
A PORTAL FRAMEWORK ARCHITECTURE FOR BUILDING
HEALTHCARE WEB-BASED APPLICATIONS
Francois Andry, Erik-Paul Gibson, Goutham Naval, Thomas Odenwald, Ben Vigil, Frank Yu
InterComponentWare Inc., 1820 Gateway Drive - Suite 300, San Mateo, CA 94404, U.S.A
Karsten Klein
InterComponentWare AG., Industriestraße 41, 69190 Walldorf, Germany
Keywords: Portal, Portlets, SOA, Security, Context Management, PHR, EHR, Care Disease Management,
Personalization.
Abstract: Portals are Web-based applications that give users a centralized point of access for information and
applications of relevance. Therefore the portal paradigm is an attractive proposition for healthcare because it
offers a solution to rapidly aggregate heterogeneous applications and services while offering a high level of
customization and personalization to the users, patients, care givers and IT personnel. In this paper, we
explain the motivations that led us to integrate a portal framework on top of our solution stack to create
healthcare solutions for our partners and customers. We describe the challenges associated with this type of
infrastructure for healthcare applications including security and context management. We present concrete
solutions for specific portal applications integrating EHR, PHR, care and disease management
functionalities.
1 INTRODUCTION
The integration of healthcare systems and data is a
major challenge. Business conditions that typically
result in fragmented data stores and limited
application functionality are prominent in the
healthcare industry (DesRoches et al. 2008), (Ashish
et al. 2009).
While other industries are advancing in SOA
principles, the healthcare industry only recently has
started to embrace the concept of service-oriented
architecture (SOA) as a solution (Sartipi, Yarmand
and Down 2007) to integrate heterogeneous and
legacy systems independently from the underlying
platforms or programming languages. The
healthcare industry is looking for ways to process
data stored in the existing silos and offer useful
healthcare services to assist clinicians in making
rapid and accurate decisions while helping to
prevent medical errors and save costs in the process.
To meet these requirements, we envision newer
healthcare services for providing interactive portals
for payers, providers, collaborative care and for
telemonitoring.
However, because not all healthcare systems are
fully modularized or offer complete external service
layers or APIs, there is a need for ways to integrate
functionalities higher in the software stack, closer to
the presentation layer through an architecture that
enables interoperability and integration (Smith
2004).
To meet these challenges, we have created a
Portal framework architecture which makes the SOA
concept less abstract by offering a concrete service
aggregation infrastructure including integration glue
like context and code mapping, transformations,
master patient index, single sign on and standards
based interfaces. The framework facilitates the
integration of various applications, so they need not
be rewritten to be able to provide services to the
portal. Our portal framework is compliant with
industry standards such as JSR 168, JSR 286 and
WSRP (Hazra 2002).
344
Andry F., Gibson E., Naval G., Odenwald T., Vigil B., Yu F. and Klein K. (2010).
A PORTAL FRAMEWORK ARCHITECTURE FOR BUILDING HEALTHCARE WEB-BASED APPLICATIONS.
In Proceedings of the Third International Conference on Health Informatics, pages 344-349
DOI: 10.5220/0002755303440349
Copyright
c
SciTePress

2 ARCHITECTURE BENEFITS
2.1 Front-end Components Aggregation
Information users often use many different systems
and interfaces. The healthcare industry offers a
typical example of this situation. Healthcare IT
systems tend to be deployed in very specific
contexts, like in departments such as labs, radiology,
ER, surgery. The data generated by these systems is
valuable to a range of users who play very different
roles in the healthcare process. The roles these users
play in their jobs are neither reflected in their
systems of choice nor in a single point of access.
Therefore, the ability to create role-based front-
end interfaces is valuable. Role-based concepts are
included in most portal offerings and offer flexible
configuration capabilities for specific targeted sets
of user groups. This is especially important in the
healthcare industry in the United States where the
market is fragmented and requires a lot of product
customization and re-branding. Aggregated in Web
portals, front-end components can be built on top of
existing data structures, enterprise and legacy
systems as well as third-party services (Deora et al.
2006).
Though, focusing solely on market factors as
drivers for front-end flexibility neglects the
underlying challenge facing healthcare software
developers. Not only are users confronted with
multiple, siloed IT systems, they are also affected by
shifting roles and a convergence of IT services made
possible by growing electronic data availability. For
example, physicians have traditionally focused on
diagnosis and treatment, rather than prevention. But
external forces like healthcare reform, Health
Information Exchanges (HIE) and Pay for
Performance (P4P) initiatives are shifting physicians'
concerns. Fortunately, as physicians change their
approach to healthcare new technologies, data and
tools are emerging to aid this transition. These same
tools also lead to expanded roles for other care
givers and a greater opportunity for collaborative
care.
This constant flux of user role definitions and
changing use cases requires exceptionally agile
development. Rapid prototyping and constant
acceptance testing are critical to solving the business
challenges of the healthcare industry. The additional
development flexibility afforded by portals enables
software companies to react more quickly to the
market and to customers needs.
Software portal containers can help software
companies break large software projects down into
smaller more manageable pieces usually referred to
as modules. Such modules can be visualized by
portlets, which can be designed and developed
separately and deployed as they are completed. As a
result, vendors can more quickly develop features
and functions as needed by their customers and
demanded by the marketplace.
2.2 Portal Characteristics
An enterprise horizontal portal is the delivery layer
for a heterogeneous environment (potentially in
healthcare, the complete continuum of care). It
usually includes the following features:
Single Point of Entry: Portal solutions offer a
unified and personalized view for various
healthcare professionals (Koufi et al. 2008),
and provide real-time access to a selected
patients’ clinical information with integrated
single sign-on (SSO) authentication
capabilities;
Permissions: the ability for portal
administrators to limit specific types of
content and services to groups of users based
on their respective roles and profiles;
Integration: the aggregation of data and
services from multiple systems including
generic content, knowledge management and
collaboration components into visual front-
end fragments or portlets;
Federation: the combination of content from
various sources;
Enhanced User Experience: an efficient and
consistent user interface (even though the
underlying services can come from multiple
sources);
Personalization: the ability for users to
choose specific services and content tailored
to their need and to customize the layout and
look and feel of their presentation layer.
2.3 Benefits to the Healthcare IT
Delivery Network
A portal approach can bring benefits to the whole
healthcare IT delivery network:
Benefits to the End-users: The portal
application represents a single point of access
to perform important healthcare tasks through
a very convenient “dashboard” paradigm.
Portal solutions also present a rich user
experience by leveraging Web 2.0
technologies (Phifer, Gootzit and Valdes
2008) and specific components (e.g. wikis,
A PORTAL FRAMEWORK ARCHITECTURE FOR BUILDING HEALTHCARE WEB-BASED APPLICATIONS
345

blogs, message boards, social networking,
maps etc). Portal customization and
personalization also offers end-users a more
personalized experience based on their
profiles such as their role in the organization
or user group and preferences (e.g. choice of
layout, look and feel, medical content);
Benefits for the Development Team: This
includes a common architecture for the
aggregation of heterogeneous components and
services, a clear separation between the
presentation layer and the service layer, and
the fact that portlets are based on standard
technologies (e.g. JSP. JSF, Spring, Hibernate,
JSR 168, JSR 286, WSRP, AJAX, Java EE, or
even Adobe Flex). We have also developed
reusable GUI components using JSF
framework and portlet templates;
Benefits for the Professional Service Team:
Portal technology can save substantial costs to
the professional service team tasked with
creating solutions. A portal approach that
includes the ability to create and combine
customized components that are easily
customizable and re-branded for customers
offers a good return on investment (ROI);
Reduce TCO (Total Cost of Ownership):
For the healthcare IT departments deploying
and maintaining services and applications, the
ability to run multiple portal sites, each with a
unique domain, on the same portal server
reduces the duplication of hardware and image
instances. Portlets can be deployed at run-time
(hot deployment) reducing down time for the
user, facilitating the maintenance of the
applications and increasing the overall quality
of service (QoS). In addition, specific content,
branding, layout and skins can be stored and
managed independently of the application in a
content management system, saving costs
during deployment and maintenance.
2.4 Standardization Benefits
Over the years there have been a lot of
standardization efforts (HL7, ISO, Continua, HITSP,
IHE) in the healthcare industry, especially in the
area of interoperability. Horizontal enterprise portals
can take advantage of these standards as a safe and
reliable means to communicate between the different
healthcare systems.
Horizontal enterprise portal servers themselves
have been used successfully for more than a decade
in various fields. As a result open source solutions
and standards have emerged (JSR 168/286, WSRP
that can be leveraged for healthcare portal
applications as well (Gootzit and Valdes 2008).
These standards define the basic behaviors of the
container, the lifecycle management of the portlets,
security, coordination between portlets,
communication protocol between a portal
application and remote portlets, packaging and
deployment of portal applications.
2.5 Enriching the Existing Standards
JSR 168 & JSR 286 standards are useful for building
relatively simple portlets. However, because today’s
users have come to expect responsive and fluid
interactions in Web based applications, the basic call
and response model of the portal server (including
systematic refresh of whole Web pages) is not
sufficient.
Popular Rich Internet Application (RIA)
technologies include AJAX (Asynchronous
JavaScript and XML), Adobe ActionScript/Flex and
Microsoft Silverlight. These technologies, which are
not part of the JSR portlet specifications, need to be
combined with portal frameworks to create modern,
interactive Graphic User Interfaces (GUI).
The solution is to build the basic functionality
based on the JSR portlet standards and then extend
the user interfaces using more advanced RIA
technologies (Phifer, Gootzit and Valdes 208). This
will allow for easy (but not seamless) portability
between popular portal containers while delivering a
modern user experience.
3 FRAMEWORK USE CASES
For the past couple of years we have collected
requirements for Healthcare Web Applications from
a number of sources: requests for information (RFI),
requests for proposals (RFP) and direct discussions
with our customers. In these requirements, portal
architecture is mentioned more and more frequently
because portals are viewed as a solution to some of
the fundamental healthcare IT challenges—siloed
systems as well as the convergence of healthcare
services.
Table 1: Requests for proposal with portal requirements.
Request for Proposals Date
Texas Medicaid Administrative
Claiming (MAC)
2009
Kentuky Health Information Exchange 2009
Ontario Diabetes Registry 2008
HEALTHINF 2010 - International Conference on Health Informatics
346

In Texas, stakeholders see portals as a solution to the
traditional problem of merging data from disparate
systems to provide an aggregate view into a patient's
status. Both Kentucky and Ontario are looking to
solve similar challenges, but they are also using the
unification of data as a driver to expand available
healthcare IT services.
For example, in the recent Ontario Diabetes
Registry RFI, the portal application includes
electronic medical record (EMR) functionalities as
well as other services like real-time vital signs
(through device integration), e-Prescribing, doctor to
patient communication, clinical guidelines, alerts
and task management. The goal of this project is not
only to solve the problem of decentralized data, but
also to support the possibilities that IT holds for
advancing healthcare delivery.
4 ARCHITECTURE DETAILS
4.1 Front-end Aggregation Layer
Our product suite was developed according to a
specific set of use cases with particular user profiles.
What we discovered through market research that
features that were intended to be consumed by a
particular user actually had relevance to other users
in the care process.
To address this type of requirement, we had to
integrate some of our existing products (Andry et al.
2008), (Andry et al. 2009) such as our Personal
Health Record solution, our Professional Exchange
Suite (PXS) in the form of our EHR (Electronic
Health Record) and CDM (Care and Disease
Management) solution, as well as third-party
components. Some components are directly
integrated at the service layer through our
integration platform (IPF) that is part of our eHealth
Framework (eHF).
The visual components (portlets) are integrated
in a lightweight front-end layer “Fig. 2”, which in
our case is a horizontal enterprise portal framework
layer. Alternative architectures include widgets/
gadgets based portals (Gootzit and Valdes 2008),
(Gootzit 2008) and mashup frameworks.
4.2 Context Management Layer
In addition to the front-end aggregation layer, a
context management layer which uses a subset of the
concepts of the HL7 Clinical Context Object
Workgroup (CCOW) standard (centralized scheme,
robust push-model, simplified context data
representation) is used to solve user mapping and
facilitate the coordination and synchronization
between visual components (portlets in our case).
This context management layer connects to the Web
services (SOAP or RESTfull) that are exposed by
the different products or in certain cases a software
development kit (SDK) which encapsulates the Web
services in functions (java or .NET) that are easier to
use.
Table 2: Components of an EHR Light Portal.
Service/portlet Product/provider
Patient Finder PXS
Patient Demographic Data PXS
Patient Medical Record PXS
Task List CDM
Medical observations LS
E-prescribing 3rd party
Figure 1: ICW Health Portal Framework Architecture.
4.2.1 Sessions and Contexts
A portal application like any other web application
works with a session. All requests are executed in
the context of such session. The session is associated
with an authentication context and a lot of other
information that is accumulated while processing the
requests that are executed with the session. A
session can be understood as a temporary storage
with a well-defined life cycle. A session is ended
either explicitly (log out, connection closing) or by a
time-out.
In the meta-model below (Fig. 2), we describe
the basic relationship between the sessions and other
relevant information.
When accessing the web application for the first
time there is no session established yet. The user is
forced to log in (providing his identity and the
credentials to prove the identity). This establishes an
authentication context which is kept within a
dedicated session. During the requests executed in a
A PORTAL FRAMEWORK ARCHITECTURE FOR BUILDING HEALTHCARE WEB-BASED APPLICATIONS
347
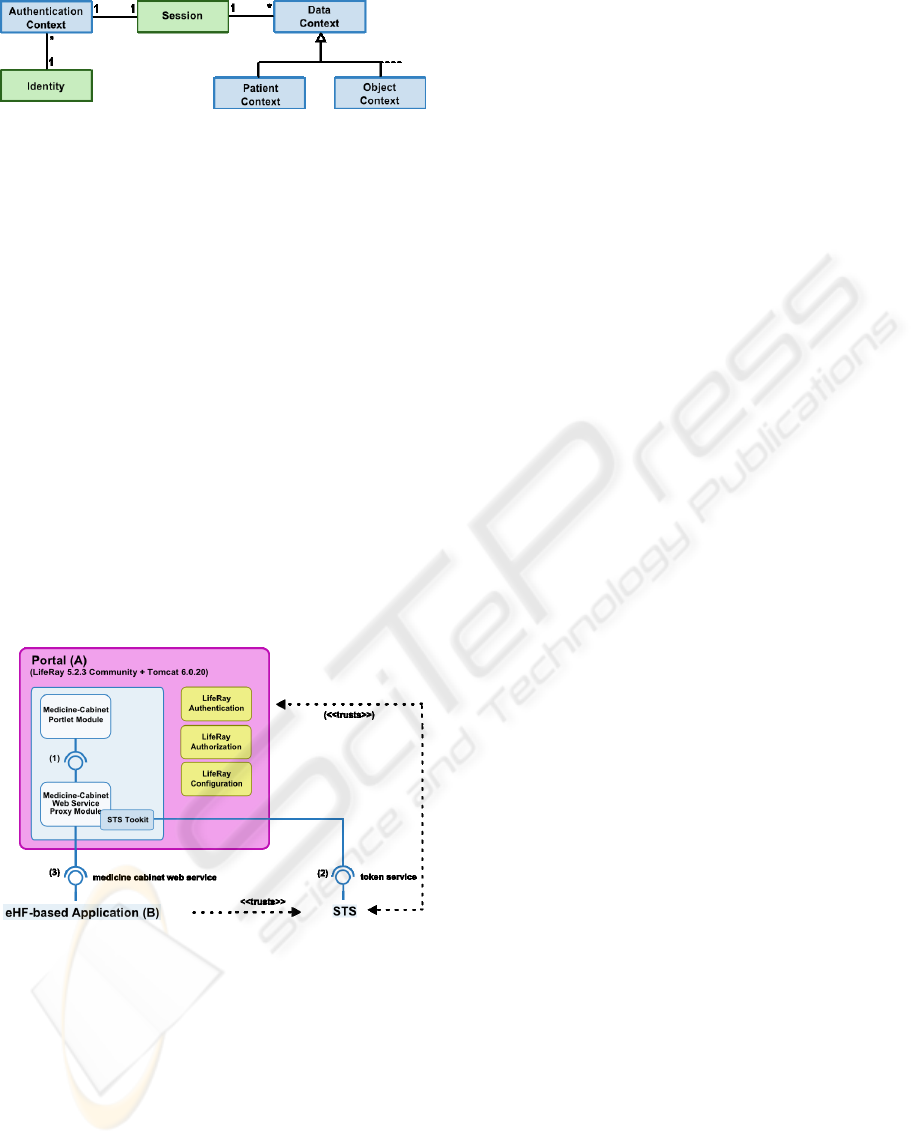
Figure 2: Meta-model connecting session and context
objects.
session, information is accumulated and processed in
the session. This kind of information is generalized
as data context with different specializations such as
context information for patient or any other
healthcare domain objects.
5 DEPLOYMENT SCENARIO
5.1 Simple Portlet Integration
In the most simple deployment use case (see fig.3)
the portal framework is used to create and deploy a
portlet (e.g. a medicine cabinet) that is hosted in a
portal container (A). The portlet uses a proxy
module that has access to remote eHF-based
Application (B) including the Medicine Cabinet
Service Module, which exposes the required web
remote interface (e.g. a RESTful web service).
Figure 3: Portal deployment use case.
5.2 Connecting the Services
Both the portal application (A) and the remote
system (B) may have their own identity management
capabilities and their own credential storage. In
order to integrate A and B we have implemented an
extended SAML based token service. The resulting
Security Token Service (STS) service includes the
token service module as well as an eHF based
context management module. This eHF Context
Module stores the mapping information between
user identifiers from A and the identities of B as
described in Figure 2.
The token service toolkit provides utilities to create,
renew and request tokens. In particular it is possible
to request a token for B based on a token from A.
The resulting token B must of course include a
mapped user identifier and assertions valid for B.
5.3 More complex Scenarios
In reality, portal applications typically consist of
multiple portlets that interact together. Each portlet
can themselves aggregate services from various
sources. This is where the portlet proxy is very
handy because it can shield the presentation layer
from back-end service implementation details.
The integration of a new application exposing
web services (SOAP or RESTful) is made easier
because eHF provides a mediation and routing
platform component (IPF) based on Apache Camel
that can wrap these services, operate transformations
on data and expose them to the portlet proxies. In
addition to this the current use of the Security Token
Service for authentication can be complemented by
the use of a Single Sign On (SSO) mechanism.
6 CONCLUSIONS
Our portal framework architecture provides
healthcare application developers a set of open
source components based on standards, tools,
methods and processes to create more complex
integrated and context-aware portal applications
covering the full continuum of care for professional
care givers and patients. Our framework offers high
security, privacy, performance and scalability
compliant with government regulations such as
HIPAA.
In the next milestones of this project we will
focus on portal usability, inter-portlet
communication, quality assurance and lifecycle best
practices, providing the users of our framework
guidelines, blueprints and sample healthcare portlets,
themes, content, as well as business perspective
material (licensing, support and revenue models)
related to the use of the framework.
ACKNOWLEDGEMENTS
We are extremely grateful to John Gillson, Liliya
Gor¸ Juergen Groothues, Andreas Kaltenbach, Igor
HEALTHINF 2010 - International Conference on Health Informatics
348

Kosoy, Salim Kizaraly, Lucy Lin, Dimiter Makariev
and Dirk Wippermueller for their help. Thank you
also to Rostislav Georgiev and the UICC team for
their JSF/UI library contribution. Our appreciation to
Richard Golden, Matthias Laux, Thomas Liebscher
and the ICW architecture board members for their
feedback on this project.
REFERENCES
Andry, L. Freeman, Gillson J., Kienitz K., Lee M., Naval
G., Nicholson D., 2008, “Highly-Interactive and User-
Friendly Web Application for People with Diabetes”,
IEEE 10th International Conference on e-Health
Networking, Application & Services (HealthCom 08),
pp. 118-120, Singapore, July 2008.
Andry F., Naval G., Nicholson D., Lee M., Kosoy I. and
Puzankov L., 2009, “Data Visualization in a Personal
Health Record Using Rich Internet Application
Graphic Components”, 2nd International Conference
on Health Informatics (HealthINF 09), pp. 111-116,
Porto, January 2009.
Ashish K. et al., "Use of Electronic Health Records in U.S.
Hospitals", The New England Journal of Medicine,
Volume 360:1628-1638, Number 16, April 2009.
Deora V., Contes A., Rana O., Rajbhandari S., Wootten
L., Tamas T. and Varga L., 2006, “Navigating
Provenance Information for Distributed Healthcare
Management”, IEEE/WIC/ACM International
Conference on Web Intelligence, 2006, pp. 859-865.
DesRoches C. et al., 2008, "Electronic Health Records in
Ambulatory Care — A National Survey of Physicians",
The New England Journal of Medicine, Volume
359:50-60, Number 1, July 2008.
Gootzit D., 2008, “Second-Generation Portlet Standards
Should Be Used for Portlet Development but Aren't the
Whole Story”, Gartner Reports, ID Number:
G00163990, December 2008.
Gootzit D., Valdes R., 2008, “Open Source and Portals”,
Gartner Reports, ID Number: G00156161, April 2008.
Gootzit D., 2009, “Get Ready for the ‘Portal-Less’ Portal,
Gartner Reports”, ID Number: G00166378, March
2009.
Hazra T., 2002, “Building Enterprise Portals: Principles
to Practice”, Proceedings of the 24th International
Conference on Software Engineering, pp. 623-633,
Orlando, Florida, 2002.
Koufi V., Malamateniou F. and Vassilacopoulos G., 2008,
“A Medical Diagnostic and Treatment Advice System
for the Provision of Home Care” Proceedings of the
1st international conference on Pervasive
Technologies Related to Assistive Environments -
PETRA'08, July 15-19, 2008, Athens, Greece.
eHF - eHealth Framework, http://idn.icw-global.com/.
Phifer G., Gootzit D., Valdes R., 2008, “Generation Six
Portal Products: When Portals Meet Web 2.0, It's
Love at First Sight” Gartner Reports, ID Number:
G00166723, March 2008.
Sartipi K., Yarmand M., and Down D., 2007, “Mined-
knowledge and Decision Support Services in
Electronic Health” International Workshop on
Systems Development in SOA Environments
(SDSOA'07), 2007.
Smith M., “Portals: Towards an Application Framework
for Interoperability”. Communications of the ACM,
Volume 47, Issue 10, 2004, pp. 93-97.
A PORTAL FRAMEWORK ARCHITECTURE FOR BUILDING HEALTHCARE WEB-BASED APPLICATIONS
349
