions that are important during the time a
patient spends in an emergency department.
By using an agent-based model human behaviour
can be modelled at the individual level, rather than
the combination and average of all human behaviour
across the simulation. This becomes more important
when the interactions at one stage may effect the man-
ner in which an individual acts in another stage, pos-
sibly creating behaviour changing feedback loops.
4.3 Generality of the Model
One of the possible reasons for the lack of mainstream
take-up of simulation as a decision support tool in
hospital emergency departments discussed previously
is the idea that a model built for one department is not
applicable to another. For this reason the model being
developed is being done so in concert with more than
one partner hospital. This has a two fold effect on the
same issue.
The first is that by working with more than one de-
partment the differences and similarities will quickly
become obvious, suggesting which parts of the model
may be given default values and which need to be im-
plemented as parameters so as to be easily change-
able by the user at a given site. When it is said that
some parts may be given default values, that may be
easily changed in the future to accommodate different
emergency departments in different hospitals. When
it comes to creating the simulator this is already good
programming practice and should not cause too many
problems.
The effect is that the model can be shown to be
applicable to more than one department from the be-
ginning of its lifecycle. This reduces the perceived
ownership and single use nature of the model just by
it being used by multiple departments at the beginning
of its life cycle.
5 MODELS OF AN INDIVIDUAL
While the modular nature of the model described in
the previous section creates an architecture of mod-
els within a model, the use of Agent-Based Modelling
creates yet another level. When using ABM each indi-
vidual is essentially an instance of a model. The num-
ber of models used to describe the agents and their
complexity depends on the level of detail required.
Each individual may be modelled using almost
any modelling or control technique available, from
simple algorithmic or boolean decision making to
methods often not seen in modelling such as sub-
sumption architecture. In fact it is quite possible
to create individuals that are in fact controlled by
their own Agent-Based Models, although logically
this cannot go on forever.
In the model described in section 4, the actions of
each individual are controlled by a Finite State Ma-
chine (FSM). The form of each FSM is dependent on
the class of the individual (patient, companion of a
patient, administrative staff, nurse, or doctor). Within
each of these five classes the behaviour of an indi-
vidual is determined by certain attributes which are
assigned to them, giving each one their own individu-
ality.
These models of individuals also govern the man-
ner in which individuals interact, both with other in-
dividuals and with the environment in which they re-
side.
HEALTHINF 2010 - International Conference on Health Informatics
440

In the same manner as the indices used to define
aspects of the real world system when using a Deci-
sion Support System, the attributes of an individual
may not all be of the same type, nor may they all
be static during the course of the simulation. Some
values may be numeric in nature, such as how much
blood a patient has lost, others may require fuzzy
states to more accurately represent naturally occur-
ring, non-numeric conditions such as human concen-
tration.
These factors can be defined as either mutable or
immutable attributes, representing factors that may or
may not change during the course of the simulation
respectively. Mutable attributes may represent such
factors as the level of pain or stress experienced by
an individual at a given moment or the short term
memory of an individual with regard to their expe-
riences within the simulated period. Immutable at-
tributes may represent the level of training a nurse or
doctor has, or the individuals ability to communicate
based on their competence in the local language, these
form the properties of the agent which are unlikely to
change during the course of the simulation.
6 CONCLUSIONS
In the field of healthcare operational management it
has been shown that simulation can be a useful tool.
A number of examples exist in the literature, although
the lack of results from complete implementations
shows that simulation in this area has not reached its
full potential.
A number of requirements for a general and ver-
ifiable simulation are presented. Starting from these
requirements a new model has been created specifi-
cally to work towards creating a tool that can be used
as a basic component of a Decision Support System
which will be easily usable to healthcare managers
to gain insight into the inner workings of current or
planned emergency departments.
A key feature of this project is the use of Agent-
Based Modelling techniques to both take into account
the important social and psychological factors that
come into play during human interactions in high
stress environments such as emergency departments,
but also to aid to reducing the dehumanising appear-
ance of simulation tools from the point of view of
healthcare managers.
The work on this model continues to proceed
based on ongoing investigation and partnership with
a number of hospitals.
ACKNOWLEDGEMENTS
We would like to thank Montse Edo for the detailed
and invaluable assistance provided in describing the
operations of the triage department where she works.
Without the help afforded, this work would not have
been possible.
REFERENCES
Ayatollahi, H., Bath, P. A., and Goodacre, S. (2009). It
in the emergency department - what is the impact of
technology? Proceedings of the International Con-
ference of Health Informatics (HEALTHINF), pages
454–457.
Brailsford, S. (2007). Tutorial: Advances and challenges
in healthcare simulation modeling. Proceedings of the
Winter Simulation Conference, pages 1436 – 1448.
Brailsford, S., Sykes, J., and Harper, P. (2006). Incorpo-
rating human behavior in healthcare simulation mod-
els. Proceedings of the Winter Simulation Conference,
pages 466–472.
Cederman, L. (2002). Endogenizing geopolitical bound-
aries with agent-based modeling. Proceedings of the
National Academy of Sciences of the United States of
America, 9(3):7296–7303.
Connelly, L. and Bair, A. (2004). Discrete event simu-
lation of emergency department activity: a platform
for system-level operations research. Academic Emer-
gency Medicine, 11(11):1177–1185.
Fone, D., Hollinghurst, S., Temple, M., and Round, A.
(2003). Systematic review of the use and value of
computer simulation modelling in population health
and health care delivery. Journal of Public Health,
25(4):325–335.
Gonz´alez, J., Dalforno, C., Suppi, R., and Luque, E. (2009).
A fuzzy logic fish school model. Procc. ICCS 2009,
LNCS, 5544:13–22.
Lowery, J. (1996). Introduction to simulation in health
care. Proceedings of the Winter Simulation Confer-
ence, pages 78 – 84.
Stainsby, H., Taboada, M., and Luque, E. (2009). Towards
an agent-based simulation of hospital emergency de-
partments. Services Computing, 2009. SCC ’09. IEEE
International Conference on, pages 536 – 539.
Taylor, K. and Dangerfield, B. (2005). Modelling the feed-
back effects of reconfiguring health services. Journal
of the Operational Research Society, 56(6):659 – 675.
Walker, D., Southgate, J., Hill, G., and ..., M. H. (2004).
The epitheliome: agent-based modelling of the social
behaviour of cells. Biosystems, 76:89–100.
Wang, J., Gwebu, K., Shanker, M., and Troutt, M. (2009).
An application of agent-based simulation to knowl-
edge sharing. Decision Support Systems, 46:532–541.
AGENT-BASED SIMULATION TO SUPPORT DECISION MAKING IN HEALTHCARE MANAGEMENT
PLANNING
441
