
USER CENTERED DESIGN OF PATIENT USER INTERFACES
FOR REMOTE TRAINING SUPERVISION
A User Study
Florian Klompmaker, Karsten Nebe
University of Paderborn, C-LAB, Fürstenallee 11, 33102 Paderborn, Germany
Andreas Bleiker
Siemens IT Solutions and Services, C-LAB, Fürstenallee 11, 33102 Paderborn, Germany
Clemens Busch, Detlev Willemsen
Schüchtermann Schiller’sche Kliniken GmbH & Co KG, Ulmenallee 5-11, 49214 Bad Rothenfelde, Germany
Keywords: Tele-medicine, Tele-monitoring, User Centered Design, Usability, User Interfaces.
Abstract: Remote training supervision is a new approach that combines medical and IT knowledge into one system.
Such a system enables patients with cardiac diseases to continue a supervised training - on an ergometer
bicycle and even when exercising outdoors - after rehabilitation phase in a clinic. The goal of the study
presented in this paper is to develop user interfaces for an ergometer. These interfaces have to allow an
intuitive interaction and to take the different capabilities, needs and preferences of potential users - often
elderly people having visual impairments and different IT knowledge - into account. In order to create
minimal attention user interfaces it is mandatory to apply user centered techniques, which involve potential
users into the design phase of the development process. The evaluation of the study served as basis for the
next iteration of the user centered design process and raised new functional requirements to the underlying
system from the user’s perspective.
1 INTRODUCTION
Current surveys of the IT inter-trade organization
Bitkom showed that 59.8% of all Germans beyond
the age of 65 would like to use tele-medicine to
extend living in their familiar environment. We
estimate similar values for whole Western Europe
and North America. Further on 58% of the
interviewed persons indicated that they would make
use of alarm systems like tumble sensors, ECG or
apnea measurement when they are in need of care. It
is shown, that elderly people do not perceive this
observation as a problem but as assistance (see
Heise Online, 2008 I). Therefore there is the demand
on politicians and the public health sector to enable
age-based assistance systems for self-determined
living at home. Since the required technology is
available, assumption of costs for applications like
telemonitoring and tele-homecare has to be provided
by health insurances. The health care system can
benefit from such systems since they help to reduce
or avoid expensive hospitalizations (Stroetmann,
2007 and Heise Online, 2008 II). In the past years
costs in health care exploded. Thereby cardiac
diseases caused the major amount of money spent in
medical care.
Rehabilitation is well established and accepted for
sustaining a healthy life style after a cardiac event.
Studies have shown that one year after such an event
and rehabilitation phase II, not all patients reach
their training goals and in some cases their cardiac
risk factors even deteriorate (EUROASPIRE I and II
Group et al., 2001 and EUROASPIRE II Study
Group, 2001). Therefore intelligent IT solutions that
provide opportunities for prevention and secondary
prevention of cardiac diseases are crucial. In
addition such systems must come along with clearly
106
Klompmaker F., Nebe K., Bleiker A., Busch C. and Willemsen D. (2010).
USER CENTERED DESIGN OF PATIENT USER INTERFACES FOR REMOTE TRAINING SUPERVISION - A User Study.
In Proceedings of the Third International Conference on Health Informatics, pages 106-113
DOI: 10.5220/0002747701060113
Copyright
c
SciTePress
arranged and intuitively operable user interfaces,
because patients with cardiac diseases are often
elderly people that are not that familiar with
information technology. It is a major challenge to
design usable tele-medicine applications for this
target group.
To face this challenges a user centered design
approach is necessary. Potentially users that are
interacting with tele-medicine applications often
suffer under their current state of health. Therefore
the system should guide them carefully. They often
have age-related visual impairments and in the setup
described in the next section they are quite far away
from the screen. These facts have to be considered
when designing user interfaces for such patients.
2 THE OSAMI-D PROJECT
The European research project OSAMI and the
German sub-project OSAMI-D are funded by the
German Ministry of Education and Research
(BMBF) et al. In the project open services for
ambient intelligence are going to be developed.
OSAMI-D addresses tele-medicine and remote
ergometer rehabilitation in particular as an example
of use. Since ergometer training is a well-known and
effective rehabilitation appliance for patients with
cardiac diseases, we think that this scenario has the
potential to be realized as a commercial solution one
day. The idea of the scenario is that patients who
successfully finished rehabilitation phase II in a
hospital should be able to continue their training
afterwards in order to keep up the rehabilitation
process and avoid a new cardiac event. Therefore a
patient after rehabilitation phase II may herself
install an ergometer at home. This ergometer comes
along with several sensors for measuring vital data,
an internet connection and a touchscreen in front of
the exercising user. During an exercise training data
from the sensors is collected, automatically analyzed
and transmitted to a supervisor system. Supervisors
may then adapt the training plan of every patient
according to abnormalities recorded in the current
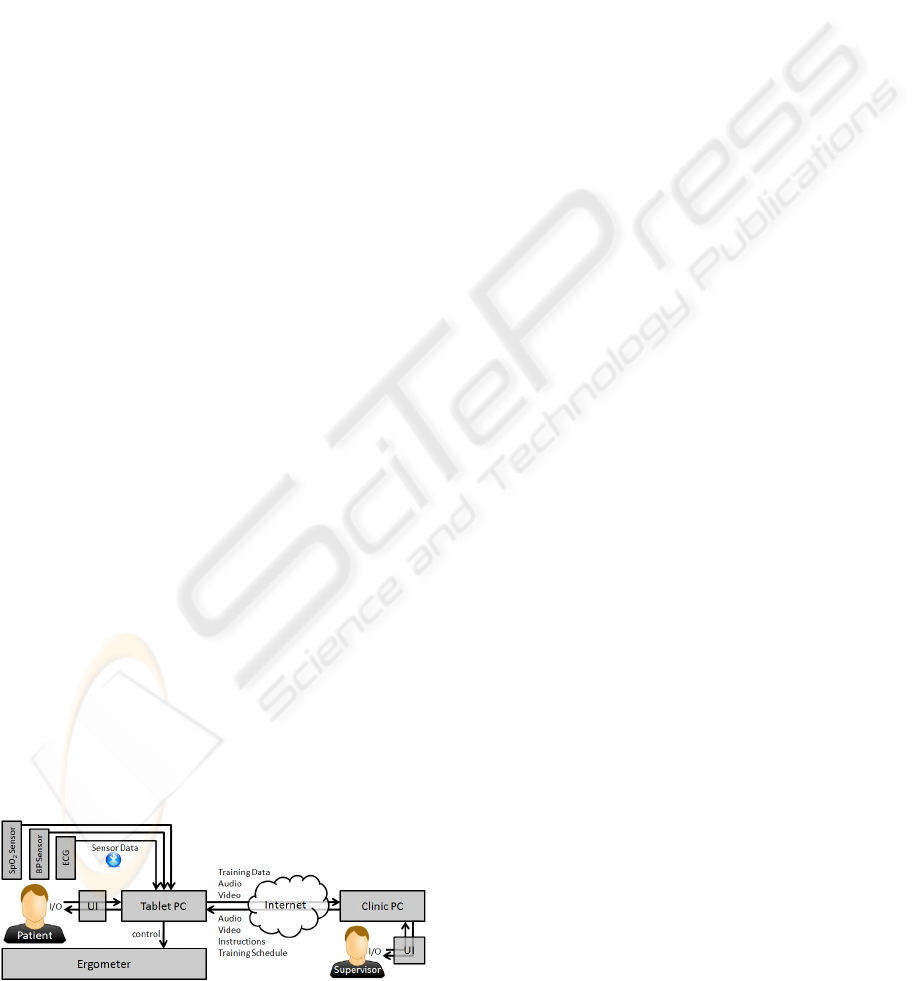
Figure 1: Scenario Schema.
and/or previous session. Figure 1 shows a schema of
the overall setup as far as the hardware components
at the patient’s home. The figure also shows the vital
data sensors that are connected wireless via
Bluetooth to the ergometer: An ECG sensor, a blood
pressure sensor and an oxygen saturation (SpO
2)
sensor. Technically, the setup consists of a tablet PC
that serves as user interface, internet gateway,
collector of sensor data and ergometer controller.
The ergometer itself offers access to adjustable
values via a network interface. E.g. it allows a
changing of the current load in Watts by applying
the correct pedaling resistance according to the
pedaling frequency of the user.
In the project we differ between three training
levels. In Level 1 there’s a one-to-one live
supervision between the patient and a supervisor.
The training data - including vital data measured by
the sensors and ergometer data - as far as audio and
video recordings of the patient are directly
transmitted to the supervisor. The supervisor
analyzes the data online and can change the training
schedule immediately or issue instructions to the
patient. Level 2 training is quite similar but here a
larger group of patients is observed by one
supervisor simultaneously. Audio and video
transmission is optional and can be manually
enabled or disabled by patients or the supervisor.
Finally Level 3 enables offline training for lower-
risk patients. These can exercise at any time they
like. The data is recorded but not transmitted before
the training is finished. A supervisor analyzes the
recorded data in post processing within a given time
period, e.g. 24 hours, and adapts the training
schedule if necessary. The schedule is transmitted to
the patient’s gateway PC afterwards. The Level 3
scenario also enables a mobile training. Patients can
use simplified versions of the vital data sensors to
collect data on their mobile phone or PDA via
Bluetooth while exercising outdoors. This provides
more flexibility to patients who can perform their
preferred sport on an arbitrary place. Even though
there’s no live supervision the system automatically
compares the vital data with threshold values
predefined in the training schedule by a supervisor.
If some data exceeds a limit the patient is informed
about that and she’s given a hint of how to react (e.g.
“Walk a bit slower”). Hence the responsibility in
terms of effectiveness and security lies on the
patient’s side solely.
3 RELATED WORK
The market of telemonitoring concepts and systems
especially designed for training demands is rare.
USER CENTERED DESIGN OF PATIENT USER INTERFACES FOR REMOTE TRAINING SUPERVISION - A User
Study
107

There are some bicycle ergometer using chipcard
controlled training, but there is no remote tele-
monitoring yet available. Currently two research
approaches exist: The SAPHIRE-Project (Busch et
al., 2009) - the precursor of the OSAMI-D project -
and the ongoing project HeartCycle
(http://www.heartcycle.eu) that also integrate online
exercise supervision into their platforms. SAPHIRE
did not consider Level 2, Level 3 or mobile training
since the project solely focused on realizing Level 1
training without audio- and video-conferencing. By
performing the user study we have been able to
gather first knowledge about what kind of user
interaction is useful and which parts of the
SAPHIRE interfaces seemed to be usable, which are
improvable and how. For the supervisor side we
already created user interface mockups that are
going to be evaluated and implemented
(Klompmaker et al., 2009). Since supervisors are
often familiar with complex visualizations of
medical data it is expected that it is more difficult to
create usable user interfaces for patients using such a
system.
Gay and Leijdekkers presented an approach on
how sensors for measuring vital data may be used in
mobile setups (Gay and Leijdekkers, 2007). Thereby
the ECG data is analyzed automatically and locally
in order to provide hints to the user or to alert pre
assigned caregivers whenever necessary. Anyway
here the data is not transmitted during or after an
exercise session but monitored permanently by
algorithms. Another project focusing on mobile
applications especially for elderly people is
presented by Oppermann et al. (2008). Here the
application that’s also monitoring vital data may also
only be controlled with the mobile device itself
resulting in small and very simple graphical user
interfaces. We can benefit from these results when
designing the mobile training application but we had
to do a user study for the user interface on the
ergometer screen from scratch.
The concept of the company T2BEAM
Technologies AG, Switzerland just emerged on the
market in January 2009. The product called athlosoft
(http://athlosoft.com) addresses healthy subjects,
who can get online training supervision. This system
is to the knowledge of the authors the most advanced
IT-telemonitoring concept on the market yet but as a
downside compared to OSAMI-D it does not allow
the definition of medical constraints controlling a
training session.
In summary we found out that there are
approaches existing that address the different
technical challenges of the OSAMI-D project and
the different end users. However there’s no system
existing using the different technical approaches of
live supervision on an ergometer, offline training
with predefined medical constraints and mobile
training altogether for patients with cardiac diseases.
We think it is necessary to achieve more insights of
the user’s needs, preferences and habits in this
specific use case. Therefore user centered design is
the best possibility towards developing a successful
and usable system.
4 USER STUDY
In the user study we did in a rehabilitation clinic we
tried to find out what the current situation and the
daily routine of patients looks like in order to use the
results for the system design. We will introduce the
interview lead through and the results here.
4.1 Current Setting
This section explains the current flow of the
ergometer training for patients with cardiac diseases
within a rehabilitation clinic. We carefully figured
out what’s important for patients and supervisors
here and how the several training steps are executed
in order to develop the OSAMI-D system according
to these workflows.
The in situ training in the early rehabilitation
phase is organized in groups of up to 15 patients that
are all exercising simultaneously. Therefore they all
start a warm-up phase simultaneously, reach the
training phase simultaneously and reach and finish
the cool down phase of the training simultaneously.
The focus of the supervisor here lies on visual
control and personal conversations. She
predominantly checks the body language and body
signals of the patients, e.g. skin color, sweating or
pedal regularity, in order to detect critical situations.
Further on she asks the patients about their
wellbeing periodically. The vital data that is
displayed on two large PC displays in a secondary
room is not that important and only considered
secondarily. Beside the proven medical effectiveness
the biggest advantage of an in situ ergometer
training is therefore the personal supervision through
qualified medical staff. Further on many patients
like the training within an exercise group because it
enables social interactions with other patients.
However there are some disadvantages of an in situ
ergometer training. It is described as very
monotonous by the patients because it provides little
variety. Comparing this exercise with an outdoor
HEALTHINF 2010 - International Conference on Health Informatics
108

bicycle training it is quite stultifying, e.g. the fresh
air, the air flow and the landscape are missing.
During in situ training the participants are looking
towards the walls of the exercise room and just
listening to quiet music. Further on patients stated
that the ergometer training is not challenging but
physically very easy. Since patients trust in the
supervisors and the training settings they accept this
issue but experience the ergometer training in a very
passive way and regular feedback from supervisors
is missing. Furthermore patients don’t even know
their personal training setting and schedule in detail.
The challenge here is besides designing intuitive
user interfaces also to raise new functional
requirements towards the underlying system in order
to implement new functionalities that motivate
patients to exercise periodically and to overcome the
monotony.
Therefore we collected the requirements and
analyzed the context of use of the OSAMI-D system
on the patient’s side as a base for the user interface
design. Since the training will not take place in situ
anymore but at the patient’s home we have to think
about numerous changes in the training flow and in
the interaction modalities between user and
computer.
4.2 Interview Lead through
We interviewed six patients in a rehabilitation clinic,
recruited by the clinic staff and in a previews session
(Klompmaker et al., 2009) also four ergometer
training supervisors. All patients have been
described as potentially adequate for remote
ergometer training supervision. Five of the six
patients were around retirement age (65 years in
Germany) one was a young adult (approximately 30
years old). All stayed in the rehabilitation clinic with
the objective of finishing a three week rehabilitation
program including in situ supervised ergometer
training three to five times a week. While five
patients did already reach their final rehabilitation
week the last one was still in the starting week of the
training. All of the interviewed persons live really
active social lives and are also physically active –
most of them stated that they like cycling and are
undertaking cycling tours quite often. Even though
some of them are beyond retirement age they all
seem to be very busy and pointed out to be pinched
for time. The patients all have basic computer
knowledge but aren’t computer experts. This seems
to be one reason the clinic stuff recruited them as
potentially adequate for remote ergometer training
supervision. Supervisors said that patients without
any computer knowledge won’t ever trust in such a
system. Therefore they won’t ever use it and are
from the clinic point of view no potential patients for
remote ergometer training supervision.
We used an interview-guideline with open
questions and performed semi-structured interviews
(Wengraf, 2001). After asking personal questions
and questions about the current in situ training (see
above) we introduced the different training levels
and scenarios to the patients. In doing so we
recorded all answers and comments as further user
input.
4.3 Results
This section introduces the main results of the semi
structured interviews by abstracting the main
declarations of the patients and analyzing the system
requirements from the user’s perspective.
Patients appreciate the possibility of performing
remote ergometer training supervision as an
expanded rehabilitation in general. At least those
with basic computer knowledge do not have doubts
regarding technology or organization. Since all of
the interviewed persons have been physically active
before they also do not have an issue with exercising
regularly in the future. Nevertheless all patients
stated that a long-term indoor ergometer training is
not attractive in comparison to alternative sports
especially outdoor ones. We think that therefore it is
desirable to develop even mobile solutions.
Patients with cardiac diseases have the need for
supervision, distraction and confirmation when
exercising. Especially they would like to get their
vital data visualized (“It would be nice if I knew my
own values!”). Knowing these values would enable
them to have food for thought and to know that
everything is copacetic. Automatic feedback (current
sensor values) is therefore very important.
Patients see many advantages in the planned
setup: They don’t need to arrange fix training dates
(at least not when applying Level 2 or Level 3
training) and they save time in comparison to an in
situ training in the clinic because they would have to
travel there. Further on they can define the
entertainment program on their own: Reading news,
listening to music, watch TV or surf the web.
Therefore an entertainment system as part of the
patient user interface is desirable. However we don’t
think that this will overcome the monotonous
training in the long term.
USER CENTERED DESIGN OF PATIENT USER INTERFACES FOR REMOTE TRAINING SUPERVISION - A User
Study
109

5 USER INTERFACE DESIGN
The results of early user questionnaires can be used
as a basis to create user interface mockups. These
serve afterwards as a basis for the second iteration of
the user centered design process where users are
asked to evaluate these mockups in a first prototype
application. In this chapter we introduce the design
implications we acquired from the results of the
questionnaires. Then we introduce some user
interface mockups as far as the conceptual ideas
behind them. Further on the interviews resulted in
new requirements towards the underlying software
system. These are introduced in an separated
chapter.
5.1 Design Implications for Remote
Super-vision
One of the most definite results we figured out is
that patients need to get their personal vital data
visualized to overcome the monotony of the training
and to compare the results concerning training
success and personal threshold values. Therefore the
graphical user interface of the OSAMI-D project
demonstrator should present the most important data
in a clearly arranged way. The interface should
further on provide a mechanism to show the
personal feedback from the supervisor in the form of
text messages as far as a calendar showing past and
future training dates.
We found out that the user interface of the
precursor project had some lack in consistency
especially regarding the colors of the graphical
elements. Patients stated that they don’t understand
the applied color coding of yellow and red buttons.
Further on some buttons aren’t even needed – e.g.
patients would never push a button when they decide
to stop the training because of illness but just stop
cycling and make further measures. Another
inconsistency in the coding was recognized at the
also implemented traffic light. Sometimes the yellow
color was used to inform the patient about a high
heart frequency - an alarm - sometimes it was used
to inform the user to continue the training. Hence it
was often unclear how dramatic the current alarm or
information really is. Another issue that was
evaluated as distracting was the length of the
questionnaires patients have to answer before and
after training in Level 2 and Level 3. Many questions
were unclear, others may be grouped, others are
completely unnecessary (e.g. “Are you feeling
good” – A patient that not feels good wouldn’t have
get on the ergometer to start training).
A last thing is that we had to take care of the size
of graphical elements and especially fonts when
designing the user interface. Patients are often
elderly people with visual impairments and they are
exercising when interacting with the interface. When
considering a mobile training it is therefore
especially important to only display the information
that is really needed. Here we’re also focusing on
auditory and physical feedback via rumble motors.
5.2 User Interface Mockups
The implications for remote supervision were used
to develop user interface mockups. Here we
introduce the most important mockup figures, the
overall layout and the idea behind it.
The main menu (Figure 2) appears after a patient
logged in using her username and password. Even
though it is not that easy for patients to remember
both we are using this login mechanism due to
security reasons. The main menu shows the latest
supervisor feedback (top left) and offers the
possibility to start a supervised training either in
online mode (bottom left, only if currently available)
or in offline mode (bottom center, always available
for low-risk patients). All is done via simple single
button clicks using a single finger. Since the user
interface elements are big (screen size is 17”) this is
easy for nearly every patient. Everything is clearly
arranged and the interface only offers the most
important functions.
Figure 2: Main Menu.
The main menu further on offers possibilities to start
a synchronization with a mobile device for
performing mobile offline training, to shut down the
system and to open the calendar. The calendar shows
all past and future training sessions as far as
information about changes in the training plan and
HEALTHINF 2010 - International Conference on Health Informatics
110
supervised or not yet supervised sessions in the past.
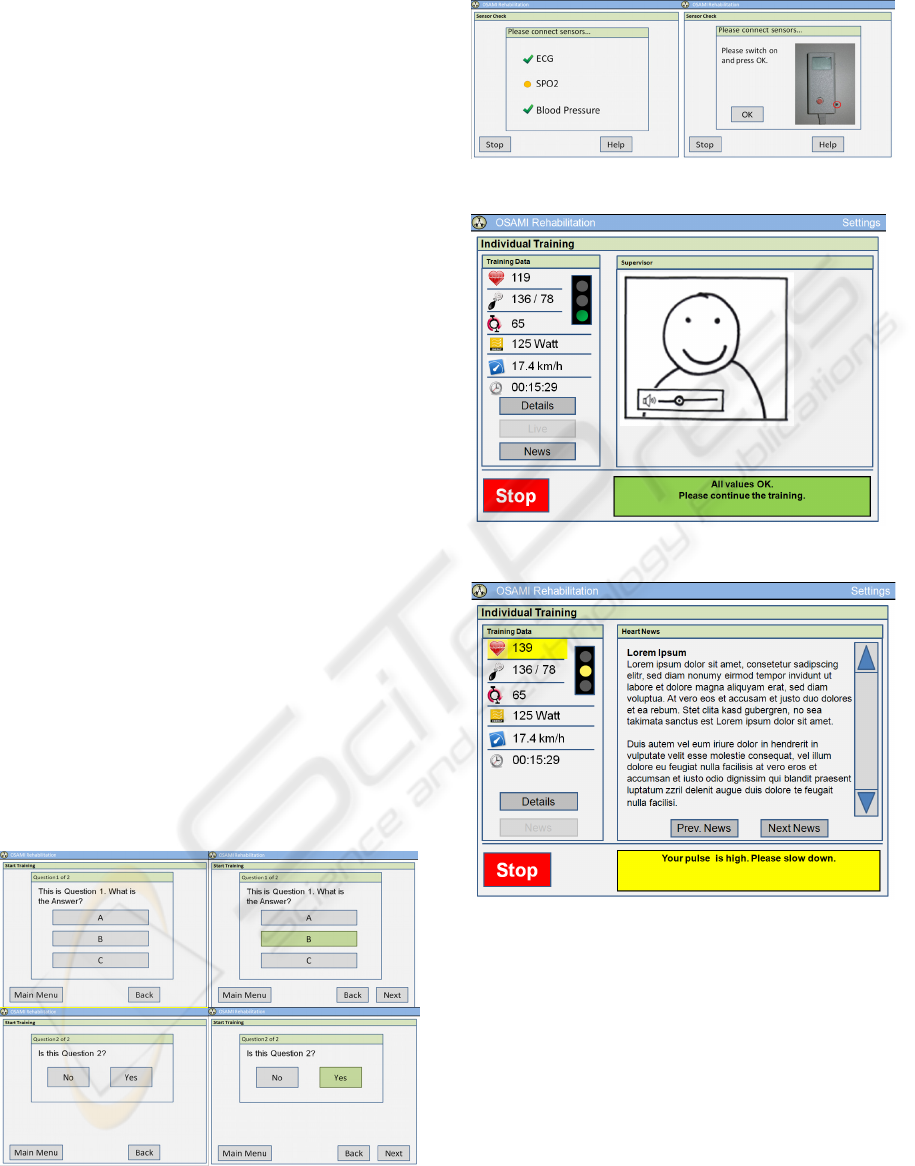
Figure 3 shows how the questions of the pre- and
post questionnaires of Level 3 training should look
like. In the interviews we found out, that the asked
people need feedback about what exactly has been
pressed on the screen. In most cases it is definite
because of the following things that are displayed
but not in case of questionnaires. Even so these are
essential for a supervisor when analyzing the
training in post processing. Therefore we decided to
first highlight a selected answer and then confirm it
by pressing the “Next” button. This was well
accepted by all test users even if they had to click
the screen twice. Figure 3 shows a multiple choice
and a yes/no question. In figure 4 easy signs that
differ in color and shape (therefore also operable by
color-blind people) and that inform a patient about
connected sensors shortly before the training starts.
If a sensor sends a problem or it is not connected the
corresponding help page automatically appears
giving further information and instructions (see
figure 4, right image).
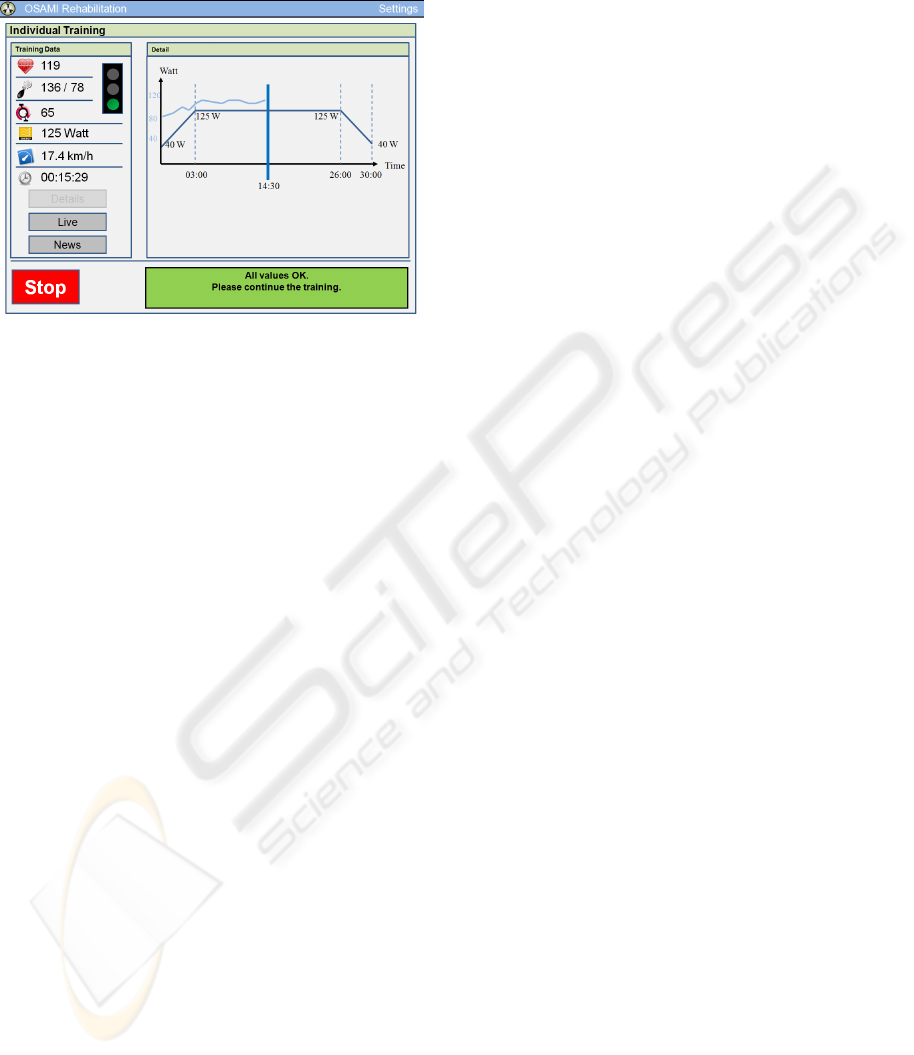
Finally figures 5, 6 and 7 show the user interface
while the patient is exercising. It can be seen that we
decided to use a traffic light metaphor to display the
overall situation, e.g. a green light means that
everything is all right and the training should be
continued. The yellow light means: Continue the
training but additional hints are given (e.g. “Slow
down”). When the red light appears the training will
be stopped after cooling down. Traffic lights can
further on also be understand by color-blind people.
We’re using a unique color scheme in the user
interfaces. Buttons always have the same look &
feel, green, yellow and red colors are used as
described.
Figure 3: Questionnaires.
Figure 4: Sensor check.
Figure 5: Level 1 Training, live view.
Figure 6: Level 3 Training with yellow alarm.
We decided to use easy symbols for the vital data
and the ergometer data to display the heart
frequency, blood pressure value, current pedaling
frequency, load, speed and time. We think that these
icons are easy to understand but we have to verify
this in the next iteration of the user centered design
process.
For the mobile version of the offline training
patients first will have to synchronize their device
with the ergometer. The current training plan is
downloaded to the device and the user can start the
training whenever she wants. Therefore the mobile
system only needs the functionality for starting a
USER CENTERED DESIGN OF PATIENT USER INTERFACES FOR REMOTE TRAINING SUPERVISION - A User
Study
111
training. Alarms during the training will cause in
auditory and physical feedback depending on the
device capabilities.
Figure 7: Level 1 Training, detail view.
5.3 Functional Requirements towards
the System
Even though the user study described above was
done in order to acquire information about the user
interface design for this very special use case, it also
raised functional requirements towards the
underlying software. First we found out that
videoconferencing is essential in Level 1 and Level 2
training since the main information about a patients
well being can be taken from his body language
(skin color, position, pedaling regularity etc.). Even
though in OSAMI-D it was planned to implement
videoconferencing at the very beginning because of
its technical feasibility we found out that it is very
desirable for both user groups – patients and
supervisors.
Automatic analysis of the vital data values is another
requirement. Some kind of data may be analyzed
quite easy (e.g. if the blood pressure value is too
high), some analysis is really hard to implement (e.g.
detect abnormalities in the ECG curve). Here third
party solutions have to be obtained and implemented
in the future.
Another functional requirement is the
entertainment system. It may help to motivate the
patients to exercise periodically and it may help to
overcome the monotony of indoor ergometer
training. Here also a mobile solution is desirable
because it enables patients to exercise outdoor and
she’s not longer limited to cycling. Therefore the
system has to offer possibilities to synchronize
mobile phones with the home gateway (in our
current setup this is the tablet PC on the ergometer)
in order to exchange training schedules and reports.
Patients prefer to have a flexible possibility of
making training appointments. Here the calendar
functionality is a nice feature that enables an
overview of training dates, the different training
levels that are available and past training events.
Since the hardware of the ergometer itself
(saddle position and material, overall weight) is not
changeable (we’re using an existing ergometer setup
in the project) we could not consider comments
regarding these values.
6 CONCLUSIONS
We found out that ergometer training competes to
more attractive physical activities like outdoor
sports. It is therefore extremely important to
generate and keep up a high motivation of patients.
Therefore the vital data of the patients should not
longer be hidden but presented to them during
training. This enables patients to compare values
with previous sessions and allows them to keep an
eye on the overall training success.
Regular feedback from supervisors further on
helps to motivate patients and gives them a feeling
of safety. This is a unique feature of a remote
supervision system. Another issue is that patients
need flexibility in organizing their free time. E-
Health systems should therefore allow them to
exercise whenever they want and wherever they like.
Patient user interfaces should guide the users fast
and intuitively. Patients don’t like an overhead of
time or frustrating questions that occur every time
they start the training. Anyway some hints from the
interviewed patients could not be considered
because they would collide with the medical
functionality of the system. E.g. patients would like
to sail elevation profiles or change the load of the
ergometer on their own.
To summarize this work: We found out
interesting insights about the needs and habits of
patients with cardiac diseases if they would decide
to participate in a remote exercise supervision
program. This helped us to design user interface
mockups and a first software prototype that provide
easy interaction, clarity and overall usability. We
also figured out several insights about this kind of
medical assistance, the problems that have to be
solved and the market potential.
HEALTHINF 2010 - International Conference on Health Informatics
112

7 FUTURE WORK
As the next step of the user centered design process
we will again present this application to patients and
staff of a rehabilitation clinic and do semi-structured
interviews during and after testing. Hopefully this
will result in some hints for refinement that are
going to be used for the final demonstrator
afterwards. The focus of the user tests will lie on
understandability and perceptibility of what’s being
presented. Further on interaction methods and menu
navigations have to be evaluated. The overall goal is
hence still to keep the user integrated during the
whole development process.
REFERENCES
Stroetmann, K. A., Jones, T., Dobrev, A. and Stroetmann,
V.N., 2007. An evaluation of the economic impact of
ten European e-health applications. Journal of
Telemedicine and Telecare
Heise online, 2008 I. Medica: Megatrend Ambient
Assisted Living, http://www.heise.de/newsticker/
Medica-Megatrend-Ambient-Assisted-Living-meldung/
119306
EUROASPIRE I and II Group, et al., 2001. Clinical reality
of coronary prevention guidelines: a comparison of
EUROASPIRE I and II in nine countries. Lancet.
EUROASPIRE II Study Group, 2001. Lifestyle and risk
factor management and use of drug therapies in
coronary patients from 15 countries; principal results
from EUROASPIRE II Euro Heart Survey
Programme. European Heart Journal
Busch, C., Baumbach, C., Willemsen, D., Nee, O., Gorath,
T., Hein, A. and Scheffold, T., 2009. Supervised
training with wireless monitoring of ECG, blood
pressure and oxygen-saturation in cardiac patients,
Journal of Telemedicine and Telecare, Vol. 15
Klompmaker, F., Nebe, K., Busch, C. and Willemsen, D.,
2009. Designing Context Aware User Interfaces for
Online Exercise Training Supervision, Proceedings of
the 2
nd
international Conference on Human System
Interaction
Gay, V. and Leijdekkers, P., 2007. A Health Monitoring
System Using Smart Phones and Wearable Sensors,
International Journal of ARM, Vol. 8, No.
Oppermann, R. and Lorenz, R.. 2008, Seniorengerechte
Gestaltung eines Dienstes zur mobilen Überwachung
von Gesundheitsparametern, Bundesministerium für
Bildung und Forschung -BMBF-: Ambient
AssistedLiving. 1. Deutscher Kongress mit Ausstellung
Wengraf, T., 2001. Qualitative Research Interviewing:
Biographic Narrative and Semi-structured Method,
Sage: London
Heise online, 2008 II. Ambient Assisted Living: IT-
Technik fürs Alter, http://www.heise.de/newsticker/
Ambient-Assisted-Living-IT-Technikfuers-Alter-
meldung/137183
USER CENTERED DESIGN OF PATIENT USER INTERFACES FOR REMOTE TRAINING SUPERVISION - A User
Study
113
