
ADAPTIVE NIBP LOW-PULSE DETECTION
Detecting Low-pulse Adaptively
Ricardo Henrique Gracini Guiraldelli and Ricardo Luis de Azevedo da Rocha
Polytechnic School, University of S
˜
ao Paulo, Prof. Luciano Gualberto Avenue, tv. 3, 158 , S
˜
ao Paulo, Brazil
Keywords:
Non-invasive blood pressure, Low pulse amplitude, Adaptive decision trees, Adaptive technology.
Abstract:
This paper presents a proposal of an adaptive device for low-pulse detection on NIBP measurements using
an adaptive decision tree algorithm (AdapTree) and a probabilistic methodology, besides featuring learning
related to expert knowledge.
1 INTRODUCTION
Non-invasive blood pressure (NIBP) is a must-have
measure on critical and day-by-day diagnosis, provid-
ing fast and contiguous feedback about general health
aspects from patients through a simple method of ar-
terial pulse observation (electronically, pneumatically
or acoustically way), supporting the medical staff de-
cisions over one treatment. But its “noninvasibility”
has some side effects such as amortized signal, what is
oddly problematic on low pulse amplitudes cases. For
instance, it has been the “neck” of NIBP and the in-
creasingly dependence on automatic electronic mea-
surement just enlarged the problem.
As as example, there is a correlate research from
(Lin et al., 2003) that deals with noise compensation
generated by movements artifacts in NIBP measures.
It uses fuzzy logic to calculate the smoothness of os-
cillometric curve. We are using adaptive technology,
on the other hand, somehow complementing it.
Aiming this specific problem, the present work
proposes a technique for low pulse amplitude recog-
nition and detection, as well as dynamic learning of
these cases, seeking to improve the facility brought
by NIBP, particularly on intensive care units (ICUs).
For text comprehension, this paper is organized as
follows: from section 2 to section 4 we introduce the
background techniques behind our proposal; at sec-
tion 5 we describe the designed solution and at the
6the section we summarize our conclusion and expec-
tations.
2 NON-INVASIVE BLOOD
PRESSURE
Measurement of the arterial pressure is of greater im-
portance on patient’s diagnostics because of the high
density of information about the body condition —
especially hemodynamic system — it provides. Al-
though the ideal arterial pressure is made invasively,
this methodology is too much costly in health as-
pect to the patient and a very risky procedure. For
this reason some non-invasive blood pressure (NIBP)
methods were developed, like auscultatory, Korotkoff
sounds and oscillometric, the latter one we will focus
on.
The oscillometric method is widely used on au-
tomatic biomedical devices because it is independent
of a human expert for proceeding with the measure-
ment and it is extremely simple, based on descendant
step-pressures (as shown on figure 1). At the end of
the measure, the signals collected allow the plot of
a pressure (mmHg) × pulse amplitude) chart, where
is possible to extract the mean arterial pressure (P
m
),
the pressure where occurs the global maximum of the
curve. Once we have the P
m
, we can calculate the sys-
tolic pressure (P
s
) and diastolic pressure (P
d
) by the
equation that follows:
P
m
=
2
3
· P
d
+
1
3
· P
s
(1)
Although the oscillometric method seems as an
ideal one, it is less efficient when the measure presents
artifacts or low pulse amplitudes. Even thou it contin-
ues to be the best method for automatic biomedical
devices nowadays.
113
Gracini Guiraldelli R. and de Azevedo da Rocha R. (2010).
ADAPTIVE NIBP LOW-PULSE DETECTION - Detecting Low-pulse Adaptively.
In Proceedings of the Third International Conference on Biomedical Electronics and Devices, pages 113-116
DOI: 10.5220/0002741101130116
Copyright
c
SciTePress
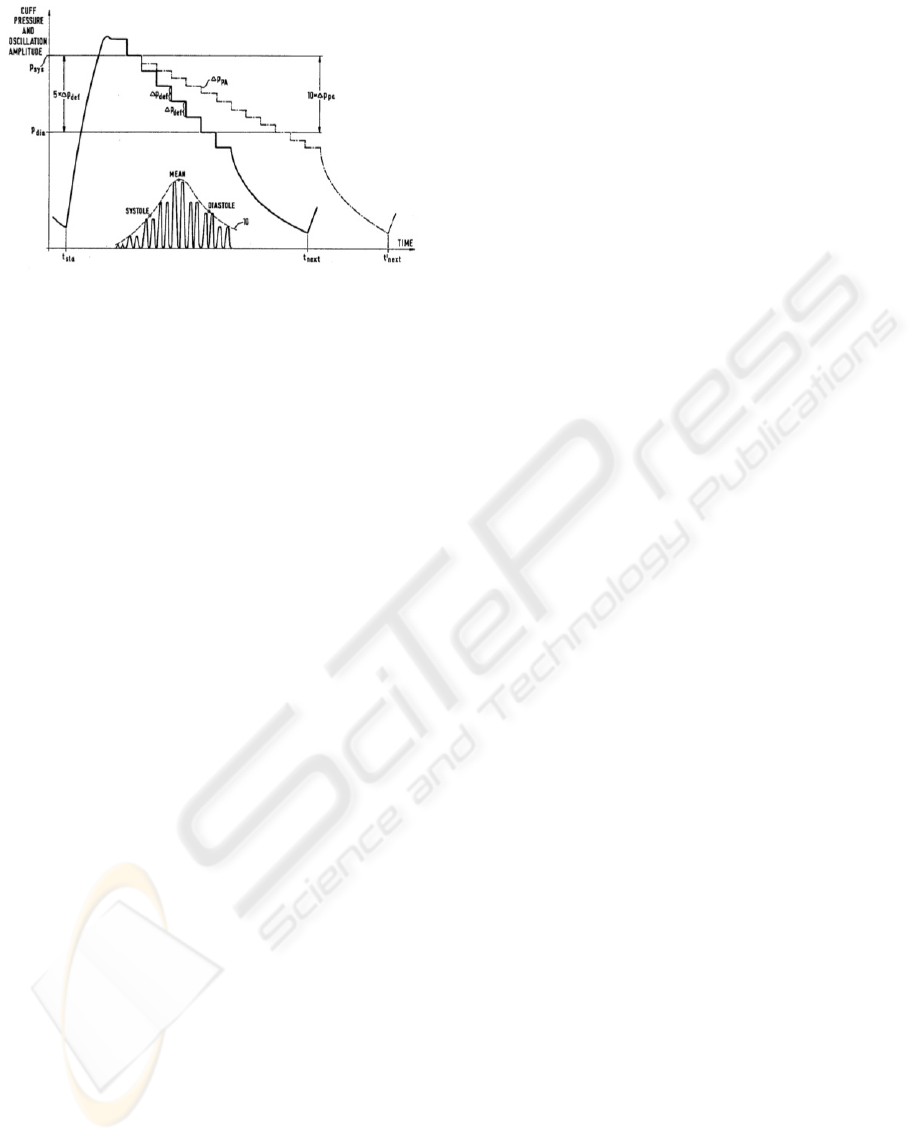
Figure 1: NIBP curve through oscillometric method
(Frankenreiter, 1990).
3 PROBABILISTICS METHODS
The probabilistic techniques have widespread use on
artificial intelligence because of their capability of in-
formation inference from small (or even lack of) data
about the decision subject and are sustained by math-
ematical formalisms giving, this way, some reliable
information.
Nowadays these techniques are even more popu-
lar because of the “smart software” development, i.e.
software that executes a whole (and complex) task
without rational human intervention (e.g. buying sug-
gestion software at online bookstores). And these ap-
plications are getting so evolved that they are already
at some specialized fields.
Resulting from that era of software development,
a probabilistic method called certainty factor (Pearl,
1988) was designed focusing on bringing some ex-
pert knowledge to probabilistic reasoning, especially
medical support one. Even more, it was thought to be
simple to implement and provide fast inferences.
Certainty factor works with a set of hypothesis-
evidences rules based on expert knowledge (interde-
pendent or not) that, interconnected, infer some sys-
tem’s information. For reasoning purposes, each hy-
pothesis or evidence has a certainty degree (c
d
) such
that −1 ≤ c
d
≤ 1, pointing out total unbelief (−1) or
total belief (1) on the events veracity.
4 ADAPTIVE TECHNOLOGY
For complex systems development, some flexibility
during decision making is an essential requirement.
Today, biological systems are almost the unique ones
that have this ability but some (mathematical) adap-
tive formalisms were developed, and they are capable
of changing themselves at runtime (Neto, 1993; Shutt,
1995).
At the present work, adaptivity means dynamic
modification of a rules set that controls a specific de-
vice, i.e. given a device, your transition function (or
rules set) is dynamically modified at runtime of such
device. It’s a rough simplification of the Adaptive
Technology concept presented on (Neto, 1993), but
keeps the main meaning of it.
Adaptive technology has wide uses, especially
in context change systems, as voice recognition and
user-personalized systems (as biomedical software).
In the attempt to satisfy the wide niche of applica-
tions, a number of adaptive devices were developed,
all of them based on pre-existing and known models;
e.g., adaptive finite automata(Neto, 1993), statecharts
(Neto et al., 1998), decision tables (Pedrazzi et al.,
2005) and trees(Pistori and Neto, 2002; Pistori and
Neto, 2003). We are going to focus particularly on
the last one.
4.1 AdapTree
When classifying data, decision trees are efficient de-
vices for the task; based on this concept, there are
numbers of algorithms(Quinlan, 1996).
Traditional decision trees needs some training
over a solved body of “problem cases”. This train-
ing is a huge limitation for systems that have a learn-
ing requirement and, for instance, there are some al-
gorithms like ID3 that envisions some kind of learn-
ing based on re-training or become almost ineffective,
though. Targeting to improve it, the AdapTree (Pis-
tori and Neto, 2003) algorithm was developed using
adaptive technology, putting together decision trees
and adaptive finite state automata.
AdapTree still requires some training, receiving
an input string with an additional data field for class
representation (figure 2), what we will call as static
learning. When changing from training mode to clas-
sification mode, we just need to suppress that addi-
tional data field for classification under the classes
previously trained.
Whenever it finds a “problem case” that has not
matched a classification pattern at the tree set, Adap-
Tree calls an statistical mechanism based on relative
observed frequency up to the moment and the string
sequence already read, concluding the most probable
class for that input data.
Although it seems too simple, AdapTree has been
well positioned on benchmarking tests(Pistori and
Neto, 2003) among several well-known algorithms,
showing a great benefit/cost relation for a large num-
ber of projects.
BIODEVICES 2010 - International Conference on Biomedical Electronics and Devices
114
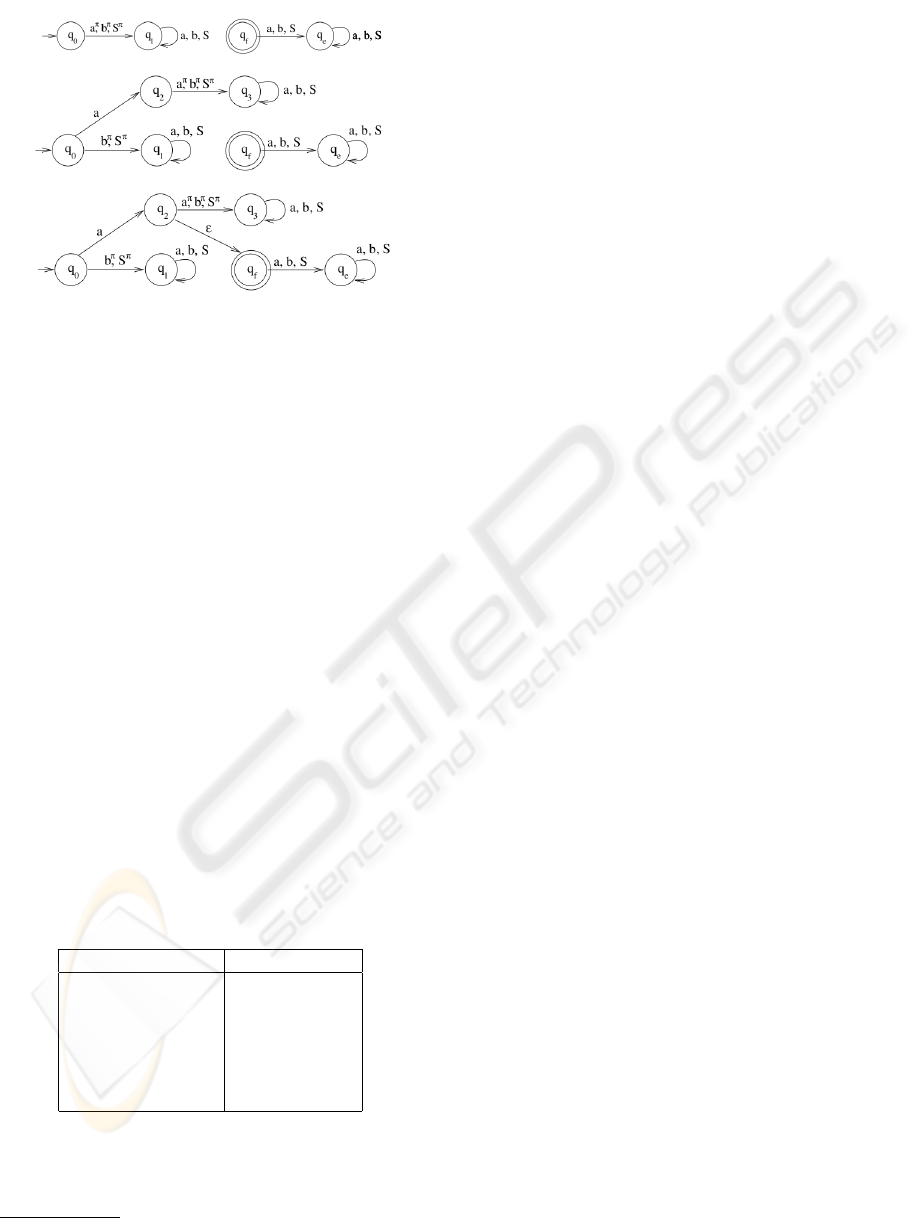
Figure 2: Three stages of AdapTree: the beginning, after a
string read a, after a string read aS, respectively.(Pistori and
Neto, 2003).
5 PROPOSAL
Once given the entire theoretical basis for understand-
ing the problem we aimed, this section formalizes a
proposal for the low-amplitude pulse problem (that
we will refer as low-pulse).
Low-pulse is a condition of extremely difficult de-
tection and though many A/D transducers have the
capability to detect that amplitude, it is not safe to
keep that sensibility activated because many environ-
mental interferences (like patient’s movement) may
be erroneously translated as pulse signal. But some
classes of special patients commonly presents this
condition, when they are under drug or pathologi-
cal effects, or even naturally, possibly introducing
complications for their correct treatment and diagno-
sis. Analyzing some NIBP measures bank
1
, we were
able to design a simple class-feature classification that
keeps cause-consequence relationship with low-pulse
as shown below:
Table 1: Classes related with low-pulse.
Class Feature
Patient Neonate
Patient Elderly
Place ICU
Place Surgical Ward
External Modules Ventilation
External Modules Anesthesia
It is important to note that the above information
are available on ICU monitor once they’re used to
configure alarms, cuff pressures and other safety re-
1
This NIBP bank of measures is private and it is exclu-
sive of an ICU monitor manufacturer.
sources. Hence, the classification is appropriate to use
on (almost) every ICU monitor without restrictions.
Although table 1 seems too simplified for some
significant improvement, it’s enough for problem def-
inition without negative side effects on quality pulse
detection; doubtful datum won’t be necessary, in this
research scope, for an appropriate solution definition.
Once we have the classes of probably low-pulse
occurrence cases, the expected step is to realize some
kind of algorithmic classification of them making
possible a correct low-pulse classification based on
those input datum. Previously, on section 4, we have
seen that decision trees are the natural mechanism
for knowledge classification; ID3 or C4.5 algorithms
could be used but, as discussed early, biomedical
equipments need some personalization characteristics
for each new patient, hence, given this requirement,
AdapTree fits as the best solution.
Using AdapTree, we should train the algorithm
with real and classified data group (training body) for
some rule determination before the classifier (deci-
sion tree) usage. In the same way it would be done if
we were using some other conventional decision tree
algorithm. With a large enough database, we could
use it as a test body and reach a significant advan-
tage once the (statistically) majority of cases would
be covered with this kind of training.
If we cover the majority number of cases, why do
we need AdapTree for? We need it for those cases
in which common decision tree algorithms are unable
to classify the complementary group, converging to
the dynamic learning region of AdapTree; this kind
of learning is usually made by statistical inference,
based on counting.
Even thou literature benchmark (Pistori and Neto,
2002) shows its great performance, we must not use
the counting mechanism because it is not based on
medical knowledge for classifying data. We will use
instead a probabilistic technique already used on med-
ical decision auxiliary software, the certainty factor
— which may be referenced as inference machine —
, developing a hermetic rules set based on specialist
knowledge (hypothesis relations) and statistical infor-
mation (hypothesis weights).
Therefore, we propose the set of hypothesis of the
inference machine as the classes presented on 1 and
the development of the relations as showed on fig-
ure 3.
5.1 Connecting the Devices “Low-pulse
Detector” and “Pulse Detector”
Once we have defined above the low-pulse detector
device, now it must be connected with the traditional
ADAPTIVE NIBP LOW-PULSE DETECTION - Detecting Low-pulse Adaptively
115
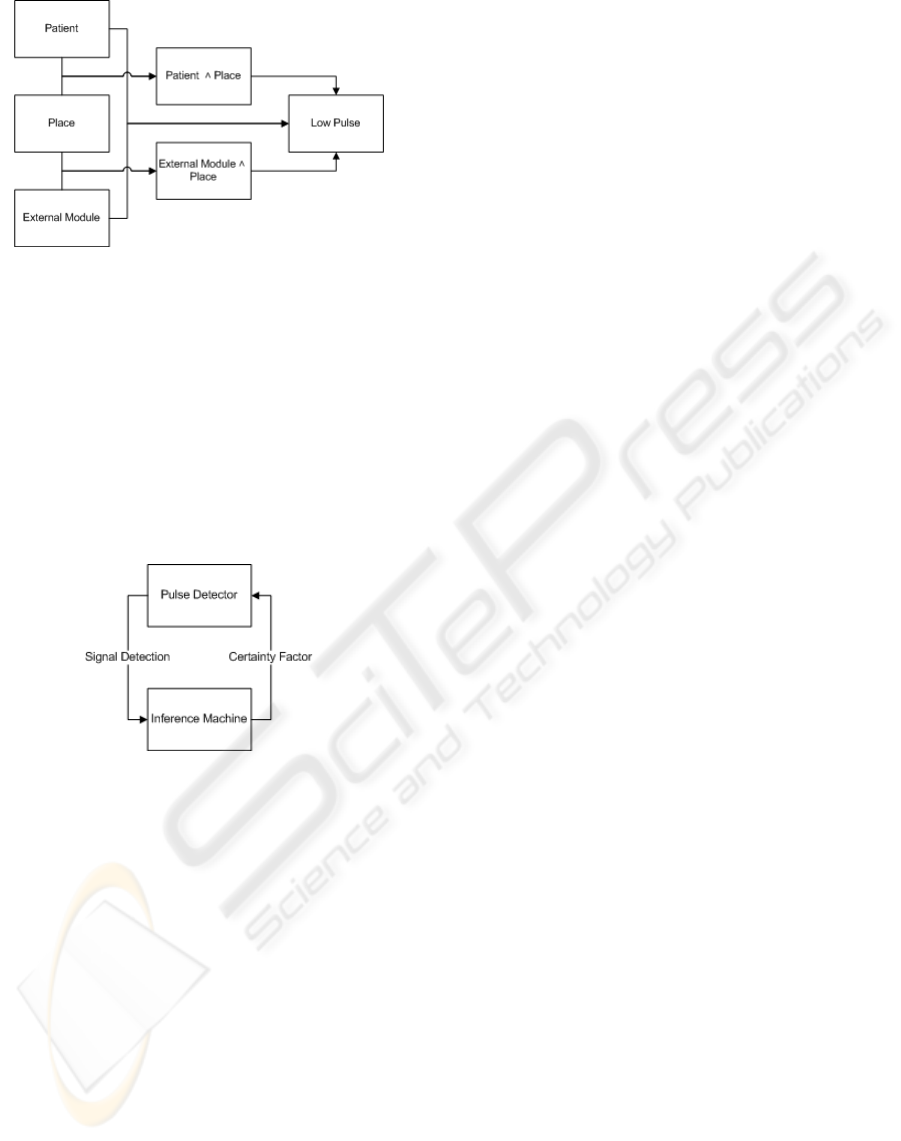
Figure 3: Hypothesis-inference machine relationship.
pulse detector device already implemented and in use
on the ICU monitor.
Focusing on minimum system interference, we
propose an event-driven (Ferg, 2006) mechanisms
connection: after a specific no pulse timeout, the main
module (which contains the pulse detector) requests,
through an event, that the low-pulse identifier (or in-
ference machine) evaluates and returns its certainty
factor as other data, for example new pulse amplitude
levels (for detection). Figure 4 shows this connection.
Figure 4: Communication interface between pulse identifier
and inference machine.
A great advantage of this kind of communication
between the modules is that it keeps the information
segregated in each module, isolating possible soft-
ware bugs from one module to affect the whole NIBP
system and exposes this new module (low-pulse de-
tector) as a system improvement, either.
6 CONCLUSIONS AND FURTHER
WORK
This work proposes an evolution on apparently stag-
nated research field of NIBP (Rolfe, 1979), dealing
with risk low-pulse cases through the use adaptive
technology and probabilistic methods. The addition
of these two features on NIBP measurements brings
personalized diagnosis to automatic measure biomed-
ical devices.
A numerical validation is planned to verify the
methodology on the “field work” of the system and
explore the opportunity to look for improvements.
These data will be provided by a brazilian ICU mon-
itor manufacturer, based on their large real measure-
ments database and their certified and validate pulse
detector algorithm.
Another step to be taken is to complete the solu-
tion, so we will also propose the design of methods
for recalculating the (maximum and minimum) cuff
pressure limits providing, this way, a complete solu-
tion for low-pulse detection.
REFERENCES
Ferg, S. (2006). Event-driven programming: Introduction,
tutorial, history. Online.
Frankenreiter, M. (1990). Method for measuring blood
pressure and apparatus for automated blood pressure
measurements.
Lin, C.-T., Liu, S.-H., Wang, J.-J., and Wen, Z.-C. (2003).
Reduction of interference in oscillometric arterial
blood pressure measurement using fuzzy logic. Trans-
action on Biomedical Engineering, 50(4):432–441.
Neto, J. J. (1993). Contributions to Compiler Design
Methology. PhD thesis, Escola Polit
´
ecnica da Uni-
versidade de S
˜
ao Paulo. In Portuguese.
Neto, J. J., de Almeira Jr., J. R., and dos Santos, J. M. N.
(1998). Synchronized statecharts for reactive systems.
Proceedings of the IASTED International Conference
on Applied Modelling and Simulation. Proceedings
of the IASTED International Conference on Applied
Modelling and Simulation.
Pearl, J. (1988). Probabilistic Reasoning in Intelligent
Systems: Networks of Plausible Inference. Morgan
Kauffman.
Pedrazzi, T., Tchemra, A., and de Azevedo da Rocha, R. L.
(2005). Adaptive decision tables - a case study of their
application to decision-taking problems. Proceedings
of International Conference on Adaptive and Natural
Computing Algorithms - ICANNGA 2005. Proceed-
ings of International Conference on Adaptive and Nat-
ural Computing Algorithms - ICANNGA 2005.
Pistori, H. and Neto, J. J. (2002). Adaptree - proposal of an
algorithm for decision tree induction based on adap-
tive technology. Anais Conferłncia Latino Americana
de Informtica - CLEI 2002. In Portuguese.
Pistori, H. and Neto, J. J. (2003). Decision tree induction
using adaptive fsa. CLEI Eletronic Journal, 6.
Quinlan, J. R. (1996). Learning decision tree classifiers.
ACM Computing Surveys.
Rolfe, P., editor (1979). Non-Invasive Physiological Mea-
surements. Academic Press.
Shutt, J. N. (1995). Self-modifying finite automata: Power
and limitations. Technical Report, (WPI-CS-TR-95-
4).
BIODEVICES 2010 - International Conference on Biomedical Electronics and Devices
116
