
FALL DETECTION SYSTEMS
A Solution based on Low Cost Sensors
Miguel A. Laguna, María J. Tirado, Javier Finat and José M. Marqués
GIRO and MoBiVAP groups, University of Valladolid, Campus M. Delibes, 47011Valladolid, Valladolid, Spain
Keywords: Fall Detection, Accelerometer, Sensor, Monitoring System.
Abstract: The problem of fall detection in elderly patients is particularly critical in persons who live alone or are alone
most of the day. The use of information and communication technologies to facilitate their autonomy is a
clear example of how technological advances can improve the quality of life of dependent people. This
article presents a prototype developed with a low cost device (the gamepad of a known video console) using
its Bluetooth communication capabilities and built-in accelerometer. The latter is much more sensitive than
other similar devices integrated in mobile phones and much cheaper than industrial accelerometers. Besides
its stand-alone use, the system can be connected to a generic remote monitoring system that has been
developed as a software product line for use in aged people’s residences.
1 INTRODUCTION
Dependence can, in general, be defined as the need
for significant aid or assistance for the activities of
daily life. Population aging is a factor that, in the
future, will significantly increase the percentage of
dependent population, due to the close relationship
between dependence and age. The role of
information and communication technologies (ICT)
as a mechanism of social integration for older,
disabled or dependent people in general is
spreading rapidly among many sectors of the
population. The increased costs of care and the
geographic dispersion of an aging population favor
the deployment of personalized services based on
low cost distributed systems with ubiquitous
computing tools. Wireless networks allow services
adapted to different scales (large areas through
wireless/cellular networks or home environments
using short-range communication technologies such
as Bluetooth) and provide overall support to these
remote monitoring systems.
These technologies have generated huge
expectations but we should ensure that their costs
are affordable. We need to provide personalized
care accessible to more people while reducing the
costs of health systems. In addition to patients,
other people with varying degrees of dependence
can improve their level of autonomy: persons with
different physical or mental disabilities, the elderly
who live alone or in residences, etc. The PATRAC
project (in Spanish,“PATrimonio ACcesible”,
Accessible Heritage) is designed as a set of services
that include monitoring of dependent visitors to
cultural environments. In this context, one of the
most common problems, especially in older people,
is the detection of accidental falls, taking into
account such facts as (Salva et al., 2004)
• 30% of people over 65 fall at least once a year.
• Fear, anxiety and depression are rising due to
the risk of falls.
• Falls are responsible for 70% of fatal injuries for
people over 75 years of age.
• A fall in an old man, even if it is a mild one, can
cause irreversible damage or death.
For these reasons we determined the development
of a system that automatically detects falls to
augment the functionality of the abovementioned
monitoring system. The advantages are clear, as
these systems can increase the safety of older
people, giving them the possibility of autonomy,
while providing comfort to their families and
caregivers. A secondary objective is to reduce the
costs of caring for dependents. The original plan
included:
• Finding or adapting a reliable fall detection
algorithm that minimizes false positives and
can detect all types of falls.
121
Laguna M., J. Tirado M., Finat J. and M. Marqués J. (2010).
FALL DETECTION SYSTEMS - A Solution based on Low Cost Sensors.
In Proceedings of the 5th International Conference on Software and Data Technologies, pages 121-126
DOI: 10.5220/0002918101210126
Copyright
c
SciTePress

• Defining the technical characteristics of the
sensor needed to implement a system using the
selected algorithm.
• Implementing the algorithm on a prototype to
check its performance in simulated falls and
rapid movements (to eliminate false positives),
leading finally to real situations.
The rest of the article details the proposed solution,
beginning with the study of the detection algorithms
published in the medical literature. As a result, an
algorithm that combines the advantages of various
methods is proposed and the requirements of the
sensors needed for the implementation are stated.
Section 3 shows how a low cost accelerometer can
achieve those requirements and finally Section 4
presents the design and the results of the
simulations carried out. Finally, similar products are
compared, and the conclusions and future work
close the paper.
2 FALL DETECTION
An initial review of the literature convinced us of
the advantages of accelerometers as the most
suitable type of sensors to detect falls. Although
there are other alternatives, such as the use of
gyroscopes (Bourke and Lyons, 2008), most works
use two or three axes accelerometers (Bourke et al.,
2004) (Chen et al., 2005). To design a reliable
detection system based on these devices, the
accelerations naturally present in the human body
must be previously documented, both in normal
movements and different types of falls. Various
medical articles have studied these accelerations.
When a person falls and hits the ground, his body
suffers accelerations above those that occur when
he is performing a normal activity. The work (Chen
et al., 2005) studied the differences between sitting
movements and falls by means of experiments with
two two-axis accelerometers. Although the graphics
were very similar, during a typical fall the
acceleration is 7g, while the accelerations measured
when a person sits down are less than 3g (about
2.6g where measured). Looking at the graphs
presented in that article, it is noteworthy that, at the
beginning of the fall, acceleration decreases
(indicating the period of fall), but immediately there
is a large peak indicating the impact against the
ground (7g approx.). The accelerometer
measurements, before and after the fall, are held at
about 1g, as expected. Similar results, even with
major peaks, were observed in lateral falls.
From the viewpoint of the type of falls, Lord et
al. (Lord et al., 1993) found that 82% occurred
when people were upright. The most common falls
occurred while an elderly person is walking, slides
and falls. Another study, conducted by (O'Neill et
al., 1994), found that, of 180 crashes recorded, 160
were forward and, in 60% of these, the subject was
taking a step forward with one bent knee and one
foot in the air, the typical movement of a walking
step.
With these studies as a reference, (Bourke et al.,
2007) attempted to define the acceleration threshold
that can automatically discriminate between normal
body movements and different types of falls. The
values of the accelerations were derived from daily
activities performed by elderly people and
simulated falls performed by young people. The
first experiment involved ten elderly people, aged
between 70 and 83, with a tri-axial accelerometer,
placed first on the trunk and then on the thigh. The
activities were sitting and rising from an armchair
or a kitchen chair, walking 10 m, etc. The second
experiment used ten young people aged between 21
and 29 who simulated six different types of falls.
Although forward falls are more frequent, they also
simulated lateral falls, as these often produce a great
impact on the trunk and often result in fractures
when they happen. The authors selected the lowest
value of the accelerations recorded during simulated
falls (upper fall threshold), and the largest of the
smaller peaks (lower fall threshold). The smallest
accelerations during a fall were about 3.5g but
others were much greater, while normal activities
usually produced accelerations of 1 to 2.5g,
although sometimes there are activities, such as
running or sitting, which can surpass this. In
conclusion, the threshold of normal movements
should be between 0.41g and 3.52g. The
acceleration values outside this range could be
considered potential falls. The success percentage
of the algorithm, including false positives, was
calculated with the accelerometer placed on the
trunk and on the thigh. The best results were
obtained for the trunk, with more than 90% correct
hits. But false positives (false alarms) remained the
real problem.
(Chen et al., 2005) used a different approach
that took into account the unexpected changes in
body orientation. They also studied the situations of
repeated impacts to determine certain types of falls
(on staircases, for example) that may be especially
dangerous. Based on these studies, we propose an
experiment using an algorithm that combines the
orientation changes postulated by Chen and the
ICSOFT 2010 - 5th International Conference on Software and Data Technologies
122

thresholds measured by Bourke. To carry out these
measurements, the required sensor must have the
following specifications:
• The accelerometer must be tri-axial.
• It must be capable of detecting accelerations
over 3.52g and under 0.41g, as these are the fall
thresholds. This requirement eliminates many of
the available accelerometers, particularly those
embedded in current mobile phones with no
more than 2g sensibility.
• It must operate in a wireless environment.
• It must work for several hours. The battery life
is the key point here.
• Its weight and size should be reduced, since it
will be placed on the patient’s body (preferably
integrated in the patient’s clothes).
3 THE WIIMOTE AS
ACCELEROMETER
The Wiimote is the main controller from the
popular Nintendo Wii game console. Its main
features are the ability to detect motion in space and
that of pointing to objects on the screen. The design
of the Wiimote is not based on traditional video
game controllers but is intended to be used with one
hand in an intuitive way. Because of its low cost
and its potential, there are many initiatives that are
evaluating their possibilities. WiiHome is an
application developed by (Lee, 2009) to control the
home through home automation devices (you can
turn on and off a light, the TV, an alarm, etc.). The
CEDETEL Research Centre (CEDETEL, 2009) is
developing a series of applications for rehabilitation
and increasing cognitive abilities for disabled
people. They use the Wiimote as a device that
allows the movements of patients to be captured
and recorded so as to monitor their assigned
exercises and to automatically control the degree of
personal improvement.
The gamepad detects the acceleration measured
along three axes using a built-in accelerometer
(Figure 1). The batteries can power the Wiimote for
60 hours using only the accelerometer function
(very interesting for our requirements). It uses
Bluetooth to communicate with the console but is
detected by other Bluetooth devices such as PCs or
mobile phones.
The built-in tri-axial accelerometer provides
instant acceleration values. The maximum value
that can be measured is about 7g, which complies
with the requirements specifications. In repose, this
acceleration is 1 g, upwards. While falling, the
Wiimote indicates lower accelerations, close to 0g.
Once the arbitrary accelerations provided by the
Wiimote are captured and assuming that the
accelerometer response is approximately linear, we
can use standard positions to calibrate the controller
on a flat surface: two horizontal positions that
provide the values (x1, y1, z1) and (x3, y3, z3) and
a third upright position giving the vector (x2, y2,
z2). Because the accelerometer records the force of
gravity, the data received in the three positions
should be matched with three orthogonal
acceleration vectors, so that in each of the three
positions indicated, two of the three components of
each vector will be zero and the third 1 g. Using the
values provided in real time by the command
(
XValue, YValue, ZValue, see Figure 1), we
can convert these values into three orthogonal
vectors with respect to g. Given
x0=(x1+x2)/2,
y0=(y1+y3)/2, and z0=(z2+z3)/2 we have:
X = (XValue - x0)/(x3 - x0)
Y = (YValue - y0)/(y2 - y0)
Z = (ZValue - z0)/(z1 - z0)
Figure 1: Wiimote and its accelerometer axes.
This transformation of the Wiimote raw data in
position 1, as described previously, gives the values
(1,0,0), in the second position (0,0,1), and in the
third one (0,1,0) . Once calibrated, we have
reproduced the studies of previous works with the
Wiimote accelerometer, checking that the values of
the accelerations measured for the same activities as
the previous research give close enough values. In
our case, the tests were carried out by three people
aged between 23 and 50. These tests were walking,
sitting, getting up (Table 1). The upper fall
threshold (UFT) in the walking test using the
Wiimote was 2.04, while in the study of (Bourke
and Lyons, 2008), it was 1.99g. In the same test, the
lower fall threshold (LFT) was 0.66g while in the
cited study it was 0.62g, both close enough. The
WiimoteLib library was used (Brian, 2009) to
manage the Bluetooth connection.
FALL DETECTION SYSTEMS - A Solution based on Low Cost Sensors
123
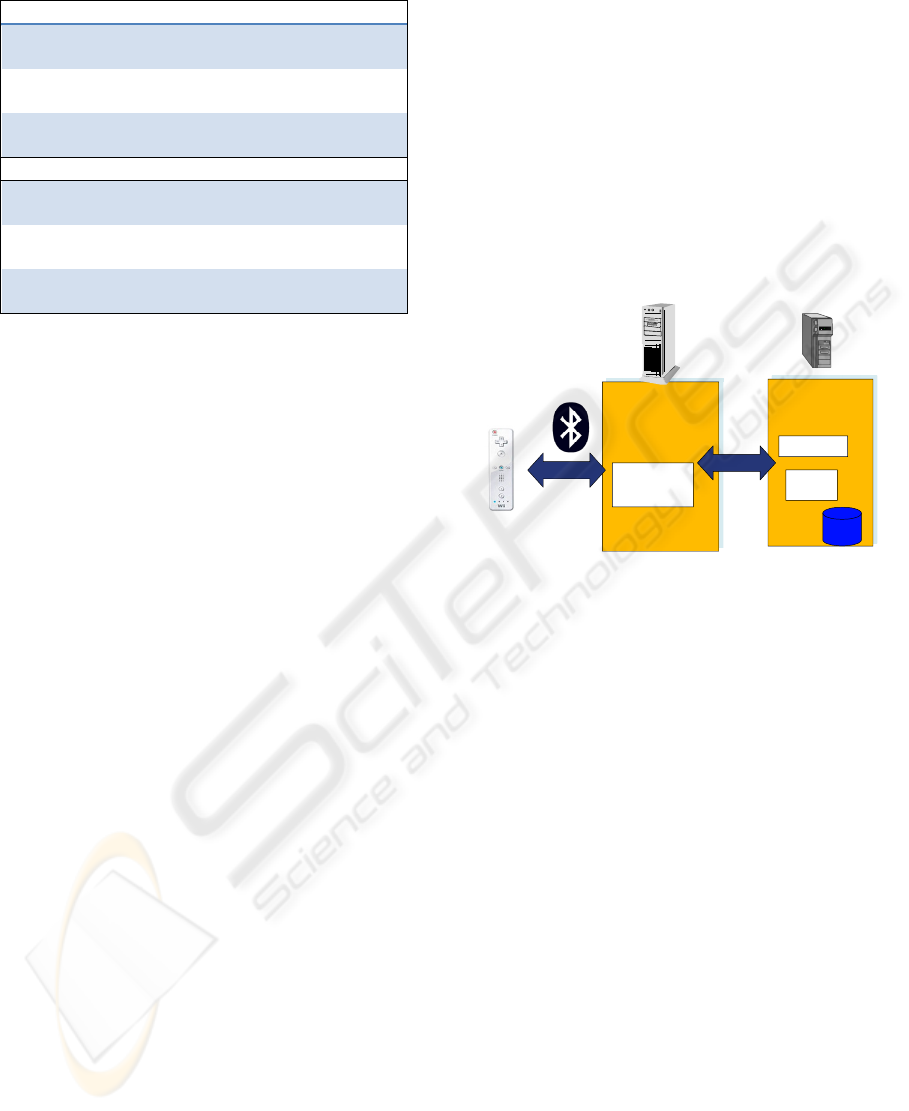
Table 1: Acceleration values (measured with a Wiimote).
Walking UFT LFT UFT LFT UFT LFT
Person
1
1.70 0.60 2.04 0.57 1.76 0.65
Person
2
1.80 0.61 1.65 0.66 1.69 0.63
Person
3
1.72 0.62 1.74 0.58 1.93 0.54
Sitting UFT LFT UFT LFT UFT LFT
Person
1
2.63 0.65 1.60 0.73 2.00 0.57
Person
2
1.36 0.83 1.33 0.80 1.36 0.79
Person
3
1.48 0.59 1.49 0.72 1.36 0.72
4 DESIGN OF THE FALL
DETECTION SYSTEM
The system was developed in response to a set of
basic requirements, validated by the medical staff of
a senior citizens’ residence to help us in developing
monitoring systems. The most representative are:
• The system must notify the medical staff in real
time that the patient has suffered a possible fall.
• The system will send an alarm to the central
server when a possible fall is detected.
• The system should allow the patient to know
when an alarm has been sent to the server.
• The system must allow the patients to deactivate
the alarm if they see they need no attention.
• The system should allow the patients to make an
emergency call when they think they need
medical attention.
• The central system should provide a status
picture of all the connected sensors, including
the battery status, at any time.
• The central system must associate a Wiimote
with each patient to identify the received data.
NET and C # were used to develop the system, due
to the ease of integration with the available platform
libraries. The main actors are the patient and
supervising personnel (usually medical staff but can
also be a member of the family). An actor models
the automatic data that are obtained every few
seconds (the time interval is configurable). The
current version has been developed for home
scenarios (or in a small residence), since the limits
are defined by the Bluetooth connection range (a
maximum theoretical distance of 100 meters).
The overall system architecture is shown in Figure
2. The acceleration data are collected by an
auxiliary computer, located at the home of the
monitored person and analyzed in real time. If a
situation reflects a possible fall, the vibration of the
patient's own Wiimote indicates the problem and
after a few seconds an alarm is generated to be sent
to a central system via http using a generic Web
service. This system allows alarms to be collected
and data to be continuously monitored, including
the patient location obtained from devices with
built-in GPS (Laguna et al., 2009). The elapsed
time from the moment of detection until the alarm
is sent allows the person to cancel the alarm if it is a
false positive.
Auxiliary PC
(Patient
home)
Web se rvice
Configuration
Data and
calibration
Historical
Data
Content
Web Service
(Medical
experts)
HTTPHTTP
Figure 2: Architecture of the fall detection system.
The tests reflected in Table 2 were planned to check
the effectiveness of the system. They were divided
into two groups: normal movements (to detect false
positives) and fall simulations by young people, due
to the high risk that real falls represent for elderly
people. For this purpose, the Wiimote was fixed to
the hip of the subjects (Figure 3) and the system
was installed on a standard PC, with a set of
windows that continuously display the status of
each registered sensor.
The tests have been encouraging. In total, 65
tests simulating falls have been conducted and the
system has identified 55 possible falls with a
success rate of 84.6%. One might consider this
success rate to be low, but we must keep in mind
the fact that the falls the system has not been able to
recognize were all of the same type, a fall type
resulting in the trunk remaining straight after the
fall (“fall to a sitting position”). The way the
detection algorithm is designed, based on shifting
and impact, does not generate an alarm, as the
sensor continues in a vertical orientation (like the
trunk of the person). We are working on improving
the algorithm, although one might think that if a
person falls into this position (perhaps the least
dangerous of the considered types of falls), there are
ICSOFT 2010 - 5th International Conference on Software and Data Technologies
124

many chances that the patient can press the
emergency button, also programmed in the sensor.
Table 2: Results of the fall detection tests.
Normal movements Tests False positives
Walking 20 meters 10 0
Going downstairs 10 0
Sitting on an arm
chair
10 0
Going up 7 steps 10 0
Lying down in bed 10 5
Getting out of bed 10 5
Running 20 meters 10 0
Simulated Falls Tests
Recognized
falls
Front fall 10 10
Reverse fall 10 10
Lateral fall 10 10
Right trunk fall 10 0
Random fall 25 25
Concerning normal movement tests, the success
rate was 88.8%. The system indicated 10 false
positives of the 90 tests performed. In this case,
false positives occurred in a specific type of
movement, lying down and getting out of bed when
the move was made without first sitting (“jumping
from the bed"). In the tests where the subject first
sat on the bed and then lay down (or got out) there
were no false positives. Given that older people
have limited mobility, it is rare they get out of bed
quickly, so the problem should be minor in practical
situations.
Figure 3: Correct placement of the sensor in the trunk.
Besides improving the algorithm, we are working
on a second version for outdoor patient monitoring,
using a Smartphone. The same algorithm has been
implemented using the accelerometers present in
two types of mobile devices based on Windows
Mobile (HTC Diamond and Omnia Samsung),
joining the sensor and the PC functionality in a
single device. The alarm can be sent via 3G Wi-Fi
(or SMS to a configurable phone number).
However, the results are not as reliable due to the
lower range of accelerations measured.
5 RELATED WORK
Given the interest in the topic, many works have
dealt with the development of devices and the
associated algorithms to detect falls. (Degen et al.,
2003) created "Speedy", a fall detector that operates
via an accelerometer placed in a wristwatch. The
algorithm uses a multi-stage approach: during the
first stage, it looks for a high acceleration toward
the ground, followed by an impact. Once the impact
is detected, if a period of inactivity greater than 40
seconds follows, an alarm is activated. This device
was successful in not producing false alarms, but
was a disaster in falls other than front variants. It
was unable to detect other fall types such as lateral
or backward falls.
The Tunstall falls detector is a commercial
system, developed by (Doughty et al., 2000), which
uses a fall detection algorithm with two steps. They
use two sensors: the first one detects the impacts,
while the second considers the orientation. In short,
when an impact is detected, the orientation of the
system during the periods previous and posterior to
the impact are analyzed and if there is a change of
orientation the alarm is activated.
The obvious advantage of our system compared
to existing products is its cost (less than 70 €
including the cost of the sensor and a Bluetooth
device that can turn any domestic PC into an alarm
detection system).
6 CONCLUSIONS
This article describes a monitoring system based on
an algorithm capable of detecting a wide range of
falls and of eliminating many false positives. Based
on published studies, the results have been
reproduced in a satisfactory manner, improving
them in some cases. Its performance has been tested
in simulated falls and normal but relatively violent
movements. The identified technical characteristics
limit the useful sensors (tri-axial accelerometer with
sensitivity better than 3.5g, wireless, light ...). A
FALL DETECTION SYSTEMS - A Solution based on Low Cost Sensors
125

basic architecture has been implemented, using a
conventional PC connected via Bluetooth with a
low cost device (the gamepad of a video game
console).
Work in progress is devoted to integrating the
system into a generic product line of mobile
monitoring. Finally, to check the device in real
patients, some tests have been scheduled in two
residences that have shown interest in the device
and have previously collaborated on the
development of the generic application of
continuous monitoring of physiological parameters.
ACKNOWLEDGEMENTS
This work is supported by the Spanish MICINN and
FEDER funds (PS-380000-2009-002 PATRAC and
TIN2008-05675 projects).
REFERENCES
Bourke, A., O’Brien, J., Lyons, G. Evaluation of a
threshold-based tri-axial accelerometer fall detection
algorithm, Gait & Posture, Volume 26:2, pp 194-199,
2007.
A. Bourke, G. Lyons, A threshold-based fall-detection
algorithm using a bi-axial gyroscope sensor, Medical
Engineering & Physics, Volume 30, Issue 1, Pages
84-90, 2008
Brian, P. WiimoteLib. availaible from
http://www.codeplex.com/WiimoteLib (2009)
CEDETEL: Centro para el Desarrollo de las
Telecomunicaciones de Castilla y León
http://www.cedetel.es/ (2009)
Clements, Paul C., Northrop, Linda. “Software Product
Lines: Practices and Patterns”. SEI Series in Software
Engineering, Addison-Wesley. 2001.
Chen J., Kwong Karric, Chang, Jerry Dennis Luk, Bajcsy
Ruzena, Wearable Sensors for Reliable Fall
Detection, Proceedings of the 2005 IEEE Engineering
in Medicine and Biology 27th Annual conference,
Shanghai, China, September 1-4, 2005
Degen T., Jaeckel H., Rufer M., and. Wyss S,”SPEEDY:
a fall detector in a wrist watch,” Proc. Seventh IEEE
International Symposium on Wearable Computing,
2003, pp. 184-187
Doughty K., Lewis R., and McIntosh A.,”The design of a
practical and reliable fall detector for community and
institutional telecare,” J. Telemed. Telecare 2000, 6
S150-4.
Laguna, M.A., Finat, J., González, J.A. Remote Health
Monitoring: A Customizable Product Line Approach.
Proceedings of IWAAN, LNCS 5518, 2009, pp 726 –
733.
Lee, J., Proyectos con Wiimote, availaible from
http://johnnylee.net/projects/wii/ (2009)
Lord SR, Ward J. A., Williams P., Anstey K. J. An
epidemiological study of falls in older community-
dwelling women: the Randwick falls and fractures
study. Aust J Public Health 1993;17(3):240–5.
O’Neill T. W., Varlow J., Silman A. J., Reeve J., Reid D.
M., Todd C., et al. Age and sex influences on fall
characteristics. Ann Rheum Dis 1994;53(11):773–5.
Salva A., Bolibar I., Pera G., Arias C. Incidence and
consequences of falls among elderly people living in
the community. Med Clin (Barc) 2004; 122 (5):
172–6.
ICSOFT 2010 - 5th International Conference on Software and Data Technologies
126
