
SMART MEDICAL SOFTWARE SYSTEMS FOR DUMMIES?
The Case for a User-centered Systems Design
Detlef Zuehlke, Gerrit Meixner
German Research Center for Artificial Intelligence (DFKI), Trippstadter Strasse 112, Kaiserslautern, Germany
Ulrike Klein
University of Heidelberg, Department of Internal Medicine, Hematology/Oncology
Im Neuenheimer Feld 410, Heidelberg, Germany
Keywords: Human-Computer Interaction in Health Care, User-centered Development, Usability of Medical
Information Systems.
Abstract: In this position paper we ask the question of whether current medical software systems adequately support
the “dumb users” in their routine work, or whether the software systems are rather function-oriented and
their development far removed from reality. In a multi-year study, the medical faculty of the University of
Heidelberg and the German Research Center for Artificial Intelligence (DFKI) cooperated on a review of
the current situation in medical software systems. The first project involved the joint development of a
prototype of a user-centered software system for the allogeneic stem cell transplantation procedure.
Additionally, a comprehensive survey was conducted among the medical staff of the Hematology and
Oncology Department at the Heidelberg University Clinic. The results of both the project and the survey are
presented here.
1 INTRODUCTION
When we look at the situation today in the area of
clinical IT systems, we can find major advances in
the performance capacities of modern software
systems, but must also note their rapid penetration
into almost every facet of the daily clinical routine.
A myriad of very good software products now exists
for patient administration, resource management,
personal data administration, drug prescriptions, and
many other activities, all of which have proven their
worth in numerous clinics.
Surveys among clinical staffs have shown,
however, that the operation of the software systems
has very little to do with the actual tasks performed
by the operator. Developers have a different way of
looking at the systems than do the future users who,
in their work, must frequently use several different
systems, each supplied by a different manufacturer,
in parallel in order to complete their tasks (cf.
Nielsen, 2005). In the event of a problem or when
the user rejects the software support system, it is
often all too easy to put the blame on the “dumb”
user. The situation is briefly introduced in the
following example.
2 SMART TRANSPLANTATION
The aim of the Smart Transplantation Project was to
determine how software systems could provide more
efficient support to medical personnel (physicians,
caregivers, transplant-coordinators) during complex
medical procedures (Meixner, Thiels and Klein,
2007). To this end, in 2007 the authors conducted a
situational analysis into the subject of software
support for allogeneic stem cell transplantation (one
of the most complex medical procedures) at the
Heidelberg University Clinic. In a comprehensive
study, user requirements, relevant data requirements,
work processes, etc. were examined by means of
observation and expert interviews. In the process, a
series of significant findings were observed.
Notably, we found that members of the medical
staff must make safe and proper decisions,
effectively and efficiently even when
350
Zuehlke D., Meixner G. and Klein U. (2010).
SMART MEDICAL SOFTWARE SYSTEMS FOR DUMMIES? - The Case for a User-centered Systems Design.
In Proceedings of the Third International Conference on Health Informatics, pages 350-354
DOI: 10.5220/0002756303500354
Copyright
c
SciTePress
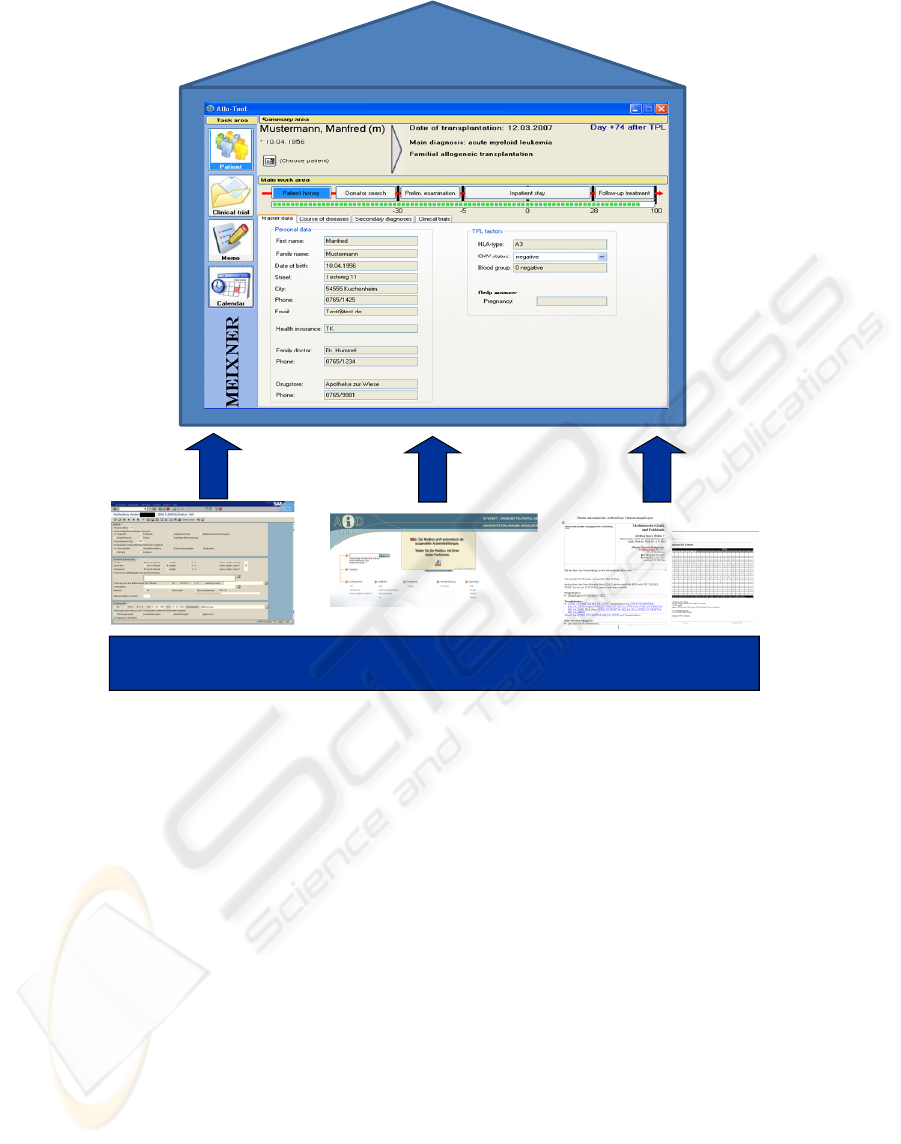
existinginformationsources
(ISH,AiD,paperetc .)
Allogeneictool
Figure 1: Integration of various information sources into the task-centered allogeneic tool.
performing under time pressure (stress). Other
aspects like the simple and intuitive use of the
operational interface (usability) or joy-of-use
(hedonics) are of equal importance.
An initial prototype was then developed with the
aims of providing optimal support to the medical
staff throughout the complete workflow of
allogeneic stem cell transplantation and integrating
the various existing IT-systems, for example, paper
based files, hospital and drug information systems
into one application (see figure 1). A previous
analysis of tasks revealed a software system that
included the following functionalities: extraction of
medical data from several different sources,
structured presentation of processed information,
and automated generation of medical documents
such as physician’s letters or pharmaceutical plans.
Furthermore, the procedure for allogeneic stem
cell transplantation was broken down into a 5-
phased treatment plan and placed onto a timeline.
The different information needs in each of the
individual phases (patient history, donator search,
preliminary examination, inpatient stay and follow-
up treatment), had to be presented according to the
respective needs of the various users. This task-
centered approach resulted in efficient search and
documentation of information and, in this way,
provided some relief to the medical staff. In
addition, the operational interface was adapted to the
needs of the respective users with various screens
developed on the basis of user groups.
Prototypes designed on the basis of the findings
in the Smart Transplantation project revealed
problems, for example, the time consuming
searches, the redundant data entries, or the use of
different software to perform the various tasks,
which could be significantly reduced by the
introduction of an integrated software system.
This project was limited in scope to one complex
medical procedure. The overall situation pertinent to
software support of medical professionals within one
department of a major healthcare clinic was
investigated by the follow-on survey.
SMART MEDICAL SOFTWARE SYSTEMS FOR DUMMIES? - The Case for a User-centered Systems Design
351

3 CLINICAL SURVEY
More than 30 staff members of the Department of
Hematology and Oncology at the Heidelberg
University Clinic participated in an online survey
which asked about various areas of application of
Information and Communications technologies
(ICT) within the hospital. 94% of those asked
responded that IT applications are critical to the
daily routine at the clinic and 90% said more than
50% of their work involves the use of computers;
58% even reported more than 75%. Important
criteria for the respondents was not only a timely
system response but also that the system be efficient
and user friendly. The responses were ambivalent
concerning the current state of integration of the IT
applications in the daily work routines. No clear
conclusions can be drawn - positive or negative –
from these answers. However, when we evaluate the
responses in terms of the question about IT systems
optimization, the dominant answers mention, besides
the timeliness, the integration of the different
individual applications into one system and the
elimination of redundant data entries. The analysis
of the individual systems used in this job area
showed major deficits in usability and effectiveness,
especially in the accounting and technically oriented
administrative applications. The assignment of
responsibility for specific functions was analyzed in
terms of the professional medical staff and the IT
applications. The functions assigned to the computer
systems were: the logistics, the processing of
previously selected data as well as the
recommendation of appropriate diagnosis and
therapy. The actual selection of patient data and the
decision making for diagnosis and therapy were
assigned without exception within the sphere of
responsibility of medical professionals. Another
subject area in the survey solicited attitudes about
decision support systems. 82% of those asked
reported no knowledge or, only a vague idea of what
the term means. After a brief clarification,
respondents were asked to comment about the uses
and benefits, the reliability, the prospect of success,
and the acceptance of decision support systems.
While the benefits were generally given a high
rating, the reliability and acceptance were rated
rather low. Nevertheless, 60% said they would
follow the recommendations of the decision support
system.
Overall, the findings of the survey show IT
technology in hospitals has attained an important
status and with the optimization of the software
structures, tasks and processes can become more
efficient, quality can be improved, and performance
stress can be reduced (time pressures). The concern
that computers will replace the professional staff
seems to have retreated in the face of the view that
IT solutions can effectively support and simplify
their work.
4 CONCLUSIONS
The contemporary leading IT applications for
hospital information services and, by extension, the
major patient data administration applications are,
with some exceptions, oriented for historical reasons
on business and accounting theory. This not only
makes them quite user-unfriendly, fairly inefficient
for a clinical environment, but also dangerous
(Nielsen, 2005; Koppel et al., 2005). At the same
time, the users recognize their dependence on
computer systems in their daily clinical routines and
criticize the inadequate level of integration among
the individual systems and the resulting need for
redundancy, poor functionality, and deficits in data
presentation. These smart systems may be brilliantly
programmed, but they go right around the actual
requirements of the various user groups found in
hospital operations. For example, some feature that a
business accountant appreciates may be totally
useless for the doctor. The issue is not the ignorance
of the user but rather, the historical development of
hospital software and the apparent lack of interest in
developing software that would satisfy the everyday
job needs of a nurse or an internist. Among this
group, the longstanding opinion that computers
would disrupt the clinical activities has been
replaced by the desire for IT systems that support
their work through integration, efficiency, and
appealing presentation of important data. The user
community today brings a readiness to use the wide
range of opportunities made possible by computers.
They are by no means dumb or unwilling, but they
simply must rely on IT concepts that, to be of any
use in practice, must be tailored to their needs. We
saw this, for example, in the willingness to use
decision support systems and not categorically reject
them; and, again in the re-assignment of some
responsibilities from the medical staff to the
intelligent software solutions. The potential is great
in daily healthcare routines for IT solutions that
isolated applications will never be able to satisfy.
Much more, it will require integrative,
comprehensive, and user friendly software products.
HEALTHINF 2010 - International Conference on Health Informatics
352
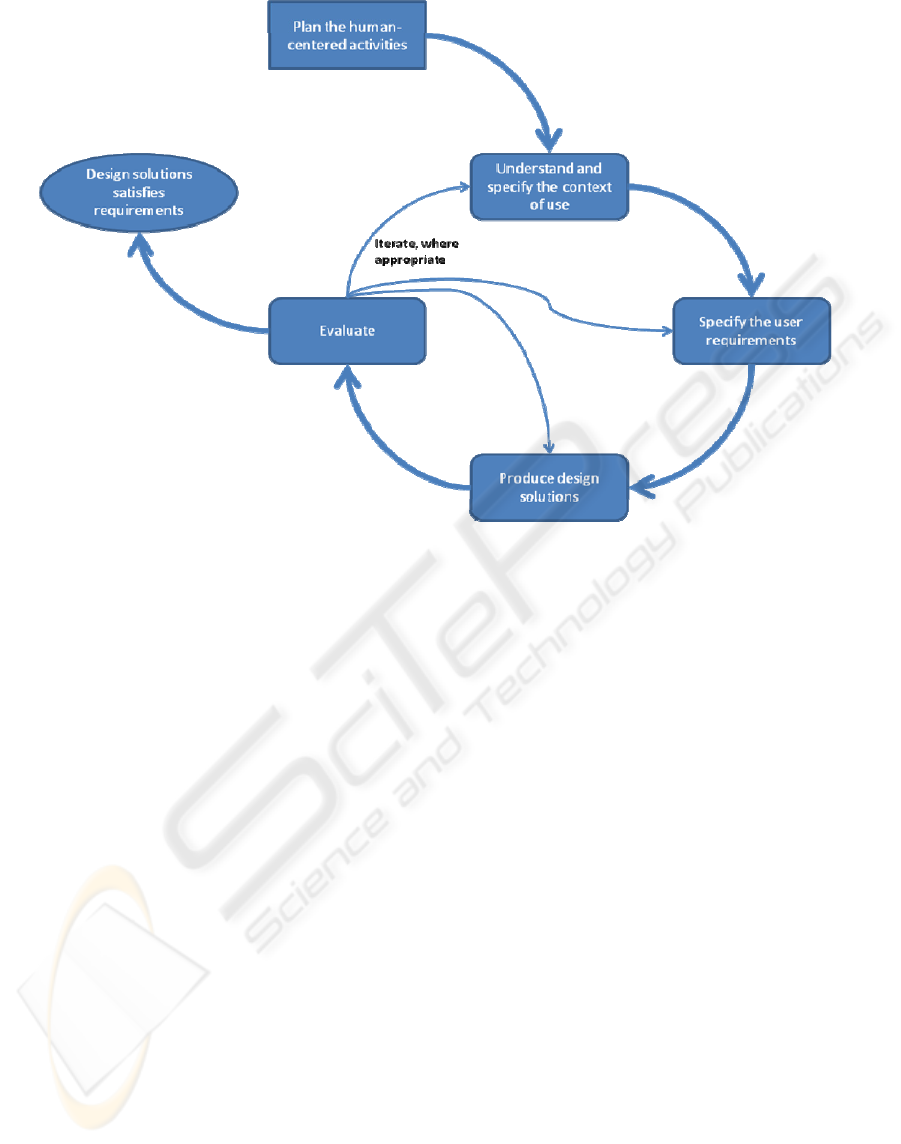
Figure 2: The interdependence of human-centered design activities (ISO, 2009).
One possible solution lies in user-centered
interface design which has long been a decisive
factor in the acceptance of new software. However,
in the fields of healthcare and medicine this
development still presents an enormous challenge.
Truly user friendly operational interface designs can
only be assured under a systematic development
process (Zuehlke and Thiels, 2008).
A user-centered development process is broken
down into several iterative phases (see figure 2).
Beginning with the user and context analyses,
requirements are defined for the operational
interface, implemented in (visual) prototypes, and
then tested and evaluated by current and future users
(ISO, 2009). Especially the evaluation of visual
prototypes is important, because prototyping and
testing can focus on specific improvements in
metaphors, mental models, navigation, interaction,
and appearance (Marcus et al., 2000).
None of these phases may be pursued in
isolation, but rather, they should be seen as
overlapping. The focus during the analysis phase is
on the users (e.g., doctors and caregivers), their
tasks, and their work environment. Several different
methods such as surveys, observations, or
questionnaires are used to identify and develop a
comprehensive list of requirements (cf. (Holzinger,
2005)). A parallel evaluation, for example,
employing structural, paper, or functional
prototypes, allows users to be integrated directly into
the test and evaluation process of the development
concept.
It is especially important to convince
manufacturers, developers, and buyers of the user-
centered development approach. The benefits are
already clear and include time and cost savings,
improved software quality and greater user
satisfaction. The successful application of user-
centered development processes for operational
interfaces in medical field has already been
demonstrated, for example, in (Meixner et al., 2008).
A key problem is still whether the users of
medical software systems are simply not smart
enough (PEBKAC: Problem Exists Between
Keyboard and Chair) to operate the systems
correctly and efficiently or, perhaps, whether the
software systems are simply inadequate, not user-
centered and, to this extent, the product of intelligent
development. In the future, the development of
medical software systems will no longer be oriented
on technology and business accounting, but will
focus more on the actual users and user support in
the daily clinical routines.
In this respect, there must also be a serious
review of the myriad of different isolated
applications and special system solutions in the
medical field. An appropriate standard for the
development of graphic displays based on a generic
SMART MEDICAL SOFTWARE SYSTEMS FOR DUMMIES? - The Case for a User-centered Systems Design
353

operational interface would be a major step towards
a standard solution. This would facilitate integration
of existing expert systems under a common
operational interface. The main benefit of such a
(platform independent) standard user interface
description language for medical software systems
(e.g. developed as a XML-language) would be the
easy adaption to specific constraints and conditions.
There would be no need for using different graphical
widget libraries – just one standard which could also
be automatically transformed into specific final user
interfaces (e.g. source code). Successful Examples
of such languages in computer science are the User
Interface Markup Language (UIML) (Ali, Pérez-
Quiñones and Abrams 2004) and the eXtensible
Interface Markup Language (XIML) (Puerta and
Eisenstein 2002).
ACKNOWLEDGEMENTS
This work was funded (in part) by the German
Federal Ministry of Education and Research under
grant number 01 IS 09027 C. The responsibility for
the content of this publication lies with the authors.
REFERENCES
Ali, M. F.; Pérez-Quiñones, M. A.; Abrams, M., 2004:
Building Multiplatform User Interfaces With UIML.
In: Multiple User Interfaces – Cross-Platform
Applications and Context-Aware Interfaces, pp.95-
118, John Wiley & Sons.
Holzinger, A., 2005: Usability Engineering for Software
Developers. Communications of the ACM, 48(1),
pp.71-74, ACM.
ISO, 2009: ISO/DIS 9241-210: Ergonomics of human-
system interaction - Part 210: Human-centered design
for interactive systems.
Koppel, R. et al., 2005: Role of Computerized Physician
Order Entry Systems in Facilitating Medication Errors,
In: Journal of the American Medical Association,
293(10), pp. 1197-1203.
Marcus, A. et al., 2000: User-Interface Design for Medical
Informatics: A Case Study of Kaiser Permanente. In:
Proceedings of the 33
rd
Hawaii International
Conference on System Sciences, HICSS 2000, Maui,
USA, IEEE Computer Society.
Meixner, G., Thiels, N., Klein, U., 2007:
SmartTransplantation - Allogeneic Stem Cell
Transplantation as a Model for a Medical Expert
System. In: Proceedings of the 3
rd
Symposiumon HCI
and Usability for Medicine and Health Care, USAB
2007, Graz, Austria, pp. 303-314, Springer.
Meixner, G. et al., 2008. Smart Transplantation - Fever of
Unknown Origin after Stem Cell Transplantation as a
Model for a Knowledge-Based Decision Support
System in Medicine. In: Proceedings of the 1
st
International Conference on Health Informatics,
HEALTHINF 2008, Funchal, Madeira, Portugal, pp.
298-304, INSTICC Press.
Nielsen, J., 2005. Medical Usability: How to Kill Patients
Through Bad Design. Jakob Nielsen's Alertbox, April
11, 2005,
http://www.useit.com/alertbox/20050411.html.
Puerta, A.; Eisenstein, J., 2002: XIML: A universal
language for user interfaces. In: Proc. of the
International Conference on Intelligent User
Interfaces, San Francisco, USA, 2002.
Zuehlke, D., Thiels, N., 2008. Useware engineering: a
methodology for the development of user-friendly
interfaces. In: Library Hi Tech, 26(1), Emerald
Insight.
HEALTHINF 2010 - International Conference on Health Informatics
354
