
ATTACK SCENARIOS FOR POSSIBLE MISUSE OF
PERIPHERAL PARTS IN THE GERMAN HEALTH
INFORMATION INFRASTRUCTURE
Ali Sunyaev, Alexander Kaletsch, Sebastian Dünnebeil and Helmut Krcmar
Chair for Information Systems, Technische Universität München, Boltzmannstraße 3, Garching, Germany
Keywords: Security Analysis, Electronic Health Card, Health Information Infrastructure.
Abstract: This paper focuses on functional issues within the peripheral parts of the German health information
infrastructure, which compromise security and patient’s information safety or might violate law. Our
findings demonstrate that a misuse of existing functionality is possible. With examples and detailed use
cases we show that the health infrastructure can be used for more than just ordinary electronic health care
services. In order to investigate this evidence from the laboratory, we tested all attack scenarios in a typical
German physician’s practice. Furthermore, security measures are provided to overcome the identified
threats and questions regarding these issues are discussed.
1 INTRODUCTION
Currently, German authorities are building up a
nationwide health information infrastructure, called
health telematics infrastructure (TI), which should
have been finished in 2006 (SGB V, 2007, § 291a).
Although there are still delays which evolved as a
consequence of various problems with the
introduction, the new electronic health card (eHC)
will be launched within the next few years (Sunyaev
et al. 2009a, p.19).
Bales (2003, p. 5) expects an improvement in
efficiency of the health care system and better
protection of patient’s rights after its introduction.
The eHC will contain administrative data as well as
information about a patient such as illnesses and
treatments. As this data is to be highly protected by
the physician-patient confidentiality and strictly
protected by law (Berg, 2004, pp.412-413), its
handling requires adequate care. Especially
complete data protection has to be ensured because
issues concerning privacy, safety, security and
availability directly apply to the patients (Sunyaev et
al. 2009b). The eHC, a smart card, is able to
guarantee this. Moreover, it can encrypt and sign
documents containing valuable information in order
to share them with trusted third persons and systems.
Based on ISO 27001 Standard for Information
Security Management Systems and BSI Security
Guidelines (BSI, 2004) as well as by extensive
laboratory experiments and an extensive review of
gematik’s specifications, we have provided a
security analysis (Sunyaev et al. 2009b), which
showed that open security issues, e.g. missing
authentication or unencrypted transmissions, can
result in making all peripheral parts of the telematics
infrastructure vulnerable.
In this paper, we present the continuation of that
security analysis. Possibilities for misuse of
functions provided by the peripheral parts of the
German health information infrastructure are
explained. The concerns are enriched with detailed
attack scenarios. Solutions and upcoming questions
to these issues are provided and discussed.
2 THE GERMAN HEALTH
TELEMATICS
INFRASTRUCTURE
Gematik (Gesellschaft für Telematikanwendungen
der Gesundheitskarte mbH), which was created
according to the law (SGB V, 2007, § 291b), is
conducting the introduction of the electronic health
card in Germany. Gematik has created all
specifications used in the health care telematics
infrastructure (these can be found at the
organization‘s website - http://www.gematik.de) and
229
Sunyaev A., Kaletsch A., Dünnebeil S. and Krcmar H. (2010).
ATTACK SCENARIOS FOR POSSIBLE MISUSE OF PERIPHERAL PARTS IN THE GERMAN HEALTH INFORMATION INFRASTRUCTURE.
In Proceedings of the 12th International Conference on Enterprise Information Systems - Databases and Information Systems Integration, pages
229-235
DOI: 10.5220/0002900102290235
Copyright
c
SciTePress

is responsible for their compliance.
Figure 1 presents the German health care
telematics infrastructure, which is divided into
central and peripheral parts. While the central part
consists of central databases stored in data centres,
the peripheral parts are used at the different
providers of service – e.g. in physicians’ practices,
hospitals or pharmacies (Schweiger et al. 2007, p.
694-695; gematik, 2008d, p.8).
Figure 1: German health care infrastructure.
In this paper, we focus on the usage of the peripheral
parts. The connector, which is the core of the
peripheral systems, manages all local connections. It
interacts with primary systems and card readers. A
primary system is a piece of software, which offers
the eHC’s functionality to the renderers of service. A
primary system can only access a card reader
through the connector, which establishes a secure
connection with the card reader using the Secure
Interoperable ChipCard Terminal (SICCT) protocol.
Any connections onto the central part are
managed by the connector. When connecting
peripheral parts and central part, the connector
establishes a protected VPN connection to the VPN
concentrator on the central side (Schweiger et al.
2007, p. 694-695; gematik, 2008d, p.8).
There will be two different kinds of cards. The
electronic Health Card (eHC), which will be
obligatory for all insurants, and the Health
Professional Card (HPC), which is for health care
staff only. Both are smartcards, i.e. each card type
has its own microprocessor with its own instruction
set (Caumanns et al., p.343). This clearly
distinguishes it from the present health insurance
card, which is only a memory card. Therefore, not
only administrative data about the insurant can be
stored. The insurant can decide whether information
for medical emergencies, pharmaceutical
documentations, prescriptions and medical reports
will be stored. Furthermore, one can decide whether
information is to be directly stored on the eHC or in
central databases (Neuhaus et. al., p.1).
Moreover, the card can perform different
functions on its own, e.g. secure signing and
encryption or decryption of documents. As the card
contains a so-called qualified signature (SGB V,
2007, § 291b), an electronic document signed by
that signature, is treated equally to hand signed
document before the law. Therefore, certificates
used by the electronic health card must be protected.
Figure 2 displays different classes of attack. In
ICEIS 2009, we already presented disruption of card
usage and spy on personal data. Disruption is
possible by compromising actions like permanent
card ejection, automatic filling or deletion of
prescriptions or even blocking a card. Personal data
can be stolen by retrieving administrative data,
prescriptions or medical emergency information
(Sunyaev et al. 2009b).
In this paper we focus on abuse of functions of
the peripheral parts. Section 3 shows how to pair a
card reader without explicit administrator
permission with the connector. After that, a scenario
is provided, which illustrates the misuse of the
connector’s and cards’ encryption and signing
functions. Finally, the creation of inconsistent
prescriptions is explained in detail in section 5.
3 ATTACHING UNSECURE
CARD READERS TO THE
CONNECTOR
As mentioned earlier, a patient’s eHC, which is
attached to a card reader, is only reachable through
the connector over the local area network in a
physician’s practice. No other type of connection
between card reader and connector is designated.
Furthermore, gematik (2008a, p. 26) enforces that
the card reader must only communicate with inserted
cards and with the connector. Therefore, it is not
possible that primary systems, which are the
interfaces to the physicians, connect directly to the
card reader and its attached cards. Thus, in order to
obtain patient information from an eHC, a data flow
from the primary system to the card reader has to be
established via the connector.
Gematik (2008a, p. 66) enforces that the card reader
initially has to be securely paired with the connector
by the administrator responsible. It has to be ensured
that the card reader is in the administrator’s personal
area. During the initial pairing process the card
reader has to be guarded, so it cannot be accessed by
any third party.
Admission is usually granted at the administra-
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
230
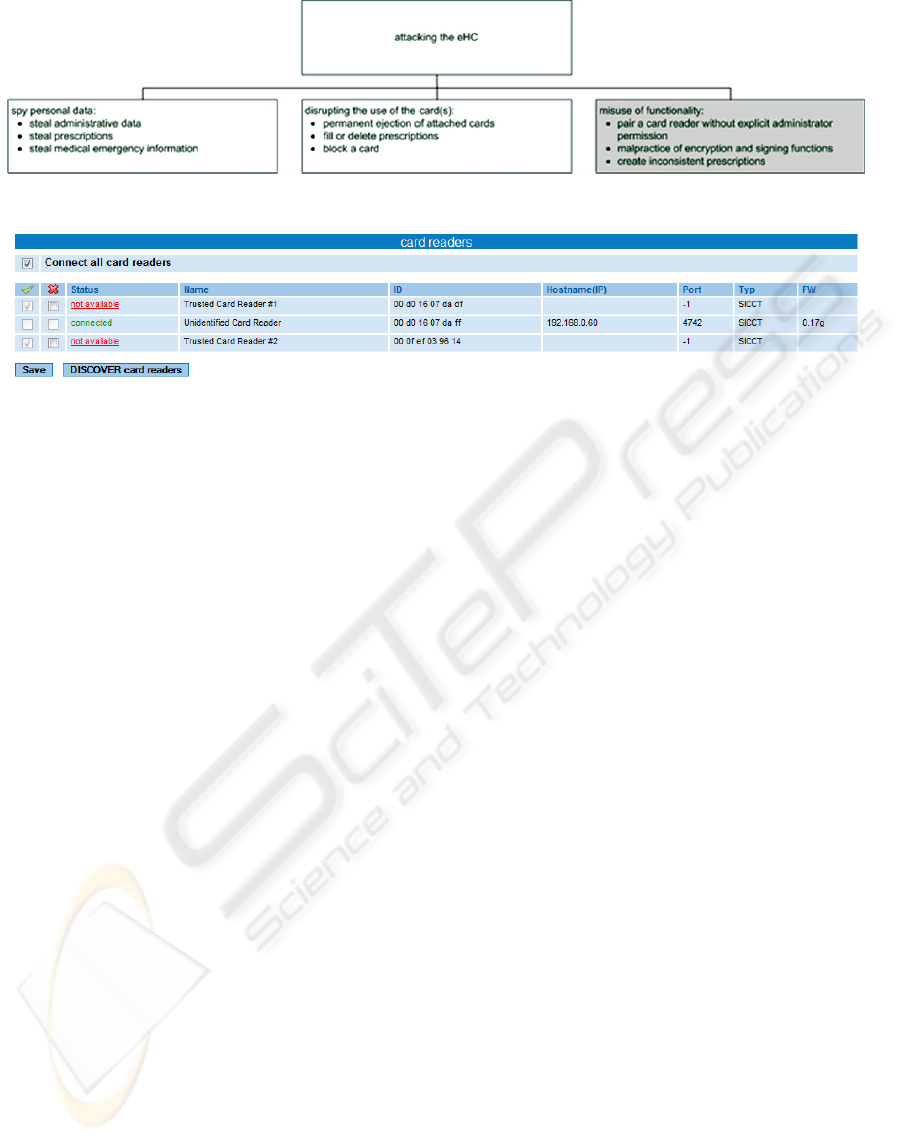
Figure 2: Attack tree.
Figure 3: Administrator web interface for granting admission to card readers.
tion website of the connector. The administrator can
select trusted card readers and put them to a
whitelist. Moreover, detailed information about
every card reader is provided to support his decision.
The connector used is part of the Futro S400
series by Siemens, version V1.07R4.8;
hpscV1.07R4_build_2533_R13907. Figure 3 shows
a table with all card readers attached. Each row
contains one card reader as well as its status, e.g.
connected, not connected or not available.
Furthermore, name of the card reader, MAC address,
IP, port, protocol and firmware-version are listed.
The administrator can approve a card reader by
checking a box in front of its representation in the
table.
The webpage of the connector offers the
possibility to set the connector into a mode, which
allows the automatic connection of every card reader
existing in the LAN. When “Connect all card
readers” is checked at the top-left of figure 3, every
card reader connected to the local area network will
be accepted automatically. Therefore, there is no
more need to activate card readers manually at the
bottom table.
This enables two different ways of proceeding.
In one case, the administrator hand selects every
card reader manually and approves each. In the other
case, all card readers are automatically accepted.
Therefore, the connector will gain access to every
card reader attached, which makes the security
check itself completely needless.
Insecure card readers in the peripheral parts of
the German health care information system acting as
regular ones constitute a threat. Those can be
utilized via the connector in order to access patient’s
data for reading or writing.
There are different possible scenarios which
could lead to serious security violations. First, an
additional card reader could be plugged into the
system without any notification. On the one hand, it
could just confuse patients and staff; on the other
hand, a foreign HPC plugged into the card reader
would enable an attacker to gain full access to all
cards plugged to any card reader in the physician’s
practice. Thus, it could be possible for the attacker to
read and write at any eHC wanted.
Secondly, a card reader could be exchanged with
a modified duplicate, which grips or modifies data in
a mischievous way. As no further approval exists,
the exchange most likely would not be detected.
Finally, after updating a currently approved card
reader to a new firmware version, there would be no
need to reinitiate the pairing manually, which could
be dangerous if the new firmware is modified in a
mischievous way.
This loss of control over the card readers
attached to the LAN is dangerous as shown in the
scenarios above. Furthermore, it violates gematik’s
regulations (gematik 2008a, p. 66). Therefore, the
automatic paring functionality has to be removed
from the connector.
4 MISUSE OF CRYPTING AND
SIGNING
In this section, we show how to abuse the functions
of connector and card to crypt and sign documents.
We show that it is possible to build up a secure
network with eHCs or HPCs. By doing so we state
ATTACK SCENARIOS FOR POSSIBLE MISUSE OF PERIPHERAL PARTS IN THE GERMAN HEALTH
INFORMATION INFRASTRUCTURE
231
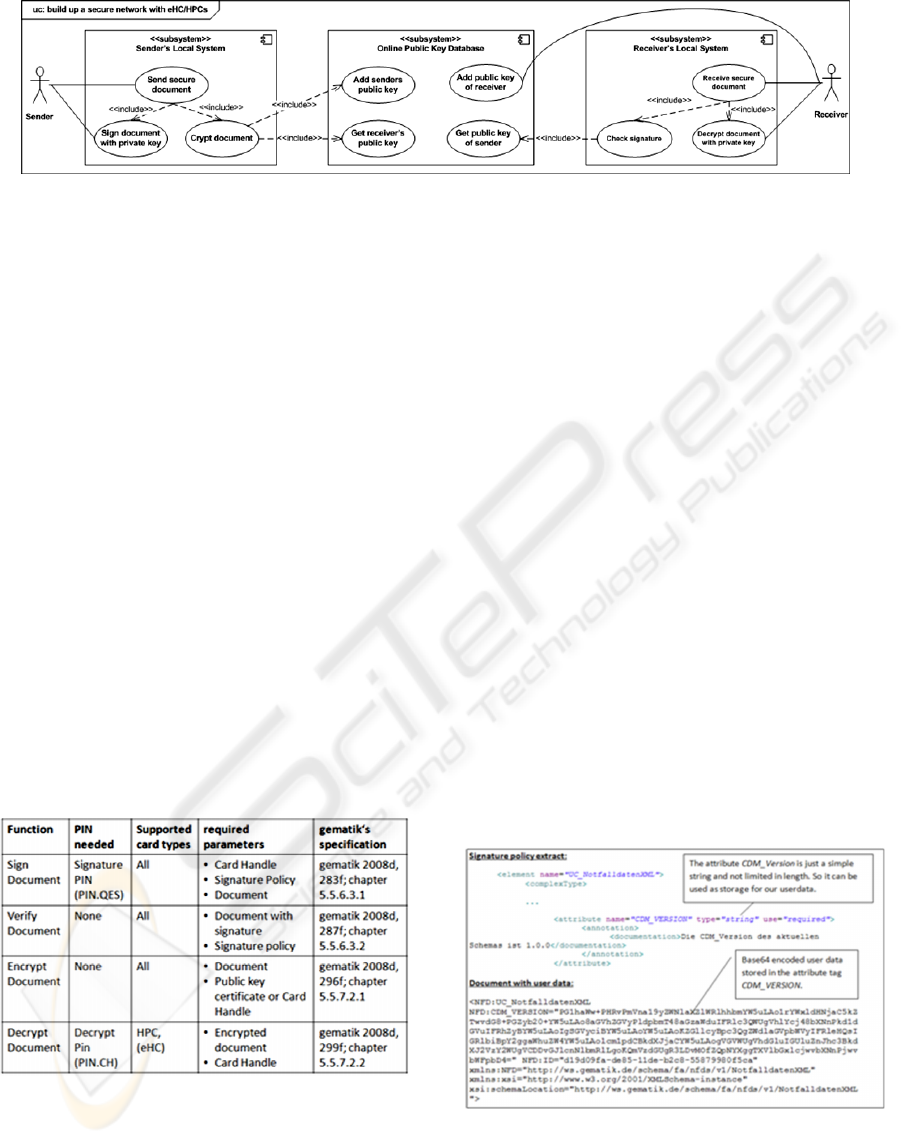
Figure 4: Secure message transportation scenario.
that the system can be used against its purpose and
therefore, against German law (SGB V, 2007, §
291a).
Figure 4 shows such a scenario in a simplified
way. It contains a sender which transmits a
confidential message. By encrypting the message
with the receiver’s public key, one can assure that it
can only be read by the receiver. The sender
identifies himself by signing the document with his
private key. Later on, the receiver can make sure to
have received the confidential message from the
right person by checking the message against the
sender’s public key.
All functionality, e.g. encrypting, decrypting,
signing and the signature check, are provided by the
sender’s and receiver’s local systems. Those consist
of standard modules of the peripheral parts of the
German health care telematics system.
Sender and receiver share an online system
which stores their public encryption keys and can
encrypt messages using them. It ensures the secure
key exchange between sender and receiver and can
prevent man-in-the-middle attacks in this phase.
Table 1: Used functions of the connector.
The sequence of actions in this scenario is the
following: At first the sender signs the document.
The signed document and its signature part then get
encrypted. After completing transportation the
receiver first decrypts the message and is then able
to check the document against its signature.
All functions used by the sender and receiver are
part of the peripheral systems of the German health
infrastructure. Table 1 lists all of them and their
required parameters, supported card types, PIN
requirements and their description in gematik’s
specification. The following sections (4.1-4.4)
explain these functions in detail.
4.1 Signing a Document
For the signing of a user document the function
SignDocument of the connector is used (see table 1).
It uses the document to sign, a corresponding
signature policy and a card handle, which refers to
the smart card that will sign the document, as
parameters. When signing the document, the card
will require the user to enter the corresponding
signature PIN at the keypad of the card reader.
Since the signing functionality of the connector
is limited to special xml structures by signature
policies (gematik 2008d, 506) a workaround
becomes necessary. A closer look into the signature
policies reveals such a workaround. In the
emergency signature policy a version attribute is set
as an unlimited string. Therefore, we can store user
data, which is base64 encoded for integrity reasons,
in there. Figure 5 shows how this works.
Figure 5: Hiding user data in an XML attribute.
4.2 Encrypting a Document
In order to encrypt a document the function
EncryptDocument of the connector, is used. All it
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
232

takes to encrypt the document is the public key
certificate. This functionality could be implemented
at the online key storage presented above, too.
In our scenario we decided to encrypt the already
signed document. Hence, the document is to base64
encode with its signature in order to hide both from
the encrypting module. It has to be mentioned that
the function expects XML documents, so a
surrounding root XML structure is created, too.
After encryption, the document can be safely sent to
the recipient.
4.3 Decrypting a Document
In order to decrypt a document, the function
DecryptDocument is called. It requires the encrypted
document and a card handle as parameters. If the
private key found on the card corresponds to the
public key, which encrypted the document, the
document will get successfully decrypted. The card
holder will have to enter his PIN at the card reader in
order to start decrypting. After removing the base64
encoding, the receiver will be able to see the plain
text, the sender transmitted to him.
It has to be stated that gematik (2008d, p. 299f)
does not allow decrypting with an eHC via the
DecryptDocument function. But in the context of
special applications it will be possible in future
(2008d, p. 299f).
4.4 Checking the Signature of a
Document
Finally, the signature of the document has to be
validated. Therefore, the function VerifyDocument
of the connector is called. As table 1 shows,
VerifyDocument requires the document with its
signature and the signature policy. If the integrity of
the signed document is verified, a confirmation
message will be shown.
4.5 Transmitting a Secure Document
Figure 6 summarizes four steps to secure a
document. The onion diagram shows in detail how
the original data document is modified and
embedded. It gives a good impression, of how the
data is modified while sending and receiving.
Figure 6: The data onion.
How Robust is such a Secure Transmitting
System?
Secure storage of private keys is most important for
the security of the system. They are stored securely
on the eHC and HPC. The backup, which exists at
the manufacturer for card-recreation and private
keys stored in the central parts of the telematics
system, can compromise security.
As those storages are well protected against
unauthorized access, we can still assume the
transmitting system to be secure.
How can One Obtain eHCs or HPCs?
Every German insurant will receive one eHC. Some
of them could try to misuse their cards for functions
like the ones mentioned above. But it is conceivable
that healthcare staff use their HPCs accordingly.
Moreover, criminals might try to simply steal
cards. E.g., it has to be assumed that the physician is
not the only one knowing the PIN.QES for a HPC.
Often nurses often do so, too. Therefore, thieves
might be able to obtain the HPC and its PIN.QES
with some social engineering.
Does Black-listing Private Keys from Stolen
Cards impRove the Situation?
It will work quite well, if access to the blacklist is
not prevented. But gematik (2008c, p. 78) explicitly
stipulates that access to private keys must be
continued, if there is no reachable blacklist.
Therefore, it will be quite easy to overcome this
feature, if one uses the offline mode of the
connector.
What would be a Possible Solution to Prevent this
Scenario?
One possible solution would be the enforcement of a
present global authentication server, which provides
ATTACK SCENARIOS FOR POSSIBLE MISUSE OF PERIPHERAL PARTS IN THE GERMAN HEALTH
INFORMATION INFRASTRUCTURE
233
blacklists for decrypting. But this would add a single
point of failure to the system.
Would not a More Restricted Signing and
Encryption Policy Help to Fix this Problem?
We are well aware that such security breaches, like
the XML specification gap, can be easily closed
when uncovered. But there would still be other
possible strategies to hide user data conforming to
the signature policy. E.g., an algorithm could split
user data into fitting parts which are then distributed
all over the conform document. Although the
message space would be quite limited, it would
mostly be enough to transmit confidential text
messages.
Can you give a Concrete Example of Usage?
We were able to encrypt and sign emails, which
were then sent to an Internet mail server. Later on,
the emails could be received and successfully be
decrypted and verified.
Therefore, two web interfaces were created. One
is used for encrypting and signing emails. The user
can grab a public key of the card or choose any user-
defined certificate. A sender’s and receiver’s email-
address can be chosen as well as the title of the
message and the document. The other contains the
interface to the receiver. After selecting the
designated email account and email message, the
corresponding card for decrypting is chosen. The
user will be shown the encrypted message as well as
the plain text message. Moreover, the interface
offers the functionality to verify an email which was
signed before.
5 CREATING INCONSISTENT
PRESCRIPTIONS
In ICEIS 2009, we presented the possibility to delete
or fill prescriptions without any effort of a
pharmacist by calling the function DeleteVO or
DispenceVO. In this section we take a closer look at
the prescription itself, which we are going to write to
an eHC by using WriteVO.
A prescription consists of information about the
insurant and his insurance coverage as well as the
dispensing institution and the drug prescription
itself. Both pieces of information about the insurant
and the dispensing institution contain the names and
addresses of the corresponding persons and are
equipped with one unique id each.
According to gematik (2008b, p. 19-27) and
verified by our tests, the XML document is checked
against a strict scheme before being signed and then
written on the eHC. Unfortunately, the plausibility
of the content written is not checked sufficiently.
Except for the insurant’s id, which is checked for
consistency with the id of the eHC, no other value is
validated. Therefore, we are able to write a XML
document containing fake data onto an eHC.
On the front side of the card there are patient-
related information, a picture of the insurant and the
microchip. Furthermore, some recognition features
are placed there, e.g. braille, the name and logo of
the providing insurance company. On the back, there
is the European health insurance card (EHIC)
(Drees, 2007, p. 1).
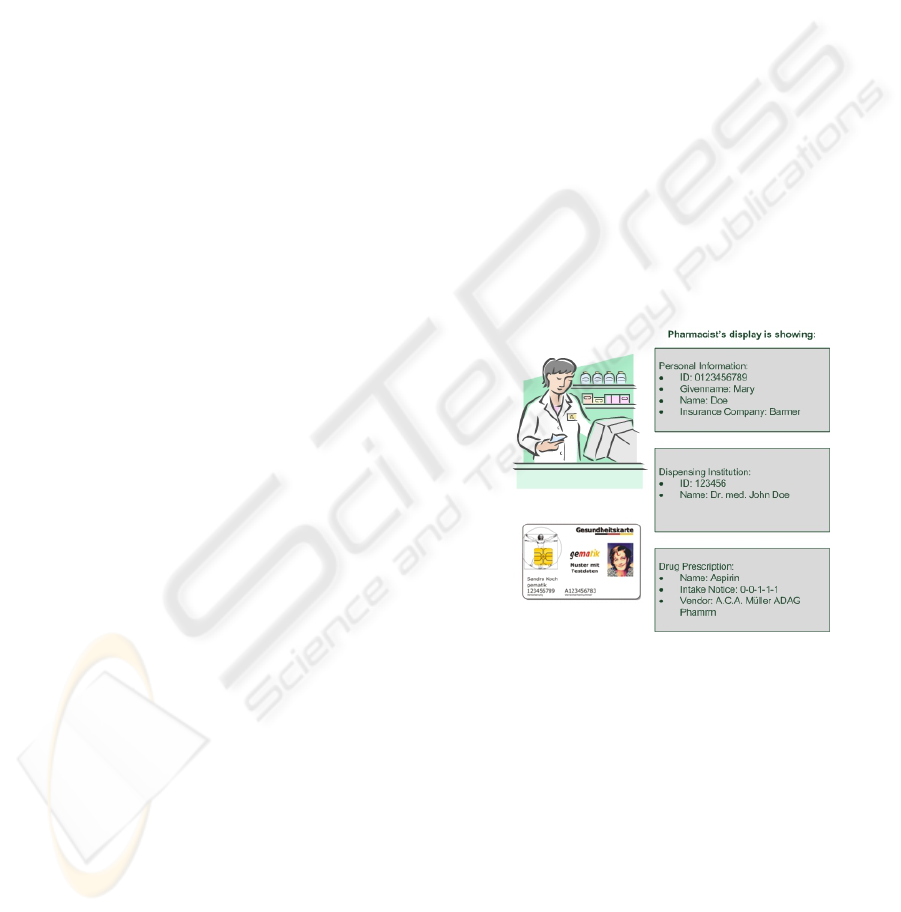
When analyzing figure 7 and comparing the
image of the HPC with the data presented on the
right sight of the figure, one will notice two out of
three of the following inconsistencies:
1) Wrong patient name
2) Wrong insurance company id and name
3) (Wrong dispensing institution)
Especially when the prescription data is displayed on
the pharmacist’s computer, it is quite likely that
these differences will not be recognized.
Figure 7: Pharmacist reading inconsistent prescription.
Why is this Dangerous?
When a pharmacist serves a patient, there probably
would not be enough time to compare every field of
the eHC to the document fields of the prescription.
Therefore, it is quite likely that inconsistencies will
not be recognized. Especially when considering, that
the card will be plugged into the card reader while
the prescription document is shown, there even will
not be a possibility of comparison.
Can the Real Values be Restored?
They can, but only at some administrative costs. As
the dispensing person’s certificate is attached to the
prescription and is delivered to the pharmacist it is
actually no problem to restore the correct physician.
ICEIS 2010 - 12th International Conference on Enterprise Information Systems
234

The patient’s real name and address can be restored
by tracking his insurant’s id. With the id and the
timestamp from the signature of the prescription it
should be possible to receive the right insurance
company’s information. Therefore, backtracking and
reconstruction is always possible, however it will
take some time and hence be costly.
How can these Costs be Saved?
Actually, there is no need to copy patient’s personal
information, insurance data or dispensing person’s
data into the prescription as it is already stored at the
eHC. Therefore, the avoidance of creating duplicate
information would not only save storage space, but
also reduce risks.
How to Deal with Prescriptions for Third Persons
and Consumables for a Doctor's Surgery?
In these special cases, a flag should be set which
informs the pharmacist. Only then it should be
allowed to add extra information about the receiving
third persons.
6 CONCLUSIONS
In this paper, we presented different scenarios,
which show that the functions of the German
electronic health card’s peripheral parts can be
abused. Three possible attacks were presented:
- Automatic pairing of card readers and
connector without administrative guidance
- Misuse of encryption and signing
- Creating inconsistent prescriptions
Possible solutions were given and further
questions discussed. The automatic pairing function
would need to be deactivated at the connector, which
will hardly cost anything. Therefore, this should be
done immediately. Preventing misuse of
functionality and creation of inconsistent
prescription might prove to be more costly. The
scenarios mentioned in this paper should be included
in the overall security specification in order to make
people aware of the possible risks.
As the German electronic health card is currently
on hold and redesigned in parts, security related
parts will have to be reconsidered and newly
checked once the moratorium ends. As presented in
this paper, there is not only a need for proving
information security, but the absence of possibilities
to abuse functions must be checked, too.
Furthermore, a security analysis concerning the
central parts as well as the use and play of value-
added-applications has to be performed.
REFERENCES
Bales, S., 2003. Die Einführung der Telematik im
Gesundheitswesen als Herausforderung für die
Weiterentwicklung der Patientenrechte in
Deutschland. [Talk] Bonn: gematik. Available at:
http://www.dimdi.de/dynamic/de/ehealth/karte/downlo
adcenter/veroeffentlichungen/vortraege/bagh-bonn-
bal-031107.pdf [Accessed 9 September 2008].
Berg, W., 2004. Telemedizin und Datenschutz.
Medizinrecht, 22 (8), pp. 411-414.
BSI, Bundesamt für Sicherheit in der Informationstechnik,
2004. Studie zu ISO-Normungsaktivitten ISO/BPM -
Anforderungen an Information Security Management
Systeme.
Caumanns, J. et al., 2006. Die eGK-Lösungsarchitektur
Architektur zur Unterstützung der Anwendungen der
elektronischen Gesundheitskarte. Informatik-
Spektrum, 29 (5), pp. 341-348.
Drees, D., 2007: The Introduction of Health Telematics in
Germany. In: European Commission Directorate
General Information Society, Information Security
Solutions Europe/SECURE 2007 Conference. Poland,
Warsaw 25 27 September 2007. Vieweg: Wiesbaden.
gematik, Gesellschaft für Telematikanwendungen der
Gesundheitskarte mbH, 2008a. Spezifikation eHealth-
Kartenterminal. Version 2.8.0.
gematik, Gesellschaft für Telematikanwendungen der
Gesundheitskarte mbH, 2008b. Facharchitektur
Verordnungsdatenmanagement (VODM). Version
1.5.1.
gematik, Gesellschaft für Telematikanwendungen der
Gesundheitskarte mbH, 2008c. Übergreifendes
Sicherheitskonzept der Gesundheitstelematik. Version
2.3.0., Anhang B.
gematik, Gesellschaft für Telematikanwendungen der
Gesundheitskarte mbH, 2008d.
Konnektorspezifikation. Version 3.0.0.
Neuhaus, J., Deiters, W. & Wiedeler, M., 2006.
Mehrwertdienste im Umfeld der elektronischen
Gesundheitskarte. Informatik-Spektrum, 22 (5),
pp.332-340
SGB V, 2007. Sozialgesetzbuch. Fünftes Buch. DTV-
Beck.
Schweiger, A., Sunyaev, A., Leimeister, J.M., Krcmar, H.
2007. Information Systems and Healthcare XX:
Toward Seamless Healthcare with Software Agents.
In: Communications of the Association for
Information Systems (CAIS), Vol. 19 (2007) Nr.
Article 33, pp. 692-709.
Sunyaev, A. et al., 2009a. Analysis of the Applications of
the Electronic Health Card in Germany. In: WI 2009,
Proceedings of Wirtschaftsinformatik 2009, Austria,
Vienna 25-27 February 2009.
Sunyaev, A., Kaletsch, A., Mauro, C. & Krcmar, H.
2009b. Security Analysis of the German electronic
Health Card’s Peripheral Parts. ICEIS 2009 -
Proceedings of the 11th International Conference on
Enterprise Information Systems, Volume ISAS, pp.
19-26.
ATTACK SCENARIOS FOR POSSIBLE MISUSE OF PERIPHERAL PARTS IN THE GERMAN HEALTH
INFORMATION INFRASTRUCTURE
235
